
A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer
 , ,
, ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
Background
2. Materials and Methods
2.1. Reagents
2.2. Clinical Samples
2.3. ELISA
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
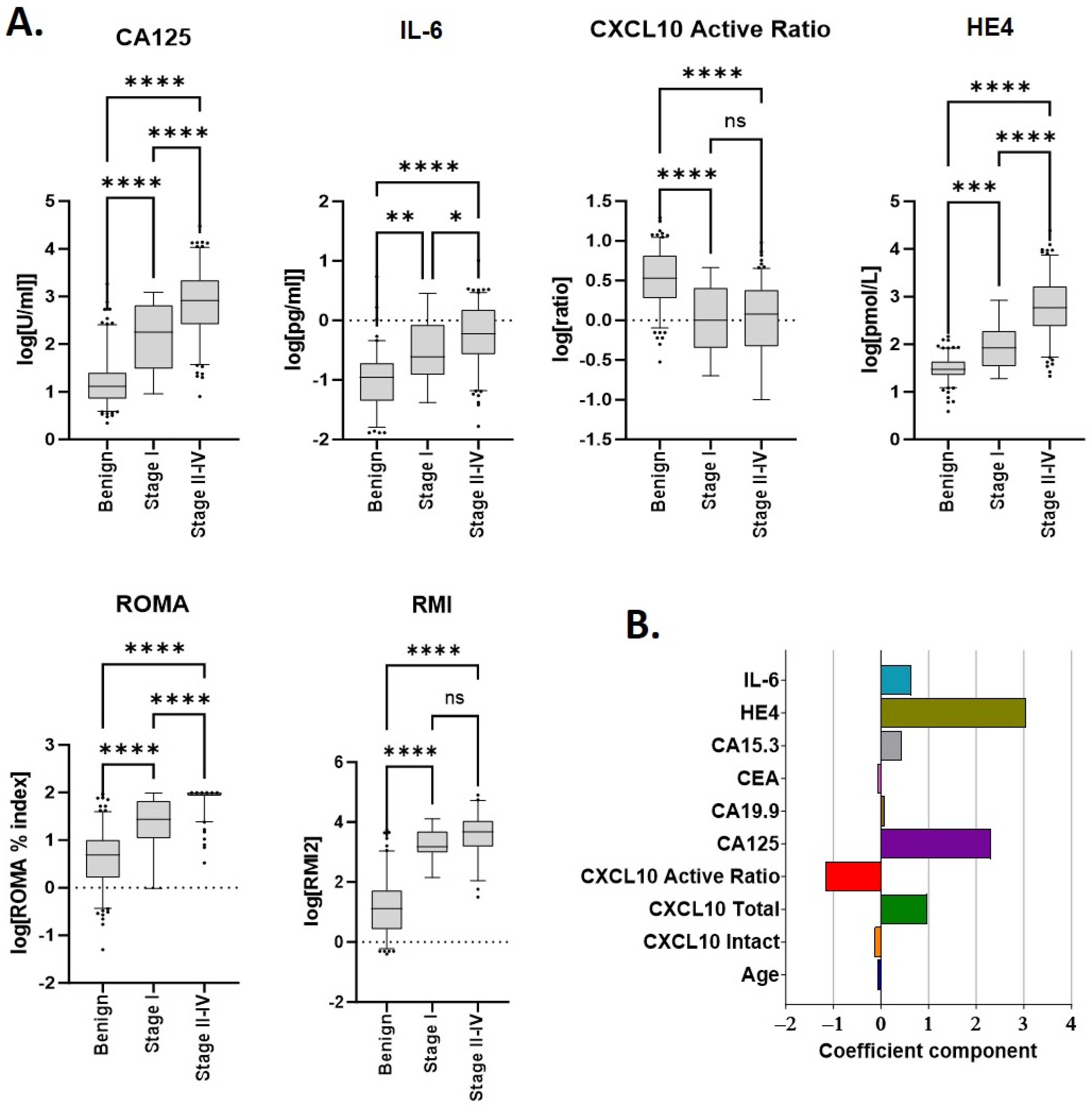
3.2. Individual Marker Performance
3.3. Development of a Combined Biomarker Model
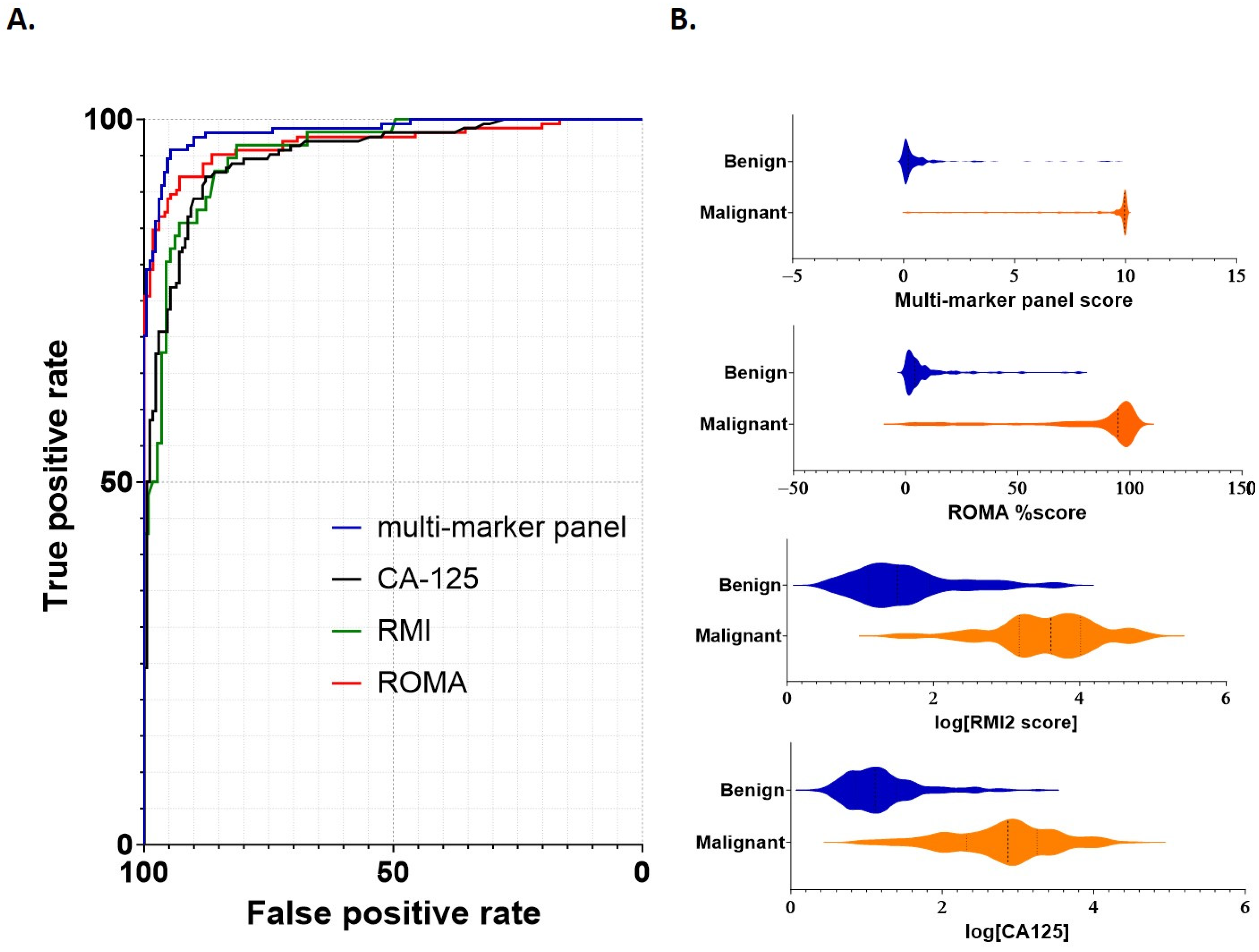
3.4. A Multi-Marker Panel Out-Performs CA125, RMI and ROMA for the Differentiation of Benign from Malignant Disease
3.5. A Multi-Marker Panel Assists in the Identification of Early Stage Cancers
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabasag, C.J.; Fagan, P.J.; Ferlay, J.; Vignat, J.; Laversanne, M.; Liu, L.; Soerjomataram, I. Ovarian cancer today and tomorrow: A global assessment by world region and Human Development Index using GLOBOCAN 2020. Int. J. Cancer 2022, 151, 1535–1541. [Google Scholar] [CrossRef] [PubMed]
- Giede, K.C.; Kieser, K.; Dodge, J.; Rosen, B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol. Oncol. 2005, 99, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Carney, M.E.; Lancaster, J.M.; Ford, C.; Tsodikov, A.; Wiggins, C.L. A population-based study of patterns of care for ovarian cancer: Who is seen by a gynecologic oncologist and who is not? Gynecol. Oncol. 2002, 84, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Earle, C.C.; Schrag, D.; Neville, B.A.; Yabroff, K.R.; Topor, M.; Fahey, A.; Trimble, E.L.; Bodurka, D.C.; Bristow, R.E.; Carney, M.; et al. Effect of surgeon specialty on processes of care and outcomes for ovarian cancer patients. J. Natl. Cancer Inst. 2006, 98, 172–180. [Google Scholar] [CrossRef]
- Arora, T.; Mullangi, S.; Lekkala, M.R. Ovarian Cancer. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Armstrong, D.K.; Alvarez, R.D.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A.; Chen, L.M.; Cristea, M.; DeRosa, M.; Eisenhauer, E.L.; et al. Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 191–226. [Google Scholar] [CrossRef]
- Jacobs, I.; Oram, D.; Fairbanks, J.; Turner, J.; Frost, C.; Grudzinskas, J.G. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br. J. Obstet. Gynaecol. 1990, 97, 922–929. [Google Scholar] [CrossRef]
- Tingulstad, S.; Hagen, B.; Skjeldestad, F.E.; Onsrud, M.; Kiserud, T.; Halvorsen, T.; Nustad, K. Evaluation of a risk of malignancy index based on serum CA125, ultrasound findings and menopausal status in the pre-operative diagnosis of pelvic masses. Br. J. Obstet. Gynaecol. 1996, 103, 826–831. [Google Scholar] [CrossRef]
- Kampan, N.C.; Kartikasari, A.E.R.; Deceneux, C.; Madondo, M.T.; McNally, O.M.; Flanagan, K.L.; Aziz, N.A.; Stephens, A.N.; Reynolds, J.; Quinn, M.A.; et al. Combining TNFR2-Expressing Tregs and IL-6 as Superior Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Masses. Cancers 2023, 15, 667. [Google Scholar] [CrossRef]
- Kang, S.W.; Rainczuk, A.; Oehler, M.K.; Jobling, T.W.; Plebanski, M.; Stephens, A.N. Active Ratio Test (ART) as a Novel Diagnostic for Ovarian Cancer. Diagnostics 2021, 11, 1048. [Google Scholar] [CrossRef]
- Karimi-Zarchi, M.; Mojaver, S.P.; Rouhi, M.; Hekmatimoghaddam, S.H.; Moghaddam, R.N.; Yazdian-Anari, P.; Teimoori, S. Diagnostic Value of the Risk of Malignancy Index (RMI) for Detection of Pelvic Malignancies Compared with Pathology. Electron. Phys. 2015, 7, 1505–1510. [Google Scholar] [CrossRef]
- Ortiz-Munoz, B.; Aznar-Oroval, E.; Garcia Garcia, A.; Covisa Peris, A.; Perez Ballestero, P.; Sanchez Yepes, M.; Garcia Lozano, T.; Illueca Ballester, C.; Garcia Garcia, E. HE4, Ca125 and ROMA algorithm for differential diagnosis between benign gynaecological diseases and ovarian cancer. Tumour Biol. 2014, 35, 7249–7258. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C., Jr.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Yeo, I.; Johnson, R.A. New Family of Power Transformations to Improve Normality or Symmetry. Biometrika 2000, 87, 6. [Google Scholar] [CrossRef]
- Watrowski, R.; Obermayr, E.; Wallisch, C.; Aust, S.; Concin, N.; Braicu, E.I.; Van Gorp, T.; Hasenburg, A.; Sehouli, J.; Vergote, I.; et al. Biomarker-Based Models for Preoperative Assessment of Adnexal Mass: A Multicenter Validation Study. Cancers 2022, 14, 1780. [Google Scholar] [CrossRef]
- Bast, R.C., Jr.; Klug, T.L.; St John, E.; Jenison, E.; Niloff, J.M.; Lazarus, H.; Berkowitz, R.S.; Leavitt, T.; Griffiths, C.T.; Parker, L.; et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N. Engl. J. Med. 1983, 309, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Liest, A.L.; Omran, A.S.; Mikiver, R.; Rosenberg, P.; Uppugunduri, S. RMI and ROMA are equally effective in discriminating between benign and malignant gynecological tumors: A prospective population-based study. Acta Obstet. Gynecol. Scand. 2019, 98, 24–33. [Google Scholar] [CrossRef]
- Schorge, J.O.; Eisenhauer, E.E.; Chi, D.S. Current surgical management of ovarian cancer. Hematol. Oncol. Clin. N. Am. 2012, 26, 93–109. [Google Scholar] [CrossRef]
- Bolstad, N.; Oijordsbakken, M.; Nustad, K.; Bjerner, J. Human epididymis protein 4 reference limits and natural variation in a Nordic reference population. Tumour Biol. 2012, 33, 141–148. [Google Scholar] [CrossRef]
- Engelen, M.J.; Kos, H.E.; Willemse, P.H.; Aalders, J.G.; de Vries, E.G.; Schaapveld, M.; Otter, R.; van der Zee, A.G. Surgery by consultant gynecologic oncologists improves survival in patients with ovarian carcinoma. Cancer 2006, 106, 589–598. [Google Scholar] [CrossRef] [PubMed]
- NIH Consensus Development Panel on Ovarian Cancer. NIH consensus conference. Ovarian cancer. Screening, treatment, and follow-up. JAMA 1995, 273, 491–497. [Google Scholar] [CrossRef]
- Sonoda, Y. Management of early ovarian cancer. Oncology 2004, 18, 343–356. [Google Scholar]
- Rainczuk, A.; Rao, J.R.; Gathercole, J.L.; Fairweather, N.J.; Chu, S.; Masadah, R.; Jobling, T.W.; Deb-Choudhury, S.; Dyer, J.; Stephens, A.N. Evidence for the antagonistic form of CXC-motif chemokine CXCL10 in serous epithelial ovarian tumours. Int. J. Cancer 2014, 134, 530–541. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin. Management of adnexal masses. Obstet. Gynecol. 2007, 110, 201–214. [Google Scholar] [CrossRef]
- Parker, W.H.; Jacoby, V.; Shoupe, D.; Rocca, W. Effect of bilateral oophorectomy on women’s long-term health. Womens Health 2009, 5, 565–576. [Google Scholar] [CrossRef] [PubMed]
- Hassan, H.; Allen, I.; Sofianopoulou, E.; Walburga, Y.; Turnbull, C.; Eccles, D.M.; Tischkowitz, M.; Pharoah, P.; Antoniou, A.C. Long-term outcomes of hysterectomy with bilateral salpingo-oophorectomy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2023; in press. [Google Scholar] [CrossRef] [PubMed]
- Gottschau, M.; Rosthoj, S.; Settnes, A.; Aalborg, G.L.; Viuff, J.H.; Munk, C.; Jensen, A.; Kjaer, S.K.; Mellemkjaer, L. Long-Term Health Consequences After Ovarian Removal at Benign Hysterectomy: A Nationwide Cohort Study. Ann. Intern. Med. 2023, 176, 596–604. [Google Scholar] [CrossRef]
- Burgess, B.T.; Ueland, F.R. Adnexal tumors in menopausal women: Surgery or surveillance? Menopause 2019, 26, 554–556. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet. Gynecol. 2016, 128, e210–e226. [Google Scholar] [CrossRef]
- Donnez, J. Fertility preservation in women, focusing on cancer, benign diseases and social reasons. Minerva Ginecol. 2018, 70, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- Schuring, A.N.; Fehm, T.; Behringer, K.; Goeckenjan, M.; Wimberger, P.; Henes, M.; Henes, J.; Fey, M.F.; von Wolff, M. Practical recommendations for fertility preservation in women by the FertiPROTEKT network. Part I: Indications for fertility preservation. Arch. Gynecol. Obstet. 2018, 297, 241–255. [Google Scholar] [CrossRef]
- Liu, D.; Cai, J.; Gao, A.; Wang, Z.; Cai, L. Fertility sparing surgery vs. radical surgery for epithelial ovarian cancer: A meta-analysis of overall survival and disease-free survival. BMC Cancer 2020, 20, 320. [Google Scholar] [CrossRef]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and algorithms for diagnosis of ovarian cancer: CA125, HE4, RMI and ROMA, a review. J. Ovarian Res. 2019, 12, 28. [Google Scholar] [CrossRef]
- Wilailak, S.; Chan, K.K.; Chen, C.A.; Nam, J.H.; Ochiai, K.; Aw, T.C.; Sabaratnam, S.; Hebbar, S.; Sickan, J.; Schodin, B.A.; et al. Distinguishing benign from malignant pelvic mass utilizing an algorithm with HE4, menopausal status, and ultrasound findings. J. Gynecol. Oncol. 2015, 26, 46–53. [Google Scholar] [CrossRef]
- Berek, J.S.; Renz, M.; Kehoe, S.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155 (Suppl. S1), 61–85. [Google Scholar] [CrossRef]
- Nolen, B.M.; Lokshin, A.E. Protein biomarkers of ovarian cancer: The forest and the trees. Future Oncol. 2012, 8, 55–71. [Google Scholar] [CrossRef]
- Moore, L.E.; Pfeiffer, R.M.; Zhang, Z.; Lu, K.H.; Fung, E.T.; Bast, R.C., Jr. Proteomic biomarkers in combination with CA 125 for detection of epithelial ovarian cancer using prediagnostic serum samples from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. Cancer 2012, 118, 91–100. [Google Scholar] [CrossRef]
- Coleman, R.L.; Herzog, T.J.; Chan, D.W.; Munroe, D.G.; Pappas, T.C.; Smith, A.; Zhang, Z.; Wolf, J. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am. J. Obstet. Gynecol. 2016, 215, 82.e1–82.e11. [Google Scholar] [CrossRef]
- Bast, R.C., Jr.; Lu, Z.; Han, C.Y.; Lu, K.H.; Anderson, K.S.; Drescher, C.W.; Skates, S.J. Biomarkers and Strategies for Early Detection of Ovarian Cancer. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2504–2512. [Google Scholar] [CrossRef]
- van Baal, J.; Van de Vijver, K.K.; Algera, M.D.; van der Aa, M.A.; Sonke, G.S.; van Driel, W.J.; Kenter, G.G.; Amant, F.C.; Lok, C.A.R. The effect of adjuvant chemotherapy on survival in patients with FIGO stage I high-grade serous ovarian cancer. Gynecol. Oncol. 2019, 153, 562–567. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| All | Pre-Menopausal | Post-Menopausal | ||
|---|---|---|---|---|
| # Participants (total) | n = 334 | n = 115 | n = 219 | |
| Age at diagnosis (years) | median | 65 | 45 | 65 |
| IQ range | 47–68 | 40–49 | 56–71 | |
| Pathology (n=) | benign | 170 | 83 | 87 |
| malignant | 164 | 32 | 132 | |
| Tumor type (n=) | serous | 126 | 18 | 108 |
| mucinous | 6 | 3 | 3 | |
| endometroid | 5 | 1 | 4 | |
| clear cell | 8 | 4 | 4 | |
| mixed epithelial | 9 | 3 | 6 | |
| other | 10 | 3 | 7 | |
| Grade (n=) | 1 | 5 | 2 | 3 |
| 2 | 20 | 8 | 12 | |
| 3 | 139 | 22 | 117 | |
| Stage (n=) | I | 17 | 11 | 6 |
| II | 4 | 0 | 4 | |
| III–IV | 143 | 21 | 122 | |
| Genetic Predisposition (n=) | BRCA1 | 43 | 25 | 18 |
| BRCA2 | 49 | 22 | 27 | |
| other (lynch, BRIP1+, PALB+, VUS) | 31 | 15 | 16 | |
| wild type | 40 | 13 | 27 | |
| unknown | 171 | 40 | 131 | |
| Ultrasound score (n=) | 1 | 101 | 50 | 51 |
| 4 | 68 | 16 | 52 | |
| unavailable | 165 | 49 | 116 | |
| Benign | Malignant | |||
|---|---|---|---|---|
| Biomarker | # Samples | Biomarker | # Samples | |
| (Median/IQ Range) | (Pre/Post-Menopausal) | (Median/IQ Range) | (Pre/Post-Menopausal) | |
| CA125 (U/mL) | 13 (7.2–25.1) | n = 83/87 | 741.5 (210.3–1785.0) | n = 32/132 |
| HE4 (pmol/L) | 30 (22.7–43.5) | n = 83/86 | 465.6 (193.9–1353) | n = 32/132 |
| CXCL10 Active Ratio (pg/pg) | 3.4 (1.9–6.5) | n = 83/87 | 1.2 (0.4–2.4) | n = 32/132 |
| IL-6 (ng/mL) | 0.0 (0.0–0.1) | n = 83/86 | 0.6 (0.2–1.4) | n = 32/132 |
| ROMA INDEX % (calculated) | 4.2 (1.6–8.7) | n = 83/86 | 94.7 (78.0–100) | n = 32/132 |
| RMI score (calculated) | 32 (13.1–88.0) | n = 57/56 | 4080 (1487–10,292) | n = 10/47 |
| CEA | 1.0 (0.6, 1.9) | n = 82/87 | 0.8 (0.5, 1.6) | n = 31/121 |
| CA15.3 | 10.8 (7.1, 14.0) | n = 82/87 | 36.7 (17.3, 89.5) | n = 31/121 |
| CA19.9 | 8.6 (5, 14.6) | n = 82/87 | 9.8 (3.9, 23.1) | n = 31/121 |
| AUC | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|
| Cross-Validation | 0.981 | 0.930 | 0.952 | 0.950 | 0.935 |
| Performance on Full Dataset | 0.984 | 0.939 | 0.953 | 0.951 | 0.942 |
| Subtractive Difference % | −0.26% | −0.85% | −0.13% | −0.09% | −0.64% |
| Predictor | Published Cutoff | Menopausal Status | n= | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Multimarker Panel | combined | 334 | 0.98 (0.97–1.00) | 0.95 (0.91–0.98) | 0.95 (0.90–0.98) | 0.95 (0.90–0.98) | 0.95 (0.91–0.98) | |
| n/a | pre | 115 | 0.95 (0.91–1.00) | 0.81 (0.64–0.93) | 0.98 (0.92–1.00) | 0.93 (0.77–0.99) | 0.93 (0.86–0.97) | |
| post | 219 | 0.99 (0.98–1.00) | 0.99 (0.95–1.00) | 0.92 (0.84–0.97) | 0.95 (0.90–0.98) | 0.98 (0.92–1.00) | ||
| CA125 | combined | 334 | 0.95 (0.93–0.97) | 0.94 (0.89–0.97) | 0.82 (0.75–0.87) | 0.83 (0.77–0.88) | 0.93 (0.88–0.97) | |
| 35 | pre | 115 | 0.92 (0.86–0.98) | 0.91 (0.75–0.98) | 0.80 (0.69–0.88) | 0.63 (0.48–0.77) | 0.96 (0.88–0.99) | |
| post | 219 | 0.96 (0.93–0.98) | 0.95 (0.89–0.98) | 0.84 (0.75–0.91) | 0.90 (0.84–0.94) | 0.91 (0.83–0.96) | ||
| ROMA% | combined | 333 | 0.97 (0.95–0.99) | 0.93 (0.88–0.96) | 0.92 (0.87–0.96) | 0.92 (0.87–0.96) | 0.93 (0.88–0.96) | |
| 13.1 | pre | 115 | 0.93 (0.87–0.99) | 0.81 (0.64–0.93) | 0.95 (0.88–0.99) | 0.87 (0.69–0.96) | 0.93 (0.85–0.97) | |
| 27.7 | post | 218 | 0.98 (0.97–1.00) | 0.96 (0.90–0.98) | 0.90 (0.81–0.95) | 0.93 (0.88–0.97) | 0.93 (0.85–0.97) | |
| RMI2 | combined | 169 | 0.95 (0.93–0.98) | 0.96 (0.88–1.00) | 0.75 (0.66–0.83) | 0.66 (0.55–0.76) | 0.98 (0.92–1.00) | |
| 200 | pre | 66 | 0.98 (0.94–1.00) | 0.89 (0.52–1.00) | 0.86 (0.74–0.94) | 0.50 (0.25–0.75) | 0.98 (0.89–1.00) | |
| post | 103 | 0.94 (0.89–0.98) | 0.98 (0.89–1.00) | 0.64 (0.50–0.77) | 0.70 (0.57–0.80) | 0.97 (0.86–1.00) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stephens, A.N.; Hobbs, S.J.; Kang, S.-W.; Bilandzic, M.; Rainczuk, A.; Oehler, M.K.; Jobling, T.W.; Plebanski, M.; Allman, R. A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer. Cancers 2023, 15, 5267. https://doi.org/10.3390/cancers15215267
Stephens AN, Hobbs SJ, Kang S-W, Bilandzic M, Rainczuk A, Oehler MK, Jobling TW, Plebanski M, Allman R. A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer. Cancers. 2023; 15(21):5267. https://doi.org/10.3390/cancers15215267
Chicago/Turabian StyleStephens, Andrew N., Simon J. Hobbs, Sung-Woon Kang, Maree Bilandzic, Adam Rainczuk, Martin K. Oehler, Tom W. Jobling, Magdalena Plebanski, and Richard Allman. 2023. "A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer" Cancers 15, no. 21: 5267. https://doi.org/10.3390/cancers15215267
APA StyleStephens, A. N., Hobbs, S. J., Kang, S.-W., Bilandzic, M., Rainczuk, A., Oehler, M. K., Jobling, T. W., Plebanski, M., & Allman, R. (2023). A Novel Predictive Multi-Marker Test for the Pre-Surgical Identification of Ovarian Cancer. Cancers, 15(21), 5267. https://doi.org/10.3390/cancers15215267