
Topographical and Chronological Analysis of Thin Cutaneous Melanoma’s Progressions: A Multicentric Study

 ,
,  ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.2. Statistical Analysis
3. Results
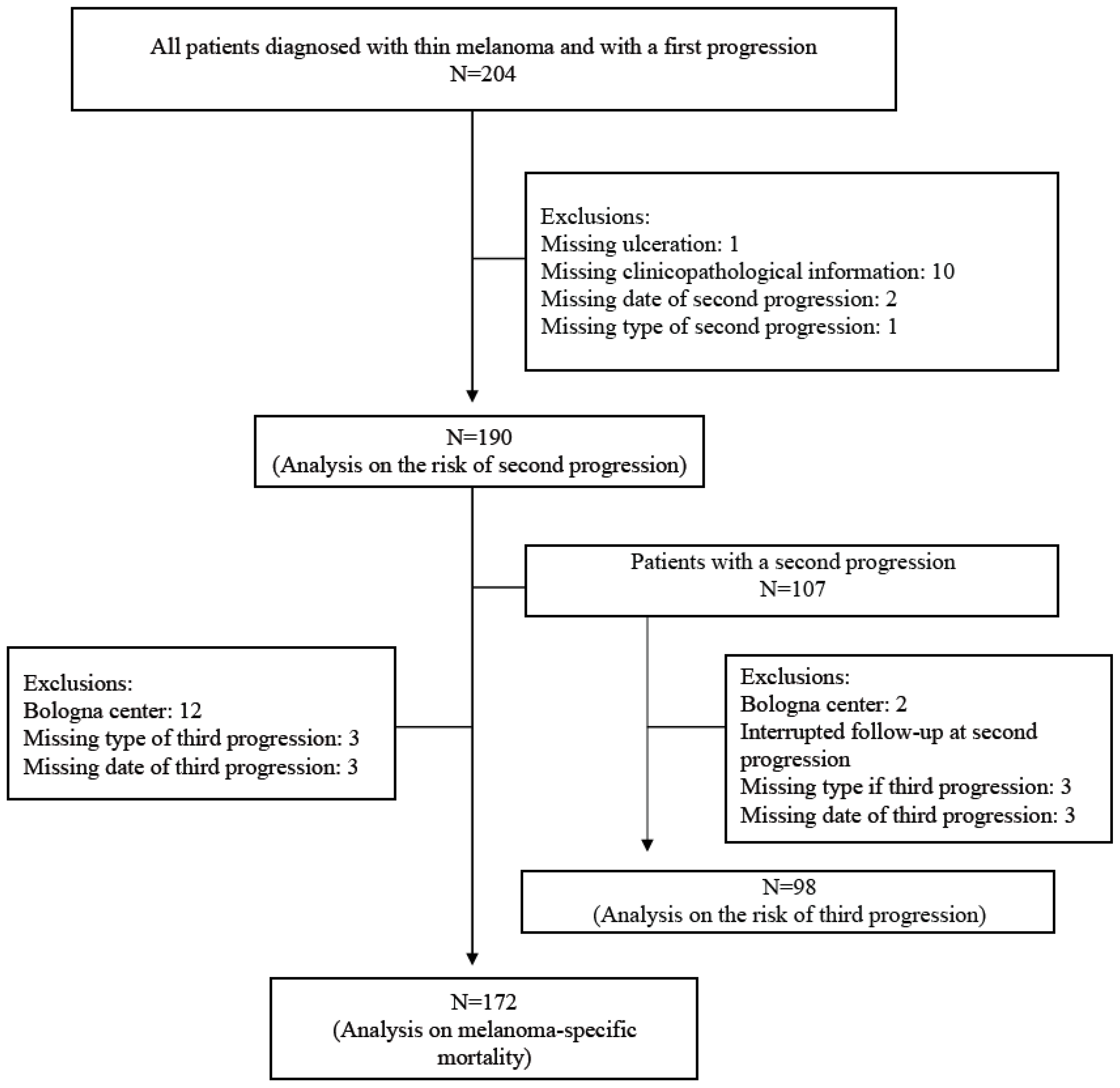
3.1. Study Population
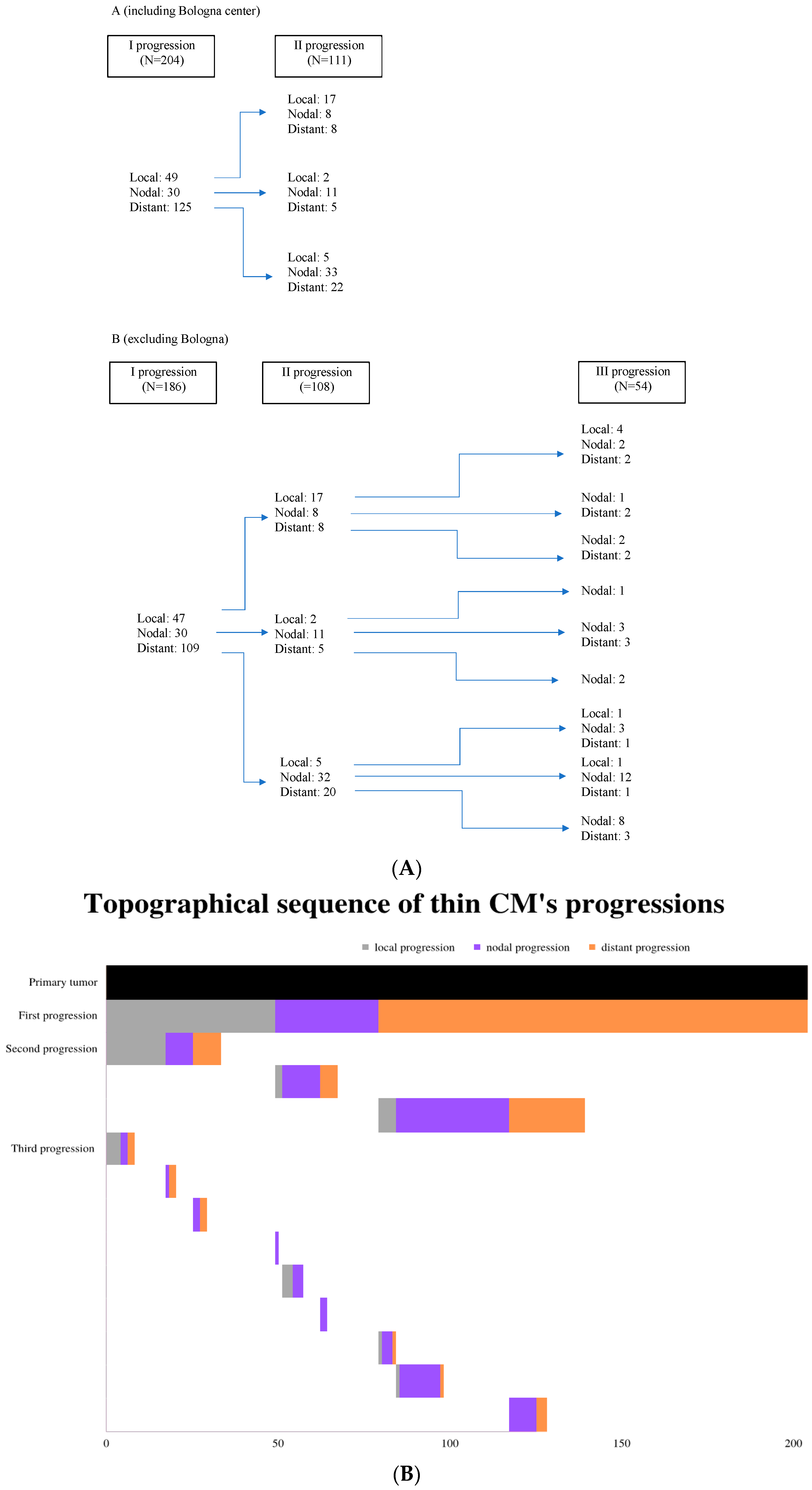
3.2. Progression Pathways
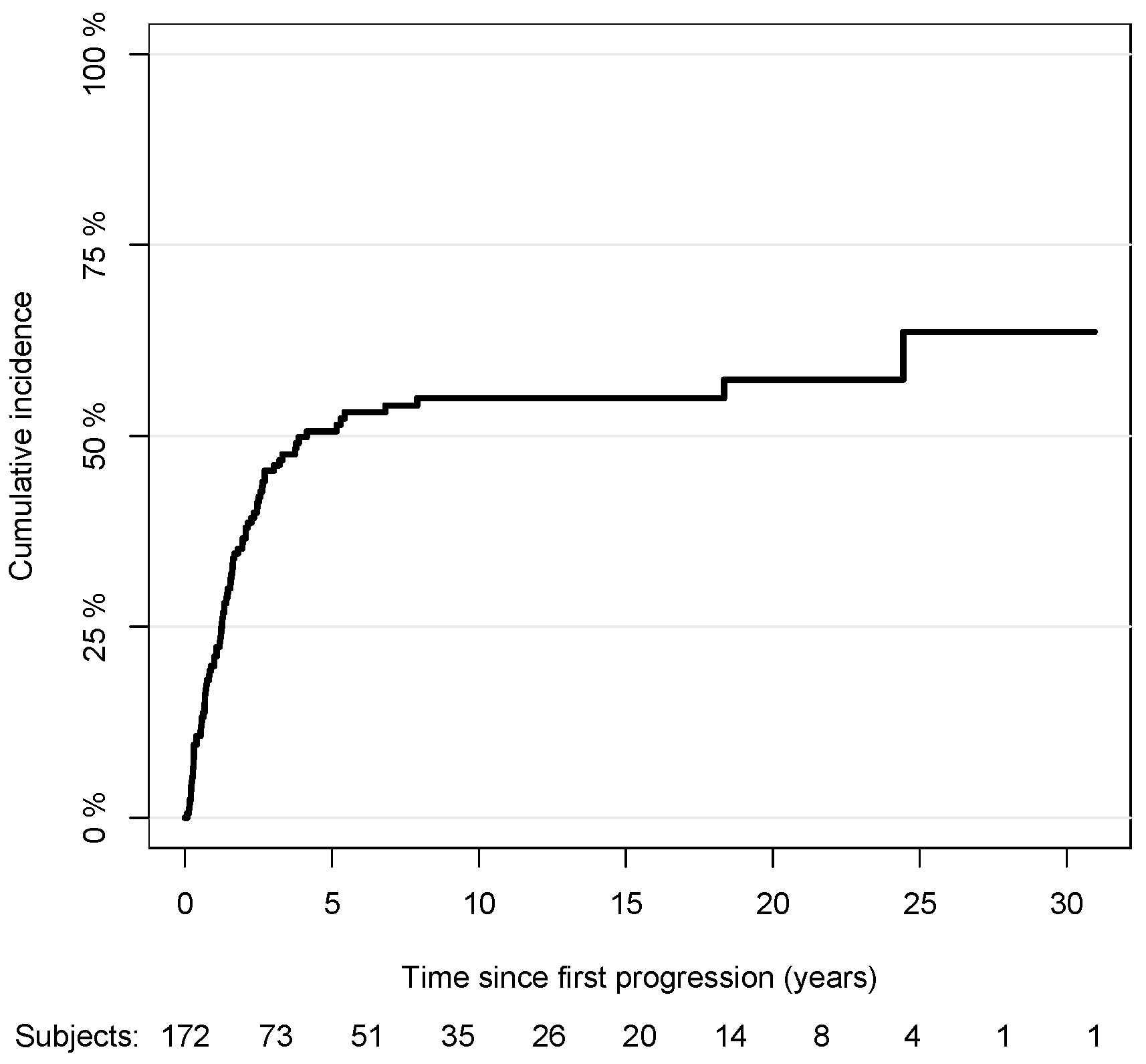
3.3. First Progression
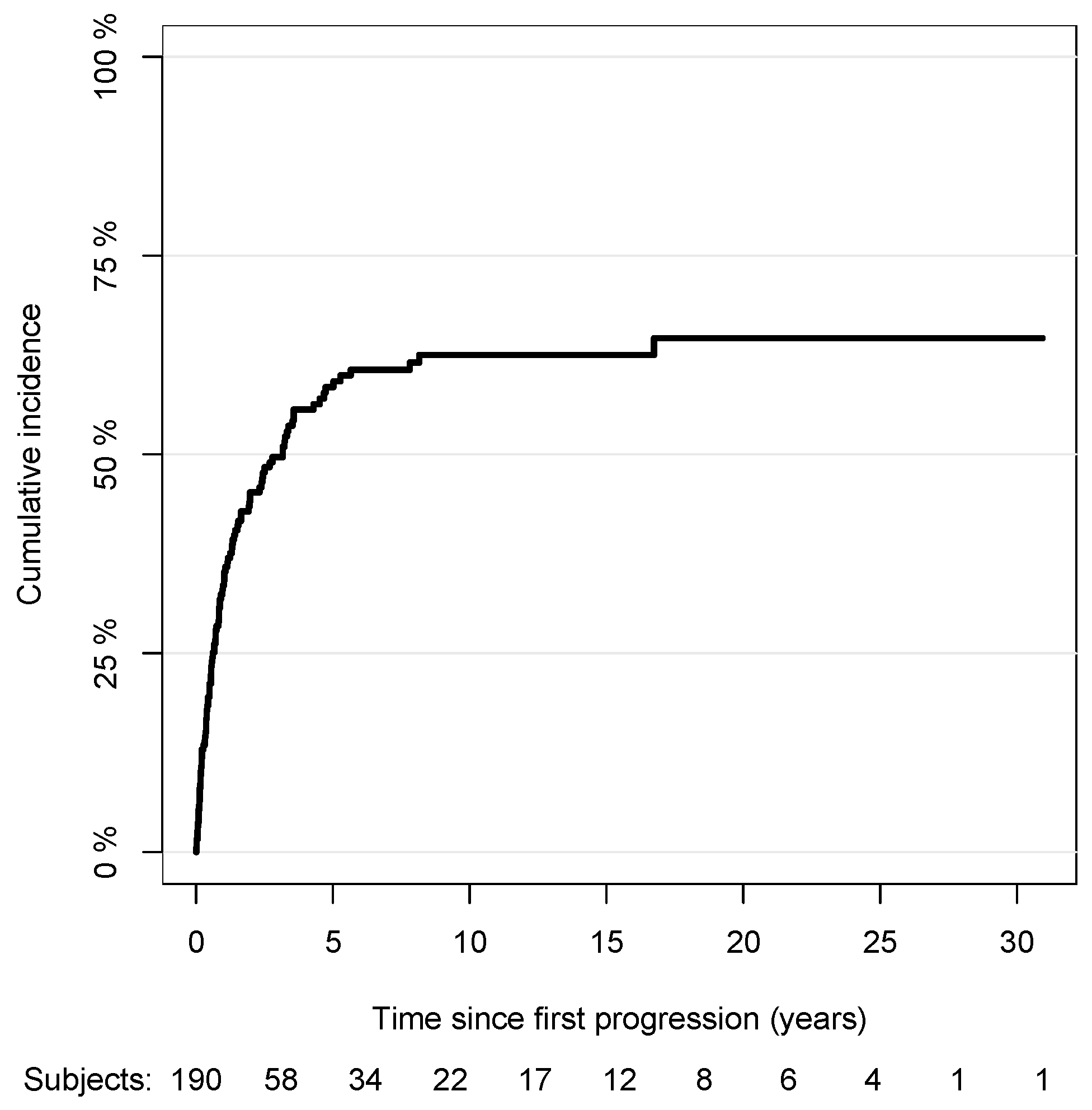
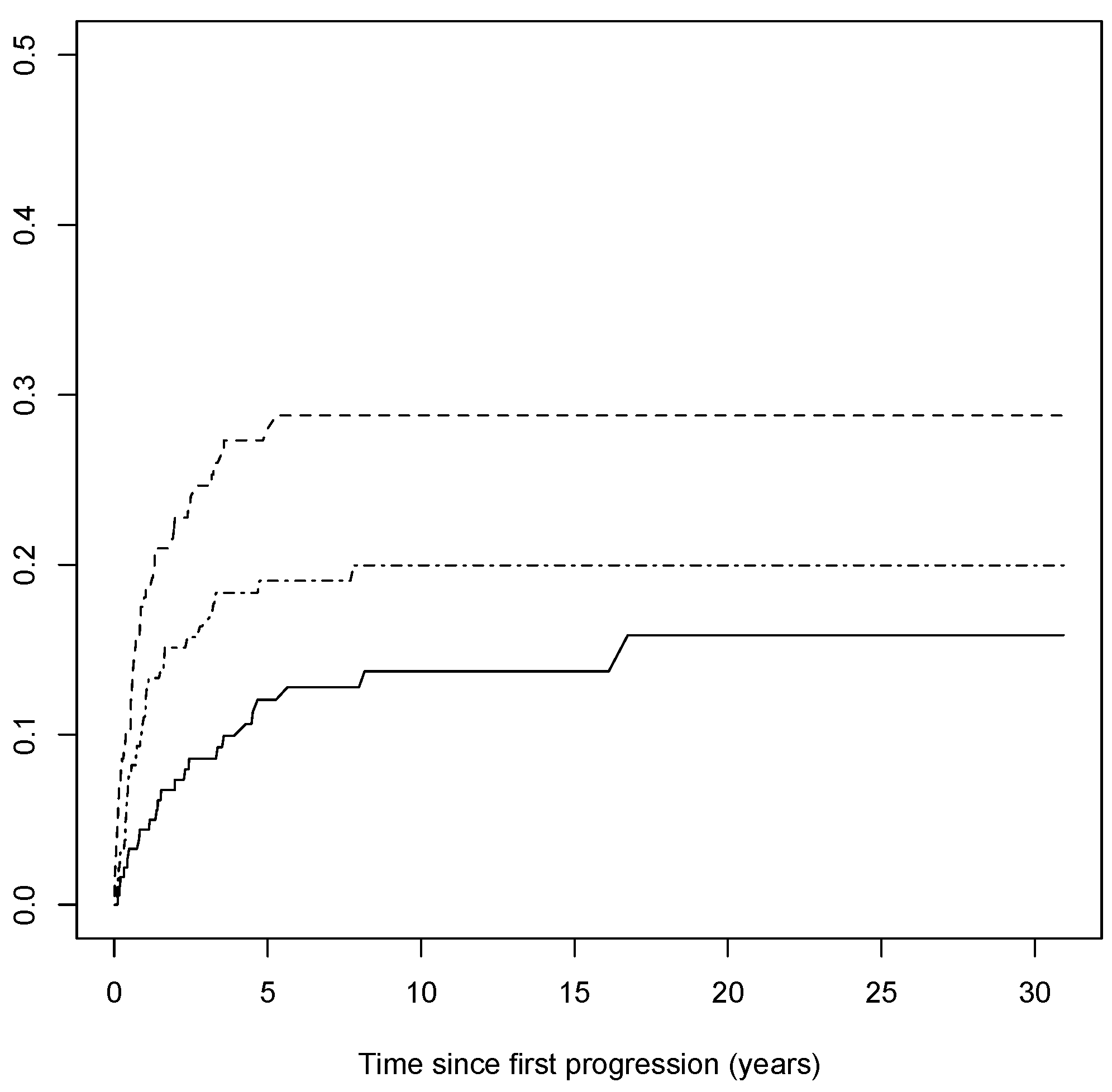
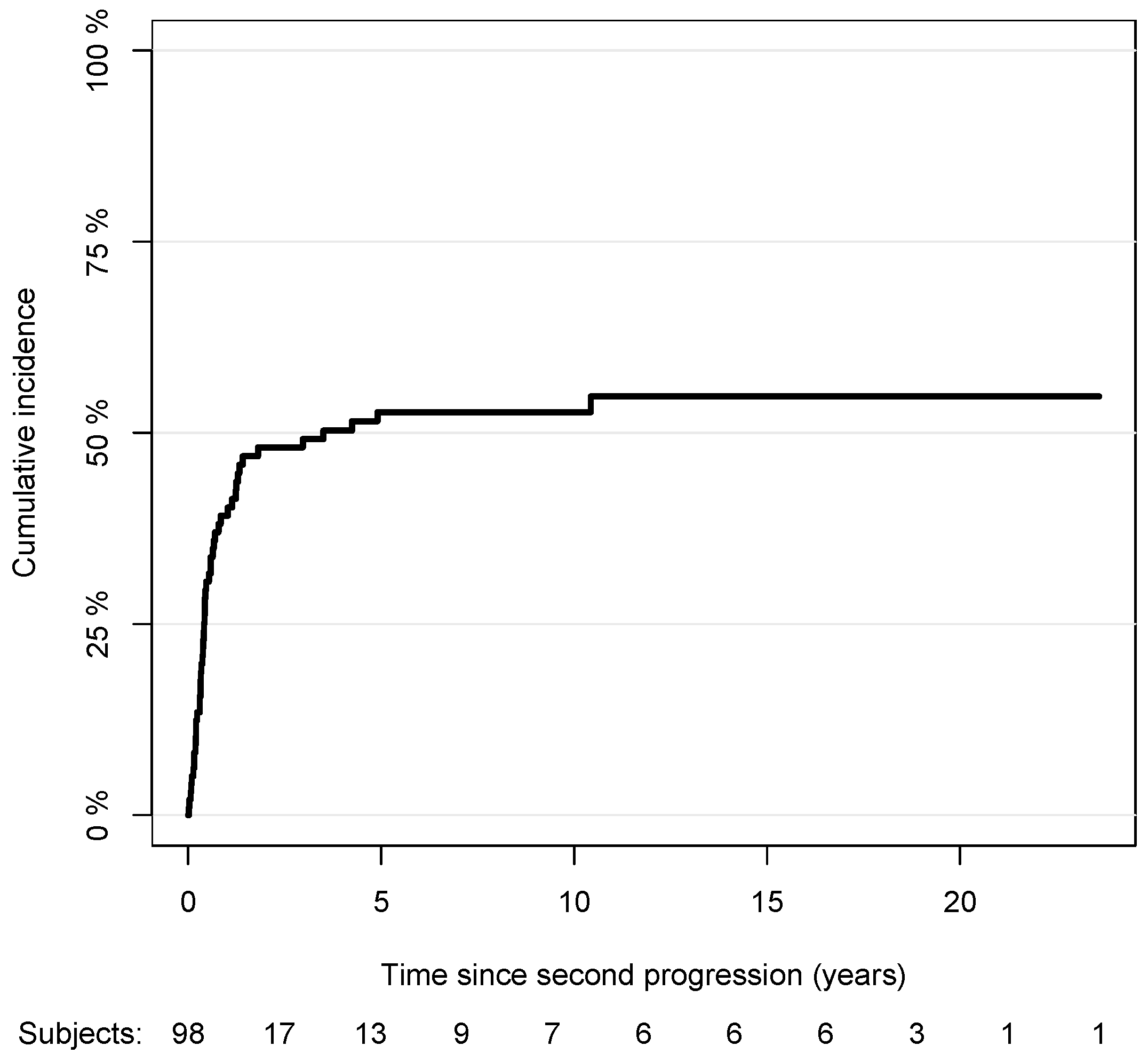
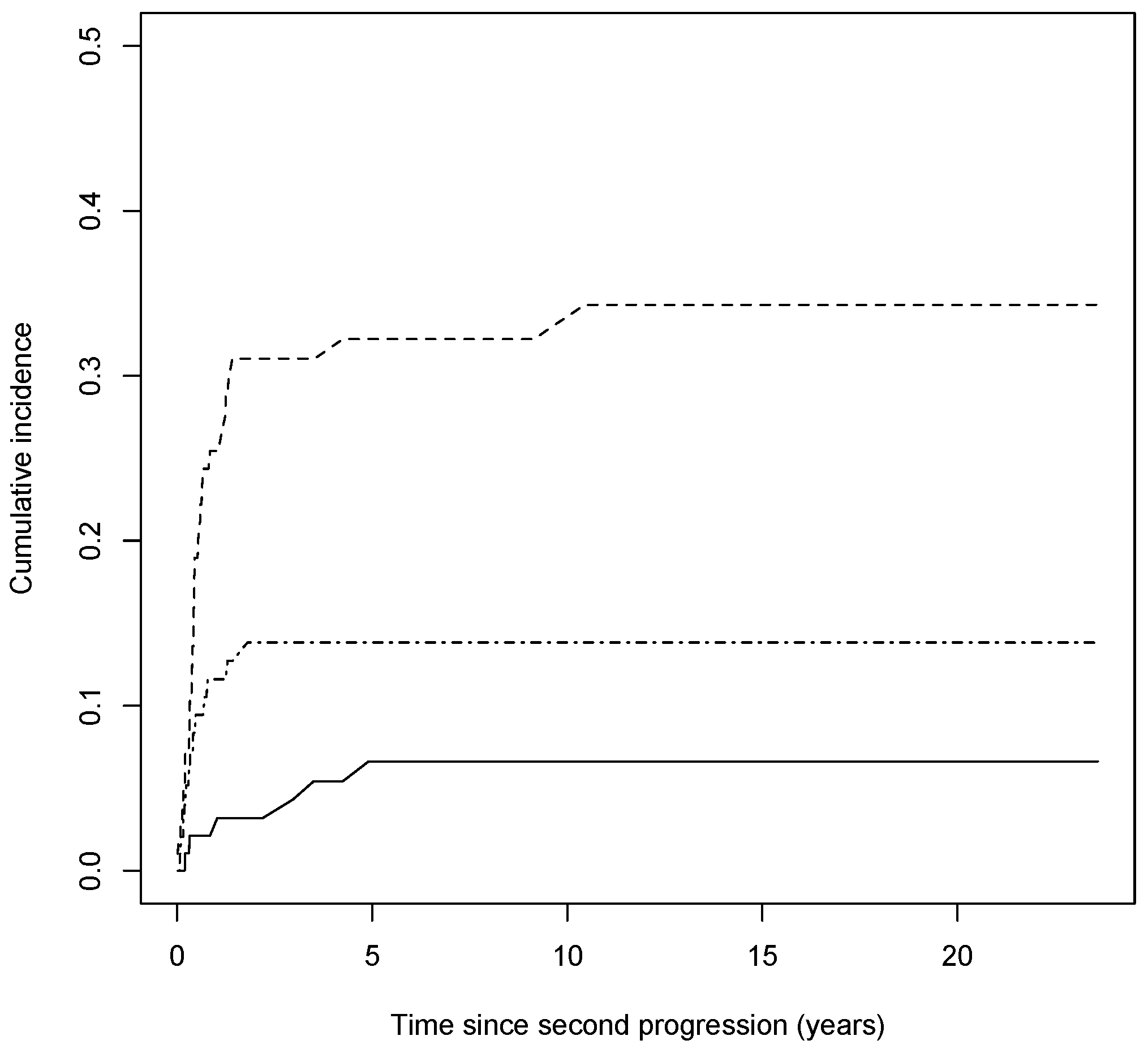
3.4. Second Progression
3.5. Third Progression
3.6. Melanoma-Specific Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siotos, C.; Grunvald, M.W.; Damoulakis, G.; Becerra, A.Z.; O’Donoghue, C.M.; Dorafshar, A.H.; Shenaq, D.S. Trends in Skin Melanoma Burden: Findings from the Global Burden of Disease Study. Eplasty 2022, 22, e9. [Google Scholar]
- Guy Jr, G.P.; Thomas, C.C.; Thompson, T.; Watson, M.; Massetti, G.M.; Richardson, L.C. Vital Signs: Melanoma Incidence and Mortality Trends and Projections—United States, 1982–2030. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 591–596. [Google Scholar]
- Gastman, B.R.; Gerami, P.; Kurley, S.J.; Cook, R.W.; Leachman, S.; Vetto, J.T. Identification of patients at risk of metastasis using a prognostic 31-gene expression profile in subpopulations of melanoma patients with favorable outcomes by standard criteria. J. Am. Acad. Dermatol. 2019, 80, 149–157.e4. [Google Scholar]
- Buja, A.; Bardin, A.; Damiani, G.; Zorzi, M.; De Toni, C.; Fusinato, R.; Spina, R.; Vecchiato, A.; Del Fiore, P.; Mocellin, S.; et al. Prognosis for Cutaneous Melanoma by Clinical and Pathological Profile: A Population-Based Study. Front. Oncol. 2021, 11, 737399. [Google Scholar]
- Clark, W.H. Tumour progression and the nature of cancer. Br. J. Cancer 1991, 64, 631–644. [Google Scholar]
- Gassenmaier, M.; Eigentler, T.K.; Keim, U.; Goebeler, M.; Fiedler, E.; Schuler, G.; Leiter, U.; Weide, B.; Grischke, E.M.; Martus, P.; et al. Serial or Parallel Metastasis of Cutaneous Melanoma? A Study of the German Central Malignant Melanoma Registry. J. Investig. Dermatol. 2017, 137, 2570–2577. [Google Scholar]
- Calomarde-Rees, L.; García-Calatayud, R.; Caballero, C.R.; Manrique-Silva, E.; Traves, V.; García-Casado, Z.; Soriano, V.; Kumar, R.; Nagore, E. Risk Factors for Lymphatic and Hematogenous Dissemination in Patients with Stages I to II Cutaneous Melanoma. JAMA Dermatol. 2019, 155, 679–687. [Google Scholar]
- Hollestein, L.M.; Nijsten, T. Survival is excellent for most patients with thin melanoma, but patients may die from thin melanoma. Br. J. Dermatol. 2021, 184, 4. [Google Scholar]
- Whiteman, D.C.; Baade, P.D.; Olsen, C.M. More people die from thin melanomas (≤1 mm) than from thick melanomas (>4 mm) in Queensland, Australia. J. Investig. Dermatol. 2015, 135, 1190–1193. [Google Scholar]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert. Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar]
- Ertekin, S.S.; Podlipnik, S.; Riquelme-Mc Loughlin, C.; Barreiro-Capurro, A.; Arance, A.; Carrera, C.; Malvehy, J.; Puig, S. Initial Stage of Cutaneous Primary Melanoma Plays a Key Role in the Pattern and Timing of Disease Recurrence. Acta Derm. Venereol. 2021, 101, adv00502. [Google Scholar]
- Richetta, A.G.; Valentini, V.; Marraffa, F.; Paolino, G.; Rizzolo, P.; Silvestri, V.; Zelli, V.; Carbone, A.; Di Mattia, C.; Calvieri, S.; et al. Metastases risk in thin cutaneous melanoma: Prognostic value of clinical-pathologic characteristics and mutation profile. Oncotarget 2018, 9, 32173–32181. [Google Scholar]
- Maurichi, A.; Miceli, R.; Camerini, T.; Mariani, L.; Patuzzo, R.; Ruggeri, R.; Gallino, G.; Tolomio, E.; Tragni, G.; Valeri, B.; et al. Prediction of survival in patients with thin melanoma: Results from a multi-institution study. J. Clin. Oncol. 2014, 32, 2479–2485. [Google Scholar]
- Tejera-Vaquerizo, A.; Boada, A.; Ribero, S.; Puig, S.; Paradela, S.; Moreno-Ramírez, D.; Cañueto, J.; de Unamuno-Bustos, B.; Brinca, A.; Descalzo-Gallego, M.A.; et al. Sentinel Lymph Node Biopsy vs. Observation in Thin Melanoma: A Multicenter Propensity Score Matching Study. J. Clin. Med. 2021, 10, 5878. [Google Scholar]
- Isaksson, K.; Nielsen, K.; Mikiver, R.; Nieweg, O.E.; Scolyer, R.A.; Thompson, J.F.; Ingvar, C. Sentinel lymph node biopsy in patients with thin melanomas: Frequency and predictors of metastasis based on analysis of two large international cohorts. J. Surg. Oncol. 2018, 118, 599–605. [Google Scholar]
- Wong, S.L.; Faries, M.B.; Kennedy, E.B.; Agarwala, S.S.; Akhurst, T.J.; Ariyan, C.; Balch, C.M.; Berman, B.S.; Cochran, A.; Delman, K.A.; et al. Sentinel Lymph Node Biopsy and Management of Regional Lymph Nodes in Melanoma: American Society of Clinical Oncology and Society of Surgical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 399–413. [Google Scholar]
- Swetter, S.M.; Thompson, J.A.; Albertini, M.R.; Barker, C.A.; Baumgartner, J.; Boland, G.; Chmielowski, B.; DiMaio, D.; Durham, A.; Fields, R.C.; et al. NCCN Guidelines® Insights: Melanoma: Cutaneous, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 364–376. [Google Scholar]
- Erickson, C.; Driscoll, M.S. Melanoma epidemic: Facts and controversies. Clin. Dermatol. 2010, 28, 281–286. [Google Scholar]
- Guitart, J.; Lowe, L.; Piepkorn, M.; Prieto, V.G.; Rabkin, M.S.; Ronan, S.G.; Shea, C.R.; Tron, V.A.; White, W.; Barnhill, R.L. Histological characteristics of metastasizing thin melanomas: A case-control study of 43 cases. Arch. Dermatol. 2002, 138, 603–608. [Google Scholar]
- Riquelme-Mc Loughlin, C.; Sandoval-Clavijo, A.; de Tord, M.B.; Boada, A.; Alos, L.; García, A.; Carrera, C.; Malvehy, J.; Puig, S.; Toll, A.; et al. Prognostic role of microsatellites in melanoma and implications in the American Joint Committee on Cancer classification system: A cohort study. J. Am. Acad. Dermatol. 2023, 88, 338–347. [Google Scholar]
- Miliotes, G.; Albertini, J.; Berman, C.; Heller, R.; Messina, J.; Glass, F.; Cruse, W.; Rapaport, D.; Puleo, C.; Fenske, N.; et al. The tumor biology of melanoma nodal metastases. Am. Surg. 1996, 62, 81–88. [Google Scholar] [PubMed]
- Morton, D.L.; Thompson, J.F.; Cochran, A.J.; Mozzillo, N.; Elashoff, R.; Essner, R.; Nieweg, O.E.; Roses, D.F.; Hoekstra, H.J.; Karakousis, C.P.; et al. Sentinel-node biopsy or nodal observation in melanoma. N. Engl. J. Med. 2006, 355, 1307–1317. [Google Scholar] [CrossRef] [Green Version]
- Rubinstein, J.C.; Han, G.; Jackson, L.; Bulloch, K.; Ariyan, S.; Narayan, D.; Rothberg, B.G.; Han, D. Regression in thin melanoma is associated with nodal recurrence after a negative sentinel node biopsy. Cancer Med. 2016, 5, 2832–2840. [Google Scholar] [CrossRef] [PubMed]
- Osella-Abate, S.; Ribero, S.; Sanlorenzo, M.; Maule, M.M.; Richiardi, L.; Merletti, F.; Tomasini, C.; Marra, E.; Macripò, G.; Fierro, M.T.; et al. Risk factors related to late metastases in 1,372 melanoma patients disease free more than 10 years. Int. J. Cancer 2015, 136, 2453–2457. [Google Scholar] [CrossRef] [PubMed]
- Barreiro-Capurro, A.; Andrés-Lencina, J.J.; Podlipnik, S.; Carrera, C.; Requena, C.; Manrique-Silva, E.; Quaglino, P.; Tonella, L.; Jaka, A.; Richarz, N.; et al. Differences in cutaneous melanoma survival between the 7th and 8th edition of the American Joint Committee on Cancer (AJCC). A multicentric population-based study. Eur. J. Cancer 2021, 145, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Basset-Seguin, N.; Bastholt, L.; Bataille, V.; Del Marmol, V.; Dréno, B.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: Diagnostics: Update 2022. Eur. J. Cancer 2022, 170, 236–255. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, S.M.; Cazzaniga, S.; Kaufmann, L.S.; Hunger, R.E.; Jafari, S.M.S. A Retrospective Cohort Study on Patients with Lentigo Maligna Melanoma. Dermatology 2019, 235, 340–345. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, J.G.; Yu, X.Q.; McCarthy, W.H.; Thompson, J.F. Prognosis for patients with thin cutaneous melanoma: Long-term survival data from New South Wales Central Cancer Registry and the Sydney Melanoma Unit. Cancer 2003, 98, 1223–1231. [Google Scholar] [CrossRef]
- Isaksson, K.; Mikiver, R.; Eriksson, H.; Lapins, J.; Nielsen, K.; Ingvar, C.; Lyth, J. Survival in 31 670 patients with thin melanomas: A Swedish population-based study. Br. J. Dermatol. 2021, 184, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Tas, F. Metastatic behavior in melanoma: Timing, pattern, survival, and influencing factors. J. Oncol. 2012, 2012, 647684. [Google Scholar] [CrossRef] [Green Version]
- Meier, F.; Will, S.; Ellwanger, U.; Schlagenhauff, B.; Schittek, B.; Rassner, G.; Garbe, C. Metastatic pathways and time courses in the orderly progression of cutaneous melanoma. Br. J. Dermatol. 2002, 147, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Kalady, M.F.; White, R.R.; Johnson, J.L.; Tyler, D.S.; Seigler, H.F. Thin melanomas: Predictive lethal characteristics from a 30-year clinical experience. Ann. Surg. 2003, 238, 528–535; discussion 535–537. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.N.; Scolyer, R.A.; Thompson, J.F. Long-Term Survival of Patients with Thin (T1) Cutaneous Melanomas: A Breslow Thickness Cut Point of 0.8 mm Separates Higher-Risk and Lower-Risk Tumors. Ann. Surg. Oncol. 2018, 25, 894–902. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Center n = 204, 0 missing | N(%) |
| Barcelona | 36(17.6) |
| Badalona | 18(8.8) |
| Valencia | 34(16.7) |
| Turin | 98(48.0) |
| Bologna | 18(8.8) |
| Sex (n = 204, 0 missing) | |
| Male | 100(49.0) |
| Female | 104(51.0) |
| Age at diagnosis (median, IQR, in years, 0 missing) | 52.5(40.0,64.9) |
| Year at diagnosis (median, IQR, in years, 0 missing) Year at latest follow-up or death (median, IQR, in years, 0 missing) | 2001(1992,2007) 2012(2003,2018) |
| Body site (n = 204, 0 missing) | |
| Head/Neck | 26(12.7) |
| Trunk | 96(47.1) |
| Arms | 27(13.2) |
| Legs | 55(27.0) |
| Breslow score (median, IQR, 0 missing) | 0.8(0.6,0.9) |
| Ulceration (n = 203, 1 missing) | |
| No | 183(90.2) |
| Yes | 20(9.8) |
| Histological subtype (n = 194, 10 missing) | |
| SSM | 155(79.9) |
| LMM | 14(7.2) |
| NM | 13(6.7) |
| Sentinel lymph node biopsy (n = 204, 0 missing) | |
| No | 147(72.1) |
| Yes | 57(27.9) |
| Regional nodal | 30(14.7) |
| Distant or subcutaneous | 125(61.3) |
| Elapsed time between diagnosis and first progression (median, IQR, years, 1 missing) | 3.10 (1.09,5.24) |
| Variable | Univariate Sub-HR | 95% CI | Multivariable Sub-HR | 95% CI |
|---|---|---|---|---|
| Sex | ||||
| Male | 1.00 | ref | 1.00 | ref |
| Female | 0.90 | 0.62,1.31 | 0.83 | 0.54,1.27 |
| Body site | ||||
| Head/Neck | 0.98 | 0.56,1.71 | 1.50 | 0.69,3.26 |
| Trunk | 1.00 | ref | 1.00 | ref |
| Arms | 0.87 | 0.48,1.56 | 0.94 | 0.52,1.71 |
| Legs | 1.02 | 0.66,1.59 | 1.06 | 0.63,1.78 |
| Breslow score (unit increase) | 1.73 | 0.76,3.94 | 2.13 | 0.80,5.66 |
| Ulceration | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 1.40 | 0.76,2.58 | 1.48 | 0.82,2.70 |
| Histological subtype | ||||
| SSM | 1.00 | ref | 1.00 | ref |
| LMM | 0.53 | 0.26,1.06 | 0.32 | 0.14,0.76 |
| NM | 1.01 | 0.45,2.28 | 1.02 | 0.43,2.45 |
| ALM | 0.61 | 0.22,1.70 | 0.65 | 0.21,1.98 |
| Sentinel lymph node | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 0.84 | 0.54,1.31 | 0.79 | 0.50,1.25 |
| Type of first progression | ||||
| Local | 1.00 | ref | 1.00 | ref |
| Nodal | 0.87 | 0.49,1.55 | 0.85 | 0.45,1.58 |
| Distant | 0.77 | 0.52,1.15 | 0.67 | 0.42,1.05 |
| Age at diagnosis (unit increase) | 1.00 | 0.99,1.02 | 1.01 | 0.99,1.02 |
| Elapsed time between diagnosis and first progression (years) | ||||
| [0–1) | 1.00 | ref | 1.00 | ref |
| [1–2) | 1.47 | 0.74,2.89 | 1.26 | 0.60,2.65 |
| [2–3) | 1.80 | 0.89,3.64 | 1.72 | 0.83,3.53 |
| 3+ | 1.15 | 0.67,1.99 | 1.10 | 0.62,1.95 |
| Variable | Univariate Sub-HR | 95% CI | Multivariable Sub-HR | 95% CI |
|---|---|---|---|---|
| Sex | ||||
| Male | 1.00 | ref | 1.00 | ref |
| Female | 1.19 | 0.68,2.08 | 1.04 | 0.48,2.25 |
| Body site | ||||
| Head/Neck | 1.25 | 0.53,2.92 | 1.20 | 0.41,3.48 |
| Trunk | 1.00 | ref | 1.00 | ref |
| Arms | 0.51 | 0.16,1.62 | 0.47 | 0.13,1.72 |
| Legs | 0.98 | 0.54,1.83 | 0.63 | 0.27,1.47 |
| Breslow score (unit increase) | 0.55 | 0.17,1.83 | 0.46 | 0.09,2.29 |
| Ulceration | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 0.37 | 0.12,1.13 | 0.32 | 0.08,1.23 |
| Histological subtype | ||||
| SSM | 1.00 | ref | 1.00 | ref |
| LMM | 0.59 | 0.17,2.05 | 0.34 | 0.09,1.33 |
| NM | 1.32 | 0.40,4.36 | 1.80 | 0.40,8.11 |
| ALM | 1.20 | 0.39,3.75 | 1.44 | 0.40,5.17 |
| Sentinel lymph node | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 0.92 | 0.49,1.72 | 1.37 | 0.67,2.81 |
| Type of second progression | ||||
| Local | 1.00 | ref | 1.00 | ref |
| Nodal | 0.61 | 0.33,1.15 | 0.52 | 0.23,1.18 |
| Distant | 1.02 | 0.53,1.95 | 1.09 | 0.44,2.65 |
| Age at diagnosis (unit increase) | 0.99 | 0.97,1.01 | 0.98 | 0.96,1.01 |
| Elapsed time between diagnosis and second progression (years) | ||||
| [0–2) | 1.00 | ref | 1.00 | ref |
| [2–4) | 0.93 | 0.33,2.64 | 0.78 | 0.25,2.49 |
| [4–6) | 1.24 | 0.46,3.37 | 1.11 | 0.31,4.03 |
| 6+ | 1.26 | 0.47,3.33 | 1.20 | 0.36,3.98 |
| Variable | Univariate Sub-HR | 95% CI | Multivariable Sub-HR | 95% CI |
|---|---|---|---|---|
| Sex | ||||
| Male | 1.00 | ref | 1.00 | ref |
| Female | 0.70 | 0.46,1.06 | 0.96 | 0.58,1.60 |
| Body site | ||||
| Head/Neck | 0.41 | 0.18,0.91 | 1.11 | 0.53,2.33 |
| Trunk | 1.00 | ref | 1.00 | ref |
| Arms | 0.47 | 0.23,0.96 | 0.52 | 0.23,1.21 |
| Legs | 0.44 | 0.27,0.74 | 0.59 | 0.29,1.19 |
| Breslow score (unit increase) | 2.90 | 1.00,8.43 | 2.46 | 0.60,10.10 |
| Ulceration | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 1.68 | 0.91,3.11 | 1.73 | 0.79,3.75 |
| Histological subtype | ||||
| SSM | 1.00 | ref | 1.00 | ref |
| LMM | 0.34 | 0.11,1.06 | 0.43 | 0.09,2.08 |
| NM | 1.11 | 0.50,2.44 | 1.11 | 0.34,3.61 |
| ALM | 1.44 | 0.54,3.83 | 2.18 | 0.58,8.10 |
| Sentinel lymph node | ||||
| No | 1.00 | ref | 1.00 | ref |
| Yes | 1.00 | 0.61,1.63 | 0.84 | 0.42,1.67 |
| Type of first progression | ||||
| Local | 1.00 | ref | 1.00 | ref |
| Nodal | 1.33 | 1.69,8.47 | 3.13 | 1.37,7.15 |
| Distant | 2.10 | 3.40,19.81 | 2.73 | 1.28,5.81 |
| Type of second progression | ||||
| None | 1.00 | ref | 1.00 | ref |
| Local | 3.93 | 1.65,9.34 | 5.78 | 2.56,13.06 |
| Nodal | 14.19 | 8.28,24.31 | 9.89 | 5.41,18.07 |
| Distant | 12.05 | 6.48,22.38 | 8.67 | 4.55,16.52 |
| Type of third progression | ||||
| None | 1.00 | ref | 1.00 | ref |
| Local | 0.85 | 0.13,5.68 | 0.68 | 0.19,2.43 |
| Nodal | 3.73 | 2.53,5.49 | 1.43 | 0.81,2.51 |
| Distant | 3.66 | 2.01,6.68 | 2.51 | 1.29,4.89 |
| Age at diagnosis (unit increase) | 1.00 | 0.99,1.02 | 1.01 | 0.99,1.03 |
| Elapsed time between diagnosis and first progression (years) | ||||
| [0–1) | 1.00 | ref | 1.00 | ref |
| [1–2) | 1.05 | 0.45,2.48 | 1.29 | 0.54,3.07 |
| [2–3) | 1.78 | 0.81,3.93 | 1.35 | 0.53,3.46 |
| 3+ | 1.29 | 0.70,2.38 | 1.34 | 0.61,2.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chousakos, E.; Zugna, D.; Dika, E.; Boada, A.; Podlipnik, S.; Carrera, C.; Malvehy, J.; Puig, S.; Requena, C.; Manrique-Silva, E.; et al. Topographical and Chronological Analysis of Thin Cutaneous Melanoma’s Progressions: A Multicentric Study. Cancers 2023, 15, 3989. https://doi.org/10.3390/cancers15153989
Chousakos E, Zugna D, Dika E, Boada A, Podlipnik S, Carrera C, Malvehy J, Puig S, Requena C, Manrique-Silva E, et al. Topographical and Chronological Analysis of Thin Cutaneous Melanoma’s Progressions: A Multicentric Study. Cancers. 2023; 15(15):3989. https://doi.org/10.3390/cancers15153989
Chicago/Turabian StyleChousakos, Emmanouil, Daniela Zugna, Emi Dika, Aram Boada, Sebastian Podlipnik, Cristina Carrera, Josep Malvehy, Susana Puig, Celia Requena, Esperanza Manrique-Silva, and et al. 2023. "Topographical and Chronological Analysis of Thin Cutaneous Melanoma’s Progressions: A Multicentric Study" Cancers 15, no. 15: 3989. https://doi.org/10.3390/cancers15153989
APA StyleChousakos, E., Zugna, D., Dika, E., Boada, A., Podlipnik, S., Carrera, C., Malvehy, J., Puig, S., Requena, C., Manrique-Silva, E., Nagore, E., Quaglino, P., Senetta, R., & Ribero, S. (2023). Topographical and Chronological Analysis of Thin Cutaneous Melanoma’s Progressions: A Multicentric Study. Cancers, 15(15), 3989. https://doi.org/10.3390/cancers15153989