

Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population and Selection Criteria
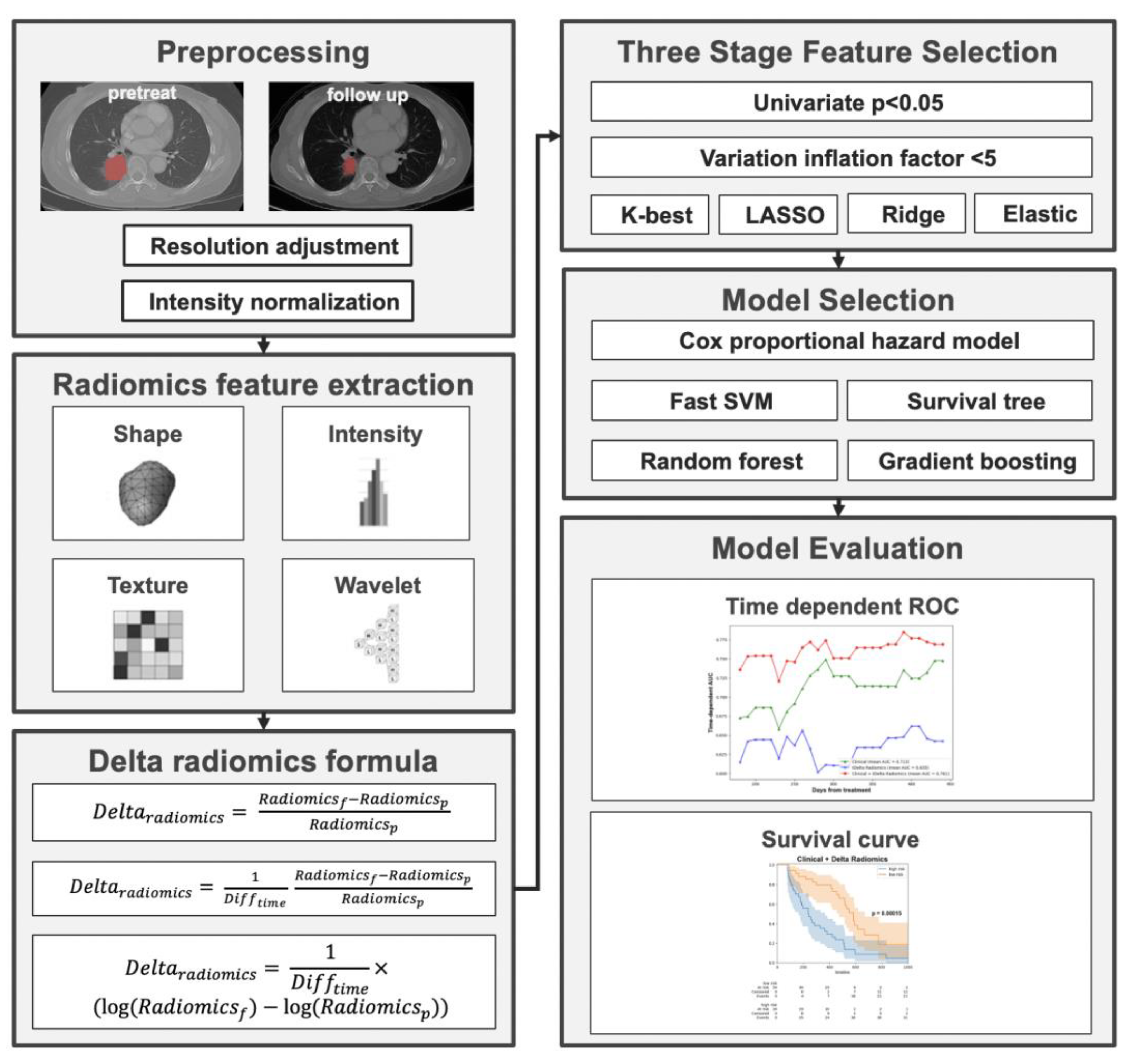
2.2. CT Data and Image Preprocessing
2.3. Radiomic Feature Extraction
2.4. Feature Selection and Predictive Modeling
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Patient Cohort
3.2. Comparison of Different Radiomics Methods
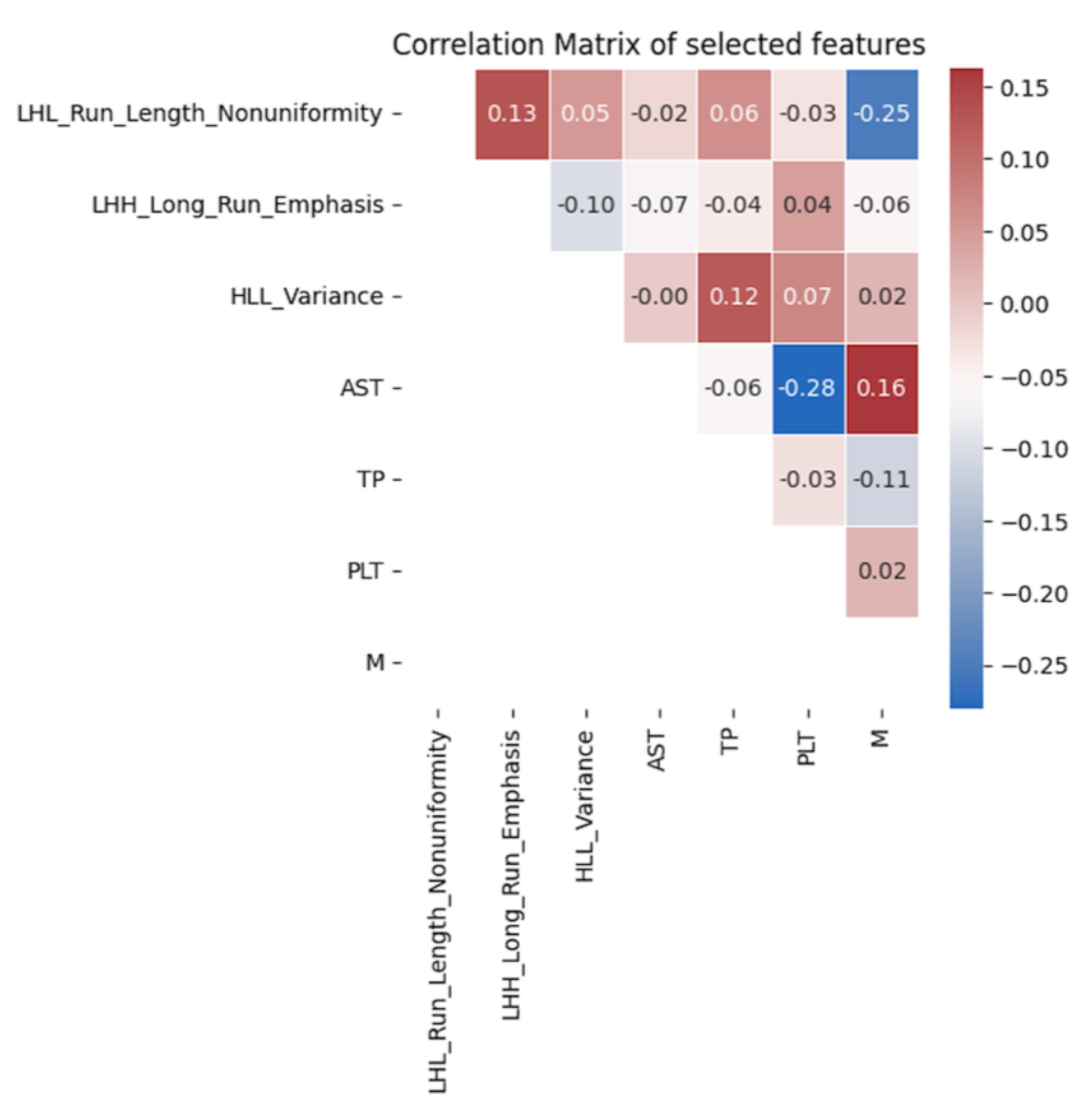
3.3. Final Selected Features Included in the Model
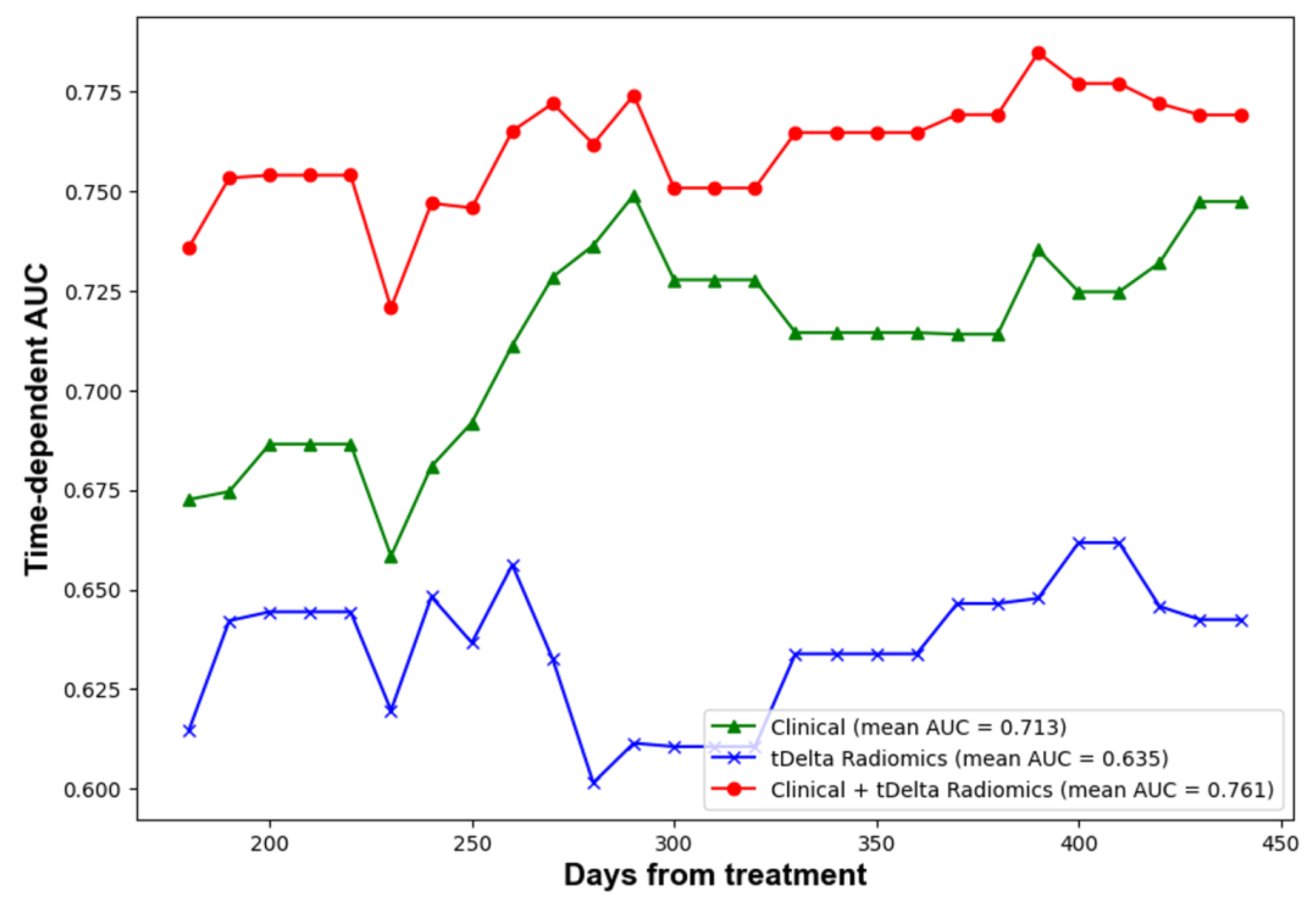
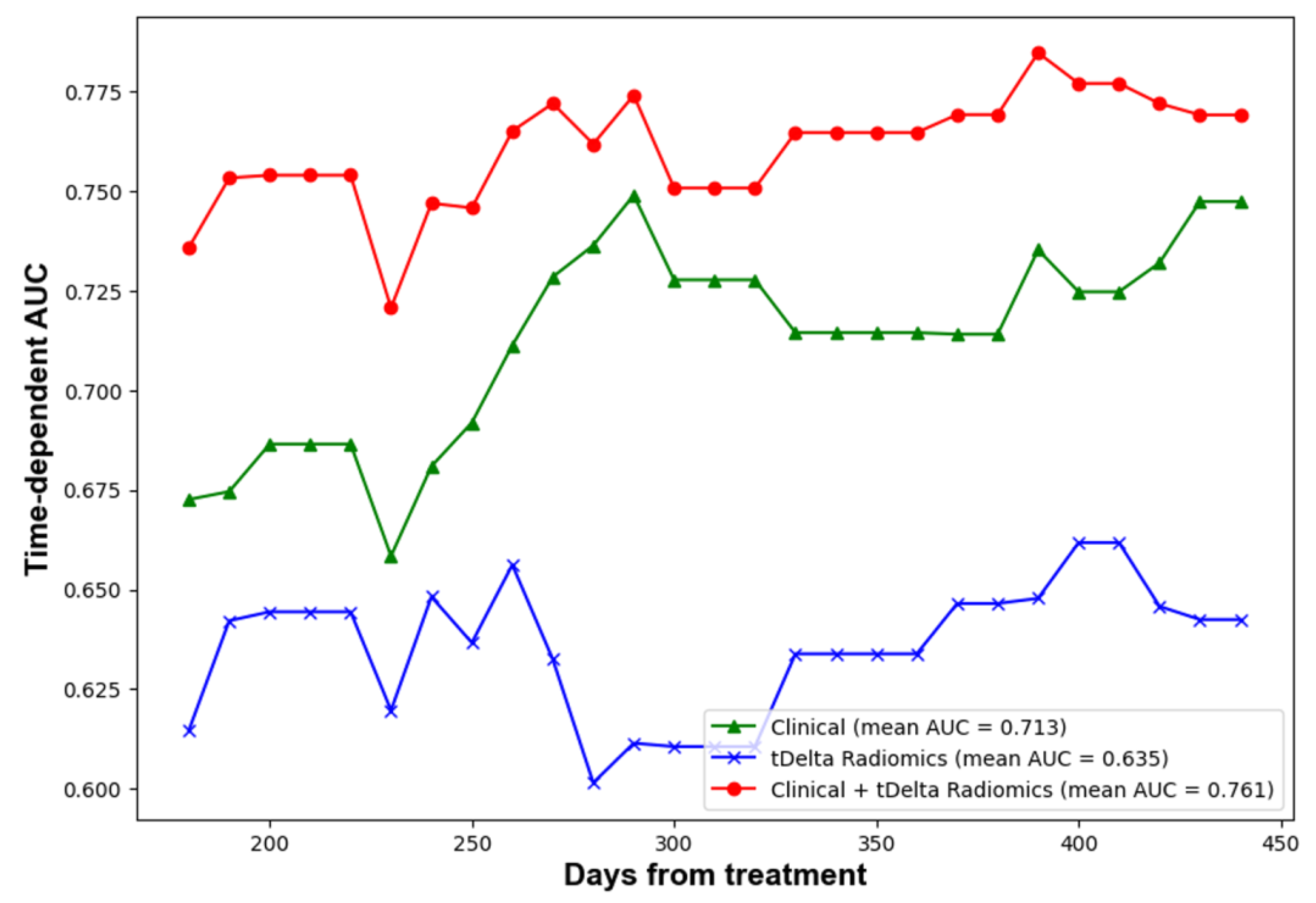
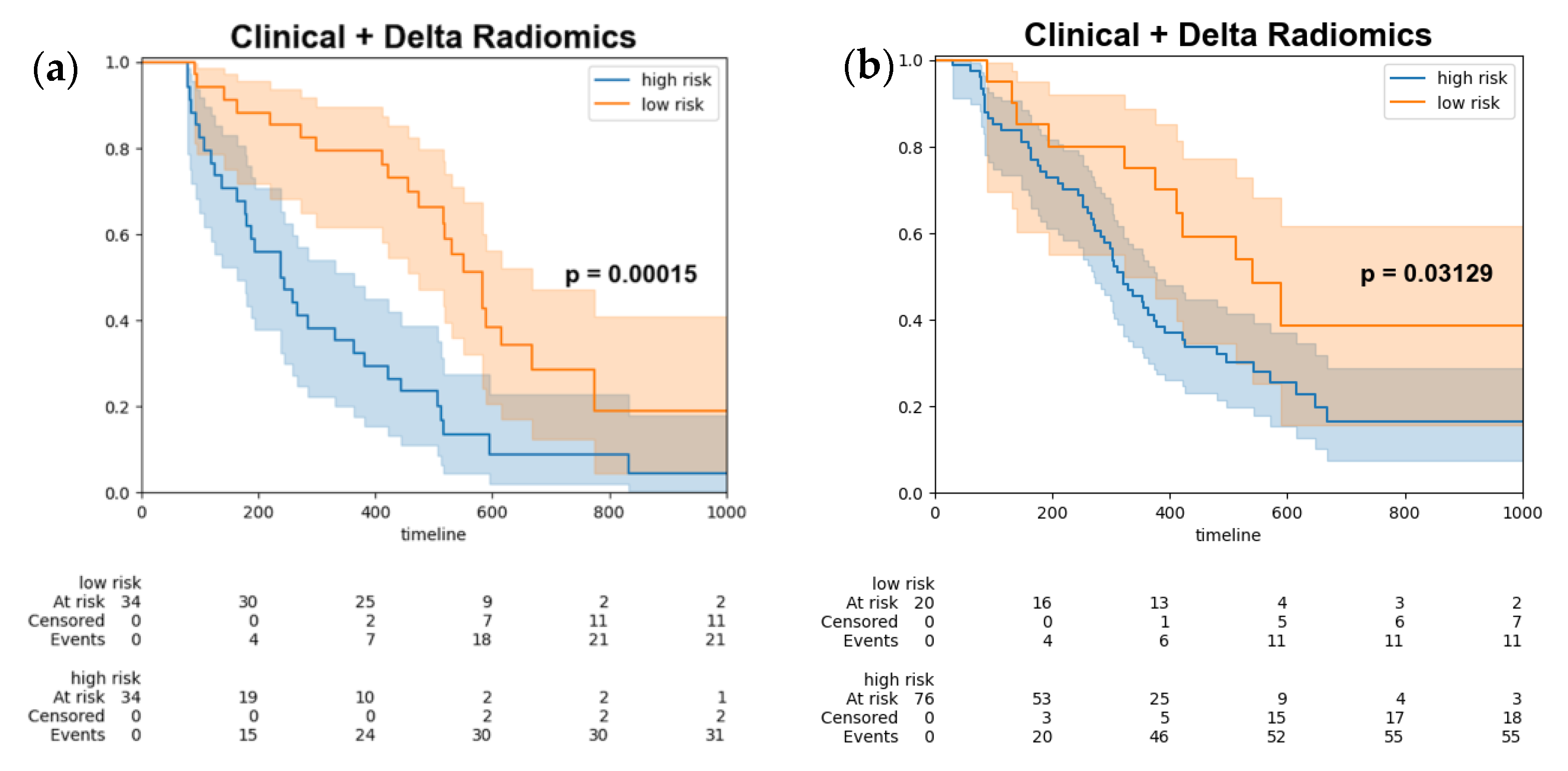
3.4. Performance of Predictive Models for the Prediction of Progression Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’amico, T.A.; et al. NCCN guidelines insights: Non–small cell lung cancer, version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in resected EGFR-mutated non–small-cell lung cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Pathiranage, V.C.; Thabrew, I.; Samarakoon, S.R.; Tennekoon, K.H.; Rajagopalan, U.; Ediriweera, M.K. Evaluation of anticancer effects of a pharmaceutically viable extract of a traditional polyherbal mixture against non-small-cell lung cancer cells. J. Integr. Med. 2020, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.Y.; Xu, L.; Li, H.G.; Tian, J.H.; Jiao, L.J.; You, S.F.; Han, Z.F.; Jiang, Y.; Guo, H.R.; Liu, H. Chemotherapy in conjunction with traditional Chinese medicine for survival of elderly patients with advanced non-small-cell lung cancer: Protocol for a randomized double-blind controlled trial. J. Integr. Med. 2014, 12, 175–181. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv192–iv237. [Google Scholar] [CrossRef]
- Naidich, D.P.; Bankier, A.A.; MacMahon, H.; Schaefer-Prokop, C.M.; Pistolesi, M.; Goo, J.M.; Macchiarini, P.; Crapo, J.D.; Herold, C.J.; Austin, J.H.; et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: A statement from the Fleischner Society. Radiology 2013, 266, 304–317. [Google Scholar] [CrossRef] [PubMed]
- van Elmpt, W.; Öllers, M.; Dingemans, A.-M.C.; Lambin, P.; De Ruysscher, D. Response assessment using 18F-FDG PET early in the course of radiotherapy correlates with survival in advanced-stage non-small cell lung cancer. J. Nucl. Med. 2012, 53, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Parmar, C.; Grossmann, P.; Bussink, J.; Lambin, P.; Aerts, H.J. Machine learning methods for quantitative radiomic biomarkers. Sci. Rep. 2015, 5, 13087. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Yip, S.S.; Aerts, H.J. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Fave, X.; Zhang, L.; Yang, J.; Mackin, D.; Balter, P.; Gomez, D.; Followill, D.; Jones, A.K.; Stingo, F.; Liao, Z.; et al. Delta-radiomics features for the prediction of patient outcomes in non-small cell lung cancer. Sci. Rep. 2017, 7, 588. [Google Scholar] [CrossRef]
- Carvalho, S.; Leijenaar, R.T.H.; Troost, E.G.C.; Van Elmpt, W.; Muratet, J.-P.; Denis, F.; De Ruysscher, D.; Aerts, H.J.W.L.; Lambin, P. Early variation of FDG-PET radiomics features in NSCLC is related to overall survival—The “delta radiomics” concept. Radiother. Oncol. 2016, 127, S19–S20. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lu, B.; Yang, X.; Lan, D.; Lin, S.; Zhou, Z.; Li, K.; Deng, D.; Peng, P.; Zeng, Z.; et al. Prognostic analysis and risk stratification of lung adenocarcinoma undergoing EGFR-TKI therapy with time-serial CT-based radiomics signature. Eur. Radiol. 2023, 33, 825–835. [Google Scholar] [CrossRef]
- Dercle, L.; Fronheiser, M.; Lu, L.; Du, S.; Hayes, W.; Leung, D.K.; Roy, A.; Wilkerson, J.; Guo, P.; Fojo, A.T.; et al. Identification of Non–Small Cell Lung Cancer Sensitive to Systemic Cancer Therapies Using Radiomics. Clin. Cancer Res. 2020, 26, 2151–2162. [Google Scholar] [CrossRef] [PubMed]
- Khorrami, M.; Prasanna, P.; Gupta, A.; Patil, P.; Velu, P.D.; Thawani, R.; Corredor, G.; Alilou, M.; Bera, K.; Fu, P.; et al. Changes in CT Radiomic Features Associated with Lymphocyte Distribution Predict Overall Survival and Response to Immunotherapy in Non–Small Cell Lung Cancer. Cancer Immunol. Res. 2020, 8, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image biomarker standardisation initiative. arXiv 2016, arXiv:1612.07003. [Google Scholar] [CrossRef]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and reproducibility of radiomic features: A systematic review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kim, J.; Balagurunathan, Y.; Li, Q.; Garcia, A.L.; Stringfield, O.; Ye, Z.; Gillies, R.J. Radiomic features are associated with EGFR mutation status in lung adenocarcinomas. Clin. Lung Cancer 2019, 20, e601–e608. [Google Scholar] [CrossRef]
- Coroller, T.P.; Agrawal, V.; Narayan, V.; Hou, Y.; Grossmann, P.; Lee, S.W.; Mak, R.H.; Aerts, H.J. Radiomic phenotype features predict pathological response in non-small cell lung cancer. Radiother. Oncol. 2020, 144, 79–86. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meter, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Aisner, D.L.; Wood, D.E.; Akerley, W.; Bauman, J.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.J.; Dobelbower, M.; et al. NCCN guidelines insights: Non–small cell lung cancer, version 4.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.-F.; Hsu, F.-T.; Hsieh, K.L.-C.; Kao, Y.-C.J.; Cheng, S.-J.; Hsu, J.B.-K.; Tsai, P.-H.; Chen, R.-J.; Huang, C.-C.; Yen, Y.; et al. Machine learning–based radiomics for molecular subtyping of gliomas. Clin. Cancer Res. 2018, 24, 4429–4436. [Google Scholar] [CrossRef]
- Lu, C.-F.; Liao, C.-Y.; Chao, H.-S.; Chiu, H.-Y.; Wang, T.-W.; Lee, Y.; Chen, J.-R.; Shiao, T.-H.; Chen, Y.-M.; Wu, Y.-T. A radiomics-based deep learning approach to predict progression free-survival after tyrosine kinase inhibitor therapy in non-small cell lung cancer. Cancer Imaging 2023, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Waljee, A.K.; Mukherjee, A.; Singal, A.G.; Zhang, Y.; Warren, J.; Balis, U.; Marrero, J.; Zhu, J.; Higgins, P.D. Comparison of imputation methods for missing laboratory data in medicine. BMJ Open 2013, 3, e002847. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural features for image classification. IEEE Trans. Syst. Man Cybern. 1973, 6, 610–621. [Google Scholar] [CrossRef]
- Quail, D.F.; Joyce, J.A. Microenvironmental regulation of tumor progression and metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef]
- O’Connor, J.P.B.; Rose, C.J.; Waterton, J.C.; Carano, R.A.D.; Parker, G.J.M.; Jackson, A. Imaging intratumor heterogeneity: Role in therapy response, resistance, and clinical outcome. Clin. Cancer Res. 2017, 21, 249–257. [Google Scholar] [CrossRef]
- Cousin, F.; Louis, T.; Dheur, S.; Aboubakar, F.; Ghaye, B.; Occhipinti, M.; Vos, W.; Bottari, F.; Paulus, A.; Sibille, A.; et al. Radiomics and Delta-Radiomics Signatures to Predict Response and Survival in Patients with Non-Small-Cell Lung Cancer Treated with Immune Checkpoint Inhibitors. Cancers 2023, 15, 1968. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Yang, P.-F.; Chen, S.; Shao, Y.-Y.; Xu, L.-M.; Wu, Y.; Teng, W.; Zhou, X.-Z.; Li, B.-H.; Luo, C.; et al. A Delta-radiomics model for preoperative evaluation of Neoadjuvant chemotherapy response in high-grade osteosarcoma. Cancer Imaging 2020, 20, 7. [Google Scholar] [CrossRef] [PubMed]
- Marcu, D.C.; Grava, C.; Marcu, L.G. Current Role of Delta Radiomics in Head and Neck Oncology. Int. J. Mol. Sci. 2023, 24, 2214. [Google Scholar] [CrossRef] [PubMed]
- Mackin, D.; Fave, X.B.; Zhang, L.; Fried, D.B.; Yang, J.; Taylor, B.; Rodriguez-Rivera, E.; Dodge, C.; Jones, A.K.; Court, L. Measuring Computed Tomography Scanner Variability of Radiomics Features. Investig. Radiol. 2015, 50, 757–765. [Google Scholar] [CrossRef]
- He, L.; Huang, Y.; Ma, Z.; Liang, C.; Liang, C.; Liu, Z. Effects of contrast-enhancement, reconstruction slice thickness and convolution kernel on the diagnostic performance of radiomics signature in solitary pulmonary nodule. Sci. Rep. 2016, 6, 34921. [Google Scholar] [CrossRef] [PubMed]
- Goh, V.; Ganeshan, B.; Nathan, P.; Juttla, J.K.; Vinayan, A.; Miles, K.A. Assessment of response to tyrosine kinase inhibitors in metastatic renal cell cancer: CT texture as a predictive biomarker. Radiology 2011, 261, 165–171. [Google Scholar] [CrossRef]
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of radiomics for deciphering tumor phenotype with imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef]
- Berenguer, R.; Pastor-Juan, M.D.R.; Canales-Vázquez, J.; Castro-García, M.; Villas, M.V.; Mansilla Legorburo, F.; Sabater, S. Radiomics of CT features may be nonreproducible and redundant: Influence of CT acquisition parameters. Radiology 2018, 288, 407–415. [Google Scholar] [CrossRef]
- Li, Y.; Lu, L.; Xiao, M.; Dercle, L.; Huang, Y.; Zhang, Z.; Schwartz, L.H.; Li, D.; Zhao, B. CT slice thickness and convolution Kernel affect performance of a radiomic model for predicting EGFR status in non-small cell lung cancer: A preliminary study. Sci. Rep. 2018, 8, 17913. [Google Scholar] [CrossRef]
- Shafiq-ul-Hassan, M.; Latifi, K.; Zhang, G.; Ullah, G.; Gillies, R.; Moros, E. Voxel size and gray level normalization of CT radiomic features in lung cancer. Sci. Rep. 2018, 8, 10545. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Lee, H.-J.; Kim, K.G.; Lee, S.H. The effect of CT scan parameters on the measurement of CT radiomic features: A lung nodule phantom study. Comput. Math. Methods Med. 2019, 2019, 8790694. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef]
- Leblanc, M.; Crowley, J. Survival Trees by Goodness of Split. J. Am. Stat. Assoc. 1993, 88, 457–467. [Google Scholar] [CrossRef]
- Ishwaran, H.; Kogalur, U.B.; Blackstone, E.H.; Lauer, M.S. Random survival forests. Ann. Appl. Stat. 2008, 2, 841–860. [Google Scholar] [CrossRef]
- Chen, Y.; Jia, Z.; Mercola, D.; Xie, X. A gradient boosting algorithm for survival analysis via direct optimization of concordance index. Comput. Math. Methods Med. 2013, 2013, 873595. [Google Scholar] [CrossRef]
- Pölsterl, S.; Navab, N.; Katouzian, A. Fast Training of Support Vector Machines for Survival Analysis. Mach. Learn. Knowl. Discov. Databases 2015, 9285, 243–259. [Google Scholar]
- Håvard, K.; Borgan, Ø.; Scheel, I. Time-to-event prediction with neural networks and Cox regression. J. Mach. Learn. Res. 2019, 20, 1–30. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Training (n = 158) | Test (n = 68) | TCGH (n = 96) |
|---|---|---|---|
| Age | |||
| <60, N (%) | 70 (44.3) | 22 (32.4) | 29 (30.2) |
| >60, N (%) | 88 (55.7) | 46 (67.6) | 67 (69.8) |
| Gender | |||
| Female, N (%) | 99 (62.7) | 35 (51.5) | 57 (59.4) |
| Smoking status | |||
| Smoker, N (%) | 35 (22.2) | 23 (33.8) | 21(21.9) |
| ECOG PS | |||
| 0, N (%) | 49 (31.0) | 35 (51.5) | 4 (4.2) |
| 1, N (%) | 91 (57.6) | 28 (41.2) | 65 (67.7) |
| 2, N (%) | 11 (7.0) | 4 (5.9) | 10 (10.4) |
| >2, N (%) | 7 (4.4) | 1 (1.5) | 17 (17.6) |
| Histology of NSCLC | |||
| Adenocarcinoma, N (%) | 155 (98.1) | 65 (95.6) | 89 (92.7) |
| Squamous cell carcinoma, N (%) | 1 (1.3) | 2 (2.9) | 0 (0) |
| Other | 2 (0.6) | 1 (1.5) | 7 (7.3) |
| Clinical T stage | |||
| 1, N (%) | 19 (12.0) | 10 (14.7) | 10 (10.4) |
| 2, N (%) | 41 (25.9) | 24 (35.3) | 23 (24) |
| 3, N (%) | 27 (17.1) | 9 (13.2) | 6 (6.2) |
| 4, N (%) | 67 (42.4) | 23 (33.8) | 57 (59.4) |
| None | 4 (2.5) | 2 (2.9) | 0 (0) |
| Clinical N stage | |||
| 0, N (%) | 45 (28.5) | 14 (20.6) | 25 (26.0) |
| 1, N (%) | 13 (8.2) | 6 (8.8) | 2 (2.1) |
| 2, N (%) | 40 (25.3) | 22 (32.4) | 36 (37.5) |
| 3, N (%) | 59 (37.3) | 25 (36.8) | 33 (34.4) |
| None | 1 (0.6) | 1 (1.5) | 0 (0) |
| Clinical M stage | |||
| 0, N (%) | 6 (3.8) | 2 (2.9) | 8 (7.9) |
| 1a, N (%) | 47 (15.2) | 24 (35.3) | 35 (36.5) |
| 1b, N (%) | 24 (27.4) | 8 (11.8) | 53 (55.2) |
| 1c, N (%) | 81 (51.2) | 34 (50.0) | |
| Clinical stage | |||
| Stage IIIB, N (%) | 14 (8.9) | 5(7.4) | 8 (8.3) |
| Stage IVA, N (%) | 62 (39.2) | 30 (44.1) | 88 (91.7) |
| Stage IVB, N (%) | 82 (51.9) | 33 (48.5) | |
| EGFR mutation status | |||
| Exon 19 deletion, N (%) | 70 (44.3) | 31 (45.6) | 29 (30.2) |
| Exon 21 L858R substitution, N (%) | 77 (48.7) | 34 (50.0) | 46 (47.9) |
| Others, N (%) | 1 (7.0) | 3 (4.4) | 1(1) |
| None, N (%) | 0 (0) | 0 (0) | 24 (25) |
| TKI | |||
| Gefitinib, N (%) | 29 (18.4) | 9 (13.2) | NA |
| Erlotinib, N (%) | 45 (28.5) | 24 (35.3) | NA |
| Afatinib, N (%) | 84 (53.2) | 35 (51.5) | NA |
| Adverse drug reaction to EGFR-TKI | |||
| Yes, N (%) | 73 (46.2) | 32 (47.1) | NA |
| Progress free survival, median(months) | 12.4 (6.1–18.4) | 13.9 (6.2–18.4) | 10.5 (5.9–15.9) |
| Platelet | |||
| median (IQR) | 269,000 (230,250, 307,500) | 269,000 (226,750–306,000) | 277,000 (237,000–340,500) |
| Not available, N (%) | 13 (8.2) | 5 (7.4) | 10 (10.4) |
| Aspartate aminotransferase | |||
| median (IQR) | 23 (18–27) | 23 (18–27) | 23 (19–28) |
| Not available, N (%) | 60 (38) | 24 (35.3) | 19 (10.8) |
| Total protein | |||
| median (IQR) | 7.125 (6.8, 7.4) | 7.075 (6.8, 7.4) | 7.1 (6.8, 7.4) |
| Not available, N (%) | 112 (70.9) | 56 (82.4) | 71 (74.0) |
| PFS | Pretreatment Radiomics | Follow Up Radiomics | Delta Radiomics | Delta Time Radiomics | Delta log Time Radiomics | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Train | Valid | Train | Valid | Train | Valid | Train | Valid | Train | Valid | |
| C-index (95%CI) | 0.55 (0.55–0.56) | 0.55 (0.53–0.56) | 0.58 (0.58–0.59) | 0.56 (0.55–0.58) | 0.63 (0.62–0.63) | 0.57 (0.55–0.58) | 0.63 (0.63–0.64) | 0.58 (0.56–0.59) | 0.58 (0.57–0.5) | 0.57 (0.56–0.59) |
| t-AUC (95%CI) | 0.56 (0.55–0.56) | 0.55 (0.52–0.57) | 0.59 (0.58–0.59) | 0.56 (0.54–0.59) | 0.65 (0.64, 0.65) | 0.57 (0.54–0.59) | 0.66 (0.66–0.67) | 0.60 (0.58–0.62) | 0.57 (0.56–0.57) | 0.56 (0.54–0.58) |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| p-Value | HR (95%CI) | p-Value | HR (95%CI) | |
| N1 vs. N0 | 0.02 | 2.43 (1.17–5.07) | <0.005 | 2.71 (1.48–4.95) |
| N2 vs. N0 | 0.24 | 1.38 (0.8–2.37) | 0.12 | 1.42 (0.05–0.58) |
| N3 vs. N0 | <0.005 | 2.24 (1.40–3.59) | <0.005 | 1.92 (1.28–2.87) |
| N None vs. N0 | <0.54 | 1.57 (0.37–6.67) | 0.28 | 2.21 (0.53–9.31) |
| M | 0.01 | 1.29 (1.06–1.57) | <0.005 | 1.32 (1.12–1.56) |
| Platelet | <0.005 | 1.37 (1.11–1.70) | <0.005 | 1.36 (1.13–1.64) |
| Aspartate aminotransferase | <0.005 | 1.22 (1.07–1.38) | <0.005 | 1.31 (1.16–1.49) |
| Total protein | 0.08 | 0.84 (0.7–1.02) | <0.005 | 1.32 (1.12–1.56) |
| LHL_Run_Length_Nonuniformity | 0.03 | 4.46 (1.52–4960) | 0.02 | 198 (1.73–22,709) |
| LHH_Long_Run_Emphasis | <0.005 | 14.39 (6817–4.63 × 108) | <0.005 | 1.4 × 107 (3.8 × 104–5.1 × 109) |
| HLL_Variance | <0.005 | 12.57 (2.19–72.13) | <0.005 | 14.19 (3.48–57.89) |
| (a): Statistical comparisons between developed prediction models with radiomics features based on test dataset | ||||||
| Test set (n = 100) | Model performance | Pre Rad (c-index = 0.53) | Follow Rad (c-index = 0.55) | Delta Rad (c-index = 0.56) | tDelta Rad (c-index = 0.58) | tDelta log Rad (c-index = 0.54) |
| 6 month | Original AUC | 0.57 | 0.53 | 0.53 | 0.61 | 0.51 |
| AUC | 0.52 (0.51, 0.54) | 0.54 (0.52, 0.56) | 0.56 (0.54, 0.57) | 0.62 (0.60, 0.62) | 0.56 (0.54, 0.57) | |
| 9 month | Original AUC | 0.46 | 0.53 | 0.57 | 0.63 | 0.51 |
| AUC | 0.5 (0.49, 0.52) | 0.53 (0.51, 0.55) | 0.55 (0.53, 0.56) | 0.62 (0.62, 0.65) | 0.58 (0.57, 0.59) | |
| 12 month | Original AUC | 0.53 | 0.50 | 0.56 | 0.65 | 0.53 |
| AUC | 0.53 (0.51, 0.54) | 0.50 (0.48, 0.51) | 0.59 (0.58, 0.61) | 0.65 (0.64, 0.67) | 0.54 (0.53, 0.55) | |
| 15 month | Original AUC | 0.58 | 0.58 | 0.55 | 0.67 | 0.55 |
| AUC | 0.59 (0.58, 0.61) | 0.58 (0.56, 0.59) | 0.58 (0.56, 0.59) | 0.67 (0.65, 0.68) | 0.55 (0.54, 0.57) | |
| p-values | ||||||
| Pre rad vs. tDelta rad | Follow rad vs. tDelta rad | Delta rad vs. tDelta rad | tdelta log rad vs. tDelta rad | |||
| 6 month | <0.001 * | <0.001 * | <0.001 * | <0.001 * | ||
| 9 month | <0.001 * | <0.001 * | <0.001 * | <0.001 * | ||
| 12 month | <0.001 * | <0.001 * | <0.001 * | <0.001 * | ||
| 15 month | <0.001 * | <0.001 * | <0.001 * | <0.001 * | ||
| (b): Statistical comparisons between developed prediction models with the addition of clinical features based on test dataset | ||||||
| Test set (n = 100) | Model performance | Clinical (c-index = 0.66) | tDelta Rad (c-index = 0.58) | Clinical + tDelta Rad (c-index = 0.70) | p-values | |
| Clinical vs Clinical + delta rad | delta rad vs clinical + delta rad | |||||
| 6 month | Original AUC | 0.67 | 0.61 | 0.74 | <0.001 * | <0.001 * |
| AUC | 0.68 (0.67~0.70) | 0.62 (0.60, 0.62) | 0.74 (0.73, 0.76) | |||
| 9 month | Original AUC | 0.73 | 0.63 | 0.77 | <0.001 * | <0.001 * |
| AUC | 0.74 (0.73~0.75) | 0.62 (0.62, 0.65) | 0.78 (0.77, 0.79) | |||
| 12 month | Original AUC | 0.71 | 0.65 | 0.77 | <0.001 * | <0.001 * |
| AUC | 0.72 (0.71~0.73) | 0.65 (0.64, 0.67) | 0.78 (0.77, 0.79) | |||
| 15 month | Original AUC | 0.75 | 0.67 | 0.78 | <0.001 * | <0.001 * |
| AUC | 0.76 (0.75~0.77) | 0.67 (0.65, 0.68) | 0.79 (0.78, 0.81) | |||
| (c): Statistical comparisons between developed prediction models with the addition of clinical features based on combined test dataset | ||||||
| Test set (n = 100) | Model performance | Clinical (c-index = 0.66) | tDelta Rad (c-index = 0.53) | Clinical + tDelta Rad (c-index = 0.64) | p-values | |
| Clinical vs Clinical + delta rad | delta rad vs clinical + delta rad | |||||
| 6 month | Original AUC | 0.73 | 0.53 | 0.68 | <0.001 * | <0.001 * |
| AUC | 0.72 (0.71~0.73) | 0.53 (0.52, 055) | 0.68 (0.67, 0.70) | |||
| 9 month | Original AUC | 0.72 | 0.59 | 0.73 | 0.003 * | <0.001 * |
| AUC | 0.67 (0.65~0.68) | 0.59 (0.58, 0.60) | 0.67 (0.66, 0.69) | |||
| 12 month | Original AUC | 0.73 | 0.54 | 0.72 | <0.001 * | <0.001 * |
| AUC | 0.71 (0.70~0.72) | 0.53 (0.52, 0.54) | 0.66 (0.65, 0.68) | |||
| 15 month | Original AUC | 0.76 | 0.53 | 0.71 | <0.001 * | <0.001 * |
| AUC | 0.73 (0.72~0.74) | 0.54 (0.53, 0.55) | 0.68 (0.66, 0.69) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.-W.; Chao, H.-S.; Chiu, H.-Y.; Lin, Y.-H.; Chen, H.-C.; Lu, C.-F.; Liao, C.-Y.; Lee, Y.; Shiao, T.-H.; Chen, Y.-M.; et al. Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients. Cancers 2023, 15, 5125. https://doi.org/10.3390/cancers15215125
Wang T-W, Chao H-S, Chiu H-Y, Lin Y-H, Chen H-C, Lu C-F, Liao C-Y, Lee Y, Shiao T-H, Chen Y-M, et al. Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients. Cancers. 2023; 15(21):5125. https://doi.org/10.3390/cancers15215125
Chicago/Turabian StyleWang, Ting-Wei, Heng-Sheng Chao, Hwa-Yen Chiu, Yi-Hui Lin, Hung-Chun Chen, Chia-Feng Lu, Chien-Yi Liao, Yen Lee, Tsu-Hui Shiao, Yuh-Min Chen, and et al. 2023. "Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients" Cancers 15, no. 21: 5125. https://doi.org/10.3390/cancers15215125
APA StyleWang, T.-W., Chao, H.-S., Chiu, H.-Y., Lin, Y.-H., Chen, H.-C., Lu, C.-F., Liao, C.-Y., Lee, Y., Shiao, T.-H., Chen, Y.-M., Huang, J.-W., & Wu, Y.-T. (2023). Evaluating the Potential of Delta Radiomics for Assessing Tyrosine Kinase Inhibitor Treatment Response in Non-Small Cell Lung Cancer Patients. Cancers, 15(21), 5125. https://doi.org/10.3390/cancers15215125