

Online Adaptive MRI-Guided Stereotactic Body Radiotherapy for Pancreatic and Other Intra-Abdominal Cancers

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
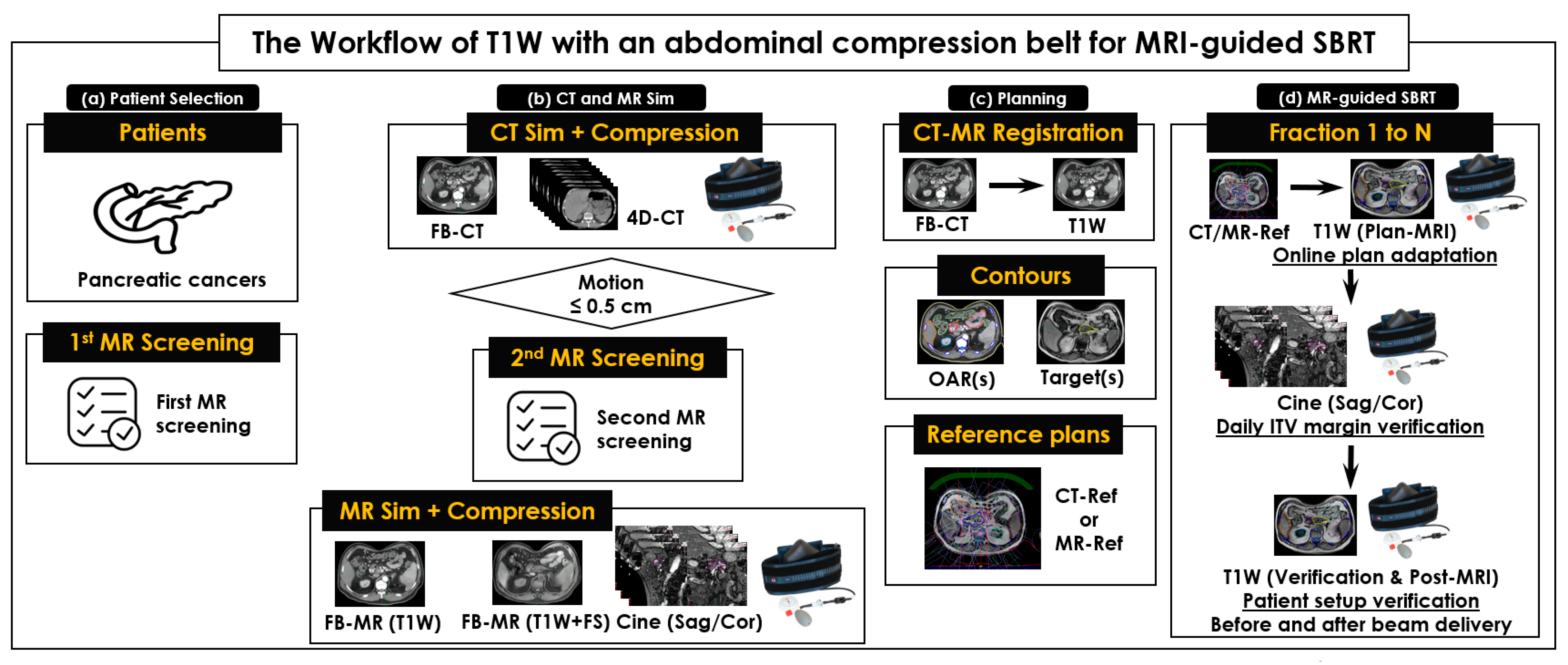
2.1. The Workflow of CT and MRI Simulations, and MRI-Guided SBRT
2.2. Patients
2.3. CT and MRI Simulations with Immobilization Devices
2.4. SBRT Planning
2.5. Online Adaptive MRI-Guided SBRT
2.6. Statistical Analysis of Plan Quality
3. Results
3.1. Patients
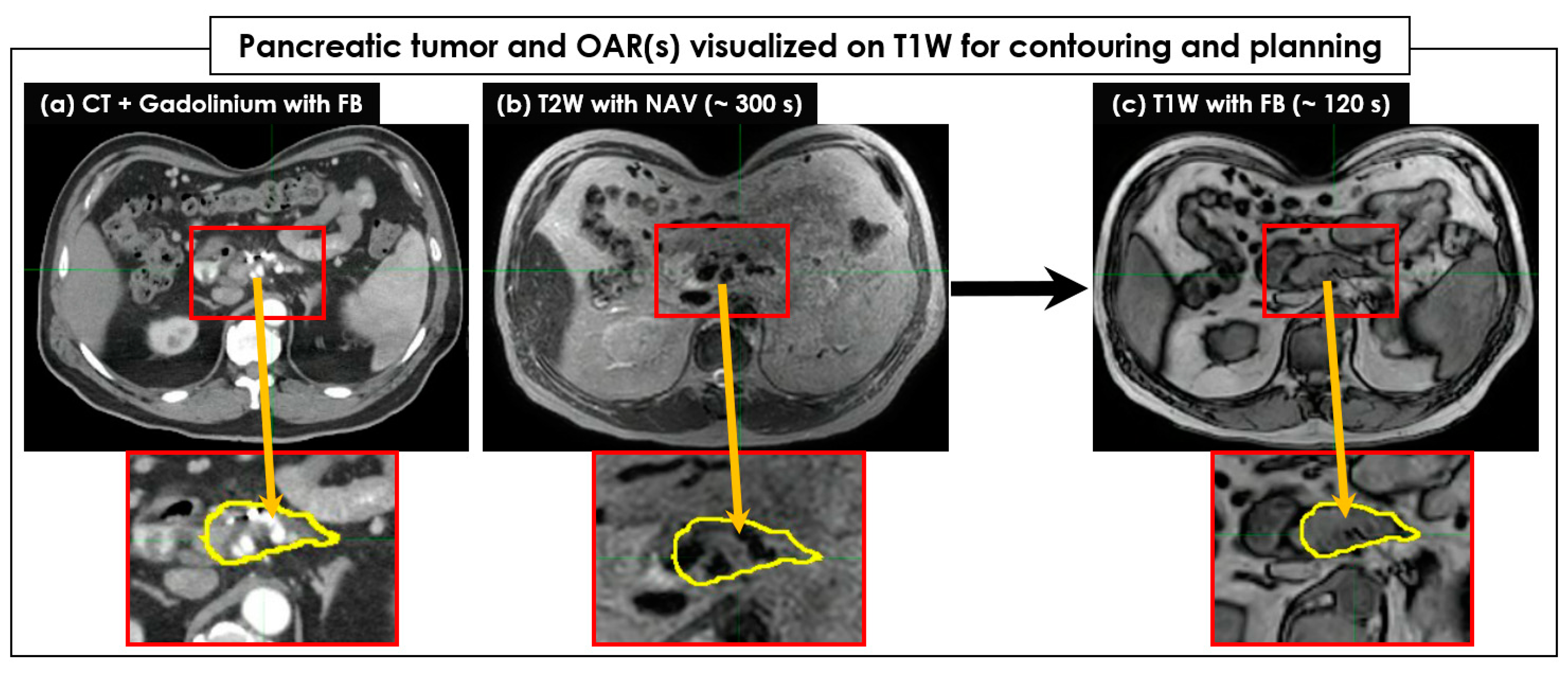
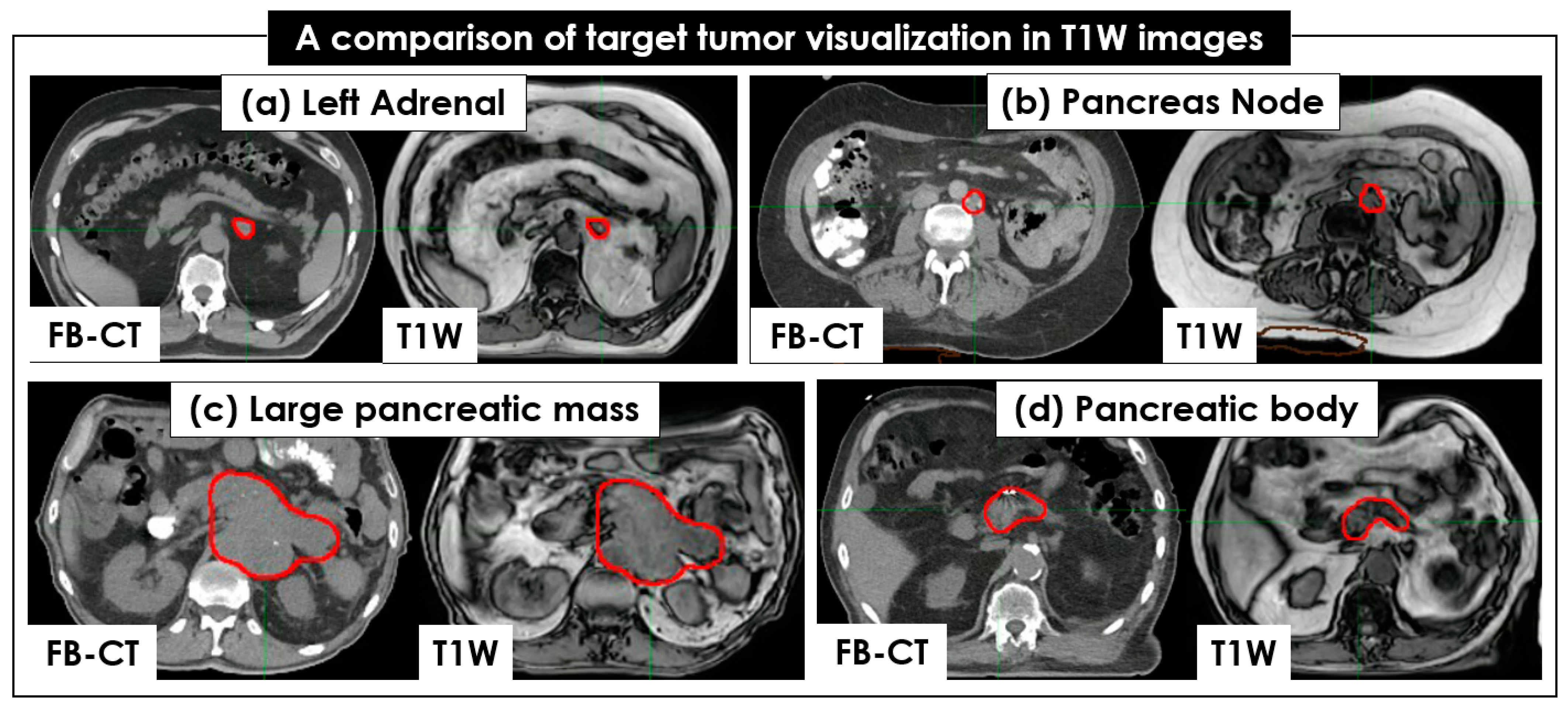
3.2. CT and MR Image Sets and Target Contouring
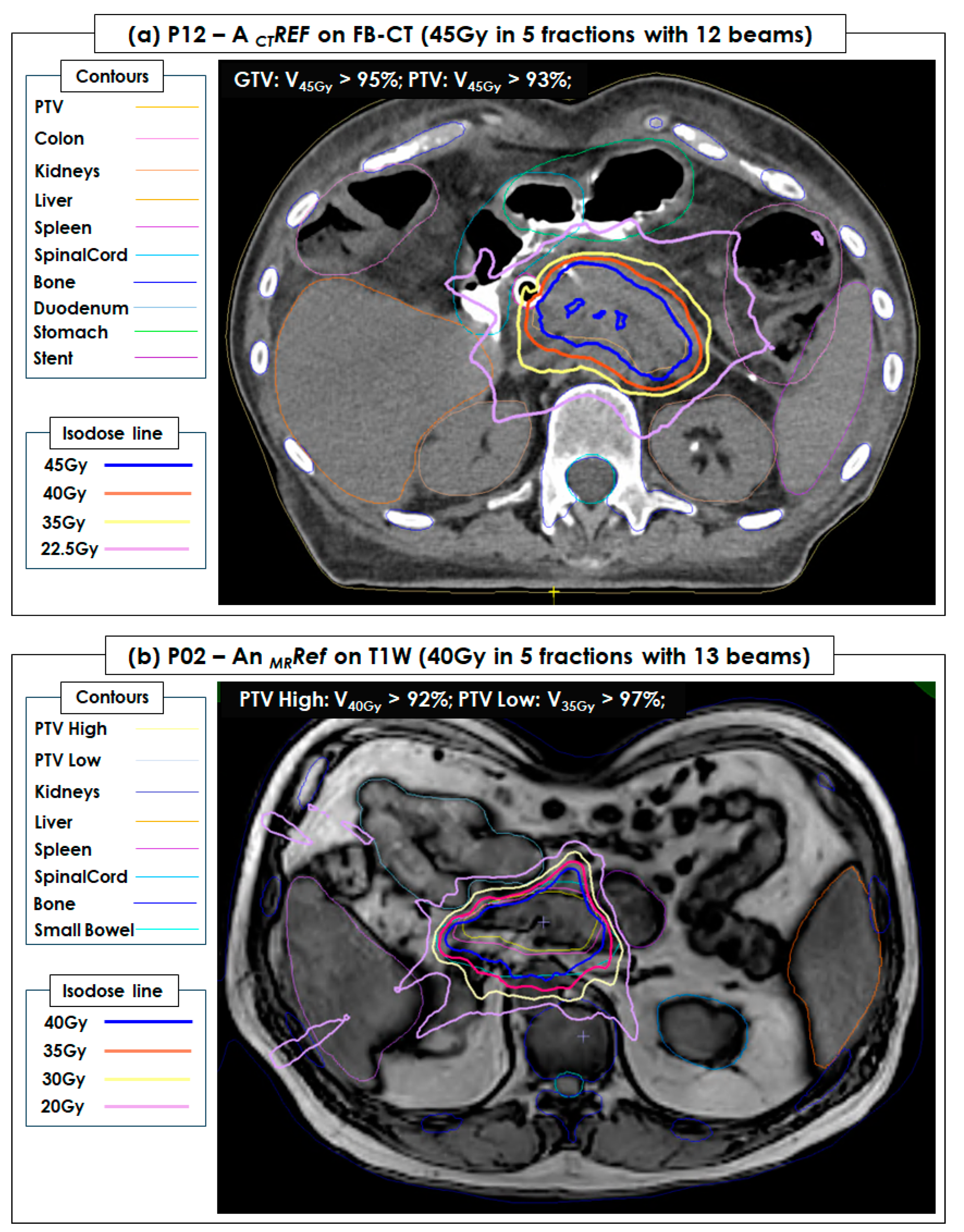
3.3. Plan Quality of Reference SBRT Plans
3.4. Online Adaptive MRI-Guided SBRT
3.5. Overall Time-Consumption of Online MRI-Guided SBRT in 10 Steps
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mutic, S.; Dempsey, J.F. The ViewRay System: Magnetic Resonance–Guided and Controlled Radiotherapy. Semin. Radiat. Oncol 2014, 24, 196–199. [Google Scholar] [CrossRef]
- Lagendijk, J.J.W.; Raaymakers, B.W.; van Vulpen, M. The Magnetic Resonance Imaging–Linac System. Semin. Radiat. Oncol. 2014, 24, 207–209. [Google Scholar] [CrossRef]
- Fallone, B.G. The Rotating Biplanar Linac–Magnetic Resonance Imaging System. Semin. Radiat. Oncol. 2014, 24, 200–202. [Google Scholar] [CrossRef]
- Keall, P.J.; Barton, M.; Crozier, S. The Australian Magnetic Resonance Imaging–Linac Program. Semin. Radiat. Oncol. 2014, 24, 203–206. [Google Scholar] [CrossRef]
- Heerkens, H.D.; van Vulpen, M.; Erickson, B.; Reerink, O.; Intven, M.P.; van den Berg, C.A.; Meijer, G.J. MRI guided stereotactic radiotherapy for locally advanced pancreatic cancer. Br. J. Radiol. 2018, 91, 20170563. [Google Scholar] [CrossRef]
- Klüter, S. Technical design and concept of a 0.35 T MR-Linac. Clin. Transl. Radiat. Oncol. 2019, 18, 98–101. [Google Scholar] [CrossRef]
- Winkel, D.; Bol, G.H.; Kroon, P.S.; van Asselen, B.; Hackett, S.S.; Werensteijn-Honingh, A.M.; Intven, M.P.; Eppinga, W.S.; Tijssen, R.H.; Kerkmeijer, L.G.; et al. Adaptive radiotherapy: The Elekta Unity MR-linac concept. Clin. Transl. Radiat. Oncol. 2019, 18, 54–59. [Google Scholar] [CrossRef]
- Hall, W.A.; Small, C.; Paulson, E.; Koay, E.J.; Crane, C.; Intven, M.; Daamen, L.A.; Meijer, G.J.; Heerkens, H.D.; Bassetti, M.; et al. Magnetic Resonance Guided Radiation Therapy for Pancreatic Adenocarcinoma, Advantages, Challenges, Current Approaches, and Future Directions. Front. Oncol. 2021, 11, 628155. [Google Scholar] [CrossRef]
- Rodriguez, L.L.; Kotecha, R.; Tom, M.C.; Chuong, M.D.; Contreras, J.A.; Romaguera, T.; Alvarez, D.; McCulloch, J.; Herrera, R.; Hernandez, R.J.; et al. CT-guided versus MR-guided radiotherapy: Impact on gastrointestinal sparing in adrenal stereotactic body radiotherapy. Radiother. Oncol. 2022, 166, 101–109. [Google Scholar] [CrossRef]
- Hoegen, P.; Katsigiannopulos, E.; Buchele, C.; Regnery, S.; Weykamp, F.; Sandrini, E.; Ristau, J.; Liermann, J.; Meixner, E.; Forster, T.; et al. Stereotactic magnetic resonance-guided online adaptive radiotherapy of adrenal metastases combines high ablative doses with optimized sparing of organs at risk. Clin. Transl. Radiat. Oncol. 2023, 39, 100567. [Google Scholar] [CrossRef]
- Rammohan, N.; Randall, J.W.; Yadav, P. History of Technological Advancements towards MR-Linac: The Future of Image-Guided Radiotherapy. JCM 2022, 11, 4730. [Google Scholar] [CrossRef] [PubMed]
- Luterstein, E.; Cao, M.; Lamb, J.; Raldow, A.C.; Low, D.A.; Steinberg, M.L.; Lee, P. Stereotactic MRI-Guided Adaptive Radiation Therapy (SMART) for Locally Advanced Pancreatic Cancer: A Promising Approach. 2018. Available online: https://www.cureus.com/articles/10922-stereotactic-mri-guided-adaptive-radiation-therapy-smart-for-locally-advanced-pancreatic-cancer-a-promising-approach (accessed on 4 April 2023).
- Hassanzadeh, C.; Rudra, S.; Bommireddy, A.; Hawkins, W.G.; Wang-Gillam, A.; Fields, R.C.; Cai, B.; Park, J.; Green, O.; Roach, M.; et al. Ablative Five-Fraction Stereotactic Body Radiation Therapy for Inoperable Pancreatic Cancer Using Online MR-Guided Adaptation. Adv. Radiat. Oncol. 2021, 6, 100506. [Google Scholar] [CrossRef] [PubMed]
- Michalet, M.; Bordeau, K.; Cantaloube, M.; Valdenaire, S.; Debuire, P.; Simeon, S.; Portales, F.; Draghici, R.; Ychou, M.; Assenat, E.; et al. Stereotactic MR-Guided Radiotherapy for Pancreatic Tumors: Dosimetric Benefit of Adaptation and First Clinical Results in a Prospective Registry Study. Front. Oncol. 2022, 12, 842402. [Google Scholar] [CrossRef] [PubMed]
- Bordeau, K.; Michalet, M.; Keskes, A.; Valdenaire, S.; Debuire, P.; Cantaloube, M.; Cabaillé, M.; Portales, F.; Draghici, R.; Ychou, M.; et al. Stereotactic MR-Guided Adaptive Radiotherapy for Pancreatic Tumors: Updated Results of the Montpellier Prospective Registry Study. Cancers 2022, 15, 7. [Google Scholar] [CrossRef]
- Heerkens, H.; Hall, W.; Li, X.; Knechtges, P.; Dalah, E.; Paulson, E.; Berg, C.v.D.; Meijer, G.; Koay, E.; Crane, C.; et al. Recommendations for MRI-based contouring of gross tumor volume and organs at risk for radiation therapy of pancreatic cancer. Pract. Radiat. Oncol. 2017, 7, 126–136. [Google Scholar] [CrossRef]
- Hall, W.A.; Heerkens, H.D.; Paulson, E.S.; Meijer, G.J.; Kotte, A.N.; Knechtges, P.; Parikh, P.J.; Bassetti, M.F.; Lee, P.; Aitken, K.L.; et al. Pancreatic gross tumor volume contouring on computed tomography (CT) compared with magnetic resonance imaging (MRI): Results of an international contouring conference. Pract. Radiat. Oncol. 2018, 8, 107–115. [Google Scholar] [CrossRef]
- Rhee, H.; Park, M.S. The Role of Imaging in Current Treatment Strategies for Pancreatic Adenocarcinoma. Korean J. Radiol. 2021, 22, 23. [Google Scholar] [CrossRef]
- Chuong, M.D.; Bryant, J.; Mittauer, K.E.; Hall, M.; Kotecha, R.; Alvarez, D.; Romaguera, T.; Rubens, M.; Adamson, S.; Godley, A.; et al. Ablative 5-Fraction Stereotactic Magnetic Resonance–Guided Radiation Therapy With On-Table Adaptive Replanning and Elective Nodal Irradiation for Inoperable Pancreas Cancer. Pract. Radiat. Oncol. 2021, 11, 134–147. [Google Scholar] [CrossRef]
- Lens, E.; van der Horst, A.; Versteijne, E.; Bel, A.; van Tienhoven, G. Considerable pancreatic tumor motion during breath-holding. Acta Oncol. 2016, 55, 1360–1368. [Google Scholar] [CrossRef]
- Lee, D.; Greer, P.B.; Arm, J.; Keall, P.; Kim, T. Audiovisual biofeedback improves image quality and reduces scan time for respiratory-gated 3D MRI. J. Phys. Conf. Ser. 2014, 489, 012033. [Google Scholar] [CrossRef]
- Tyagi, N.; Liang, J.; Burleson, S.; Subashi, E.; Scripes, P.G.; Tringale, K.R.; Romesser, P.B.; Reyngold, M.; Crane, C.H. Feasibility of ablative stereotactic body radiation therapy of pancreas cancer patients on a 1.5 Tesla magnetic resonance-linac system using abdominal compression. Phys. Imaging Radiat Oncol. 2021, 19, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Simeonov, A.; Stanescu, T.; Dawson, L.A.; Brock, K.K.; Velec, M. MRI evaluation of normal tissue deformation and breathing motion under an abdominal compression device. J. Appl. Clin. Med. Phys. 2021, 22, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Veeraraghavan, H.; Tringale, K.; Amoateng, E.; Subashi, E.; Wu, A.J.; Crane, C.H.; Tyagi, N. Inter-and intrafraction motion assessment and accumulated dose quantification of upper gastrointestinal organs during magnetic resonance-guided ablative radiation therapy of pancreas patients. Phys. Imaging Radiat Oncol. 2022, 21, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Axford, A.; Dikaios, N.; Roberts, D.A.; Clark, C.H.; Evans, P.M. An end-to-end assessment on the accuracy of adaptive radiotherapy in an MR-linac. Phys. Med. Biol. 2021, 66, 055021. [Google Scholar] [CrossRef]
- Tirkes, T.; Menias, C.O.; Sandrasegaran, K. MR Imaging Techniques for Pancreas. Radiol. Clin. North Am. 2012, 50, 379–393. [Google Scholar] [CrossRef]
- Keall, P.J.; Mageras, G.S.; Balter, J.M.; Emery, R.S.; Forster, K.M.; Jiang, S.B.; Kapatoes, J.M.; Low, M.J.; Murphy, S.B.; Murray, B.R.; et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76a): Respiratory motion in radiation oncology. Med. Phys. 2006, 33, 3874–3900. [Google Scholar] [CrossRef]
- Grimbergen, G.; Eijkelenkamp, H.; Heerkens, H.D.; Raaymakers, B.W.; Intven, M.P.W.; Meijer, G.J. Intrafraction pancreatic tumor motion patterns during ungated magnetic resonance guided radiotherapy with an abdominal corset. Phys. Imaging Radiat. Oncol. 2022, 21, 1–5. [Google Scholar] [CrossRef]
- Oh, S.; Kim, S. Deformable image registration in radiation therapy. Radiat Oncol. J. 2017, 35, 101–111. [Google Scholar] [CrossRef]
- Rong, Y.; Rosu-Bubulac, M.; Benedict, S.H.; Cui, Y.; Ruo, R.; Connell, T.; Kashani, R.; Latifi, K.; Chen, Q.; Geng, H.; et al. Rigid and Deformable Image Registration for Radiation Therapy: A Self-Study Evaluation Guide for NRG Oncology Clinical Trial Participation. Pr. Radiat. Oncol. 2021, 11, 282–298. [Google Scholar] [CrossRef]
- Expert Panel on MR Safety; Kanal, E.; Barkovich, A.J.; Bell, C.; Borgstede, J.P.; Bradley, W.G., Jr.; Froelich, J.W.; Gimbel, J.R.; Gosbee, J.W.; Kuhni-Kaminski, E.; et al. ACR guidance document on MR safe practices. J. Magn. Reson. Imaging 2013, 37, 501–530. [Google Scholar]
- Glide-Hurst, C.K.; Paulson, E.S.; McGee, K.; Tyagi, N.; Hu, Y.; Balter, J.; Bayouth, J. Task group 284 report: Magnetic resonance imaging simulation in radiotherapy: Considerations for clinical implementation, optimization, and quality assurance. Med. Phys. 2021, 48, E636–E670. Available online: https://aapm.onlinelibrary.wiley.com/doi/10.1002/mp.14695 (accessed on 7 September 2023). [CrossRef] [PubMed]
- Malkov, V.N.; Rogers, D.W.O. Sensitive volume effects on Monte Carlo calculated ion chamber response in magnetic fields. Med. Phys. 2017, 44, 4854–4858. [Google Scholar] [CrossRef]
- Strand, S.; Boczkowski, A.; Smith, B.; E Snyder, J.; Hyer, D.E.; Yaddanapudi, S.; Dunkerley, D.A.P.; St-Aubin, J. Analysis of patient-specific quality assurance for Elekta Unity adaptive plans using statistical process control methodology. J. Appl. Clin. Med. Phys. 2021, 22, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Sonke, J.J.; Aznar, M.; Rasch, C. Adaptive Radiotherapy for Anatomical Changes. Semin. Radiat. Oncol. 2019, 29, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Ashida, R.; Nakamura, M.; Yoshimura, M.; Mizowaki, T. Impact of interfractional anatomical variation and setup correction methods on interfractional dose variation in IMPT and VMAT plans for pancreatic cancer patients: A planning study. J. Appl. Clin. Med. Phys. 2020, 21, 49–59. [Google Scholar] [CrossRef]
- Qiu, Z.; Olberg, S.; Den Hertog, D.; Ajdari, A.; Bortfeld, T.; Pursley, J. Online adaptive planning methods for intensity-modulated radiotherapy. Phys. Med. Biol. 2023, 68, 10TR01. [Google Scholar] [CrossRef]
- Goldsworthy, S.; Latour, J.M.; Palmer, S.; McNair, H.A.; Cramp, M. Patient and therapeutic radiographer experiences of comfort during the radiotherapy pathway: A qualitative study. Radiography 2023, 29, S24–S31. [Google Scholar] [CrossRef]
- Matuszak, M.M.; Larsen, E.W.; Fraass, B.A. Reduction of IMRT beam complexity through the use of beam modulation penalties in the objective function: IMRT beam complexity reduction using modulation penalties. Med. Phys. 2007, 34, 507–520. [Google Scholar] [CrossRef]
- Kamperis, E.; Kodona, C.; Hatziioannou, K.; Giannouzakos, V. Complexity in Radiation Therapy: It’s Complicated. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 182–184. [Google Scholar] [CrossRef]
- Saroj, D.; Yadav, S.; Paliwal, N. Does fluence smoothing reduce the complexity of the intensity-modulated radiation therapy treatment plan? A dosimetric analysis. J. Med. Phys. 2022, 47, 336. [Google Scholar]
- Prunaretty, J.; Boisselier, P.; Aillères, N.; Riou, O.; Simeon, S.; Bedos, L.; Azria, D.; Fenoglietto, P. Tracking, gating, free-breathing, which technique to use for lung stereotactic treatments? A dosimetric comparison. Rep. Pract. Oncol. Radiother. 2019, 24, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, D.; Dhont, J.; Boldrini, L.; Chiloiro, G.; Romano, A.; Votta, C.; Longo, S.; Placidi, L.; Azario, L.; De Spirito, M.; et al. Reliability of ITV approach to varying treatment fraction time: A retrospective analysis based on 2D cine MR images. Radiat Oncol. 2020, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Dolde, K.; Dávid, C.; Echner, G.; Floca, R.; Hentschke, C.; Maier, F.; Niebuhr, N.I.; Ohmstedt, K.; Saito, N.; Alimusaj, M.; et al. 4DMRI-based analysis of inter—And intrafractional pancreas motion and deformation with different immobilization devices. Biomed Phys. Eng. Express 2019, 5, 025012. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organs | Dose Constraints (5 Fractions) of 40 Gy in 8 Gy × 5 Fractions |
|---|---|
| PTV (or PTV_eval) | >90% coverage |
| GTV | 90–95% Rx to cover 90–95% |
| Cord | V20Gy < 0.03 cc |
| Liver | V12Gy < 50% |
| Bilat kidneys | V12Gy < 50% |
| Stomach PRV (2 mm) | V40Gy < 0.5 cc, V35Gy < 1 cc, V30Gy < 2 cc |
| Duodenum PRV (2 mm) | V40Gy < 0.5 cc, V35Gy < 1 cc, V30Gy < 2 cc |
| Small bowel PRV (2 mm) | V40Gy < 0.5 cc, V35Gy < 1 cc, V30Gy < 2 cc |
| Colon PRV (2 mm) | V40Gy < 0.5 cc, V35Gy < 1 cc, V30Gy < 2 cc |
| Jejunum PRV (2 mm) | V40Gy < 0.5 cc, V35Gy < 1 cc, V30Gy < 2 cc |
| Spleen | < 4 Gy |
| Heart | Dmax ≤ 20 Gy |
| Patient # | Diagnosis | Age | Gender | SBRT Prescription | # of Beams | Type of Adaptive Planning |
|---|---|---|---|---|---|---|
| P01 | Pancreatic head | 70 | M | 35 Gy in 5 fractions | 13 | ATP (n = 0), ATS (n = 5) |
| P02 | Pancreatic head | 65 | M | 40 Gy in 5 fractions | 13 | ATP (n = 0), ATS (n = 5) |
| P03 | Left adrenal | 61 | M | 30 Gy in 3 fractions | 11 | ATP (n = 0), ATS (n = 3) |
| P04 | Left pancreatic lymph nodes | 72 | M | 45 Gy in 5 fractions | 13 | ATP (n = 0), ATS (n = 5) |
| P05 | Left pancreatic lymph nodes | 60 | F | 40 Gy in 5 fractions | 8 | ATP (n = 0), ATS (n = 5) |
| P06 | Left adrenal gland | 63 | M | 30 Gy in 3 fractions | 9 | ATP (n = 0), ATS (n = 3) |
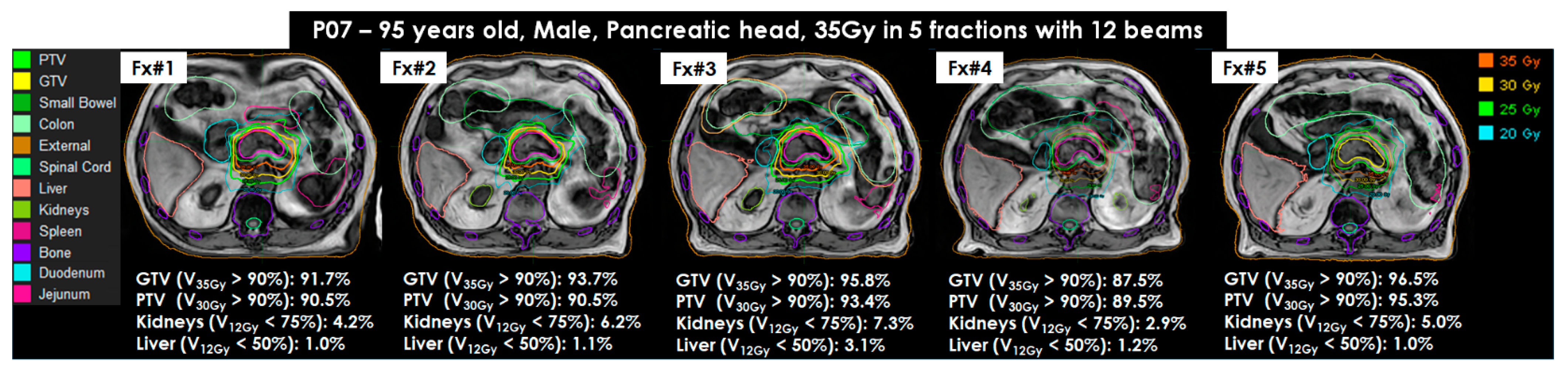
| P07 | Pancreatic head | 95 | M | 35 Gy in 5 fractions | 12 | ATP (n = 0), ATS (n = 5) |
| P08 | Pancreatic head | 65 | F | 45 Gy in 5 fractions | 12 | ATP (n = 4), ATS (n = 1) |
| P09 | Pancreas Boost | 64 | F | 15 Gy in 5 fractions | 12 | ATP (n = 0), ATS (n = 5) |
| P10 | Pancreatic tail | 67 | M | 40 Gy in 5 fractions | 12 | ATP (n = 3), ATS (n = 2) |
| P11 | Pancreas | 79 | M | 35 Gy in 5 fractions | 8 | ATP (n = 0), ATS (n = 5) |
| P12 | Pancreas head/body | 83 | M | 35 Gy in 5 fractions | 11 | ATP (n = 0), ATS (n = 5) |
| P13 | Aortocaval lymph nodes | 64 | M | 25 Gy in 5 fractions | 11 | ATP (n = 4), ATS (n = 1) |
| P14 | Pancreatic body | 77 | F | 45 Gy in 5 fractions | 12 | ATP (n = 1), ATS (n = 4) |
| P15 | Pancreatic head | 57 | F | 37.5 Gy in 5 fractions | 12 | ATP (n = 3), ATS (n = 2) |
| P16 | Pancreatic head | 67 | F | 37.5 Gy in 5 fractions | 14 | ATP (n = 3), ATS (n = 2) |
| P17 | Pancreatic head | 74 | M | 40 Gy in 5 fractions | 11 | ATP (n = 3), ATS (n = 2) |
| P18 | Pancreatic head | 73 | F | 45 Gy in 5 fractions | 7 | ATP (n = 4), ATS (n = 1) |
| P19 | Portocaval node | 62 | M | 40 Gy in 5 fractions | 10 | ATP (n = 5), ATS (n = 0) |
| P20 | Pancreas | 83 | M | 40 Gy in 5 fractions | 13 | ATP (n = 2), ATS (n = 3) |
| P21 | Pancreas | 71 | M | 45 Gy in 5 fractions | 10 | ATP (n = 3), ATS (n = 2) |
| P22 | Pancreatic tail | 72 | F | 40 Gy in 5 fractions | 12 | ATP (n = 2), ATS (n = 3) |
| P23 | Pancreatic body mass | 79 | F | 40 Gy in 5 fractions | 12 | ATP (n = 1), ATS (n = 4) |
| P24 | Pancreatic head | 61 | F | 40 Gy in 5 fractions | 8 | ATP (n = 4), ATS (n = 1) |
| P25 | Pancreatic head | 72 | M | 45 Gy in 5 fractions | 8 | ATP (n = 4), ATS (n = 1) |
| P26 | Left adrenal | 81 | M | 32 Gy in 4 fractions | 7 | ATP (n = 3), ATS (n = 2) |
| Mean ± STD or Total number | 71 ± 9 | M (n = 16), F (n = 10) | 15 Gy to 45 Gy in 3–5 fractions | 7–14 | ATP (n = 49), ATS (n = 77) | |
| Adaptive | MRI Screening | Patient Setup | Imaging Plan-MRI | Fusion/Contouring | Plan Optimization | Plan Review | Plan QA/Approval | Therapist Check | BEAM Delivery | Imaging Post-MRI | Seconds | Minutes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Imaging Verification-MRI | ||||||||||||
| ATP | 81 ± 35 | 493 ± 144 | 276 ± 99 | 763 ± 546 | 330 ± 180 | 264 ± 328 | 248 ± 113 | 17 ± 17 | 725 ± 238 | 97 ± 14 | 3296 ± 925 | 54.9 ± 15.4 |
| ATS | 77 ± 39 | 622 ± 254 | 238 ± 90 | 1629 ± 739 | 545 ± 545 | 337 ± 271 | 337 ± 396 | 26 ± 45 | 850 ± 261 | 98 ± 17 | 4759 ± 1243 | 79.3 ± 20.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.; Renz, P.; Oh, S.; Hwang, M.-S.; Pavord, D.; Yun, K.L.; Collura, C.; McCauley, M.; Colonias, A.; Trombetta, M.; et al. Online Adaptive MRI-Guided Stereotactic Body Radiotherapy for Pancreatic and Other Intra-Abdominal Cancers. Cancers 2023, 15, 5272. https://doi.org/10.3390/cancers15215272
Lee D, Renz P, Oh S, Hwang M-S, Pavord D, Yun KL, Collura C, McCauley M, Colonias A, Trombetta M, et al. Online Adaptive MRI-Guided Stereotactic Body Radiotherapy for Pancreatic and Other Intra-Abdominal Cancers. Cancers. 2023; 15(21):5272. https://doi.org/10.3390/cancers15215272
Chicago/Turabian StyleLee, Danny, Paul Renz, Seungjong Oh, Min-Sig Hwang, Daniel Pavord, Kyung Lim Yun, Colleen Collura, Mary McCauley, Athanasios (Tom) Colonias, Mark Trombetta, and et al. 2023. "Online Adaptive MRI-Guided Stereotactic Body Radiotherapy for Pancreatic and Other Intra-Abdominal Cancers" Cancers 15, no. 21: 5272. https://doi.org/10.3390/cancers15215272
APA StyleLee, D., Renz, P., Oh, S., Hwang, M.-S., Pavord, D., Yun, K. L., Collura, C., McCauley, M., Colonias, A., Trombetta, M., & Kirichenko, A. (2023). Online Adaptive MRI-Guided Stereotactic Body Radiotherapy for Pancreatic and Other Intra-Abdominal Cancers. Cancers, 15(21), 5272. https://doi.org/10.3390/cancers15215272