
Survival Prediction of Patients with Bladder Cancer after Cystectomy Based on Clinical, Radiomics, and Deep-Learning Descriptors

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
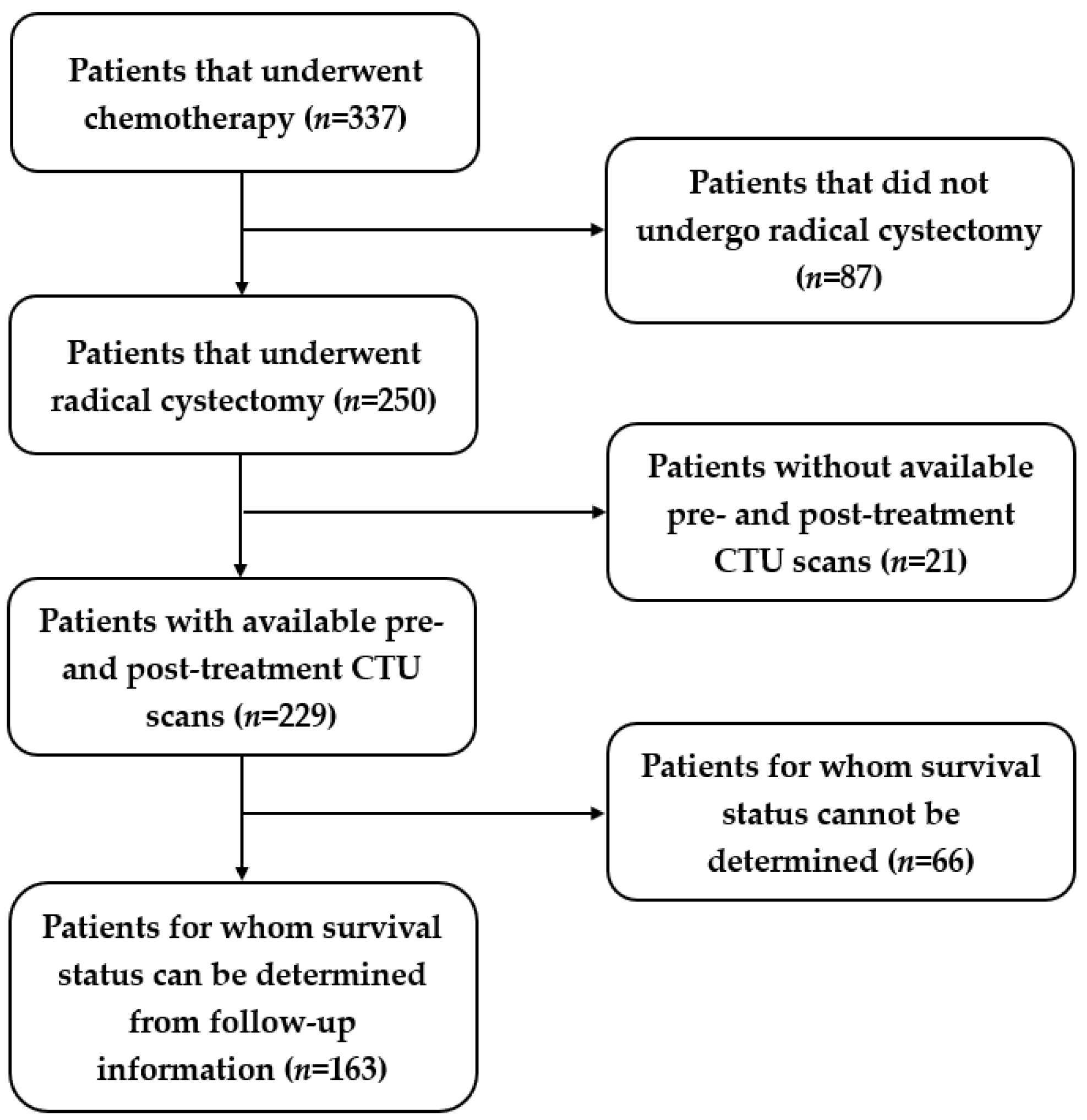
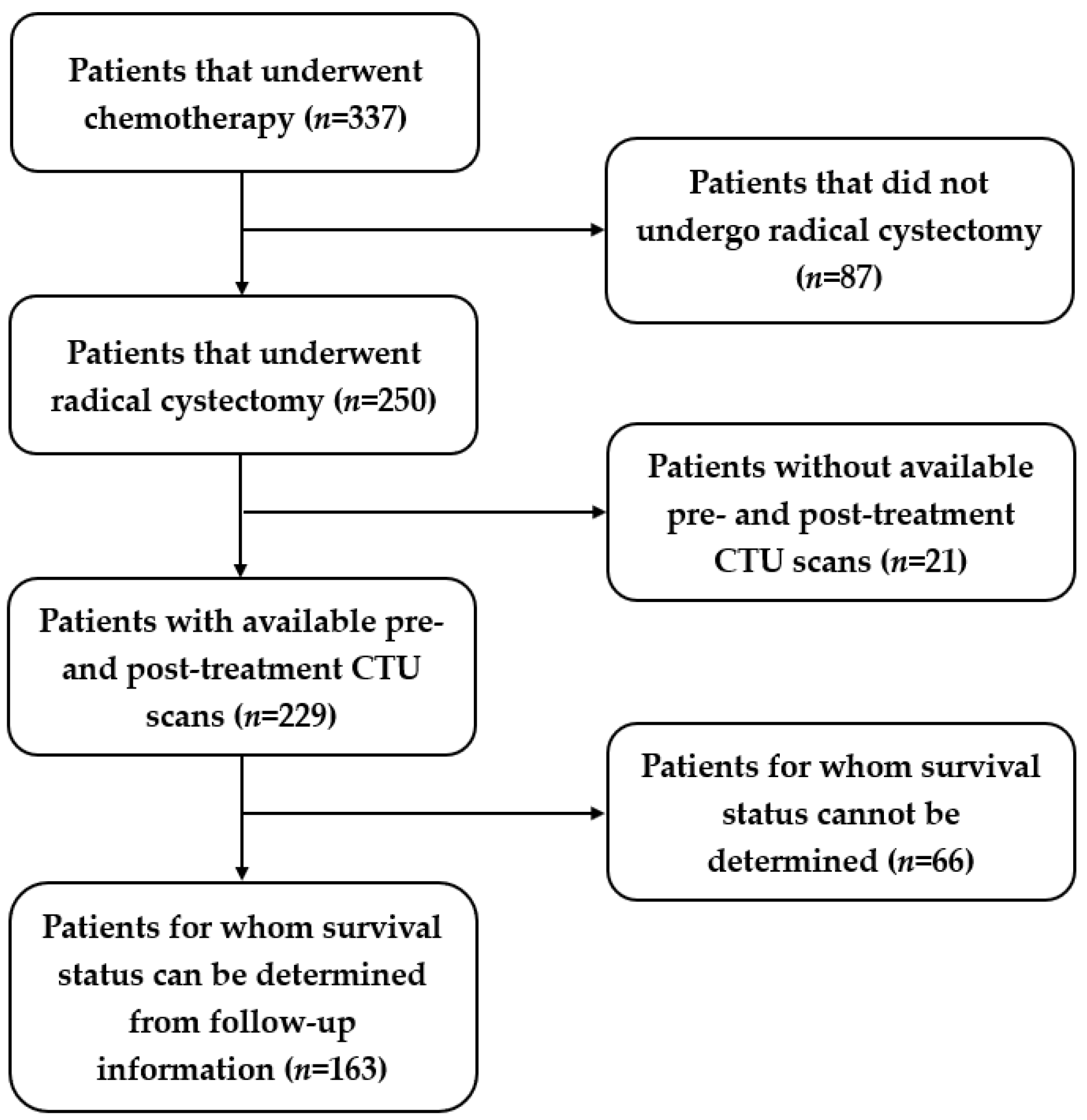
2.1. Patient Cohorts
2.2. Nomogram
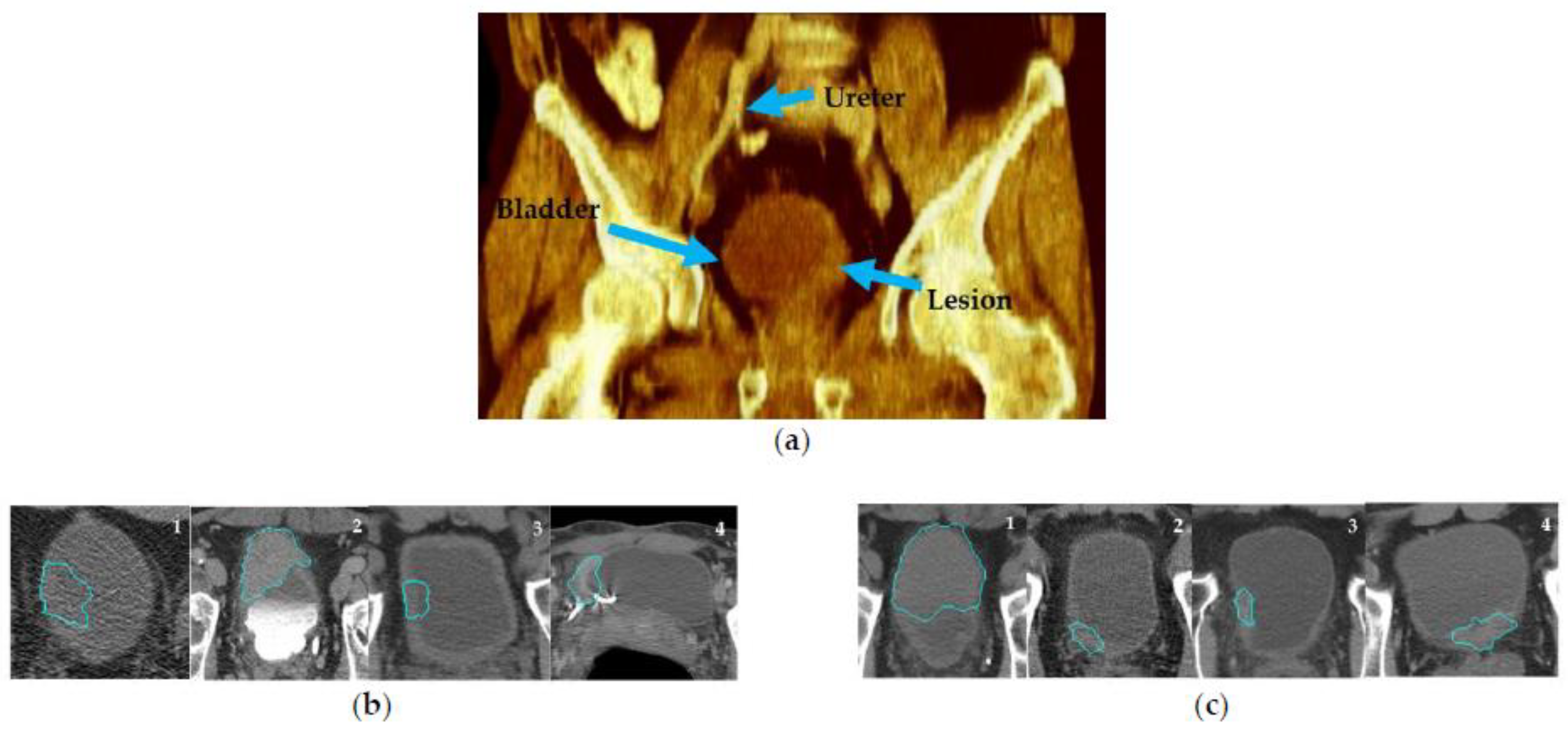
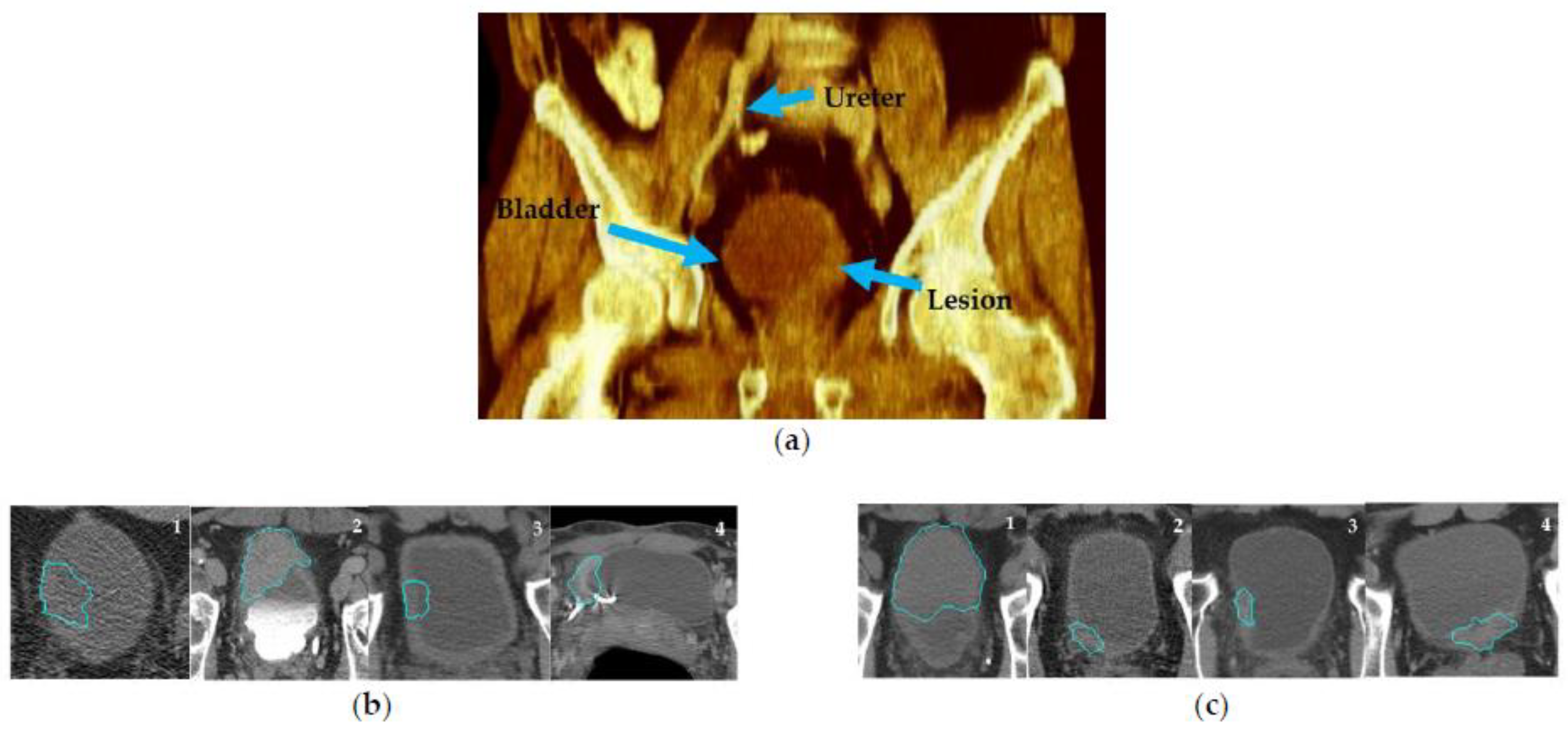
2.3. CTU Scans Processing
2.4. Radiomics Model
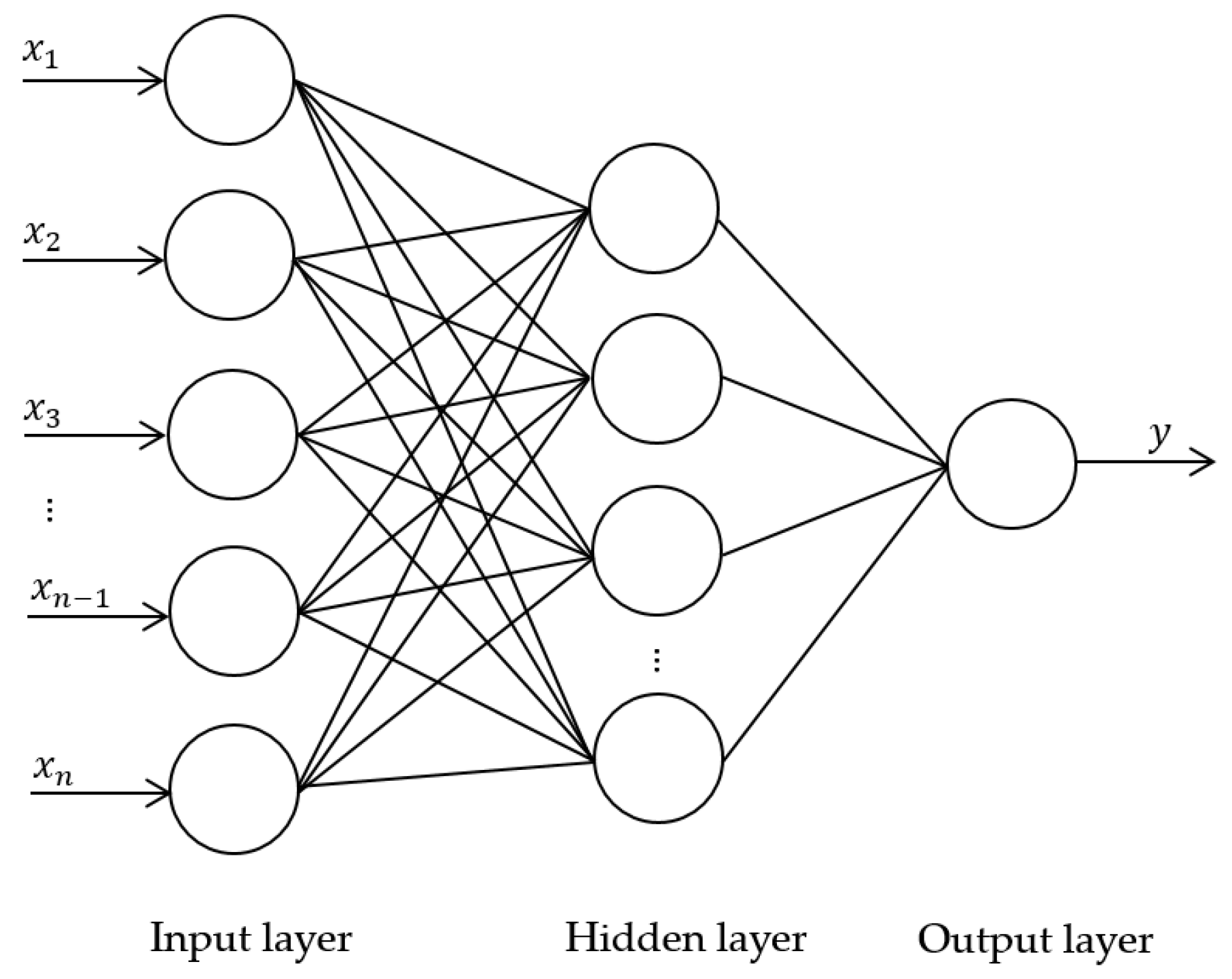
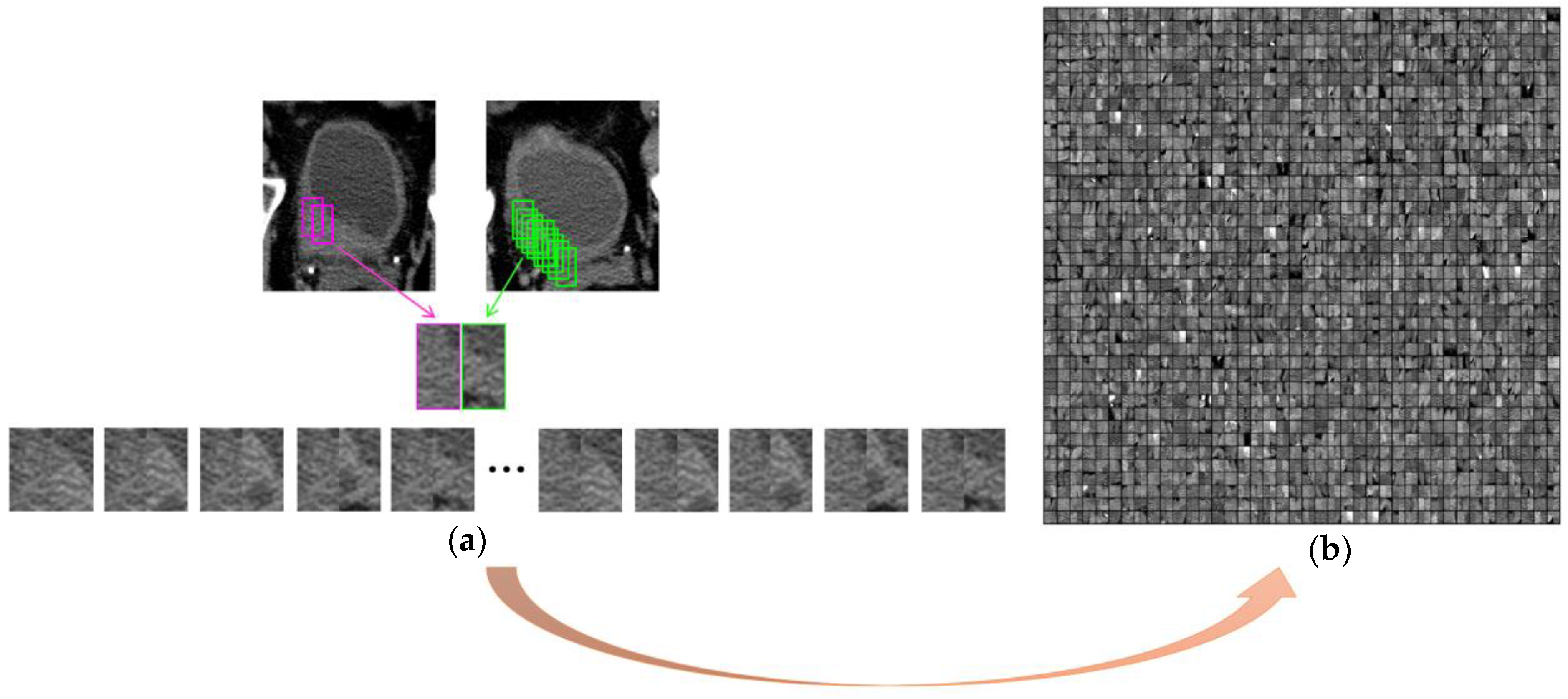
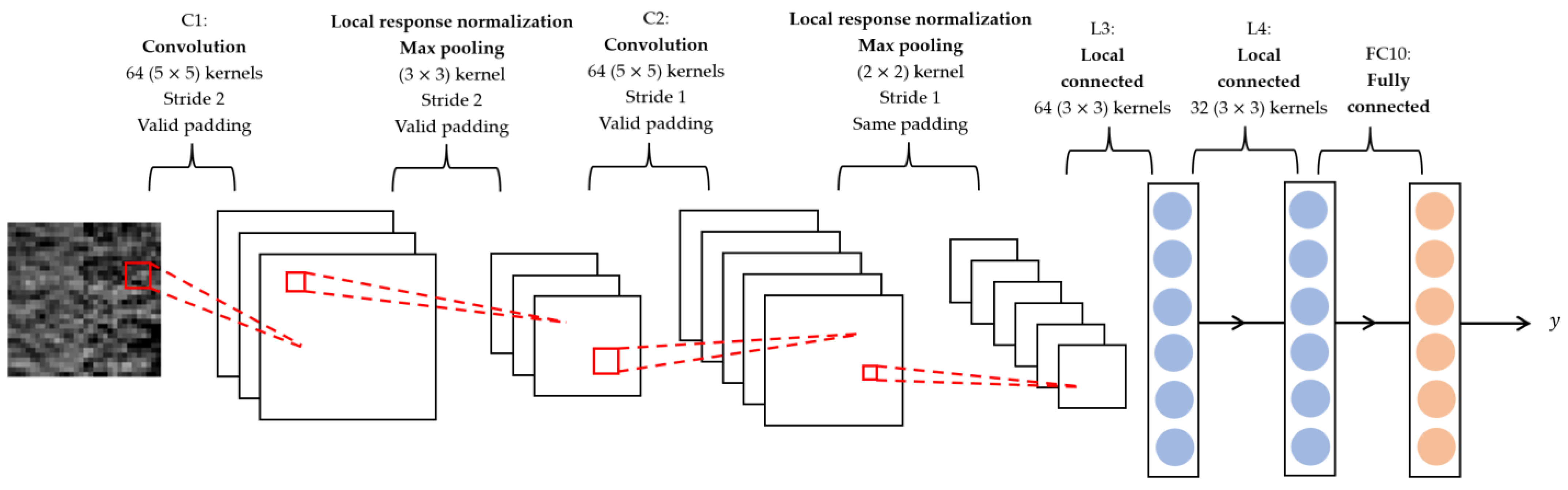
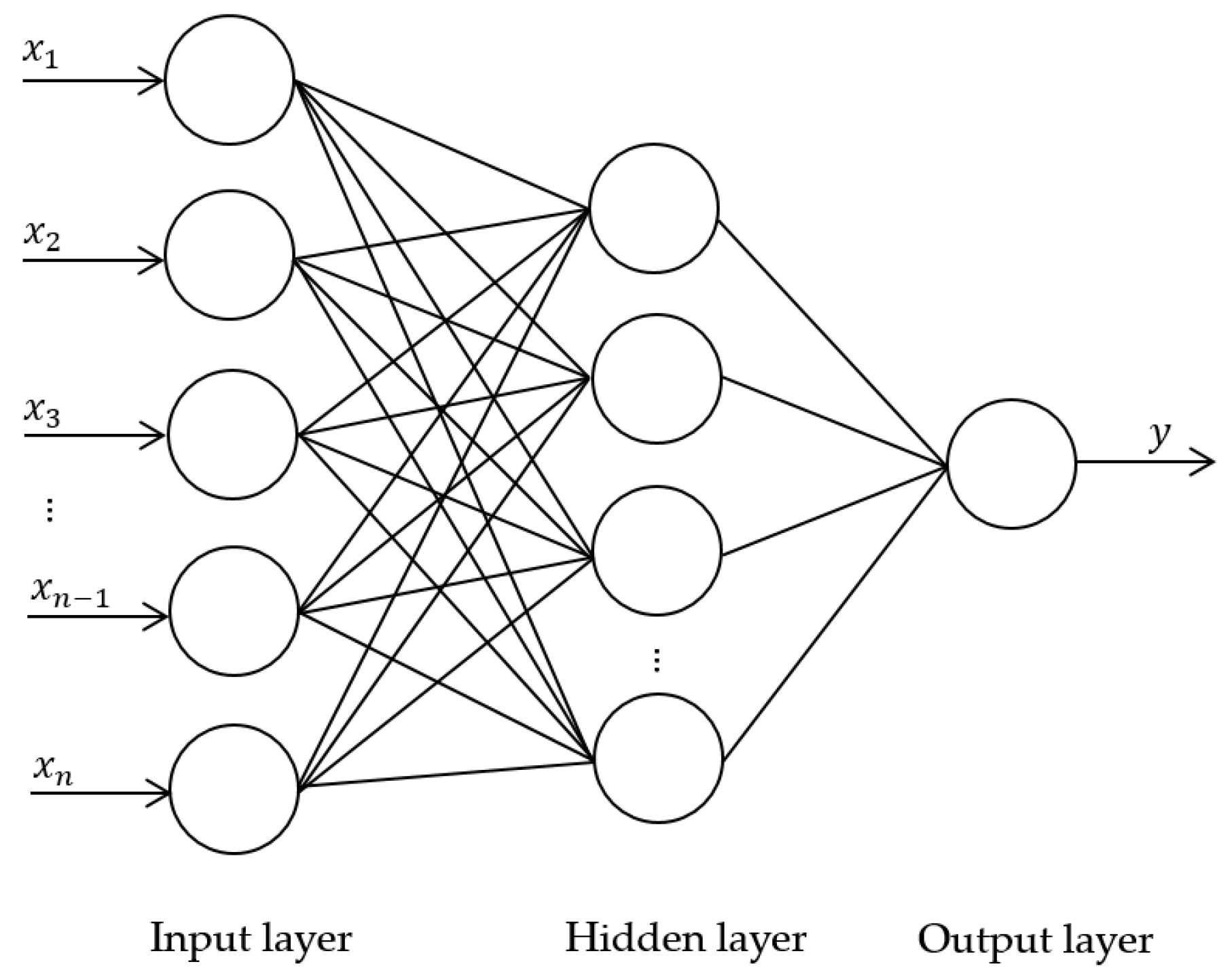
2.5. Deep-Learning Model
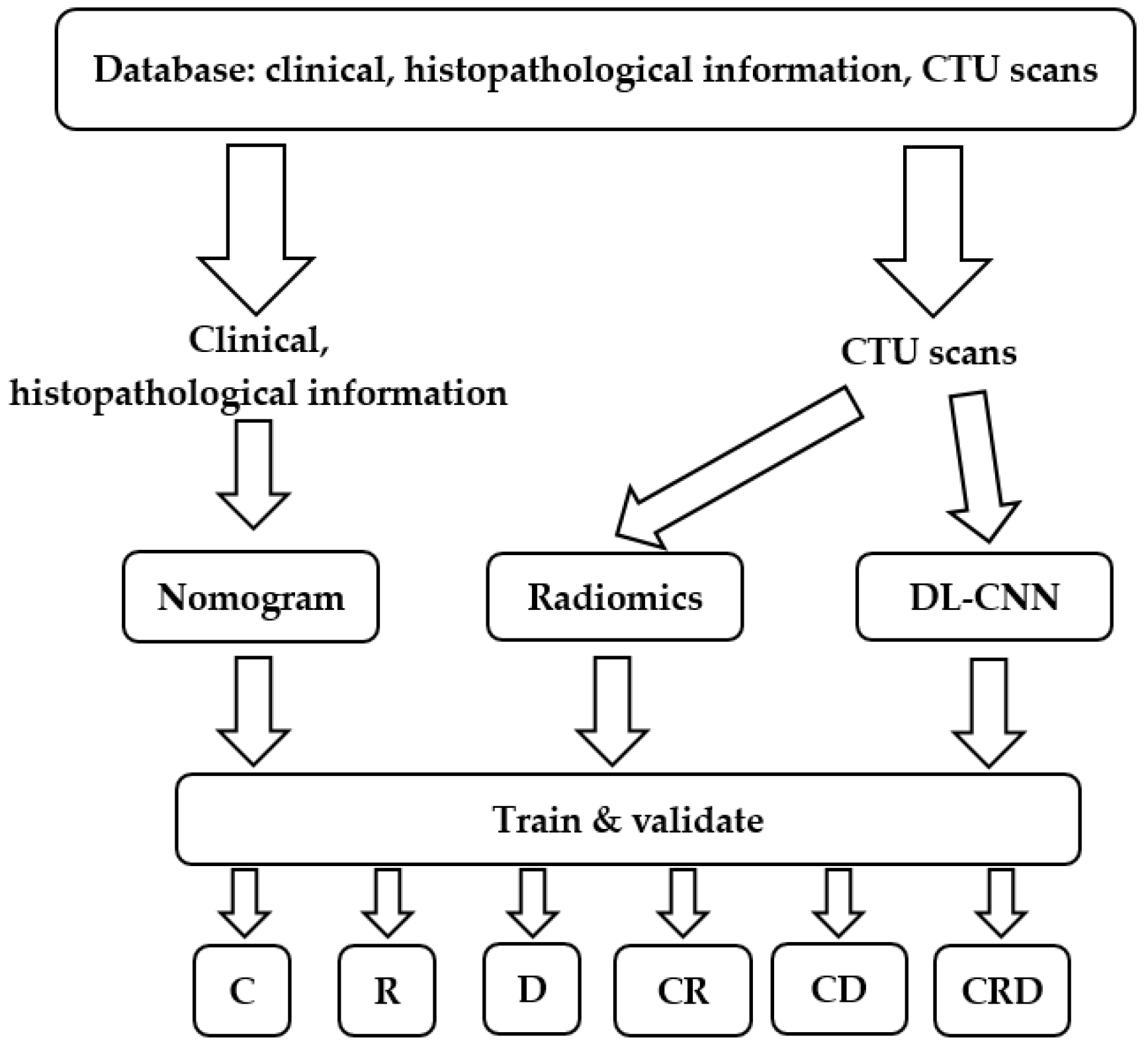
2.6. Classification
2.7. Statistical Analysis
3. Results
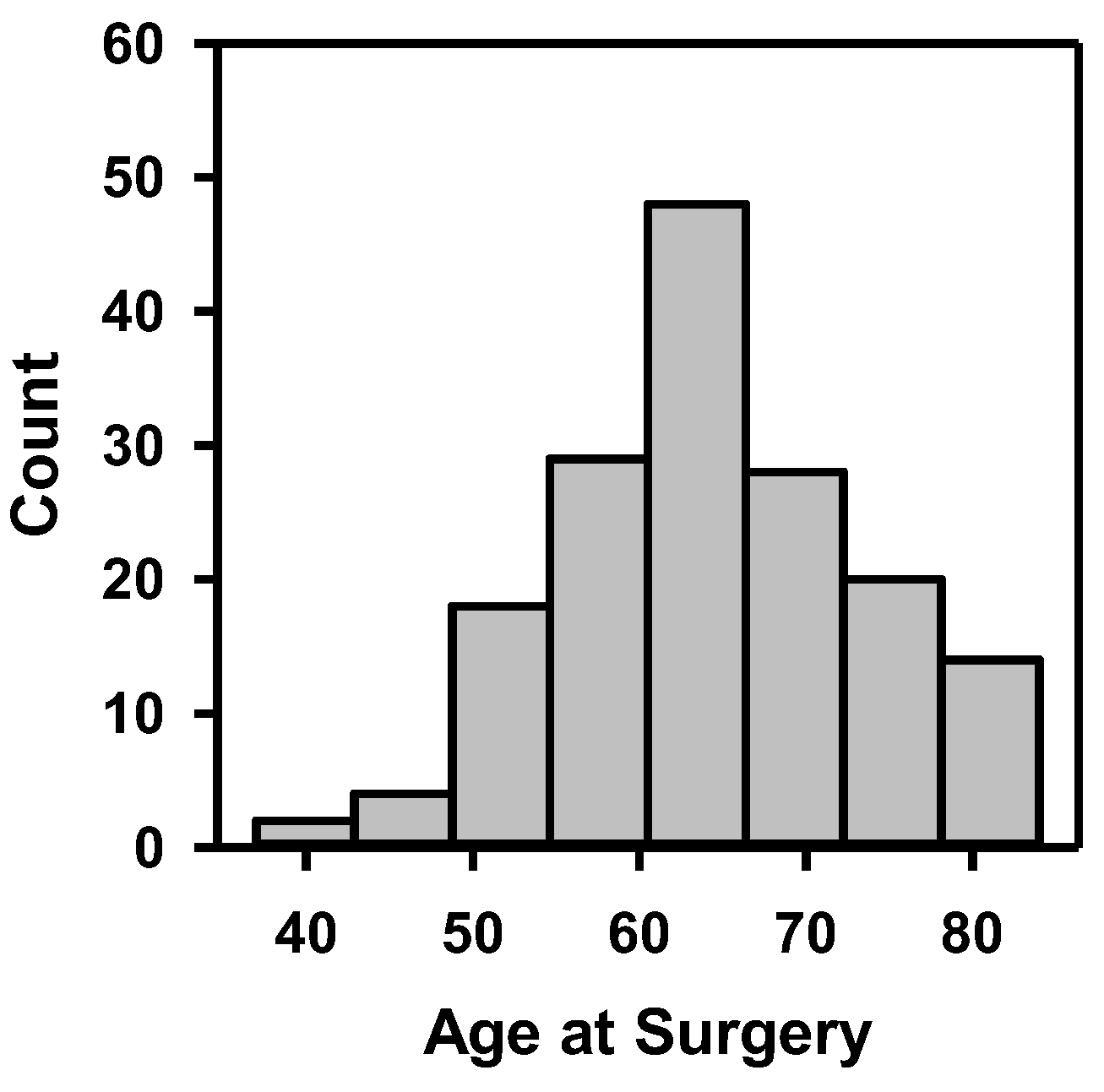
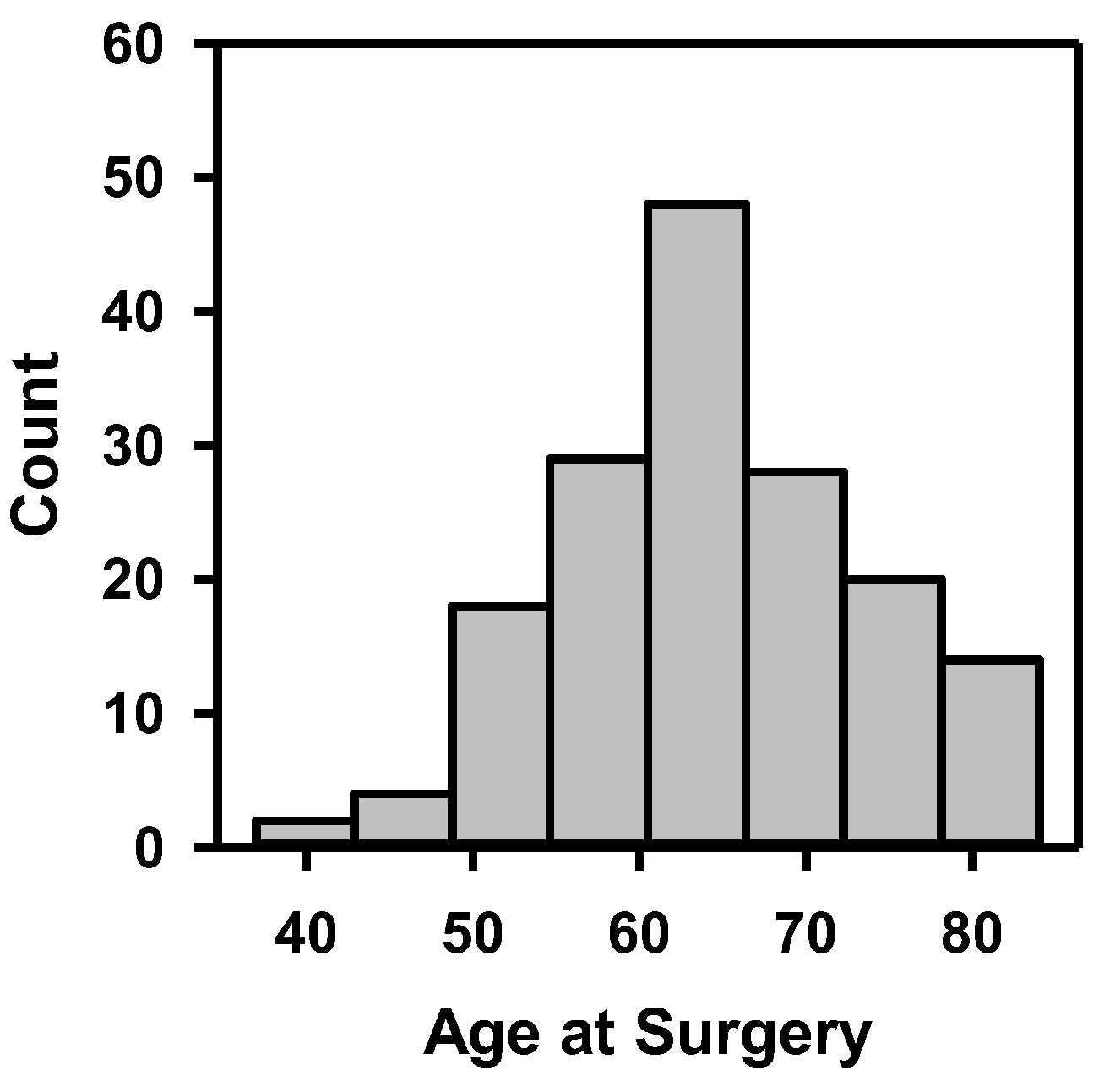
3.1. Cohort Statistics
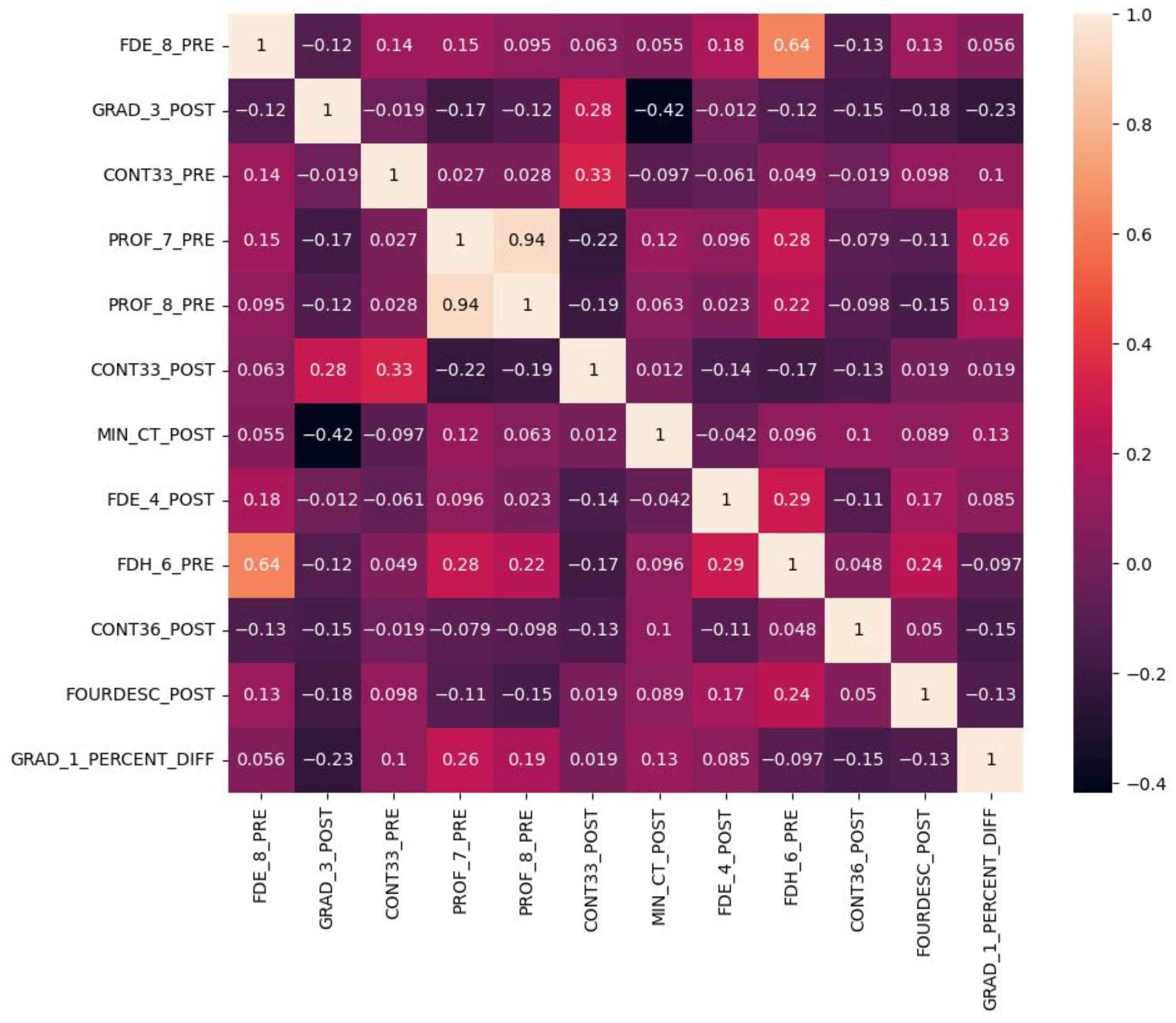
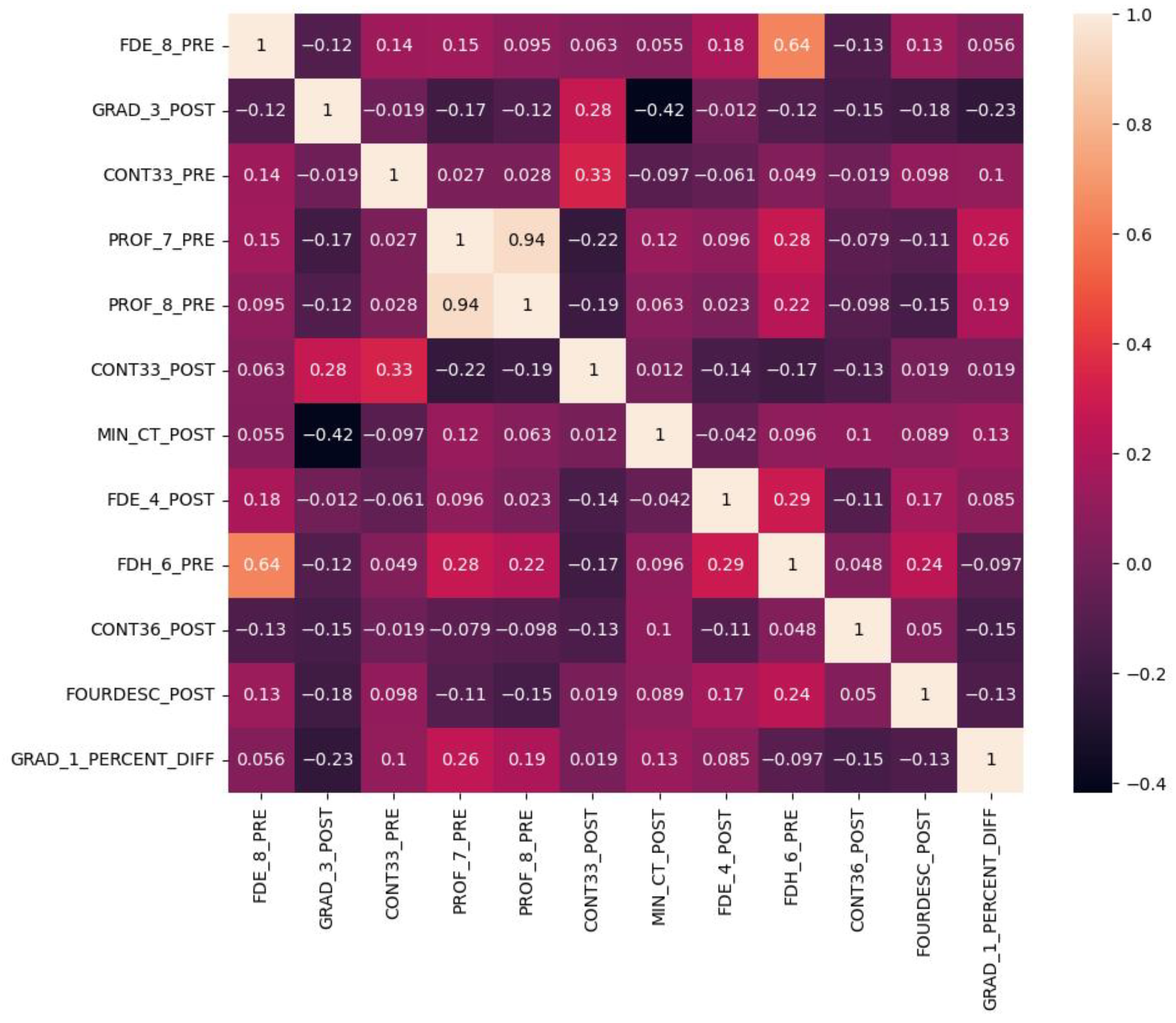
3.2. Radiomics Features
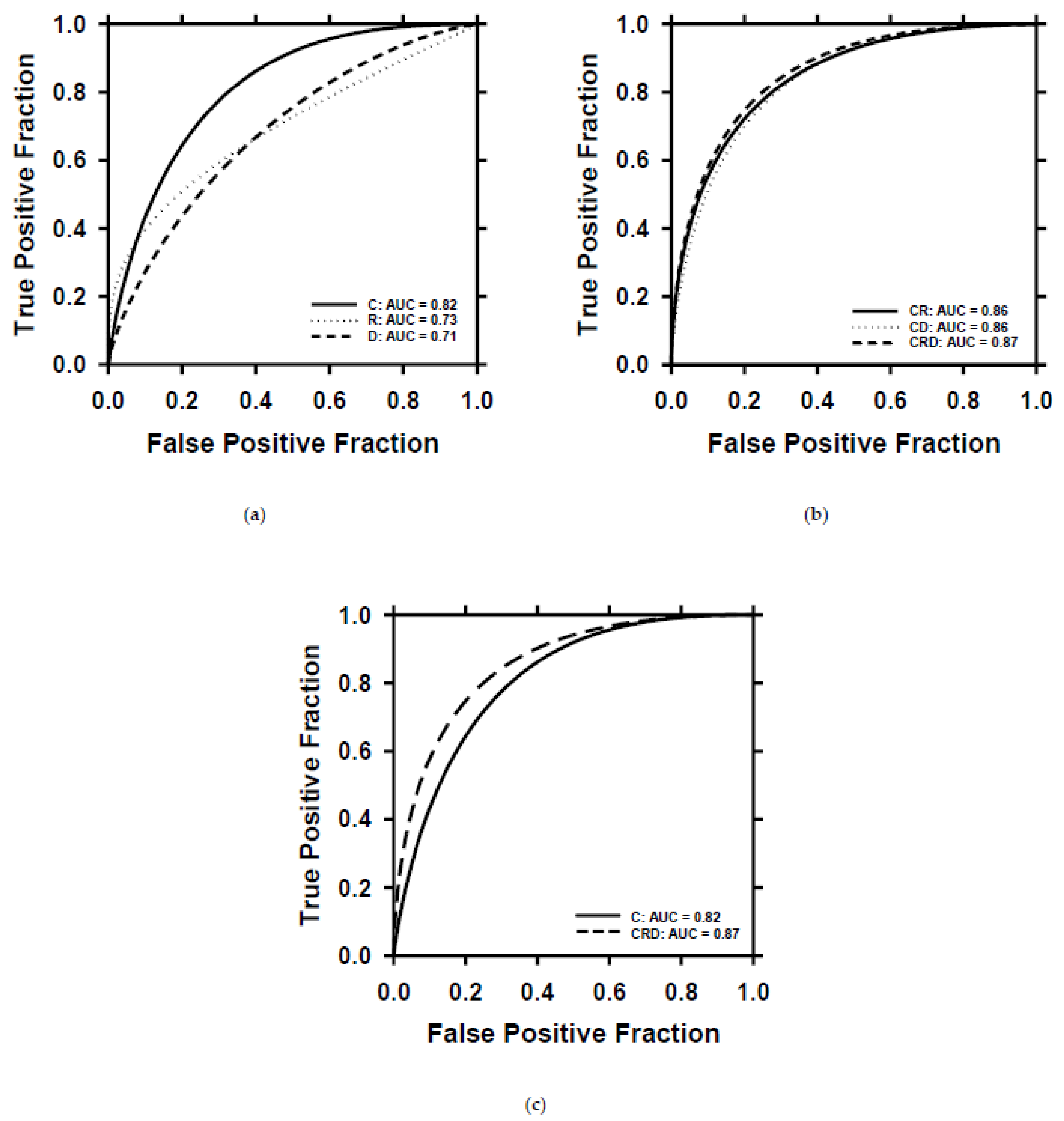
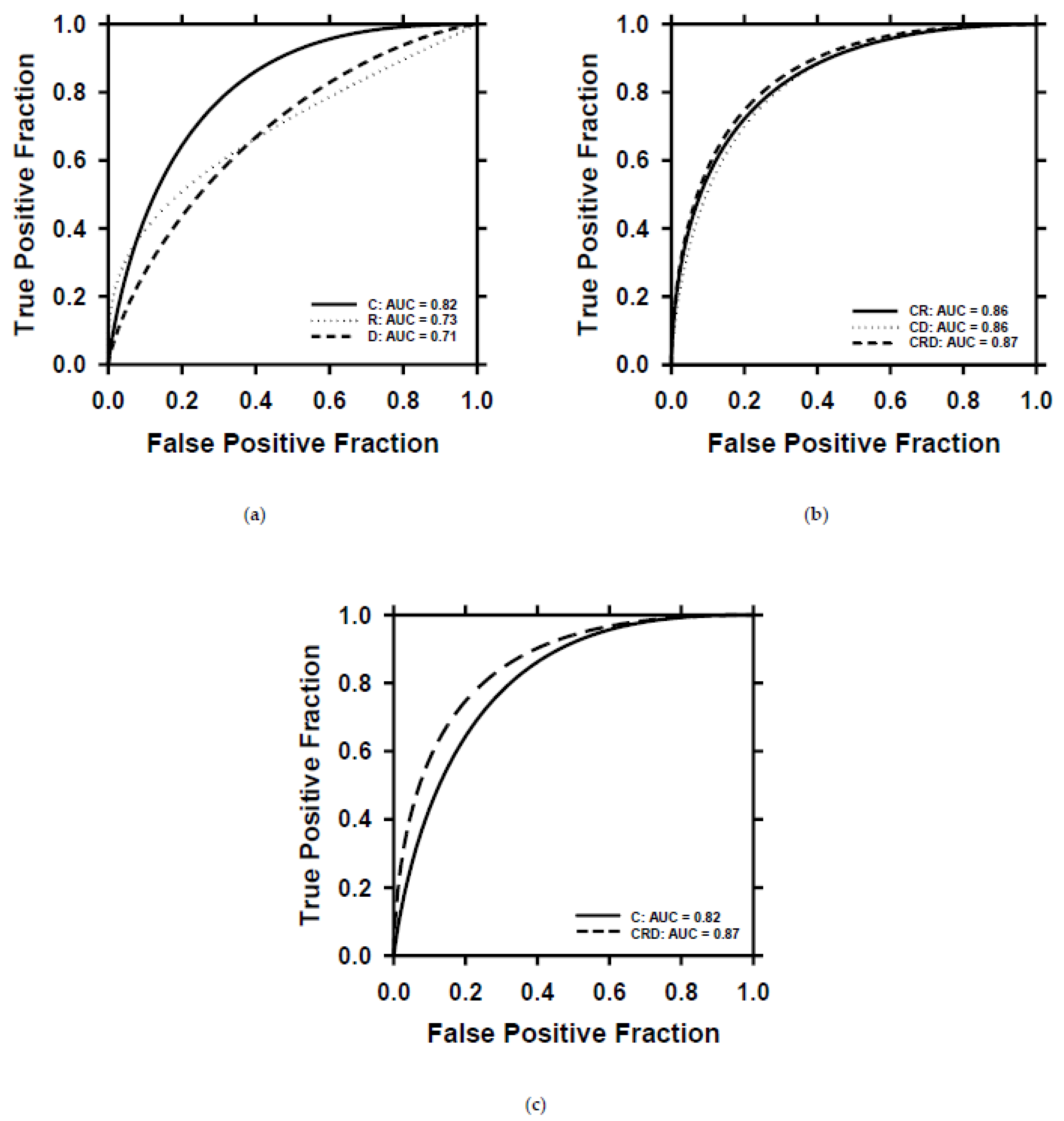
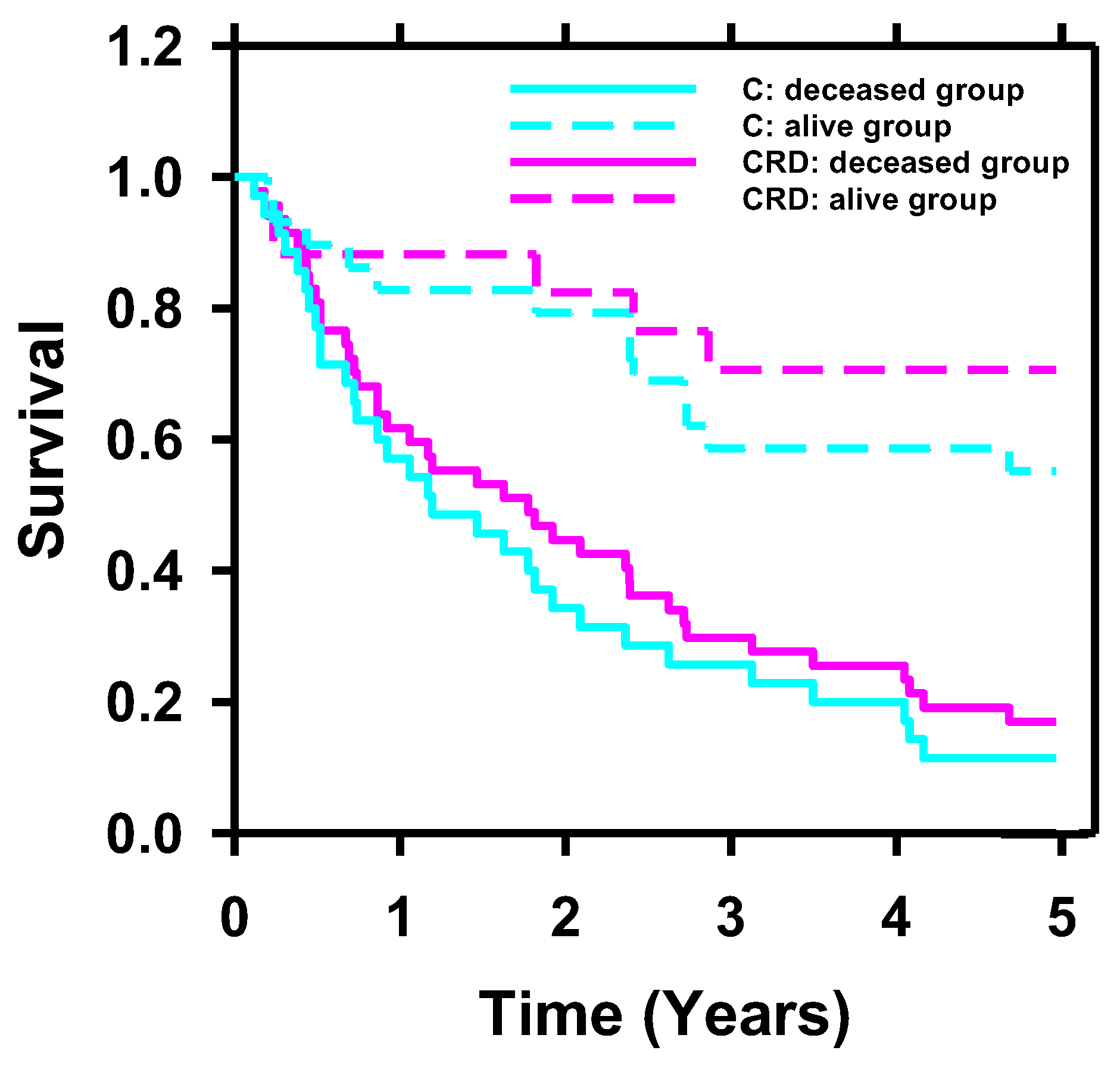
3.3. Survival Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Facts & Figures 2023; American Cancer Society: Atlanta, GA, USA, 2023. [Google Scholar]
- Gschwend, J.E.; Fair, W.R.; Vieweg, J. Radical cystectomy for invasive bladder cancer: Contemporary results and remaining controversies. Eur. Urol. 2000, 38, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Cookson, M.S. Non-muscle-invasive bladder cancer: The role of radical cystectomy. Urology 2005, 66, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Modh, R.A.; Mulhall, J.P.; Gilbert, S.M. Sexual dysfunction after cystectomy and urinary diversion. Nat. Rev. Urol. 2014, 11, 445–453. [Google Scholar] [CrossRef]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef]
- Eisenberg, M.S.; Boorjian, S.A.; Cheville, J.C.; Thompson, R.H.; Thapa, P.; Kaushik, D.; Frank, I. The SPARC score: A multifactorial outcome prediction model for patients undergoing radical cystectomy for bladder cancer. J. Urol. 2013, 190, 2005–2010. [Google Scholar] [CrossRef]
- Gavriel, C.G.; Dimitriou, N.; Brieu, N.; Nearchou, I.P.; Arandjelović, O.; Schmidt, G.; Harrison, D.J.; Caie, P.D. Assessment of immunological features in muscle-invasive bladder cancer prognosis using ensemble learning. Cancers 2021, 13, 1624. [Google Scholar] [CrossRef]
- Zheng, Q.; Yang, R.; Ni, X.; Yang, S.; Xiong, L.; Yan, D.; Xia, L.; Yuan, J.; Wang, J.; Jiao, P. Accurate Diagnosis and Survival Prediction of Bladder Cancer Using Deep Learning on Histological Slides. Cancers 2022, 14, 5807. [Google Scholar] [CrossRef]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.; Winters, B.; Douglas, J.; Van Kessel, K.E.; van de Putte, E.E.F.; Sommerlad, M.; Wang, N.Q. Impact of molecular subtypes in muscle-invasive bladder cancer on predicting response and survival after neoadjuvant chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef]
- Bhambhvani, H.P.; Zamora, A.; Shkolyar, E.; Prado, K.; Greenberg, D.R.; Kasman, A.M.; Liao, J.; Shah, S.; Srinivas, S.; Skinner, E.C. Development of robust artificial neural networks for prediction of 5-year survival in bladder cancer. In Urologic Oncology: Seminars and Original Investigations; Elsevier: Amsterdam, The Netherlands, 2021; pp. 193.e7–193.e12. [Google Scholar]
- Gavriel, C.G.; Dimitriou, N.; Brieu, N.; Nearchou, I.P.; Arandjelović, O.; Schmidt, G.; Harrison, D.J.; Caie, P.D. Identification of immunological features enables survival prediction of muscle-invasive bladder cancer patients using machine learning. BioRxiv 2020. [Google Scholar] [CrossRef]
- Riester, M.; Taylor, J.M.; Feifer, A.; Koppie, T.; Rosenberg, J.E.; Downey, R.J.; Bochner, B.H.; Michor, F. Combination of a novel gene expression signature with a clinical nomogram improves the prediction of survival in high-risk bladder cancer. Clin. Cancer Res. 2012, 18, 1323–1333. [Google Scholar] [CrossRef]
- Shariat, S.F.; Bolenz, C.; Godoy, G.; Fradet, Y.; Ashfaq, R.; Karakiewicz, P.I.; Isbarn, H.; Jeldres, C.; Rigaud, J.; Sagalowsky, A.I. Predictive value of combined immunohistochemical markers in patients with pT1 urothelial carcinoma at radical cystectomy. J. Urol. 2009, 182, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Shariat, S.F.; Karakiewicz, P.I.; Palapattu, G.S.; Amiel, G.E.; Lotan, Y.; Rogers, C.G.; Vazina, A.; Bastian, P.J.; Gupta, A.; Sagalowsky, A.I. Nomograms provide improved accuracy for predicting survival after radical cystectomy. Clin. Cancer Res. 2006, 12, 6663–6676. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Hadjiiski, L.; Chan, H.-P.; Caoili, E.M.; Cohan, R.H.; Wei, J.; Zhou, C. Auto-initialized cascaded level set (AI-CALS) segmentation of bladder lesions on multidetector row CT urography. Acad. Radiol. 2013, 20, 148–155. [Google Scholar] [CrossRef]
- Way, T.W.; Hadjiiski, L.M.; Sahiner, B.; Chan, H.P.; Cascade, P.N.; Kazerooni, E.A.; Bogot, N.; Zhou, C. Computer-aided diagnosis of pulmonary nodules on CT scans: Segmentation and classification using 3D active contours. Med. Phys. 2006, 33, 2323–2337. [Google Scholar] [CrossRef]
- Way, T.W.; Sahiner, B.; Chan, H.P.; Hadjiiski, L.; Cascade, P.N.; Chughtai, A.; Bogot, N.; Kazerooni, E. Computer-aided diagnosis of pulmonary nodules on CT scans: Improvement of classification performance with nodule surface features. Med. Phys. 2009, 36, 3086–3098. [Google Scholar] [CrossRef] [PubMed]
- Sahiner, B.; Chan, H.P.; Petrick, N.; Helvie, M.A.; Goodsitt, M.M. Computerized characterization of masses on mammograms: The rubber band straightening transform and texture analysis. Med. Phys. 1998, 25, 516–526. [Google Scholar] [CrossRef]
- Kirby, J.S.; Armato, S.G.; Drukker, K.; Li, F.; Hadjiiski, L.; Tourassi, G.D.; Clarke, L.P.; Engelmann, R.M.; Giger, M.L.; Redmond, G.; et al. LUNGx Challenge for computerized lung nodule classification. J. Med. Imaging 2016, 3, 044506. [Google Scholar]
- Sahiner, B.; Chan, H.P.; Petrick, N.; Helvie, M.A.; Hadjiiski, L.M. Improvement of mammographic mass characterization using spiculation measures and morphological features. Med. Phys. 2001, 28, 1455–1465. [Google Scholar] [CrossRef]
- Sun, D.; Hadjiiski, L.; Alva, A.; Zakharia, Y.; Joshi, M.; Chan, H.-P.; Garje, R.; Pomerantz, L.; Elhag, D.; Cohan, R.H. Computerized decision support for bladder cancer treatment response assessment in CT urography: Effect on diagnostic accuracy in multi-institution multi-specialty study. Tomography 2022, 8, 644–656. [Google Scholar] [CrossRef]
- Chan, H.P.; Sahiner, B.; Wagner, R.F.; Petrick, N. Classifier design for computer-aided diagnosis: Effects of finite sample size on the mean performance of classical and neural network classifiers. Med. Phys. 1999, 26, 2654–2668. [Google Scholar] [CrossRef] [PubMed]
- Sahiner, B.; Chan, H.P.; Petrick, N.; Wagner, R.F.; Hadjiiski, L. Feature selection and classifier performance in computer-aided diagnosis: The effect of finite sample size. Med. Phys. 2000, 27, 1509–1522. [Google Scholar] [CrossRef] [PubMed]
- Way, T.W.; Sahiner, B.; Hadjiiski, L.M.; Chan, H.P. Effect of finite sample size on feature selection and classification: A simulation study. Med. Phys. 2010, 37, 907–920. [Google Scholar] [CrossRef]
- Battiti, R. Using mutual information for selecting features in supervised neural net learning. IEEE Trans. Neural Netw. 1994, 5, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Cha, K.H.; Hadjiiski, L.; Chan, H.-P.; Weizer, A.Z.; Alva, A.; Cohan, R.H.; Caoili, E.M.; Paramagul, C.; Samala, R.K. Bladder cancer treatment response assessment in CT using radiomics with deep-learning. Sci. Rep. 2017, 7, 8738. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.; Hadjiiski, L.M.; Samala, R.K.; Chan, H.-P.; Cha, K.H.; Richter, C.; Cohan, R.H.; Caoili, E.M.; Paramagul, C.; Alva, A. Deep learning approach for assessment of bladder cancer treatment response. Tomography 2019, 5, 201–208. [Google Scholar] [CrossRef]
- Goh, A.T. Back-propagation neural networks for modeling complex systems. Artif. Intell. Eng. 1995, 9, 143–151. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Feng, Z.; Yi, X. A general introduction to adjustment for multiple comparisons. J. Thorac. Dis. 2017, 9, 1725. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Multiple significance tests: The Bonferroni method. BMJ 1995, 310, 170. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Samala, R.K.; Chan, H.-P.; Hadjiiski, L.; Helvie, M.A.; Richter, C.D.; Cha, K.H. Breast cancer diagnosis in digital breast tomosynthesis: Effects of training sample size on multi-stage transfer learning using deep neural nets. IEEE Trans. Med. Imaging 2018, 38, 686–696. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Attributes | # | |
|---|---|---|
| Gender | Male | 131 |
| Female | 32 | |
| Race | White | 142 |
| Black/African Am. | 13 | |
| Am. Indian/Native | 1 | |
| Asian | 2 | |
| Unknown | 5 | |
| Tobacco use | Current | 40 |
| Former | 88 | |
| Never | 34 | |
| Unknown | 1 | |
| Post-surgery stage | pT0 | 35 |
| pTa/pTi/pTis | 15 | |
| pT1 | 16 | |
| pT2 | 36 | |
| pT3 | 45 | |
| pT4 | 16 | |
| Lymphovascular invasion (LVI) | Yes | 61 |
| No | 102 | |
| Pathologic node stage | N0 | 112 |
| N1 | 24 | |
| N2 | 23 | |
| N3 | 4 | |
| Neoadjuvant chemotherapy | Yes | 163 |
| No | 0 | |
| Adjuvant radiotherapy | Yes | 0 |
| No | 163 |
| Comparison | p-Value (Adjusted α = 0.017) |
|---|---|
| C vs. CRD | 0.153 |
| R vs. CRD | 0.056 |
| D vs. CRD | 0.007 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, D.; Hadjiiski, L.; Gormley, J.; Chan, H.-P.; Caoili, E.M.; Cohan, R.H.; Alva, A.; Gulani, V.; Zhou, C. Survival Prediction of Patients with Bladder Cancer after Cystectomy Based on Clinical, Radiomics, and Deep-Learning Descriptors. Cancers 2023, 15, 4372. https://doi.org/10.3390/cancers15174372
Sun D, Hadjiiski L, Gormley J, Chan H-P, Caoili EM, Cohan RH, Alva A, Gulani V, Zhou C. Survival Prediction of Patients with Bladder Cancer after Cystectomy Based on Clinical, Radiomics, and Deep-Learning Descriptors. Cancers. 2023; 15(17):4372. https://doi.org/10.3390/cancers15174372
Chicago/Turabian StyleSun, Di, Lubomir Hadjiiski, John Gormley, Heang-Ping Chan, Elaine M. Caoili, Richard H. Cohan, Ajjai Alva, Vikas Gulani, and Chuan Zhou. 2023. "Survival Prediction of Patients with Bladder Cancer after Cystectomy Based on Clinical, Radiomics, and Deep-Learning Descriptors" Cancers 15, no. 17: 4372. https://doi.org/10.3390/cancers15174372
APA StyleSun, D., Hadjiiski, L., Gormley, J., Chan, H.-P., Caoili, E. M., Cohan, R. H., Alva, A., Gulani, V., & Zhou, C. (2023). Survival Prediction of Patients with Bladder Cancer after Cystectomy Based on Clinical, Radiomics, and Deep-Learning Descriptors. Cancers, 15(17), 4372. https://doi.org/10.3390/cancers15174372