

Artificial Intelligence in Digital Pathology for Bladder Cancer: Hype or Hope? A Systematic Review

 , , , , , , , and
, , , , , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
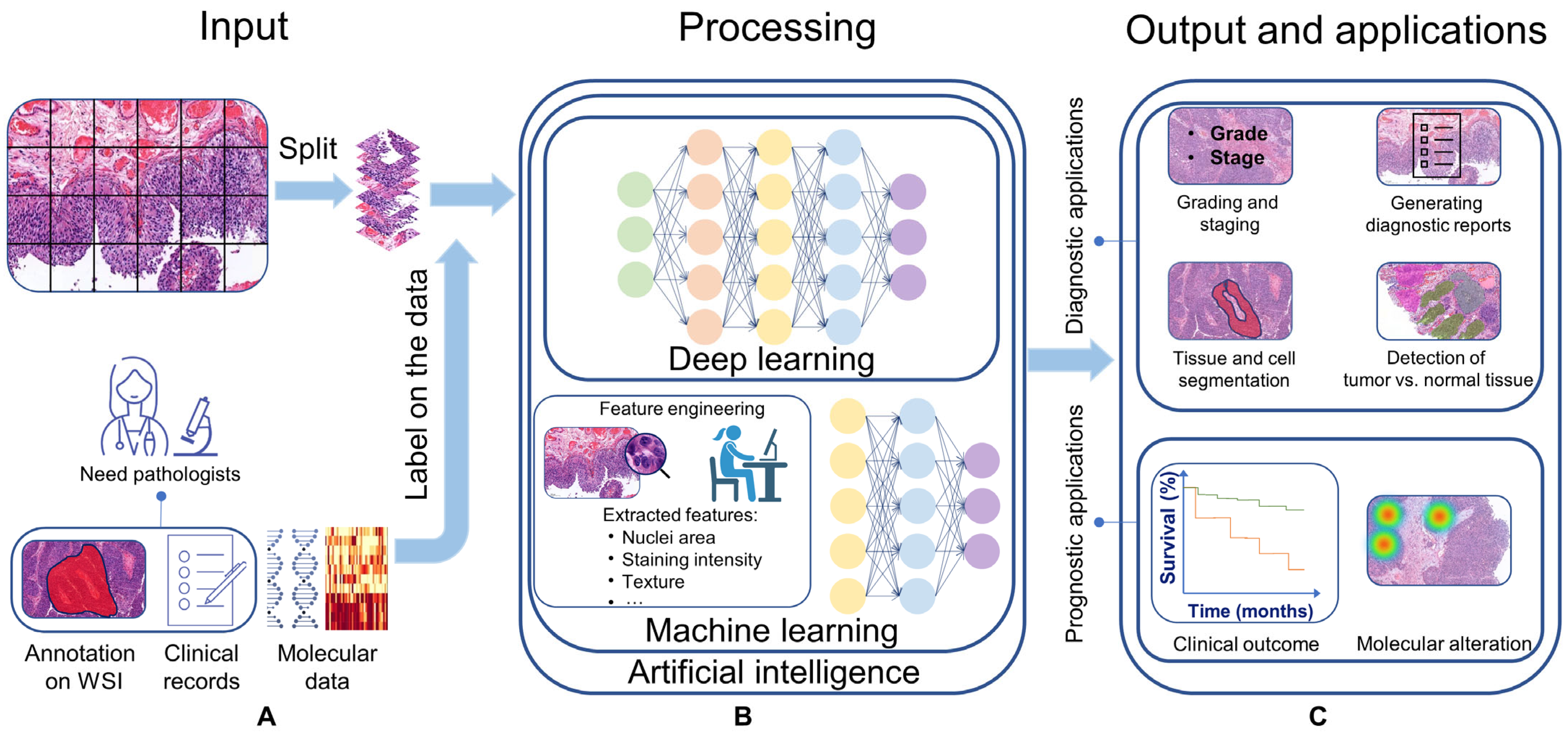
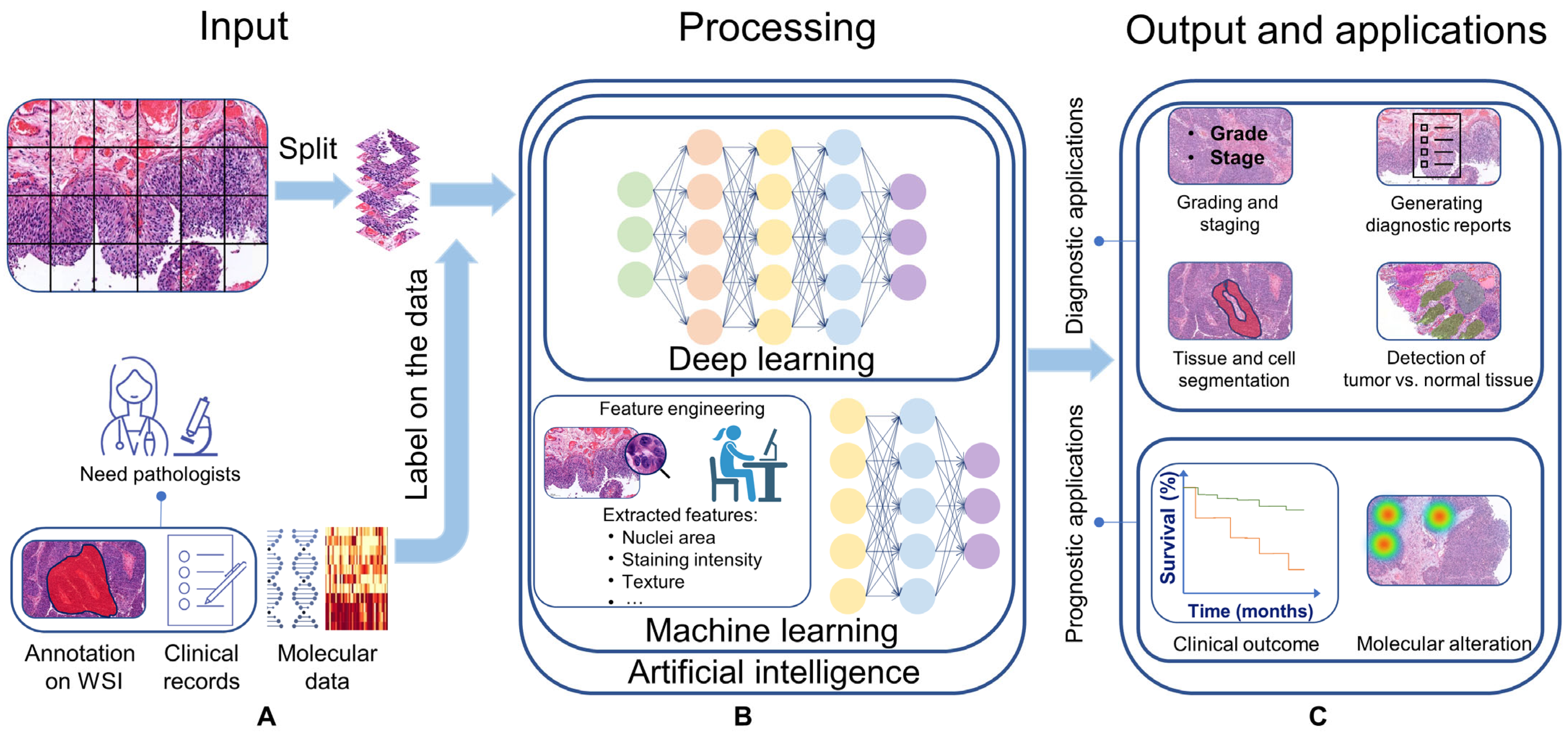
1.1. Artificial Intelligence
1.2. AI in BC Image Analysis
- Provide a comprehensive overview of the present BC CPATH landscape in diagnosis and prognosis;
- Highlight existing gaps between CPATH research and clinical practice;
- Offer recommendations to address these gaps;
- Discuss challenges that can shape future research in BC CPATH.
2. Materials and Methods
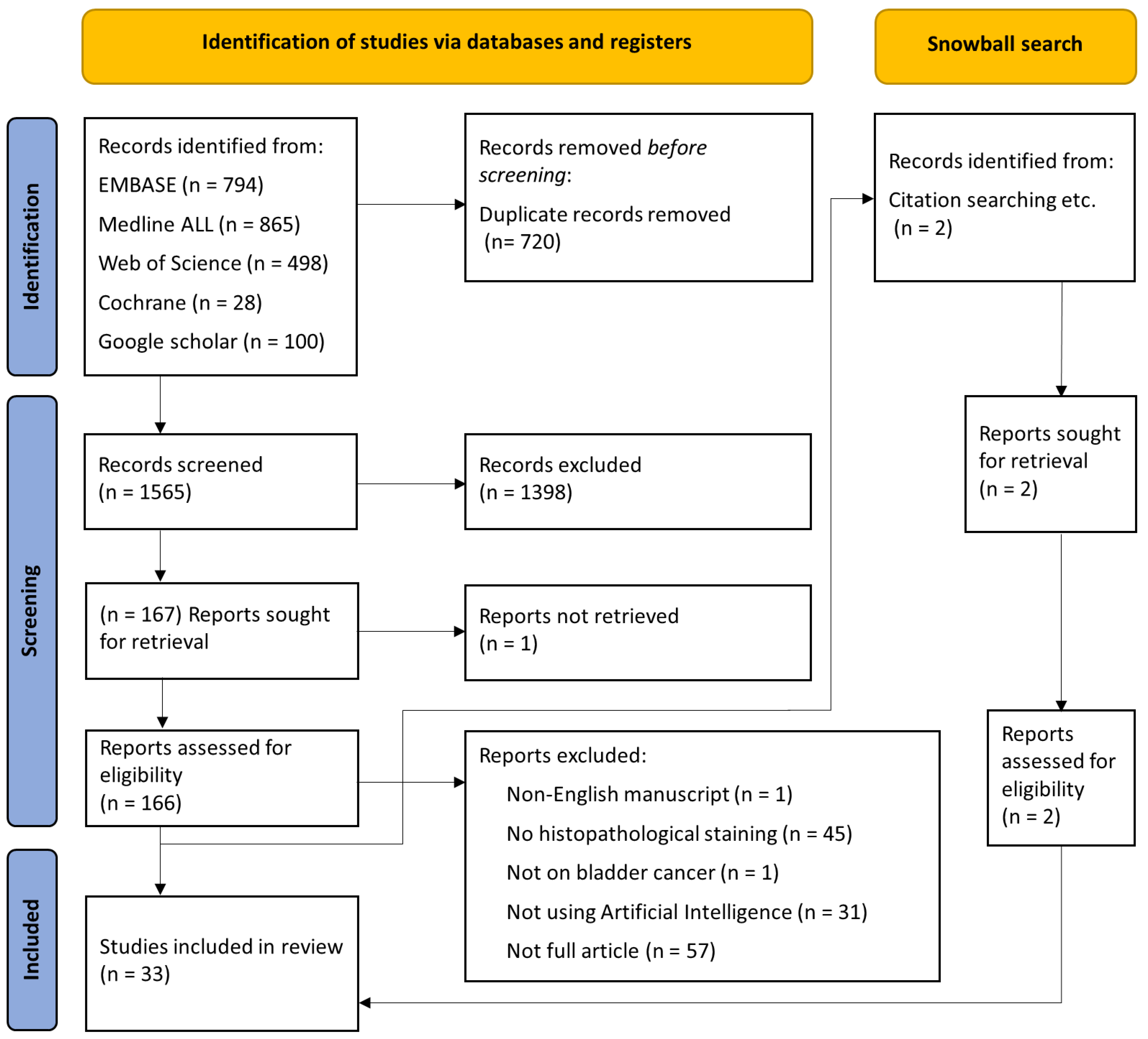
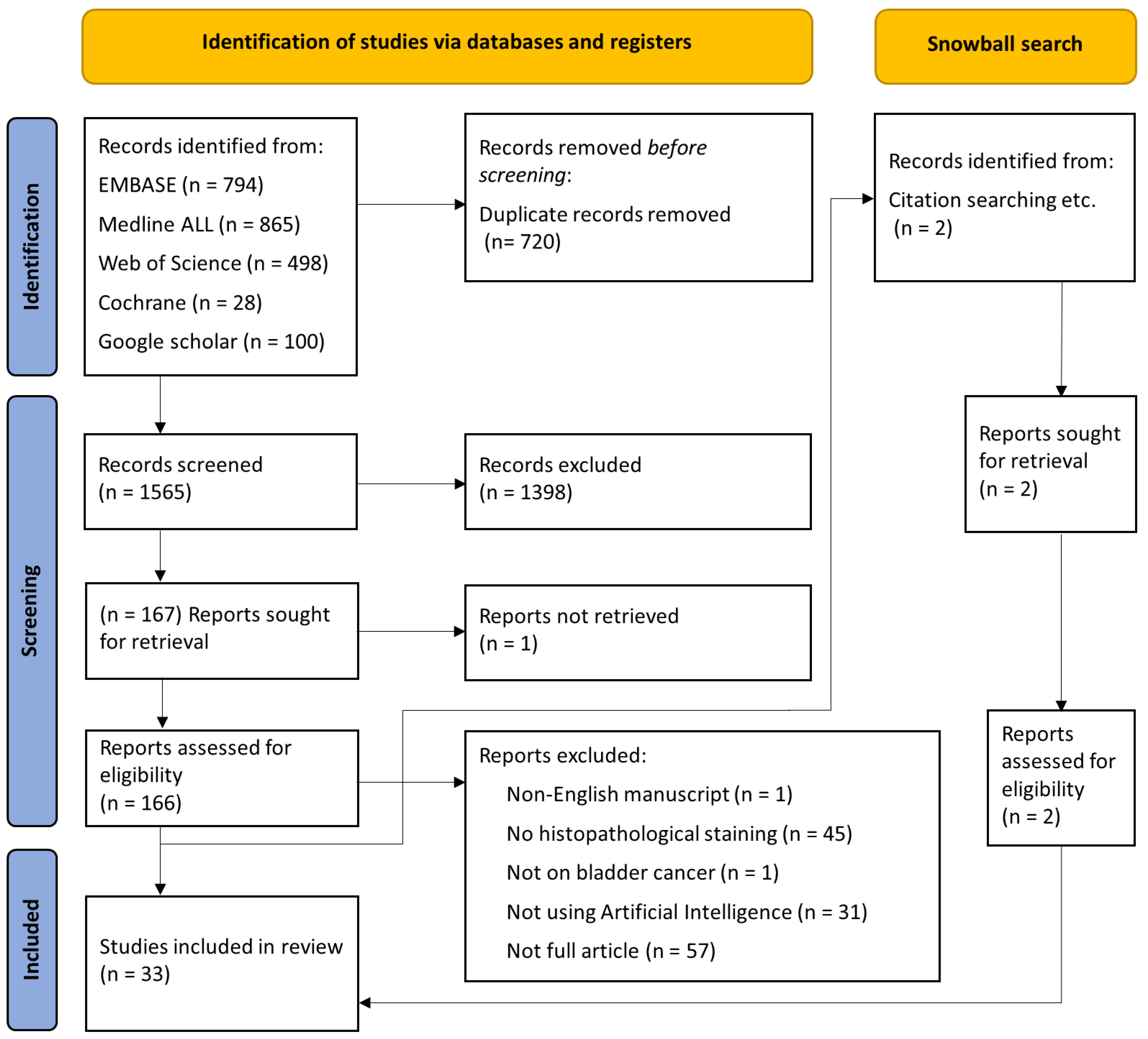
2.1. Literature Review
2.2. Study Eligibility and Selection
- i.
- No histopathological staining;
- ii.
- Not on bladder cancer;
- iii.
- Not using artificial intelligence;
- iv.
- No full article available;
- v.
- Non-English manuscript.
2.3. Data Extraction
2.4. Data Synthesis
3. Results
3.1. Literature Search
3.2. Applications of AI Methods for Diagnosis
3.2.1. Tissue and Cell Segmentation
3.2.2. Detection of Tumor vs. Normal Tissue
3.2.3. Grading and Staging
3.2.4. Generation of a Diagnostic Report
3.3. Applications of AI Methods for Prognosis
3.3.1. Predicting Clinical Outcome
3.3.2. Detection of Biomarkers and Molecular Alterations

{kind=link}
{kind=link}
| Study | Year | Aim of the Study (Related to AI Image Analysis on BC) | Diagnosis or Prognosis | Dataset | Number of Patients | Type of Model in Use | Staining Type |
|---|---|---|---|---|---|---|---|
| Niazi et al. [24] | 2020 | Tissue type segmentation (urothelium, stroma, muscle, and blood) | Diagnosis | In-house | 54 (T1 samples) | Supervised DL | HE |
| Wetteland et al. [28] | 2020 | Tissue type segmentation (urothelium, stroma, muscle, and blood) | Diagnosis | In-house | 39 | Supervised DL | HES |
| Loukas [29] | 2013 | Vessel segmentation | Diagnosis | In-house | 107 | Unsupervised ML | CD31 |
| Glotsos et al. [26] | 2004 | Cell nuclei segmentation (for selected urothelium regions) | Diagnosis | In-house | 50 | Supervised ML | HE |
| Zhang et al. [5] | 2019 | Detecting tumor area, grading classification, producing an interpretable pathology report | Diagnosis | TCGA, in-house | 913 | Supervised DL | HE |
| Jang et al. [32] | 2021 | Tissue classification into tumor vs. normal areas for six cancer types to assess the generalizability of diagnostic DL models. | Diagnosis | TCGA | NA | Supervised DL | HE |
| Kalra et al. [33] | 2020 | Pan-cancer classification with CBIR approach to assess diagnostic consensus through searching archival WSIs | Diagnosis | TCGA | 410 (before exclusion) | Unsupervised DL | HE |
| Yin et al. [37] | 2020 | Ta and T1 staging classification | Diagnosis | In-house | 1177 | Supervised ML | HE |
| Spyridonos et al. [39] | 2001 | Nuclei segmentation and tumor grading | Diagnosis | In-house | 92 | Supervised ML | HE |
| Spyridonos et al. [40] | 2002 | Nuclei segmentation and tumor grading | Diagnosis | In-house | 92 | Supervised ML | HE |
| Spyridonos et al. [41] | 2006 | Tumor grading | Diagnosis | In-house | 129 (NMIBC patients) | Supervised ML | HE |
| Papageorgiou et al. [42] | 2006 | Tumor grading | Diagnosis | In-house | 129 | Unsupervised and supervised ML | HE |
| Wetteland et al. [43] | 2021 | Tumor grading | Diagnosis | In-house | 300 (NMIBC patients) | Supervised DL | HE |
| Jansen et al. [44] | 2020 | Automated tumor detection and grading | Diagnosis | In-house | 232 (NMIBC patients) | Supervised DL | HE |
| García et al. [47] | 2021 | Detecting histological patterns (normal, mild, or trabecular in IHC images | Diagnosis | In-house | 136 | Unsupervised DL | IHC (Cytokeratin AE1/AE3) |
| Zhang et al. [48] | 2017 | Produce an interpretable pathology report for the corresponding ROI | Diagnosis | TCGA, in-house | 32 | Supervised DL | HE |
| Noorbakhsh et al. [31] | 2020 | Classifying tumor/non-tumor slides, cancer subtype, and TP53 mutation | Diagnosis and prognosis | TCGA | 27,815 a | Unsupervised DL | HE |
| Khosravi et al. [34] | 2018 | Tissue type (bladder, breast, and lung cancer) and biomarker classification | Diagnosis and prognosis | TCGA and TMAD | 2139 IHC, 543 H&E, and 2139 IHC images | Supervised DL | HE, IHC (CK14, GATA3, S0084, and S100P) |
| Brieu et al. [51] | 2019 | Detecting tumor budding to improve prognosis by predicting survival | prognosis | In-house | 100 | Supervised DL and ML | HE |
| Tasoulis et al. [52] | 2006 | Collecting and quantification of cell nuclei characteristics to improve prognosis by predicting recurrence | prognosis | In-house | 127 | Supervised ML | HE |
| Chen et al. [53] | 2021 | Predicting overall survival by using extracted quantitative phenotypic tissue features | prognosis | TCGA and in-house | 514 | Supervised ML | HE |
| Chen et al. [54] | 2021 | Provide a novel nomogram for decision-making and predicting overall survival by using extracted quantitative features and combining them with neutrophil-to-lymphocyte ratio information | prognosis | TCGA and in-house | 508 | Supervised ML | HE |
| Tokuyama et al. [55] | 2021 | Predict recurrence by using extracted quantitative nuclei features | prognosis | In-house | 125 (NMIBC patients) | Supervised ML | HE |
| Gavriel et al. [59] | 2021 | Predict cancer-specific survival by combining image, clinical and spatial features extracted from IHC images | prognosis | In-house | 78 | Supervised ML | IHC (Pan CK, CD3, CD8, CD68, CD163, PD-L1) |
| Mi et al. [60] | 2021 | Predict response to neoadjuvant chemotherapy by using extracted cell nuclei features | prognosis | TCGA and in-house | 73 | Supervised DL | HE, IHC (P16, P53, P63, Ki67, CK20, CK5/6, GATA3, and Her2Neu) |
| Lucas et al. [6] | 2020 | Predicting recurrence by combining image features with clinical information | prognosis | In-house | 359 | Unsupervised DL | HE |
| Harmon et al. [61] | 2020 | Predicting lymph node metastasis by combining extracted image features with a spatial tumor-infiltrating-lymphocytes probability model | prognosis | TCGA, in-house | 307 | Supervised DL and ML | HE |
| Woerl et al. [4] | 2019 | Predicting molecular subtypes from H&E slides | prognosis | TCGA, in-house | 379 | Supervised DL | HE |
| Lakshmi et al. [65] | 2019 | Estimating Ki-67 index by segmentation and classification of cell nuclei | prognosis | In-house | 8 b | Supervised DL | Ki-67 |
| Lakshmi et al. [25] | 2020 | Estimating Ki-67 index by segmentation and classification of cell nuclei, which use automatically labeled data | prognosis | In-house | 8 b | Supervised DL | HE |
| Saltz et al. [62] | 2018 | Mapping of tumor-infiltrating lymphocytes by training an algorithm that shows the representation of cell nuclei and lymphocytes, which is optimized with pathologist-labeled data | prognosis | TCGA | 5202 c | Supervised DL | HE |
| Velmahos et al. [70] | 2021 | Predicting FGFR mutation by estimating TILs proportion | prognosis | TCGA | 290 | Supervised DL | HE |
| Loeffler et al. [72] | 2021 | Detecting FGFR3 mutation from H&E images | prognosis | TCGA and in-house | 574 | Supervised DL | HE |
| Research Phase | Area to Improve | Recommendation | Reason |
|---|---|---|---|
| Data collection | Model robustness | Large number of patients (>100) | Avoid overfitting and develop accurate models |
| Open access resources | Publish WSI and annotation dataset publicly | Reproducible output | |
| Patient monitoring period | Period-covering follow-up | Cover the full timeframe to assess treatment efficacy | |
| Process uniformity | Standardization of data collection and keeping records of each step | Ensure consistency, reproducibility, and increase transparency for legal aspects | |
| Data pre-processing | Image dataset quality | Remove noise, such as artifacts, from the images | Increase generalizability and accuracy |
| Experiments and analysis | Study design transparency | Keep track of collection and adjustments made in the dataset, experiments, and algorithm | Reproducible study design and increase transparency for legal aspects |
| Transparent algorithm design | Publish the developed algorithm publicly | Reproducible output | |
| Results consistency and standardization | Report all basic results for classifications (e.g., accuracy, F1 score, AUC) | Make results comparable | |
| Cross-demographic algorithm evaluation | Further validation and testing of CPATH algorithms in diverse patient populations | ensure generalizability and accuracy | |
| Interpretation | Transparency in the decision-making process | Assess the outcome and interpret the rationale behind the decision an algorithm has made | Shed light on the black box for transparent and legally acceptable outcomes in clinical practice |
| Clinical implementation | Clinical utility and efficacy assessment | Implement trained models in the clinical setting | Integrating the AI models into the clinical workflow |
| Adaptive learning | Monitor the model’s performance and update it with new data | Maximize the model’s utility in real-world settings in varied scenarios |
4. Discussion
4.1. CPATH for BC Diagnosis
4.2. CPATH for BC Prediction of Prognosis
4.3. Navigating the Future: Challenges and Improvements in BC CPATH
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Bladder cancer |
| CPATH | Computational pathology |
| AI | Artificial intelligence |
| WSI | Whole-slide image |
| ML | Machine learning |
| DL | Deep learning |
| ROI | Region of interest |
| PRISMA | Preferred Reporting Items for Systematic Review and Meta-Analysis |
| H&E | Hematoxylin and eosin |
| AUC | Area under the curve |
| TB | Tumor budding |
| OS | Overall survival |
| CSS | Cancer-specific survival |
| MIBC | Muscle-invasive bladder cancer |
| NMIBC | Non-muscle-invasive bladder cancer |
| LNM | Lymph node metastasis |
| TILs | Tumor-infiltrating-lymphocytes |
| FGFR | Fibroblast growth factor receptor |
| BCG | Bacillus Calmette-Guérin |
References
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Van der Laak, J.; Litjens, G.; Ciompi, F. Deep learning in histopathology: The path to the clinic. Nat. Med. 2021, 27, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- Woerl, A.-C.; Eckstein, M.; Geiger, J.; Wagner, D.C.; Daher, T.; Stenzel, P.; Fernandez, A.; Hartmann, A.; Wand, M.; Roth, W.; et al. Deep Learning Predicts Molecular Subtype of Muscle-invasive Bladder Cancer from Conventional Histopathological Slides. Eur. Urol. 2020, 78, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Chen, P.; McGough, M.; Xing, F.; Wang, C.; Bui, M.; Xie, Y.; Sapkota, M.; Cui, L.; Dhillon, J.; et al. Pathologist-level interpretable whole-slide cancer diagnosis with deep learning. Nat. Mach. Intell. 2019, 1, 236–245. [Google Scholar] [CrossRef]
- Lucas, M.; Jansen, I.; van Leeuwen, T.G.; Oddens, J.R.; de Bruin, D.M.; Marquering, H.A. Deep Learning–based Recurrence Prediction in Patients with Non–muscle-invasive Bladder Cancer. Eur. Urol. Focus 2020, 8, 165–172. [Google Scholar] [CrossRef]
- Alloghani, M.; Al-Jumeily, D.; Mustafina, J.; Hussain, A.; Aljaaf, A.J. A Systematic Review on Supervised and Unsupervised Machine Learning Algorithms for Data Science. In Supervised and Unsupervised Learning for Data Science; Springer: Cham, Switzerland, 2019; pp. 3–21. [Google Scholar] [CrossRef]
- Serag, A.; Ion-Margineanu, A.; Qureshi, H.; McMillan, R.; Saint Martin, M.J.; Diamond, J.; O’Reilly, P.; Hamilton, P. Translational AI and Deep Learning in Diagnostic Pathology. Front. Med. 2019, 6, 185. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology guidelines on non–muscle-invasive bladder cancer (Ta, T1, and carcinoma in situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Kvikstad, V.; Mangrud, O.M.; Gudlaugsson, E.; Dalen, I.; Espeland, H.; Baak, J.P.A.; Janssen, E.A.M. Prognostic value and reproducibility of different microscopic characteristics in the WHO grading systems for pTa and pT1 urinary bladder urothelial carcinomas. Diagn. Pathol. 2019, 14, 90. [Google Scholar] [CrossRef]
- Engers, R. Reproducibility and reliability of tumor grading in urological neoplasms. World J. Urol. 2007, 25, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, G.S.; Hakenberg, O.W.; Gschwend, J.E.; Thalmann, G.; Kassouf, W.; Kamat, A.; Zlotta, A. An Updated Critical Analysis of the Treatment Strategy for Newly Diagnosed High-grade T1 (Previously T1G3) Bladder Cancer. Eur. Urol. 2010, 57, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Bonert, M.; Zafar, U.; Maung, R.; El-Shinnawy, I.; Naqvi, A.; Finley, C.; Cutz, J.-C.; Major, P.; Kapoor, A. Pathologist workload, work distribution and significant absences or departures at a regional hospital laboratory. PLoS ONE 2022, 17, e0265905. [Google Scholar] [CrossRef] [PubMed]
- Skrede, O.-J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestøl, K.; Maddison, J.; Askautrud, H.A.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep learning for prediction of colorectal cancer outcome: A discovery and validation study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef]
- Courtiol, P.; Maussion, C.; Moarii, M.; Pronier, E.; Pilcer, S.; Sefta, M.; Manceron, P.; Toldo, S.; Zaslavskiy, M.; Le Stang, N.; et al. Deep learning-based classification of mesothelioma improves prediction of patient outcome. Nat. Med. 2019, 25, 1519–1525. [Google Scholar] [CrossRef]
- Wang, Y.; Acs, B.; Robertson, S.; Liu, B.; Solorzano, L.; Wählby, C.; Hartman, J.; Rantalainen, M. Improved breast cancer histological grading using deep learning. Ann. Oncol. 2022, 33, 89–98. [Google Scholar] [CrossRef]
- FDA. FDA Authorizes Software that Can Help Identify Prostate Cancer. 2021. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-software-can-help-identify-prostate-cancer (accessed on 30 August 2023).
- Da Silva, L.M.; Pereira, E.M.; Salles, P.G.; Godrich, R.; Ceballos, R.; Kunz, J.D.; Casson, A.; Viret, J.; Chandarlapaty, S.; Ferreira, C.G.; et al. Independent real-world application of a clinical-grade automated prostate cancer detection system. J. Pathol. 2021, 254, 147–158. [Google Scholar] [CrossRef]
- Abels, E.; Pantanowitz, L.; Aeffner, F.; Zarella, M.D.; Laak, J.; Bui, M.M.; Vemuri, V.N.; Parwani, A.V.; Gibbs, J.; Agosto-Arroyo, E.; et al. Computational pathology definitions, best practices, and recommendations for regulatory guidance: A white paper from the Digital Pathology Association. J. Pathol. 2020, 249, 286–294. [Google Scholar] [CrossRef]
- Motterle, G.; Andrews, J.R.; Morlacco, A.; Karnes, R.J. Predicting Response to Neoadjuvant Chemotherapy in Bladder Cancer. Eur. Urol. Focus 2020, 6, 642–649. [Google Scholar] [CrossRef]
- Wong, V.K.; Ganeshan, D.; Jensen, C.T.; Devine, C.E. Imaging and Management of Bladder Cancer. Cancers 2021, 13, 1396. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Niazi, M.K.K.; Yazgan, E.; Tavolara, T.E.; Li, W.; Lee, C.T.; Parwani, A.; Gurcan, M.N. Semantic segmentation to identify bladder layers from H&E Images. Diagn. Pathol. 2020, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- Lakshmi, S.; Ritwik, K.V.S.; Vijayasenan, D.; Sumam, S.D.; Sreeram, S.; Suresh, P.K. Deep Learning Model based Ki-67 Index estimation with Automatically Labelled Data. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1412–1415. [Google Scholar] [CrossRef]
- Glotsos, D.; Spyridonos, P.; Cavouras, D.; Ravazoula, P.; Dadioti, P.-A.; Nikiforidis, G. Automated segmentation of routinely hematoxylin-eosin-stained microscopic images by combining support vector machine clustering and active contour models. Anal. Quant. Cytol. Histol. 2004, 26, 331–340. [Google Scholar]
- Raciti, P.; Sue, J.; Ceballos, R.; Godrich, R.; Kunz, J.D.; Kapur, S.; Reuter, V.; Grady, L.; Kanan, C.; Klimstra, D.S.; et al. Novel artificial intelligence system increases the detection of prostate cancer in whole slide images of core needle biopsies. Mod. Pathol. 2020, 33, 2058–2066. [Google Scholar] [CrossRef] [PubMed]
- Wetteland, R.; Engan, K.; Eftestøl, T.; Kvikstad, V.; Janssen, E.A.M. A Multiscale Approach for Whole-Slide Image Segmentation of five Tissue Classes in Urothelial Carcinoma Slides. Technol. Cancer Res. Treat. 2020, 19, 1533033820946787. [Google Scholar] [CrossRef]
- Loukas, C. Assessment of tumour angiogenesis in tissue section images based on a self-organising map (SOM). Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2013, 1, 111–118. [Google Scholar] [CrossRef]
- Bono, A.V.; Celato, N.; Cova, V.; Salvadore, M.; Chinetti, S.; Novario, R. Microvessel density in prostate carcinoma. Prostate Cancer Prostatic Dis. 2002, 5, 123–127. [Google Scholar] [CrossRef]
- Noorbakhsh, J.; Farahmand, S.; Pour, A.F.; Namburi, S.; Caruana, D.; Rimm, D.; Soltanieh-Ha, M.; Zarringhalam, K.; Chuang, J.H. Deep learning-based cross-classifications reveal conserved spatial behaviors within tumor histological images. Nat. Commun. 2020, 11, 6367. [Google Scholar] [CrossRef]
- Jang, H.-J.; Song, I.H.; Lee, S.H. Generalizability of Deep Learning System for the Pathologic Diagnosis of Various Cancers. Appl. Sci. 2021, 11, 808. [Google Scholar] [CrossRef]
- Kalra, S.; Tizhoosh, H.R.; Shah, S.; Choi, C.; Damaskinos, S.; Safarpoor, A.; Shafiei, S.; Babaie, M.; Diamandis, P.; Campbell, C.J.V.; et al. Pan-cancer diagnostic consensus through searching archival histopathology images using artificial intelligence. npj Digit. Med. 2020, 3, 31. [Google Scholar] [CrossRef]
- Khosravi, P.; Kazemi, E.; Imielinski, M.; Elemento, O.; Hajirasouliha, I. Deep Convolutional Neural Networks Enable Discrimination of Heterogeneous Digital Pathology Images. eBioMedicine 2018, 27, 317–328. [Google Scholar] [CrossRef]
- Kamat, A.M.; Li, R.; O’Donnell, M.A.; Black, P.C.; Roupret, M.; Catto, J.W.; Comperat, E.; Ingersoll, M.A.; Witjes, W.P.; McConkey, D.J.; et al. Predicting response to intravesical Bacillus Calmette-Guérin immunotherapy: Are we there yet? A systematic review. Eur. Urol. 2018, 73, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Fuster, S.; Khoraminia, F.; Kiraz, U.; Kanwal, N.; Kvikstad, V.; Eftestol, T.; Zuiverloon, T.C.; Janssen, E.A.; Engan, K. Invasive Cancerous Area Detection in Non-Muscle Invasive Bladder Cancer Whole Slide Images. In Proceedings of the 2022 IEEE 14th Image, Video, and Multidimensional Signal Processing Workshop (IVMSP), Nafplio, Greece, 26–29 June 2022; pp. 1–5. [Google Scholar] [CrossRef]
- Yin, P.-N.; Kc, K.; Wei, S.; Yu, Q.; Li, R.; Haake, A.R.; Miyamoto, H.; Cui, F. Histopathological distinction of non-invasive and invasive bladder cancers using machine learning approaches. BMC Med. Inform. Decis. Mak. 2020, 20, 162. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Spyridonos, P.; Ravazoula, D.; Cavouras, K.; Berberidis, G.; Nikiforidis, P. Computer-based grading of haematoxylin-eosin stained tissue sections of urinary bladder carcinomas. Med. Inform. Internet Med. 2001, 26, 179–190. [Google Scholar] [CrossRef]
- Spyridonos, P.; Cavouras, D.; Ravazoula, P.; Nikiforidis, G. Neural network-based segmentation and classification system for automated grading of histologic sections of bladder carcinoma. Anal. Quant. Cytol. Histol. 2002, 24, 317–324. [Google Scholar]
- Spyridonos, P.; Petalas, P.; Glotsos, D.; Cavouras, D.; Ravazoula, P.; Nikiforidis, G. Comparative evaluation of support vector machines and probabilistic neural networks in superficial bladder cancer classification. J. Comput. Methods Sci. Eng. 2006, 6, 283–292. [Google Scholar] [CrossRef]
- Papageorgiou, E.; Georgoulas, G.; Stylios, C.; Nikiforidis, G.; Groumpos, P. Combining Fuzzy Cognitive Maps with Support Vector Machines for Bladder Tumor Grading. In Knowledge-Based Intelligent Information and Engineering Systems; Pt 1, Proceedings; Springer: Berlin/Heidelberg, Germany, 2006; pp. 515–523. [Google Scholar] [CrossRef]
- Wetteland, R.; Kvikstad, V.; Eftestol, T.; Tossebro, E.; Lillesand, M.; Janssen, E.A.M.; Engan, K. Automatic Diagnostic Tool for Predicting Cancer Grade in Bladder Cancer Patients Using Deep Learning. IEEE Access 2021, 9, 115813–115825. [Google Scholar] [CrossRef]
- Jansen, I.; Lucas, M.; Bosschieter, J.; de Boer, O.J.; Meijer, S.L.; van Leeuwen, T.G.; Marquering, H.A.; Nieuwenhuijzen, J.A.; de Bruin, D.M.; Savci-Heijink, C.D. Automated Detection and Grading of Non–Muscle-Invasive Urothelial Cell Carcinoma of the Bladder. Am. J. Pathol. 2020, 190, 1483–1490. [Google Scholar] [CrossRef]
- Eckstein, M.; Matek, C.; Wagner, P.; Erber, R.; Büttner-Herold, M.; Wild, P.J.; Taubert, H.; Wach, S.; Sikic, D.; Wullich, B.; et al. Proposal for a Novel Histological Scoring System as a Potential Grading Approach for Muscle-invasive Urothelial Bladder Cancer Correlating with Disease Aggressiveness and Patient Outcomes. Eur. Urol. Oncol. 2023. advance online publication. [Google Scholar] [CrossRef]
- Jimenez, R.E.; Gheiler, E.; Oskanian, P.; Tiguert, R.; Sakr, W.; Wood, D.P., Jr.; Pontes, J.E.; Grignon, D.J. Grading the Invasive Component of Urothelial Carcinoma of the Bladder and Its Relationship with Progression-Free Survival. Am. J. Surg. Pathol. 2000, 24, 980–987. [Google Scholar] [CrossRef] [PubMed]
- García, G.; Esteve, A.; Colomer, A.; Ramos, D.; Naranjo, V. A novel self-learning framework for bladder cancer grading using histopathological images. Comput. Biol. Med. 2021, 138, 104932. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xie, Y.; Xing, F.; McGough, M.; Yang, L. MDNet: A Semantically and Visually Interpretable Medical Image Diagnosis Network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 6428–6436. [Google Scholar] [CrossRef]
- Martin-Doyle, W.; Leow, J.J.; Orsola, A.; Chang, S.L.; Bellmunt, J. Faculty Opinions recommendation of Improving selection criteria for early cystectomy in high-grade t1 bladder cancer: A meta-analysis of 15,215 patients. J. Clin. Oncol. 2018, 33, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Ghoneim, M.A.; Abdel-Latif, M.; El-Mekresh, M.; Abol-Enein, H.; Mosbah, A.; Ashamallah, A.; El-Baz, M.A. Radical Cystectomy for Carcinoma of the Bladder: 2,720 Consecutive Cases 5 Years Later. J. Urol. 2008, 180, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Brieu, N.; Gavriel, C.G.; Nearchou, I.P.; Harrison, D.J.; Schmidt, G.; Caie, P.D. Automated tumour budding quantification by machine learning augments TNM staging in muscle-invasive bladder cancer prognosis. Sci. Rep. 2019, 9, 5174. [Google Scholar] [CrossRef]
- Tasoulis, D.K.; Spyridonos, P.; Pavlidis, N.G.; Plagianakos, V.P.; Ravazoula, P.; Nikiforidis, G.; Vrahatis, M.N. Cell-nuclear data reduction and prognostic model selection in bladder tumor recurrence. Artif. Intell. Med. 2006, 38, 291–303. [Google Scholar] [CrossRef]
- Chen, S.; Jiang, L.; Zheng, X.; Shao, J.; Wang, T.; Zhang, E.; Gao, F.; Wang, X.; Zheng, J. Clinical use of machine learning-based pathomics signature for diagnosis and survival prediction of bladder cancer. Cancer Sci. 2021, 112, 2905–2914. [Google Scholar] [CrossRef]
- Chen, S.; Jiang, L.; Zhang, E.; Hu, S.; Wang, T.; Gao, F.; Zhang, N.; Wang, X.; Zheng, J. A Novel Nomogram Based on Machine Learning-Pathomics Signature and Neutrophil to Lymphocyte Ratio for Survival Prediction of Bladder Cancer Patients. Front. Oncol. 2021, 11, 703033. [Google Scholar] [CrossRef]
- Tokuyama, N.; Saito, A.; Muraoka, R.; Matsubara, S.; Hashimoto, T.; Satake, N.; Matsubayashi, J.; Nagao, T.; Mirza, A.H.; Graf, H.-P.; et al. Prediction of non-muscle invasive bladder cancer recurrence using machine learning of quantitative nuclear features. Mod. Pathol. 2022, 35, 533–538. [Google Scholar] [CrossRef]
- Karamitopoulou, E.; Zlobec, I.; Born, D.; Kondi-Pafiti, A.; Lykoudis, P.; Mellou, A.; Gennatas, K.; Gloor, B.; Lugli, A. Tumour budding is a strong and independent prognostic factor in pancreatic cancer. Eur. J. Cancer 2013, 49, 1032–1039. [Google Scholar] [CrossRef]
- Van Wyk, H.C.; Park, J.H.; Edwards, J.; Horgan, P.G.; McMillan, D.C.; Going, J.J. The relationship between tumour budding, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Br. J. Cancer 2016, 115, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Zink, D.; Fischer, A.H.; Nickerson, J.A. Nuclear structure in cancer cells. Nature reviews. Cancer 2004, 4, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Gavriel, C.G.; Dimitriou, N.; Brieu, N.; Nearchou, I.P.; Arandjelović, O.; Schmidt, G.; Harrison, D.J.; Caie, P.D. Assessment of Immunological Features in Muscle-Invasive Bladder Cancer Prognosis Using Ensemble Learning. Cancers 2021, 13, 1624. [Google Scholar] [CrossRef] [PubMed]
- Mi, H.; Bivalacqua, T.J.; Kates, M.; Seiler, R.; Black, P.C.; Popel, A.S.; Baras, A.S. Predictive models of response to neoadjuvant chemotherapy in muscle-invasive bladder cancer using nuclear morphology and tissue architecture. Cell Rep. Med. 2021, 2, 100382. [Google Scholar] [CrossRef]
- Harmon, S.; Sanford, T.; Daneshvar, M.; Brown, G.T.; Yang, C.; Mehralivand, S.; Shih, J.; Jacob, J.; Valera, V.; Agarwal, P.; et al. PD47-10 Multiresolution Application of artificial intelligence in digital pathology for prediction of positive lymph nodes from primary tumors in bladder cancer. J. Urol. 2020, 203, e929. [Google Scholar] [CrossRef]
- Saltz, J.; Gupta, R.; Hou, L.; Kurc, T.; Singh, P.; Nguyen, V.; Samaras, D.; Shroyer, K.R.; Zhao, T.; Batiste, R.; et al. Spatial Organization and Molecular Correlation of Tumor-Infiltrating Lymphocytes Using Deep Learning on Pathology Images. Cell Rep. 2018, 23, 181–193.e7. [Google Scholar] [CrossRef]
- Miyamoto, D.T.; Mouw, K.W.; Feng, F.Y.; Shipley, W.U.; Efstathiou, J.A. Molecular biomarkers in bladder preservation therapy for muscle-invasive bladder cancer. Lancet Oncol. 2018, 19, e683–e695. [Google Scholar] [CrossRef]
- Rose, T.L.; Weir, W.H.; Mayhew, G.M.; Shibata, Y.; Eulitt, P.; Uronis, J.M.; Zhou, M.; Nielsen, M.; Smith, A.B.; Woods, M.; et al. Fibroblast growth factor receptor 3 alterations and response to immune checkpoint inhibition in metastatic urothelial cancer: A real world experience. Br. J. Cancer 2021, 125, 1251–1260. [Google Scholar] [CrossRef]
- Lakshmi, S.; Vijayasenan, D.; Sumam, D.S.; Sreeram, S.; Suresh, P.K. An Integrated Deep Learning Approach towards Automatic Evaluation of Ki-67 Labeling Index. In Proceedings of the 2019 IEEE Region 10 Conference, IEEE, New York, NY, USA, 17–20 October 2019; pp. 2310–2314. [Google Scholar] [CrossRef]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.; Winters, B.; Douglas, J.; Van Kessel, K.E.; van de Putte, E.E.F.; Summerland, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef]
- Fong, M.H.Y.; Feng, M.; McConkey, D.J.; Choi, W. Update on bladder cancer molecular subtypes. Transl. Androl. Urol. 2020, 9, 2881–2889. [Google Scholar] [CrossRef]
- Kamoun, A.; de Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef]
- Ascione, C.M.; Napolitano, F.; Esposito, D.; Servetto, A.; Belli, S.; Santaniello, A.; Scagliarini, S.; Crocetto, F.; Bianco, R.; Formisano, L. Role of FGFR3 in bladder cancer: Treatment landscape and future challenges. Cancer Treat. Rev. 2023, 115, 102530. [Google Scholar] [CrossRef] [PubMed]
- Velmahos, C.S.; Badgeley, M.; Lo, Y.-C. Using deep learning to identify bladder cancers with FGFR -activating mutations from histology images. Cancer Med. 2021, 10, 4805–4813. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.A.; Sweis, R.F.; Bao, R.; Luke, J.J. T Cell–Inflamed versus Non-T Cell–Inflamed Tumors: A Conceptual Framework for Cancer Immunotherapy Drug Development and Combination Therapy Selection. Cancer Immunol. Res. 2018, 6, 990–1000. [Google Scholar] [CrossRef]
- Loeffler, C.M.; Bruechle, N.O.; Jung, M.; Seillier, L.; Rose, M.; Laleh, N.G.; Knuechel, R.; Brinker, T.J.; Trautwein, C.; Gaisa, N.T.; et al. Artificial Intelligence–based Detection of FGFR3 Mutational Status Directly from Routine Histology in Bladder Cancer: A Possible Preselection for Molecular Testing? Eur. Urol. Focus 2021, 8, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Kanwal, N.; Fuster, S.; Khoraminia, F.; Zuiverloon, T.C.; Rong, C.; Engan, K. Quantifying the effect of color processing on blood and damaged tissue detection in Whole Slide Images. In Proceedings of the 2022 IEEE 14th Image, Video, and Multidimensional Signal Processing Workshop (IVMSP), Nafplio, Greece, 26–29 June 2022; pp. 1–5. [Google Scholar] [CrossRef]
- Lu, M.Y.; Williamson, D.F.K.; Chen, T.Y.; Chen, R.J.; Barbieri, M.; Mahmood, F. Data-efficient and weakly supervised computational pathology on whole-slide images. Nat. Biomed. Eng. 2021, 5, 555–570. [Google Scholar] [CrossRef]
- Campanella, G.; Hanna, M.G.; Geneslaw, L.; Miraflor, A.; Silva, V.W.K.; Busam, K.J.; Brogi, E.; Reuter, V.E.; Klimstra, D.S.; Fuchs, T.J. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat. Med. 2019, 25, 1301–1309. [Google Scholar] [CrossRef]
- Baruah, A.; Bhuyan, G.; Saikia, P. Histopathological categorization of desmoplastic reaction in gallbladder carcinoma: Its relation to cancer invasiveness and prognostic utility. Egypt. Liver J. 2023, 13, 19. [Google Scholar] [CrossRef]
- Ueno, H.; Ishiguro, M.; Nakatani, E.; Ishikawa, T.; Uetake, H.; Murotani, K.; Matsui, S.; Teramukai, S.; Sugai, T.; Ajioka, Y.; et al. Prognostic value of desmoplastic reaction characterisation in stage II colon cancer: Prospective validation in a Phase 3 study (SACURA Trial). Br. J. Cancer 2021, 124, 1088–1097. [Google Scholar] [CrossRef]
- Ibrahim, A.; Lashen, A.G.; Katayama, A.; Mihai, R.; Ball, G.; Toss, M.S.; Rakha, E.A. Defining the area of mitoses counting in invasive breast cancer using whole slide image. Mod. Pathol. 2022, 35, 739–748. [Google Scholar] [CrossRef]
- Zaleski, M.; Gogoj, A.; Walter, V.; Raman, J.D.; Kaag, M.; Merrill, S.B.; Drabick, J.; Joshi, M.; Holder, S.; DeGraff, D.J.; et al. Mitotic activity in noninvasive papillary urothelial carcinoma: Its value in predicting tumor recurrence and comparison with the contemporary 2-tier grading system. Hum. Pathol. 2019, 84, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Kashani-Sabet, M.; Miller, J.R.; Lo, S.; Nosrati, M.; Stretch, J.R.; Shannon, K.F.; Spillane, A.J.; Saw, R.P.M.; Cleaver, J.E.; Kim, K.B.; et al. Reappraisal of the prognostic significance of mitotic rate supports its reincorporation into the melanoma staging system. Cancer 2020, 126, 4717–4725. [Google Scholar] [CrossRef] [PubMed]
- Sturm, B.; Creytens, D.; Smits, J.; Ooms, A.H.A.G.; Eijken, E.; Kurpershoek, E.; Küsters-Vandevelde, H.V.N.; Wauters, C.; Blokx, W.A.M.; van der Laak, J.A.W.M. Computer-Aided Assessment of Melanocytic Lesions by Means of a Mitosis Algorithm. Diagnostics 2022, 12, 436. [Google Scholar] [CrossRef] [PubMed]
- Jaroensri, R.; Wulczyn, E.; Hegde, N.; Brown, T.; Flament-Auvigne, I.; Tan, F.; Cai, Y.; Nagpal, K.; Rakha, E.A.; Dabbs, D.J.; et al. Deep learning models for histologic grading of breast cancer and association with disease prognosis. Npj Breast Cancer 2022, 8, 113. [Google Scholar] [CrossRef]
- Slotman, A.; Xu, M.; Lindale, K.; Hardy, C.; Winkowski, D.; Baird, R.; Chen, L.; Lal, P.; van der Kwast, T.; Jackson, C.L.; et al. Quantitative Nuclear Grading: An Objective, Artificial Intelligence–Facilitated Foundation for Grading Noninvasive Papillary Urothelial Carcinoma. Lab. Investig. 2023, 103, 100155. [Google Scholar] [CrossRef]
- Yu, K.-H.; Zhang, C.; Berry, G.J.; Altman, R.B.; Ré, C.; Rubin, D.L.; Snyder, M. Predicting non-small cell lung cancer prognosis by fully automated microscopic pathology image features. Nat. Commun. 2016, 7, 12474. [Google Scholar] [CrossRef]
- Chen, R.J.; Lu, M.Y.; Wang, J.; Williamson, D.F.K.; Rodig, S.J.; Lindeman, N.I.; Mahmood, F. Pathomic Fusion: An Integrated Framework for Fusing Histopathology and Genomic Features for Cancer Diagnosis and Prognosis. IEEE Trans. Med. Imaging 2020, 41, 757–770. [Google Scholar] [CrossRef]
- Liu, H.; Xu, W.-D.; Shang, Z.-H.; Wang, X.-D.; Zhou, H.-Y.; Ma, K.-W.; Zhou, H.; Qi, J.-L.; Jiang, J.-R.; Tan, L.-L.; et al. Breast Cancer Molecular Subtype Prediction on Pathological Images with Discriminative Patch Selection and Multi-Instance Learning. Front. Oncol. 2022, 12, 858453. [Google Scholar] [CrossRef]
- Wu, S.; Hong, G.; Xu, A.; Zeng, H.; Chen, X.; Wang, Y.; Luo, Y.; Wu, P.; Liu, C.; Jiang, N.; et al. Artificial intelligence-based model for lymph node metastases detection on whole slide images in bladder cancer: A retrospective, multicentre, diagnostic study. Lancet Oncol. 2023, 24, 360–370. [Google Scholar] [CrossRef]
- Dehkharghanian, T.; Bidgoli, A.A.; Riasatian, A.; Mazaheri, P.; Campbell, C.J.V.; Pantanowitz, L.; Tizhoosh, H.R.; Rahnamayan, S. Biased data, biased AI: Deep networks predict the acquisition site of TCGA images. Diagn. Pathol. 2023, 18, 67. [Google Scholar] [CrossRef]
- Mazaheri, P.; Bidgoli, A.A.; Rahnamayan, S.; Tizhoosh, H. Ranking loss and sequestering learning for reducing image search bias in histopathology. Appl. Soft Comput. 2023, 142, 110346. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khoraminia, F.; Fuster, S.; Kanwal, N.; Olislagers, M.; Engan, K.; van Leenders, G.J.L.H.; Stubbs, A.P.; Akram, F.; Zuiverloon, T.C.M. Artificial Intelligence in Digital Pathology for Bladder Cancer: Hype or Hope? A Systematic Review. Cancers 2023, 15, 4518. https://doi.org/10.3390/cancers15184518
Khoraminia F, Fuster S, Kanwal N, Olislagers M, Engan K, van Leenders GJLH, Stubbs AP, Akram F, Zuiverloon TCM. Artificial Intelligence in Digital Pathology for Bladder Cancer: Hype or Hope? A Systematic Review. Cancers. 2023; 15(18):4518. https://doi.org/10.3390/cancers15184518
Chicago/Turabian StyleKhoraminia, Farbod, Saul Fuster, Neel Kanwal, Mitchell Olislagers, Kjersti Engan, Geert J. L. H. van Leenders, Andrew P. Stubbs, Farhan Akram, and Tahlita C. M. Zuiverloon. 2023. "Artificial Intelligence in Digital Pathology for Bladder Cancer: Hype or Hope? A Systematic Review" Cancers 15, no. 18: 4518. https://doi.org/10.3390/cancers15184518
APA StyleKhoraminia, F., Fuster, S., Kanwal, N., Olislagers, M., Engan, K., van Leenders, G. J. L. H., Stubbs, A. P., Akram, F., & Zuiverloon, T. C. M. (2023). Artificial Intelligence in Digital Pathology for Bladder Cancer: Hype or Hope? A Systematic Review. Cancers, 15(18), 4518. https://doi.org/10.3390/cancers15184518