Differentiation of Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma through MRI Radiomics

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MRI Acquisition
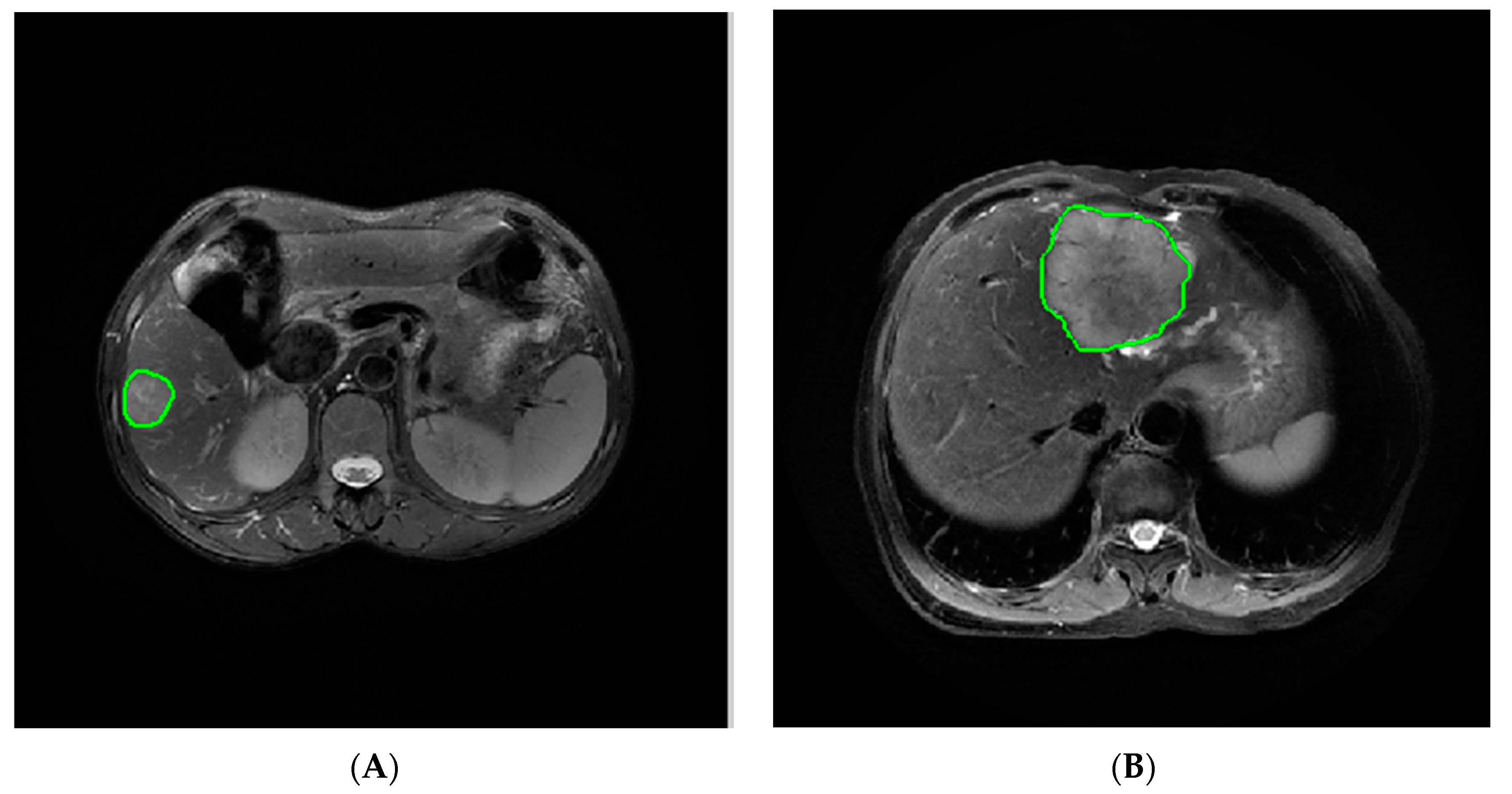
2.3. Image Segmentation and Feature Extraction
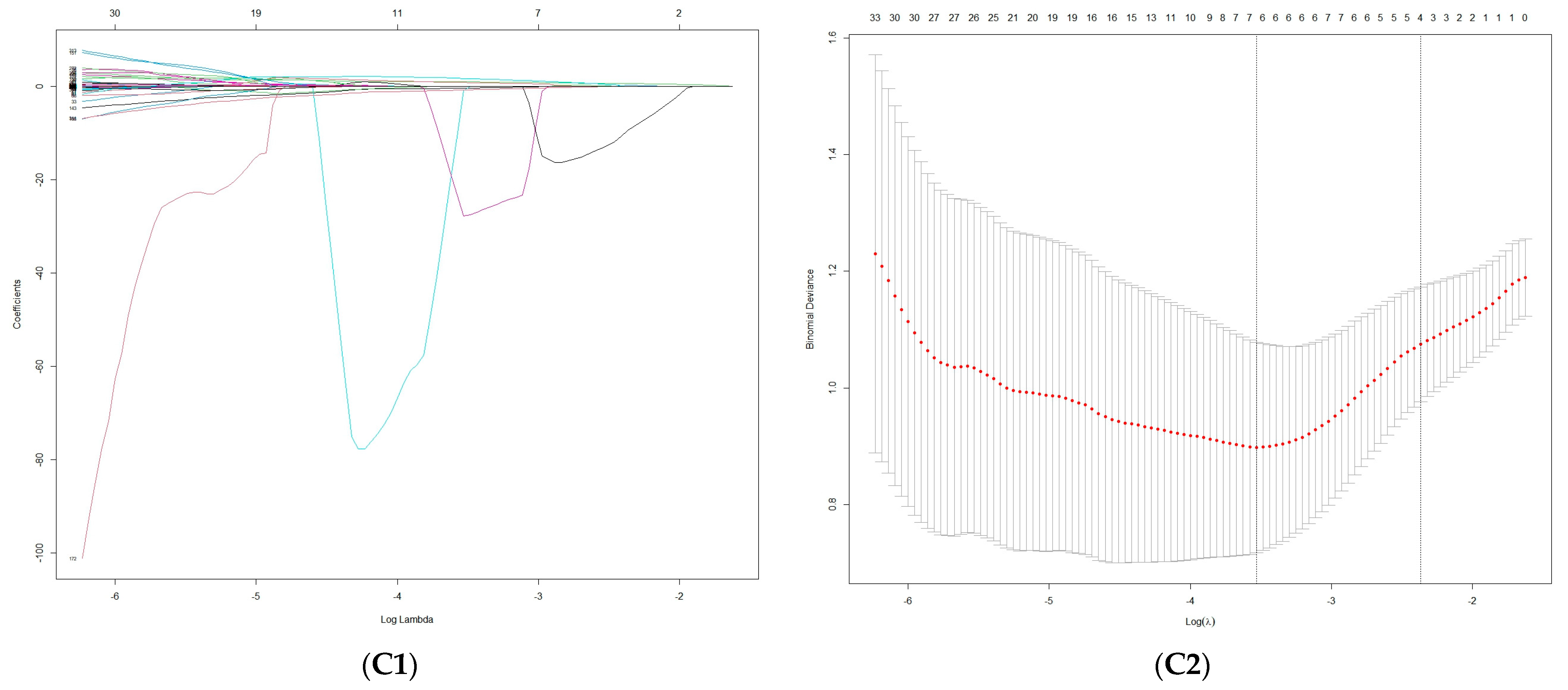
2.4. Feature Selection
2.5. Model Establishment and Evaluation
2.6. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Feature Extraction and Selection
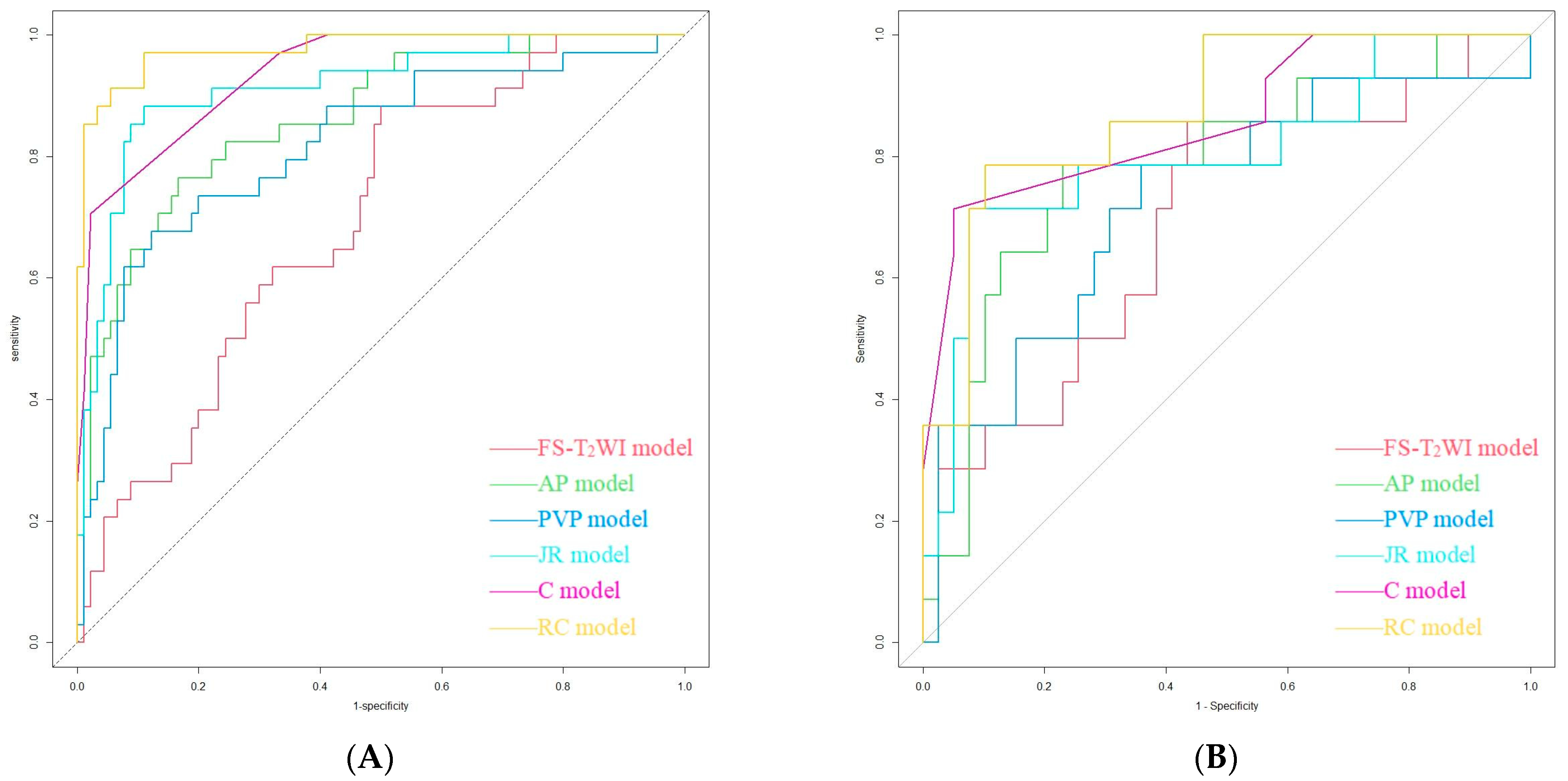
3.3. Model Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.Q.; Wang, X.Q.; Pan, C.C.; Wang, Y.; Lu, Z.M. An Efficient Nomogram for Discriminating Intrahepatic Cholangiocarcinoma From Hepatocellular Carcinoma: A Retrospective Study. Front. Oncol. 2022, 12, 833999. [Google Scholar] [CrossRef] [PubMed]
- Cheng, N.; Khoo, N.; Chung, A.Y.F.; Goh, B.K.P.; Cheow, P.C.; Chow, P.K.H.; Lee, S.Y.; Ooi, L.L.; Jeyaraj, P.R.; Kam, J.H.; et al. Pre-operative Imaging Characteristics in Histology-Proven Resected Intrahepatic Cholangiocarcinoma. World J. Surg. 2020, 44, 3862–3867. [Google Scholar] [CrossRef] [PubMed]
- Florio, A.A.; Ferlay, J.; Znaor, A.; Ruggieri, D.; Alvarez, C.S.; Laversanne, M.; Bray, F.; McGlynn, K.A.; Petrick, J.L. Global trends in intrahepatic and extrahepatic cholangiocarcinoma incidence from 1993 to 2012. Cancer 2020, 126, 2666–2678. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-Year Trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the Rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D.; ESMO Guidelines Committee. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27 (Suppl. S5), v28–v37. [Google Scholar] [CrossRef]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Gupta, A.; Dixon, E. Epidemiology and risk factors: Intrahepatic cholangiocarcinoma. Hepatobiliary Surg. Nutr. 2017, 6, 101–104. [Google Scholar] [CrossRef]
- Nart, D.; Ertan, Y.; Pala, E.E.; Zeytunlu, M.; Kilic, M.; Yilmaz, F. Intrahepatic cholangiocarcinoma arising in chronic viral hepatitis-associated cirrhosis: Two transplant cases. Transplant. Proc. 2008, 40, 3813–3815. [Google Scholar] [CrossRef]
- Kelley, R.K.; Bridgewater, J.; Gores, G.J.; Zhu, A.X. Systemic therapies for intrahepatic cholangiocarcinoma. J. Hepatol. 2020, 72, 353–363. [Google Scholar] [CrossRef]
- Banales, J.M.; Iñarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntané, J.; Muñoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology 2019, 70, 547–562. [Google Scholar] [CrossRef] [PubMed]
- Buettner, S.; van Vugt, J.L.; IJzermans, J.N.; Groot Koerkamp, B. Intrahepatic cholangiocarcinoma: Current perspectives. Onco Targets Ther. 2017, 10, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, K.; Bao, Q.; Sun, Y.; Xing, B.C. Hepatic resection provided long-term survival for patients with intermediate and advanced-stage resectable hepatocellular carcinoma. World J. Surg. Oncol. 2016, 14, 62. [Google Scholar] [CrossRef]
- Weber, S.M.; Ribero, D.; O’Reilly, E.M.; Kokudo, N.; Miyazaki, M.; Pawlik, T.M. Intrahepatic cholangiocarcinoma: Expert consensus statement. HPB 2015, 17, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Kim, Y.; Alexandrescu, S.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Clark Gamblin, T.; Miura, J.; Maithel, S.K.; Squires, M.H.; et al. Is Hepatic Resection for Large or Multifocal Intrahepatic Cholangiocarcinoma Justified? Results from a Multi-Institutional Collaboration. Ann. Surg. Oncol. 2015, 22, 2218–2225. [Google Scholar] [CrossRef]
- Bruix, J.; Reig, M.; Sherman, M. Evidence-Based Diagnosis, Staging, and Treatment of Patients With Hepatocellular Carcinoma. Gastroenterology 2016, 150, 835–853. [Google Scholar] [CrossRef]
- Moris, D.; Palta, M.; Kim, C.; Allen, P.J.; Morse, M.A.; Lidsky, M.E. Advances in the treatment of intrahepatic cholangiocarcinoma: An overview of the current and future therapeutic landscape for clinicians. CA Cancer J. Clin. 2023, 73, 198–222. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.M.; Ahn, S.J.; Kang, H.J.; Yang, H.K.; Yoon, J.H. LI-RADS Version 2017 versus Version 2018: Diagnosis of Hepatocellular Carcinoma on Gadoxetate Disodium-enhanced MRI. Radiology 2019, 292, 655–663. [Google Scholar] [CrossRef]
- Liu, X.; Ni, X.; Li, Y.; Yang, C.; Wang, Y.; Ma, C.; Zhou, C.; Lu, X. Diagnostic Performance of LI-RADS Version 2018 for Primary Liver Cancer in Patients With Liver Cirrhosis on Enhanced MRI. Front. Oncol. 2022, 12, 934045. [Google Scholar] [CrossRef]
- Feng, M.; Pan, Y.; Kong, R.; Shu, S. Therapy of Primary Liver Cancer. Innovation 2020, 1, 100032. [Google Scholar] [CrossRef]
- Huang, D.; Lin, Q.; Song, J.; Xu, B. Prognostic Value of Pretreatment Serum CA199 in Patients with Locally Advanced Rectal Cancer Treated with CRT Followed by TME with Normal Pretreatment Carcinoembryonic Antigen Levels. Dig. Surg. 2021, 38, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Qi, F.; Zhou, A.; Yan, L.; Yuan, X.; Wang, D.; Chang, R.; Zhang, Y.; Shi, F.; Han, X.; Hou, J.; et al. The diagnostic value of PIVKA-II, AFP, AFP-L3, CEA, and their combinations in primary and metastatic hepatocellular carcinoma. J. Clin. Lab. Anal. 2020, 34, e23158. [Google Scholar] [CrossRef] [PubMed]
- Afshar, M.; Fletcher, P.; Bardoli, A.D.; Ma, Y.T.; Punia, P. Non-secretion of AFP and neutrophil lymphocyte ratio as predictors for survival in hepatocellular carcinoma patients treated with sorafenib: A large UK cohort. Oncotarget 2018, 9, 16988–16995. [Google Scholar] [CrossRef] [PubMed]
- Teng, D.; Wu, K.; Sun, Y.; Zhang, M.; Wang, D.; Wu, J.; Yin, T.; Gong, W.; Ding, Y.; Xiao, W.; et al. Significant increased CA199 levels in acute pancreatitis patients predicts the presence of pancreatic cancer. Oncotarget 2018, 9, 12745–12753. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Lafaro, K.J.; Cosgrove, D.; Geschwind, J.F.; Kamel, I.; Herman, J.M.; Pawlik, T.M. Multidisciplinary Care of Patients with Intrahepatic Cholangiocarcinoma: Updates in Management. Gastroenterol. Res. Pract. 2015, 2015, 860861. [Google Scholar] [CrossRef]
- Hennedige, T.P.; Neo, W.T.; Venkatesh, S.K. Imaging of malignancies of the biliary tract—An update. Cancer Imaging 2014, 14, 14. [Google Scholar] [CrossRef]
- European Association for Study of Liver; European Organisation for Research and Treatment of Cancer. European Organisation For Research And Treatment Of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef]
- Li, R.; Cai, P.; Ma, K.S.; Ding, S.Y.; Guo, D.Y.; Yan, X.C. Dynamic enhancement patterns of intrahepatic cholangiocarcinoma in cirrhosis on contrast-enhanced computed tomography: Risk of misdiagnosis as hepatocellular carcinoma. Sci. Rep. 2016, 6, 26772. [Google Scholar] [CrossRef]
- Huang, B.; Wu, L.; Lu, X.Y.; Xu, F.; Liu, C.F.; Shen, W.F.; Jia, N.Y.; Cheng, H.Y.; Yang, Y.F.; Shen, F. Small Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma in Cirrhotic Livers May Share Similar Enhancement Patterns at Multiphase Dynamic MR Imaging. Radiology 2016, 281, 150–157. [Google Scholar] [CrossRef]
- Galassi, M.; Iavarone, M.; Rossi, S.; Bota, S.; Vavassori, S.; Rosa, L.; Leoni, S.; Venerandi, L.; Marinelli, S.; Sangiovanni, A.; et al. Patterns of appearance and risk of misdiagnosis of intrahepatic cholangiocarcinoma in cirrhosis at contrast enhanced ultrasound. Liver Int. 2013, 33, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Iavarone, M.; Piscaglia, F.; Vavassori, S.; Galassi, M.; Sangiovanni, A.; Venerandi, L.; Forzenigo, L.V.; Golfieri, R.; Bolondi, L.; Colombo, M. Contrast enhanced CT-scan to diagnose intrahepatic cholangiocarcinoma in patients with cirrhosis. J. Hepatol. 2013, 58, 1188–1193. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, J.M.; Han, J.K.; Kim, K.H.; Lee, J.Y.; Choi, B.I. Peripheral mass-forming cholangiocarcinoma in cirrhotic liver. AJR Am. J. Roentgenol. 2007, 189, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.F.; Aguirre, D.A.; Kased, N.; Emery, S.C.; Peterson, M.R.; Sirlin, C.B. Cirrhosis-associated hepatocellular nodules: Correlation of histopathologic and MR imaging features. Radiographics 2008, 28, 747–769. [Google Scholar] [CrossRef]
- Choi, S.Y.; Kim, Y.K.; Min, J.H.; Kang, T.W.; Jeong, W.K.; Ahn, S.; Won, H. Added value of ancillary imaging features for differentiating scirrhous hepatocellular carcinoma from intrahepatic cholangiocarcinoma on gadoxetic acid-enhanced MR imaging. Eur. Radiol. 2018, 28, 2549–2560. [Google Scholar] [CrossRef]
- Chong, Y.S.; Kim, Y.K.; Lee, M.W.; Kim, S.H.; Lee, W.J.; Rhim, H.C.; Lee, S.J. Differentiating mass-forming intrahepatic cholangiocarcinoma from atypical hepatocellular carcinoma using gadoxetic acid-enhanced MRI. Clin. Radiol. 2012, 67, 766–773. [Google Scholar] [CrossRef]
- Potretzke, T.A.; Tan, B.R.; Doyle, M.B.; Brunt, E.M.; Heiken, J.P.; Fowler, K.J. Imaging Features of Biphenotypic Primary Liver Carcinoma (Hepatocholangiocarcinoma) and the Potential to Mimic Hepatocellular Carcinoma: LI-RADS Analysis of CT and MRI Features in 61 Cases. AJR Am. J. Roentgenol. 2016, 207, 25–31. [Google Scholar] [CrossRef]
- Losic, B.; Craig, A.J.; Villacorta-Martin, C.; Martins-Filho, S.N.; Akers, N.; Chen, X.; Ahsen, M.E.; von Felden, J.; Labgaa, I.; D’Avola, D.; et al. Intratumoral heterogeneity and clonal evolution in liver cancer. Nat. Commun. 2020, 11, 291. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef]
- Tao, Y.Y.; Shi, Y.; Gong, X.Q.; Li, L.; Li, Z.M.; Yang, L.; Zhang, X.M. Radiomic Analysis Based on Magnetic Resonance Imaging for Predicting PD-L2 Expression in Hepatocellular Carcinoma. Cancers 2023, 15, 365. [Google Scholar] [CrossRef]
- Mao, Q.; Zhou, M.T.; Zhao, Z.P.; Liu, N.; Yang, L.; Zhang, X.M. Role of radiomics in the diagnosis and treatment of gastrointestinal cancer. World J. Gastroenterol. 2022, 28, 6002–6016. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Liu, X.; Liu, P.; Xu, D.; Li, Z.; Lin, H.; Xie, A. The Application Value of MRI T2∗WI Radiomics Nomogram in Discriminating Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma. Comput. Math. Methods Med. 2022, 2022, 7099476. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhou, G.; Zhang, J.; Xu, C.; Zhu, F.; Xu, P. DCE-MRI based radiomics nomogram for preoperatively differentiating combined hepatocellular-cholangiocarcinoma from mass-forming intrahepatic cholangiocarcinoma. Eur. Radiol. 2022, 32, 5004–5015. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Khalvati, F.; Namdar, K.; Fischer, S.; Lewis, S.; Taouli, B.; Haider, M.A.; Jhaveri, K.S. Can machine learning radiomics provide pre-operative differentiation of combined hepatocellular cholangiocarcinoma from hepatocellular carcinoma and cholangiocarcinoma to inform optimal treatment planning? Eur. Radiol. 2021, 31, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Gu, D.; Wei, J.; Ding, Y.; Yang, L.; Zhu, K.; Luo, R.; Rao, S.X.; Tian, J.; Zeng, M. A radiomics-based biomarker for cytokeratin 19 status of hepatocellular carcinoma with gadoxetic acid-enhanced MRI. Eur. Radiol. 2020, 30, 3004–3014. [Google Scholar] [CrossRef] [PubMed]
- Mokrane, F.Z.; Lu, L.; Vavasseur, A.; Otal, P.; Peron, J.M.; Luk, L.; Yang, H.; Ammari, S.; Saenger, Y.; Rousseau, H.; et al. Radiomics machine-learning signature for diagnosis of hepatocellular carcinoma in cirrhotic patients with indeterminate liver nodules. Eur. Radiol. 2020, 30, 558–570. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.K.; Jamshidi, N.; Felker, E.R.; Raman, S.S.; Lu, D.S. Radiomics and radiogenomics of primary liver cancers. Clin. Mol. Hepatol. 2019, 25, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Liu, X.; Chen, J.; Wei, Y.; Lee, J.M.; Cao, L.; Wu, Y.; Duan, T.; Li, X.; Ma, L.; et al. Man or machine? Prospective comparison of the version 2018 EASL, LI-RADS criteria and a radiomics model to diagnose hepatocellular carcinoma. Cancer Imaging 2019, 19, 84. [Google Scholar] [CrossRef]
- Hectors, S.J.; Lewis, S.; Besa, C.; King, M.J.; Said, D.; Putra, J.; Ward, S.; Higashi, T.; Thung, S.; Yao, S.; et al. MRI radiomics features predict immuno-oncological characteristics of hepatocellular carcinoma. Eur. Radiol. 2020, 30, 3759–3769. [Google Scholar] [CrossRef]
- Chen, S.; Feng, S.; Wei, J.; Liu, F.; Li, B.; Li, X.; Hou, Y.; Gu, D.; Tang, M.; Xiao, H.; et al. Pretreatment prediction of immunoscore in hepatocellular cancer: A radiomics-based clinical model based on Gd-EOB-DTPA-enhanced MRI imaging. Eur. Radiol. 2019, 29, 4177–4187. [Google Scholar] [CrossRef]
- Yang, L.; Gu, D.; Wei, J.; Yang, C.; Rao, S.; Wang, W.; Chen, C.; Ding, Y.; Tian, J.; Zeng, M. A Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion in Hepatocellular Carcinoma. Liver Cancer 2019, 8, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Nebbia, G.; Zhang, Q.; Arefan, D.; Zhao, X.; Wu, S. Pre-operative Microvascular Invasion Prediction Using Multi-parametric Liver MRI Radiomics. J. Digit. Imaging 2020, 33, 1376–1386. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.W.; Zhu, F.P.; Xu, Q.; Wang, K.; Wu, M.Y.; Tang, W.W.; Li, X.C.; Wang, X.H. Machine-learning analysis of contrast-enhanced CT radiomics predicts recurrence of hepatocellular carcinoma after resection: A multi-institutional study. EBioMedicine 2019, 50, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Long, L.H.; Cui, Y.; Jia, A.Y.; Zhu, X.G.; Wang, H.Z.; Wang, Z.; Zhan, C.M.; Wang, Z.H.; Wang, W.H. MRI-based radiomics model for preoperative prediction of 5-year survival in patients with hepatocellular carcinoma. Br. J. Cancer 2020, 122, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Lubner, M.G.; Smith, A.D.; Sandrasegaran, K.; Sahani, D.V.; Pickhardt, P.J. CT Texture Analysis: Definitions, Applications, Biologic Correlates, and Challenges. Radiographics 2017, 37, 1483–1503. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; Jong, E.E.C.; Timmeren, J.T.; Sanduleanu, S.; Larue, R.T.H.L.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Surveillance group; Diagnosis group; Staging group; Surgery group; Local ablation group; TACE/TARE/HAI group; Target therapy/systemic therapy group; Radiotherapy group; Prevention group; Drafting group. Management consensus guideline for hepatocellular carcinoma: 2016 updated by the Taiwan Liver Cancer Association and the Gastroenterological Society of Taiwan. J. Formos. Med. Assoc. 2018, 117, 381–403. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, J.M.; Lee, J.S.; Lee, H.Y.; Park, B.H.; Kim, Y.H.; Han, J.K.; Choi, B.I. Hepatocellular carcinoma: Diagnostic performance of multidetector CT and MR imaging-a systematic review and meta-analysis. Radiology 2015, 275, 97–109. [Google Scholar] [CrossRef]
- Liu, X.; Jiang, H.; Chen, J.; Zhou, Y.; Huang, Z.; Song, B. Gadoxetic acid disodium-enhanced magnetic resonance imaging outperformed multidetector computed tomography in diagnosing small hepatocellular carcinoma: A meta-analysis. Liver Transpl. 2017, 23, 1505–1518. [Google Scholar] [CrossRef]
- Choi, S.H.; Lee, S.S.; Kim, S.Y.; Park, H.P.; Park, S.H.; Kim, K.M.; Hong, S.M.; Yu, E.; Lee, M.G. Intrahepatic Cholangiocarcinoma in Patients with Cirrhosis: Differentiation from Hepatocellular Carcinoma by Using Gadoxetic Acid-enhanced MR Imaging and Dynamic CT. Radiology 2017, 282, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Gao, F.; Zheng, D.; Huang, Z.; Wang, M.; Hu, F.; Chen, C.; Duan, T.; Chen, J.; Cao, L.; et al. Intrahepatic cholangiocarcinoma in the setting of HBV-related cirrhosis: Differentiation with hepatocellular carcinoma by using Intravoxel incoherent motion diffusion-weighted MR imaging. Oncotarget 2018, 9, 7975–7983. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.; Peti, S.; Hectors, S.J.; King, M.; Rosen, A.; Kamath, A.; Putra, J.; Thung, S.; Taouli, B. Volumetric quantitative histogram analysis using diffusion-weighted magnetic resonance imaging to differentiate HCC from other primary liver cancers. Abdom. Radiol. 2019, 44, 912–922. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Lü, L.; Lin, P.; Chen, Z.; Quan, Z.; Tang, Z. Multiple cellular origins and molecular evolution of intrahepatic cholangiocarcinoma. Cancer Lett. 2016, 379, 253–261. [Google Scholar] [CrossRef]
- Peng, J.; Zheng, J.; Yang, C.; Wang, R.; Zhou, Y.; Tao, Y.Y.; Gong, X.Q.; Wang, W.C.; Zhang, X.M.; Yang, L. Intravoxel incoherent motion diffusion-weighted imaging to differentiate hepatocellular carcinoma from intrahepatic cholangiocarcinoma. Sci. Rep. 2020, 10, 7717. [Google Scholar] [CrossRef]
- Choi, I.Y.; Lee, S.S.; Sung, Y.S.; Cheong, H.; Lee, H.; Byun, J.B.; Kim, S.Y.; Lee, S.J.; Shin, Y.M.; Lee, M.G. Intravoxel incoherent motion diffusion-weighted imaging for characterizing focal hepatic lesions: Correlation with lesion enhancement. J. Magn. Reson. Imaging 2017, 45, 1589–1598. [Google Scholar] [CrossRef]
- Shao, S.; Shan, Q.; Zheng, N.; Wang, B.; Wang, J. Role of Intravoxel Incoherent Motion in Discriminating Hepatitis B Virus-Related Intrahepatic Mass-Forming Cholangiocarcinoma from Hepatocellular Carcinoma Based on Liver Imaging Reporting and Data System v2018. Cancer Biother. Radiopharm. 2019, 34, 511–518. [Google Scholar] [CrossRef]
- Çelebi, F.; Yaghouti, K.; Cindil, E.; Dogusoy, G.B.; Tokat, Y.; Balcı, C. The Role of 18F-FDG PET/MRI in the Assessment of Primary Intrahepatic Neoplasms. Acad. Radiol. 2021, 28, 189–198. [Google Scholar] [CrossRef]
- Wang, X.; Wang, S.; Yin, X.; Zheng, Y. MRI-based radiomics distinguish different pathological types of hepatocellular carcinoma. Comput. Biol. Med. 2022, 141, 105058. [Google Scholar] [CrossRef]
- Han, X.; Sun, M.; Wang, M.; Fan, R.; Chen, D.; Xie, L.; Liu, A. The enhanced T2 star weighted angiography (ESWAN) value for differentiating borderline from malignant epithelial ovarian tumors. Eur. J. Radiol. 2019, 118, 187–193. [Google Scholar] [CrossRef]
- Gong, X.Q.; Tao, Y.Y.; Wu, Y.K.; Liu, N.; Yu, X.; Wang, R.; Zheng, J.; Liu, N.; Huang, X.H.; Li, J.D.; et al. Progress of MRI Radiomics in Hepatocellular Carcinoma. Front. Oncol. 2021, 11, 698373. [Google Scholar] [CrossRef] [PubMed]
- Greiner, M.; Pfeiffer, D.; Smith, R.D. Principles and practical application of the receiver-operating characteristic analysis for diagnostic tests. Prev. Vet. Med. 2000, 45, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Zeng, D.; Zhou, R.; Yu, Y.; Luo, Y.; Zhang, J.; Sun, H.; Bin, J.; Liao, Y.; Rao, J.; Zhang, Y.; et al. Gene expression profiles for a prognostic immunoscore in gastric cancer. Br. J. Surg. 2018, 105, 1338–1348. [Google Scholar] [CrossRef]
- Fahmy, D.; Alksas, A.; Elnakib, A.; Mahmoud, A.; Kandil, H.; Khalil, A.; Ghazal, M.; Bogaert, E.; Contractor, S.; El-Baz, A. The Role of Radiomics and AI Technologies in the Segmentation, Detection, and Management of Hepatocellular Carcinoma. Cancers 2022, 14, 6123. [Google Scholar] [CrossRef]
- Jiang, C.; Zhao, L.; Xin, B.; Ma, G.; Wang, X.; Song, S. 18F-FDG PET/CT radiomic analysis for classifying and predicting microvascular invasion in hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Quant. Imaging Med. Surg. 2022, 12, 4135–4150. [Google Scholar] [CrossRef]
- Xu, X.; Mao, Y.; Tang, Y.; Liu, Y.; Xue, C.; Yue, Q.; Liu, Q.; Wang, J.; Yin, Y. Classification of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma Based on Radiomic Analysis. Comput. Math. Methods Med. 2022, 2022, 5334095. [Google Scholar] [CrossRef]
- Ren, S.; Li, Q.; Liu, S.; Qi, Q.; Duan, S.; Mao, B.; Li, X.; Wu, Y.; Zhang, L. Clinical Value of Machine Learning-Based Ultrasomics in Preoperative Differentiation Between Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: A Multicenter Study. Front. Oncol. 2021, 11, 749137. [Google Scholar] [CrossRef]
- Peng, Y.; Lin, P.; Wu, L.; Wan, D.; Zhao, Y.; Liang, L.; Ma, X.; Qin, H.; Liu, Y.; Li, X.; et al. Ultrasound-Based Radiomics Analysis for Preoperatively Predicting Different Histopathological Subtypes of Primary Liver Cancer. Front. Oncol. 2020, 10, 1646. [Google Scholar] [CrossRef]
- Zhang, J.; Huang, Z.; Cao, L.; Zhang, Z.; Wei, Y.; Zhang, X.; Song, B. Differentiation combined hepatocellular and cholangiocarcinoma from intrahepatic cholangiocarcinoma based on radiomics machine learning. Ann. Transl. Med. 2020, 8, 119. [Google Scholar] [CrossRef]
- Gao, R.; Zhao, S.; Aishanjiang, K.; Cai, H.; Wei, T.; Zhang, Y.; Liu, Z.; Zhou, J.; Han, B.; Wang, J.; et al. Deep learning for differential diagnosis of malignant hepatic tumors based on multi-phase contrast-enhanced CT and clinical data. J. Hematol. Oncol. 2021, 14, 154. [Google Scholar] [CrossRef]
- Just, N. Improving tumour heterogeneity MRI assessment with histograms. Br. J. Cancer 2014, 111, 2205–2213. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.J.; Chen, W.X.; Wu, D.S.; Zhang, W.Y.; Zheng, L.R. Differentiation of mass-forming intrahepatic cholangiocarcinoma from poorly differentiated hepatocellular carcinoma: Based on the multivariate analysis of contrast-enhanced computed tomography findings. Abdom. Radiol. 2016, 41, 978–989. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | TR/TE (ms) | FA (°) | Matrix (mm2) | FOV (mm2) | ST (mm) |
|---|---|---|---|---|---|
| BH Ax LAVA-Flex | 4/2 | 12 | 260 × 192 | 320 × 320–360 × 360 | 2.6 |
| RTr Ax fs T2WI | 2609/97 | 110 | 384 × 384 | 320 × 320–380 × 380 | 5 |
| BH Ax LAVA-Flex+C | 4/2 | 12 | 224 × 192 | 320 × 320–360 × 360 | 5 |
| Parameter | Training Cohort (n = 124) | Validation Cohort (n = 53) | p Value |
|---|---|---|---|
| Sex | 0.565 | ||
| Male | 94 | 38 | |
| Female | 30 | 15 | |
| Age | 0.751 | ||
| ≤60 | 78 | 32 | |
| >60 | 46 | 21 | |
| Satellite nodules | 0.618 | ||
| Yes | 47 | 18 | |
| No | 77 | 35 | |
| Diameter | 0.076 | ||
| ≤5 | 41 | 25 | |
| >5 | 83 | 28 | |
| Ascites | 0.514 | ||
| Yes | 36 | 18 | |
| No | 88 | 35 | |
| Hemorrhagic necrosis | 0.162 | ||
| Yes | 86 | 31 | |
| No | 38 | 22 | |
| Pseudocapsule | 0.975 | ||
| Yes | 26 | 11 | |
| No | 98 | 42 | |
| Extrahepatic metastases | 0.234 | ||
| Yes | 23 | 6 | |
| No | 101 | 47 | |
| Portal vein tumor thrombus | 0.445 | ||
| Yes | 35 | 18 | |
| No | 89 | 35 | |
| Cirrhosis | 0.533 | ||
| Yes | 83 | 38 | |
| No | 41 | 15 | |
| Hepatitis B or C | 0.891 | ||
| Yes | 90 | 39 | |
| No | 34 | 14 | |
| AFP (ng/mL) | 0.259 | ||
| <20 | 54 | 30 | |
| 20~400 | 21 | 8 | |
| >400 | 49 | 15 | |
| DCP (mAU/mL) | 0.905 | ||
| ≤27.8 | 11 | 5 | |
| >27.8 | 113 | 48 | |
| CA19-9 (U/mL) | 0.244 | ||
| ≤37 | 68 | 24 | |
| >37 | 56 | 29 | |
| CEA (µg/L) | 0.601 | ||
| ≤5 | 80 | 32 | |
| >5 | 44 | 21 | |
| Histologic result | 0.891 | ||
| HCC | 90 | 39 | |
| ICC | 34 | 14 |
| Cohort | Feature Type | Feature Name |
|---|---|---|
| FS-T2WI | Shape features (n = 1) | Roundness |
| Arterial phase | Texture features (n = 3) | |
| GLCM (n = 1) | 45-7InverseDiffMomentNorm | |
| GLRLM (n = 2) | 0LongRunEmphasis | |
| 90ShortRunLowGrayLevelEmpha | ||
| Intensity histogram features (n = 1) | InterQuartileRange | |
| Shape features (n = 2) | Mass | |
| Roundness | ||
| Portal venous phase | Texture features (n = 2) | |
| GLCM (n = 2) | 90-1Contrast | |
| 45-7InverseDiffMomentNorm | ||
| Intensity histogram features (n = 2) | InterQuartileRange | |
| MeanAbsoluteDeviation |
| Cohort | Model | AUC | Sen | Spe | PPV | NPV | ACC | F1 Score |
|---|---|---|---|---|---|---|---|---|
| Training | FS-T2WI model | 0.693 | 0.147 | 0.956 | 0.556 | 0.748 | 0.734 | 0.233 |
| AP model | 0.863 | 0.588 | 0.933 | 0.769 | 0.857 | 0.839 | 0.667 | |
| PVP model | 0.818 | 0.588 | 0.922 | 0.741 | 0.856 | 0.831 | 0.656 | |
| JR model | 0.914 | 0.706 | 0.922 | 0.774 | 0.892 | 0.863 | 0.738 | |
| C model | 0.936 | 0.706 | 0.978 | 0.923 | 0.898 | 0.903 | 0.800 | |
| RC model | 0.977 | 0.853 | 0.978 | 0.935 | 0.946 | 0.944 | 0.892 | |
| Validation | FS-T2WI model | 0.690 | 0.071 | 0.974 | 0.5 | 0.745 | 0.736 | 0.125 |
| AP model | 0.784 | 0.571 | 0.897 | 0.667 | 0.854 | 0.811 | 0.615 | |
| PVP model | 0.727 | 0.357 | 0.897 | 0.556 | 0.795 | 0.756 | 0.435 | |
| JR model | 0.802 | 0.571 | 0.923 | 0.727 | 0.857 | 0.83 | 0.640 | |
| C model | 0.860 | 0.714 | 0.949 | 0.833 | 0.902 | 0.887 | 0.769 | |
| RC model | 0.877 | 0.714 | 0.897 | 0.714 | 0.897 | 0.849 | 0.714 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, N.; Wu, Y.; Tao, Y.; Zheng, J.; Huang, X.; Yang, L.; Zhang, X. Differentiation of Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma through MRI Radiomics. Cancers 2023, 15, 5373. https://doi.org/10.3390/cancers15225373
Liu N, Wu Y, Tao Y, Zheng J, Huang X, Yang L, Zhang X. Differentiation of Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma through MRI Radiomics. Cancers. 2023; 15(22):5373. https://doi.org/10.3390/cancers15225373
Chicago/Turabian StyleLiu, Ning, Yaokun Wu, Yunyun Tao, Jing Zheng, Xiaohua Huang, Lin Yang, and Xiaoming Zhang. 2023. "Differentiation of Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma through MRI Radiomics" Cancers 15, no. 22: 5373. https://doi.org/10.3390/cancers15225373
APA StyleLiu, N., Wu, Y., Tao, Y., Zheng, J., Huang, X., Yang, L., & Zhang, X. (2023). Differentiation of Hepatocellular Carcinoma from Intrahepatic Cholangiocarcinoma through MRI Radiomics. Cancers, 15(22), 5373. https://doi.org/10.3390/cancers15225373