
Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Data Collection
2.3. Definition of PST
2.4. Primary and Secondary Outcomes
2.5. 11C-Methionine PET-MRI
2.6. Statistical Analysis
3. Results
3.1. Demographics and Baseline Characteristics
3.2. Etiology for PST and Patient Outcome
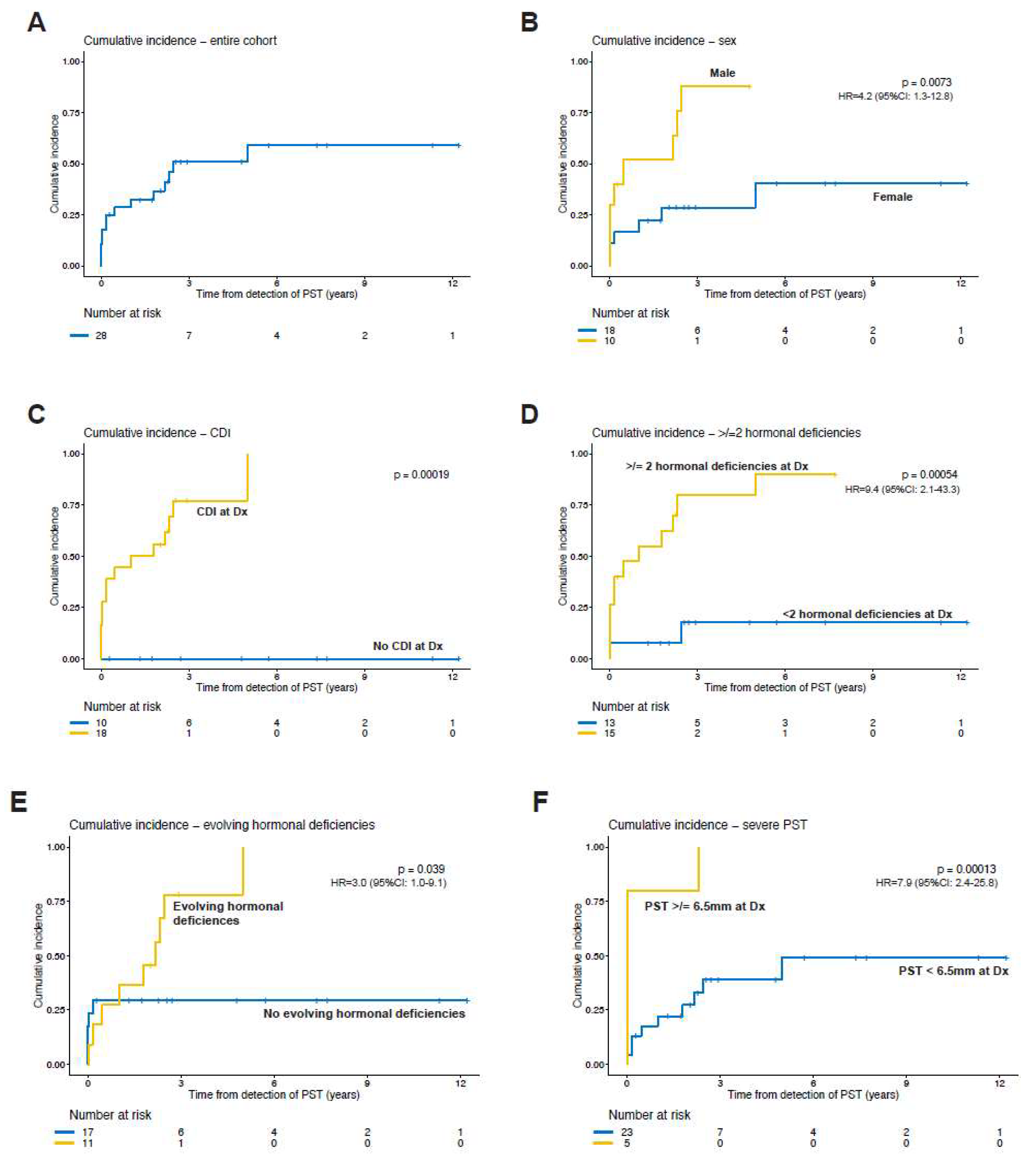
3.3. Risk Factors for Underlying Neoplasm
3.4. Clinical Course and Endocrine Outcome
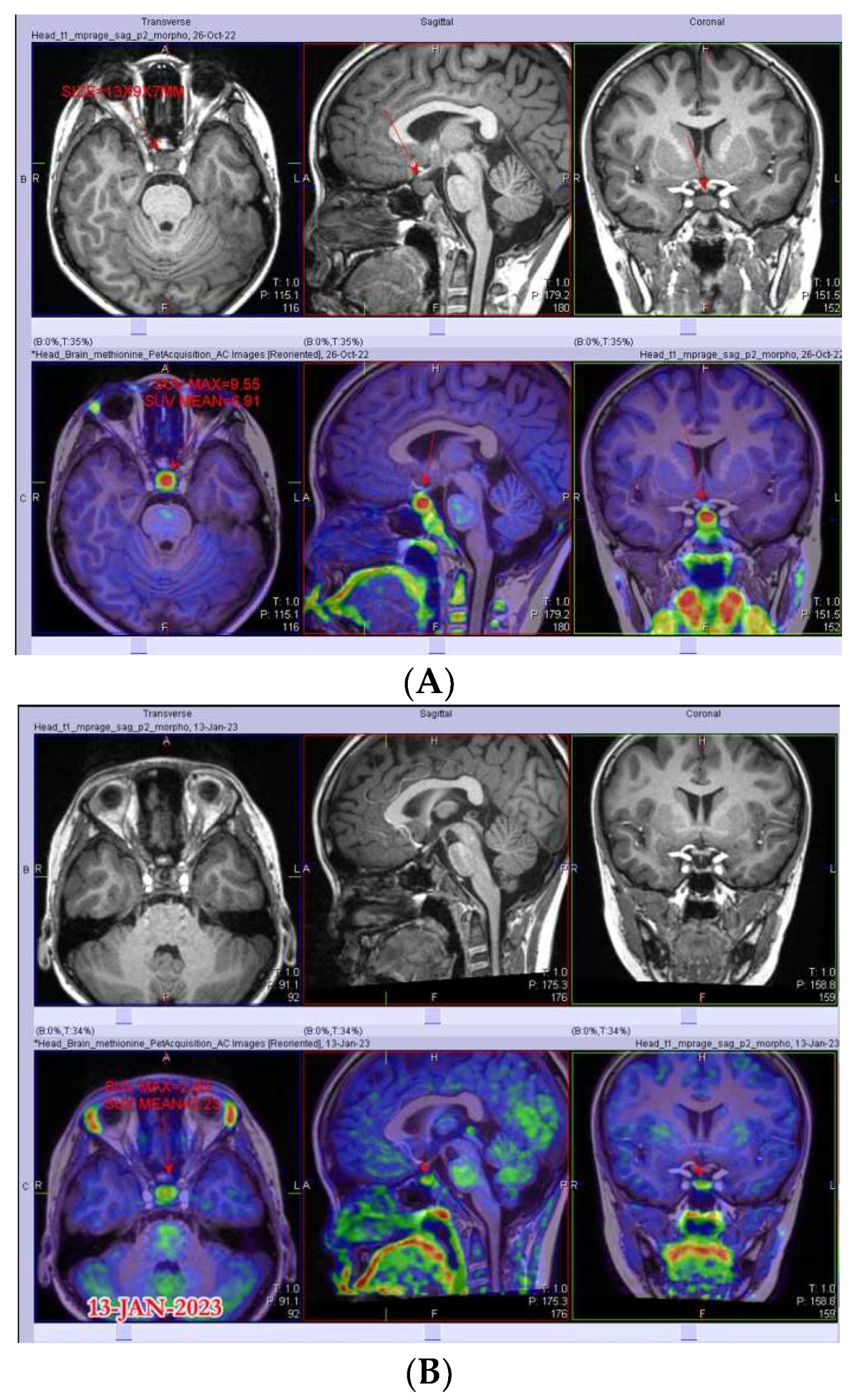
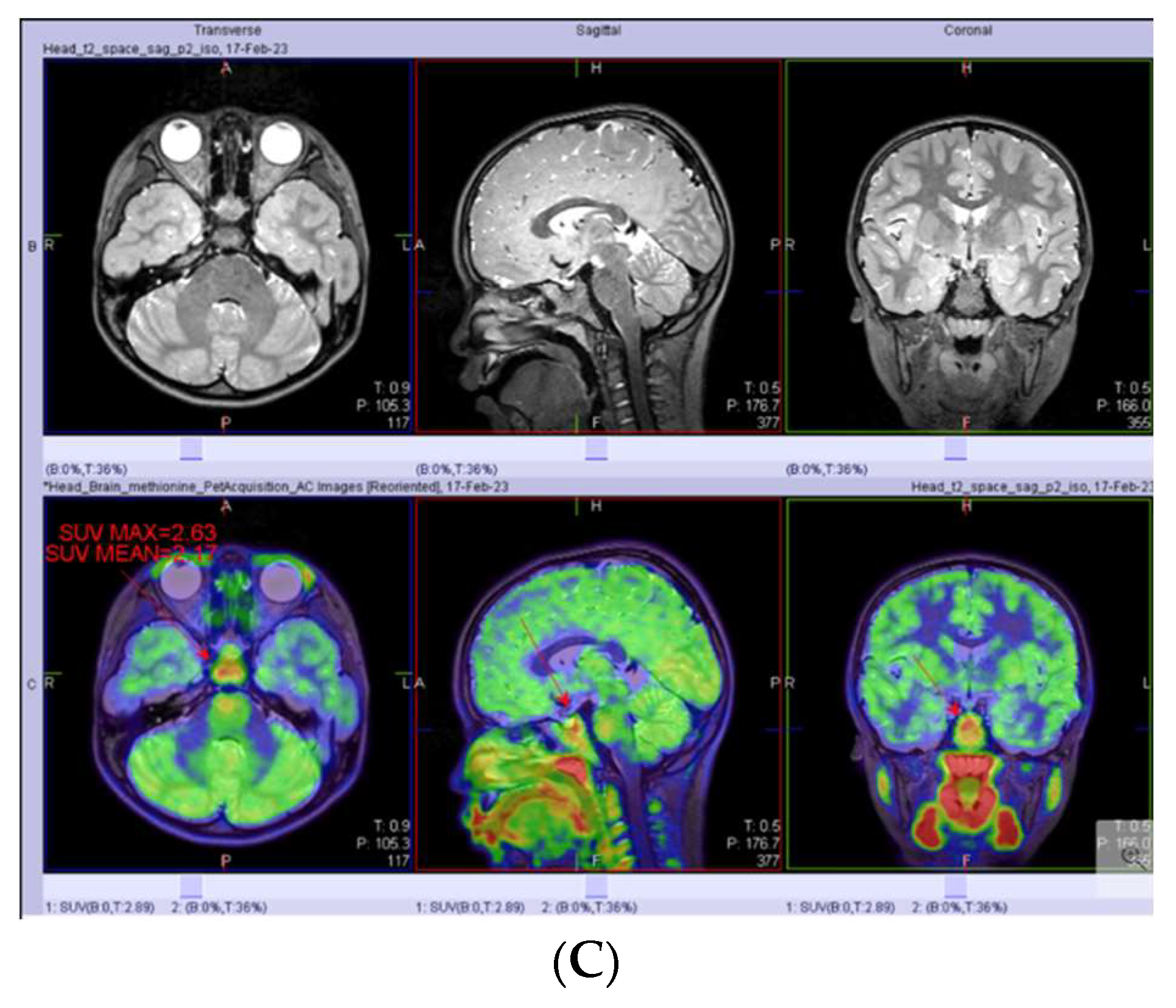
3.5. PET-MRI as a Complementary Tool in PST Diagnostics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sbardella, E.; Joseph, R.N.; Jafar-Mohammadi, B.; Isidori, A.M.; Cudlip, S.; Grossman, A.B. Pituitary stalk thickening: The role of an innovative MRI imaging analysis which may assist in determining clinical management. Eur. J. Endocrinol. 2016, 175, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Ni, M.; Xu, Y.; Zhong, L.Y. Pituitary Stalk Germ Cell Tumors: Retrospective Case Series and Literature Review. Int. J. Endocrinol. 2022, 2022, 9213220. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Hou, J.; Liu, X.; Wang, L.; Li, G. Causes and Follow-Up of Central Diabetes Insipidus in Children. Int. J. Endocrinol. 2019, 2019, 5303765. [Google Scholar] [CrossRef]
- Redhu, R.; Nadkarni, T.; Mahesh, R. Diabetes insipidus associated with a thickened pituitary stalk in a case of Langerhans Cell Histiocytosis. J. Pediatr. Neurosci. 2011, 6, 62–64. [Google Scholar] [PubMed]
- Kluczyński, Ł.; Gilis-Januszewska, A.; Godlewska, M.; Wójcik, M.; Zygmunt-Górska, A.; Starzyk, J.; Hubalewska-Dydejczyk, A. Diversity of Pathological Conditions Affecting Pituitary Stalk. J. Clin. Med. 2021, 10, 1692. [Google Scholar] [CrossRef]
- Alter, C.A.; Bilaniuk, L.T. Utility of magnetic resonance imaging in the evaluation of the child with central diabetes insipidus. J. Pediatr. Endocrinol. Metab. 2002, 15 (Suppl. 2), 681–687. [Google Scholar] [CrossRef]
- Prosch, H.; Grois, N.; Bökkerink, J.; Prayer, D.; Leuschner, I.; Minkov, M.; Gadner, H. Central diabetes insipidus: Is it Langerhans cell histiocytosis of the pituitary stalk? A diagnostic pitfall. Pediatr. Blood Cancer 2006, 46, 363–366. [Google Scholar] [CrossRef]
- Robison, N.J.; Prabhu, S.P.; Sun, P.; Chi, S.N.; Kieran, M.W.; Manley, P.E.; Cohen, L.E.; Goumnerova, L.; Smith, E.R.; Scott, R.M.; et al. Predictors of neoplastic disease in children with isolated pituitary stalk thickening. Pediatr. Blood Cancer 2013, 60, 1630–1635. [Google Scholar] [CrossRef]
- Maghnie, M. Diabetes insipidus. Horm. Res. 2003, 59 (Suppl. 1), 42–54. [Google Scholar] [CrossRef]
- Mootha, S.L.; Barkovich, A.J.; Grumbach, M.M.; Edwards, M.S.; Gitelman, S.E.; Kaplan, S.L.; Conte, F.A. Idiopathic hypothalamic diabetes insipidus, pituitary stalk thickening, and the occult intracranial germinoma in children and adolescents. J. Clin. Endocrinol. Metab. 1997, 82, 1362–1367. [Google Scholar]
- Turcu, A.F.; Erickson, B.J.; Lin, E.; Guadalix, S.; Schwartz, K.; Scheithauer, B.W.; Atkinson, J.L.D.; Young, W.F. Pituitary stalk lesions: The Mayo Clinic experience. J. Clin. Endocrinol. Metab. 2013, 98, 1812–1818. [Google Scholar] [CrossRef]
- Czernichow, P.; Garel, C.; Léger, J. Thickened pituitary stalk on magnetic resonance imaging in children with central diabetes insipidus. Horm. Res. 2000, 53 (Suppl. 3), 61–64. [Google Scholar] [CrossRef]
- Leger, J.; Velasquez, A.; Garel, C.; Hassan, M.; Czernichow, P. Thickened pituitary stalk on magnetic resonance imaging in children with central diabetes insipidus. J. Clin. Endocrinol. Metab. 1999, 84, 1954–1960. [Google Scholar] [CrossRef]
- Yoon, S.C.; Shin, C.H.; Yang, S.W.; Lee, S.Y. Clinical and radiological features of pituitary stalk lesions in children and adolescents. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 202–207. [Google Scholar] [CrossRef]
- Halefoglu, A.M. Magnetic resonance imaging of thickened pituitary stalk proceeding to Langerhans cell histiocytosis in a child. Australas. Radiol. 2006, 50, 175–178. [Google Scholar] [CrossRef]
- Moszczyńska, E.; Baszyńska-Wilk, M.; Zasada, K.; Majak, D.; Szaniawska, M.; Szalecki, M. Pituitary stalk thickening in patients under 18 years of age—The most common causes and diagnostic procedures. Pediatr. Endocrinol. Diabetes Metab. 2022, 28, 213–227. [Google Scholar] [CrossRef]
- Langlois, F.; Varlamov, E.V.; Fleseriu, M. Hypophysitis, the Growing Spectrum of a Rare Pituitary Disease. J. Clin. Endocrinol. Metab. 2022, 107, 10–28. [Google Scholar] [CrossRef]
- Di Iorgi, N.; Morana, G.; Maghnie, M. Pituitary stalk thickening on MRI: When is the best time to re-scan and how long should we continue re-scanning for? Clin. Endocrinol. 2015, 83, 449–455. [Google Scholar] [CrossRef]
- Uddin, A.; Kalladi Puthanpurayil, S. Central Diabetes Insipidus with Pituitary Stalk Thickening. In Diabetes Insipidus in Children: A Pocket Guide; Springer: Berlin/Heidelberg, Germany, 2021; pp. 41–53. [Google Scholar]
- Devuyst, F.; Kazakou, P.; Balériaux, D.; Alexopoulou, O.; Burniat, A.; Salenave, S.; Chanson, P.; Corvilain, B.; Maiter, D. Central diabetes insipidus and pituitary stalk thickening in adults: Distinction of neoplastic from non-neoplastic lesions. Eur. J. Endocrinol. 2020, 183, 95–105. [Google Scholar] [CrossRef]
- Moszczyńska, E.; Kunecka, K.; Baszyńska-Wilk, M.; Perek-Polnik, M.; Majak, D.; Grajkowska, W. Pituitary Stalk Thickening: Causes and Consequences. The Children’s Memorial Health Institute Experience and Literature Review. Front. Endocrinol. 2022, 13, 868558. [Google Scholar] [CrossRef]
- Chaudhary, V.; Bano, S. Imaging of pediatric pituitary endocrinopathies. Indian J. Endocrinol. Metab. 2012, 16, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Capra, M.; Wherrett, D.; Weitzman, S.; Dirks, P.; Hawkins, C.; Bouffet, E. Pituitary stalk thickening and primary central nervous system lymphoma. J. Neurooncol. 2004, 67, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Jian, F.; Bian, L.; Sun, S.; Yang, J.; Chen, X.; Chen, Y.; Ma, Q.; Miao, F.; Wang, W.; Ning, G.; et al. Surgical biopsies in patients with central diabetes insipidus and thickened pituitary stalks. Endocrine 2014, 47, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Beni-Adani, L.; Sainte-Rose, C.; Zerah, M.; Brunelle, F.; Constantini, S.; Renier, D.; Lellouch-Tubiana, A.; Leger, J.; Pierre-Kahn, A. Surgical implications of the thickened pituitary stalk accompanied by central diabetes insipidus. J. Neurosurg. 2005, 103 (Suppl. 2), 142–147. [Google Scholar] [CrossRef] [PubMed]
- Day, E.L.; Smith, E.R.; Fehnel, K.P. Single-institution case series of pituitary biopsy for suspected germinoma in the pediatric population: Diagnostic utility, operative risks, and biopsy approaches. Sci. Rep. 2020, 10, 15257. [Google Scholar] [CrossRef]
- Cerbone, M.; Visser, J.; Bulwer, C.; Ederies, A.; Vallabhaneni, K.; Ball, S.; Kamaly-Asl, I.; Grossman, A.; Gleeson, H.; Korbonits, M.; et al. Management of children and young people with idiopathic pituitary stalk thickening, central diabetes insipidus, or both: A national clinical practice consensus guideline. Lancet Child Adolesc. Health 2021, 5, 662–676. [Google Scholar] [CrossRef]
- Zhou, X.; Zhu, H.; Yao, Y.; Lian, X.; Feng, F.; Wang, L.; Liu, S.; Deng, K.; You, H.; Yang, H.; et al. Etiological Spectrum and Pattern of Change in Pituitary Stalk Thickening: Experience in 321 Patients. J. Clin. Endocrinol. Metab. 2019, 104, 3419–3427. [Google Scholar] [CrossRef]
- Ji, X.; Wang, Z.; Wang, W.; Gao, L.; Guo, X.; Feng, C.; Lian, W.; Deng, K.; Xing, B. Clinical Characteristics of Pediatric Patients With Sellar and Suprasellar Lesions Who Initially Present With Central Diabetes Insipidus: A Retrospective Study of 55 Cases From a Large Pituitary Center in China. Front. Endocrinol. 2020, 11, 76. [Google Scholar] [CrossRef]
- Satogami, N.; Miki, Y.; Koyama, T.; Kataoka, M.; Togashi, K. Normal pituitary stalk: High-resolution MR imaging at 3T. Am. J. Neuroradiol. 2010, 31, 355–359. [Google Scholar] [CrossRef]
- Di Iorgi, N.; Allegri, A.E.M.; Napoli, F.; Calcagno, A.; Calandra, E.; Fratangeli, N.; Vannati, M.; Rossi, A.; Bagnasco, F.; Haupt, R.; et al. Central diabetes insipidus in children and young adults: Etiological diagnosis and long-term outcome of idiopathic cases. J. Clin. Endocrinol. Metab. 2014, 99, 1264–1272. [Google Scholar] [CrossRef]
- Marchand, I.; Barkaoui, M.A.; Garel, C.; Polak, M.; Donadieu, J.; Committee, W. Central diabetes insipidus as the inaugural manifestation of Langerhans cell histiocytosis: Natural history and medical evaluation of 26 children and adolescents. J. Clin. Endocrinol. Metab. 2011, 96, E1352–E1360. [Google Scholar] [CrossRef]
- Skrypek, M.; Brown, A.; Pape-Blabolil, J.; Bendelsmith, C.; Patel, S.; Patterson, R.; Abuzzahab, M.J.; Ingram, K.; Linabery, A.; Bendel, A. EPID-13. Isolated Pituitary Stalk Thickening (IPST) in Children: Natural History and Predictors of Neoplastic Disease. Neuro-Oncology 2018, 20 (Suppl. 2), i83. [Google Scholar] [CrossRef][Green Version]
- Simmons, G.E.; Suchnicki, J.E.; Rak, K.M.; Damiano, T.R. MR imaging of the pituitary stalk: Size, shape, and enhancement pattern. AJR Am. J. Roentgenol. 1992, 159, 375–377. [Google Scholar] [CrossRef]
- Liu, S.Y.; Tung, Y.C.; Lee, C.T.; Liu, H.M.; Peng, S.F.; Wu, M.Z.; Kuo, M.-F.; Tsai, W.-Y. Clinical characteristics of central diabetes insipidus in Taiwanese children. J. Formos. Med. Assoc. 2013, 112, 616–620. [Google Scholar] [CrossRef]
- Liu, A.P.Y.; Liu, Q.; Shing, M.M.K.; Ku, D.T.L.; Fu, E.; Luk, C.W.; Ling, S.-C.; Cheng, K.K.F.; Kwong, D.L.W.; Ho, W.W.S.; et al. Incidence and Outcomes of CNS Tumors in Chinese Children: Comparative Analysis With the Surveillance, Epidemiology, and End Results Program. JCO Glob. Oncol. 2020, 6, 704–721. [Google Scholar] [CrossRef]
- Gao, Y.; Jiang, J.; Liu, Q. Clinicopathological and immunohistochemical features of primary central nervous system germ cell tumors: A 24-years experience. Int. J. Clin. Exp. Pathol. 2014, 7, 6965–6972. [Google Scholar]
- Qaddoumi, I.; Merchant, T.E.; Boop, F.A.; Gajjar, A. Diagnostic delay in children with central nervous system tumors and the need to improve education. J. Neurooncol. 2019, 145, 591–592. [Google Scholar] [CrossRef]
- Arnautovic, A.; Billups, C.; Broniscer, A.; Gajjar, A.; Boop, F.; Qaddoumi, I. Delayed diagnosis of childhood low-grade glioma: Causes, consequences, and potential solutions. Childs Nerv. Syst. 2015, 31, 1067–1077. [Google Scholar] [CrossRef]
- Park, Y.J.; Lee, J.W.; Cho, H.W.; Choe, Y.S.; Lee, K.H.; Choi, J.Y.; Sung, K.W.; Moon, S.H. Value of C-11 methionine PET/CT in patients with intracranial germinoma. PLoS ONE 2022, 17, e0263690. [Google Scholar] [CrossRef]
- Treglia, G.; Muoio, B.; Trevisi, G.; Mattoli, M.V.; Albano, D.; Bertagna, F.; Giovanella, L. Diagnostic Performance and Prognostic Value of PET/CT with Different Tracers for Brain Tumors: A Systematic Review of Published Meta-Analyses. Int. J. Mol. Sci. 2019, 20, 4669. [Google Scholar] [CrossRef]
- Kawai, N.; Miyake, K.; Yamamoto, Y.; Nishiyama, Y.; Maeda, Y.; Kageji, T.; Tamiya, T. Use of 11C-methionine positron emission tomography in basal germinoma: Assessment of treatment response and residual tumor. Childs Nerv. Syst. 2009, 25, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Fujii, Y.; Saito, Y.; Ogawa, T.; Fujii, S.; Kamitani, H.; Kondo, S.; Horie, Y.; Togawa, M.; Senda, M.; Maegaki, Y.; et al. Basal ganglia germinoma: Diagnostic value of MR spectroscopy and (11)C-methionine positron emission tomography. J. Neurol. Sci. 2008, 270, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Okochi, Y.; Nihashi, T.; Fujii, M.; Kato, K.; Okada, Y.; Ando, Y.; Maesawa, S.; Takebayashi, S.; Wakabayashi, T.; Naganawa, S. Clinical use of (11)C-methionine and (18)F-FDG-PET for germinoma in central nervous system. Ann. Nucl. Med. 2014, 28, 94–102. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Koulouri, O.; Kandasamy, N.; Hoole, A.C.; Gillett, D.; Heard, S.; Powlson, A.S.; O’donovan, D.G.; Annamalai, A.K.; Simpson, H.L.; A Akker, S.; et al. Successful treatment of residual pituitary adenoma in persistent acromegaly following localisation by 11C-methionine PET co-registered with MRI. Eur. J. Endocrinol. 2016, 175, 485–498. [Google Scholar] [CrossRef]
- Kawai, N.; Miyake, K.; Nishiyama, Y.; Yamamoto, Y.; Miki, A.; Haba, R.; Imai, T.; Tamiya, T.; Nagao, S. Targeting optimal biopsy location in basal ganglia germinoma using (11)C-methionine positron emission tomography. Surg. Neurol. 2008, 70, 408–413; discussion 13. [Google Scholar] [CrossRef]
- Sonoda, Y.; Kumabe, T.; Sugiyama, S.-I.; Kanamori, M.; Yamashita, Y.; Saito, R.; Ariga, H.; Takai, Y.; Tominaga, T. Germ cell tumors in the basal ganglia: Problems of early diagnosis and treatment. J. Neurosurg. Pediatr. 2008, 2, 118–124. [Google Scholar] [CrossRef]
- Schönberger, S.; Mohseni, M.M.; Ellinger, J.; Tran, G.V.Q.; Becker, M.; Claviez, A.; Classen, C.-F.; Hermes, B.; Driever, P.H.; Jorch, N.; et al. MicroRNA-profiling of miR-371~373- and miR-302/367-clusters in serum and cerebrospinal fluid identify patients with intracranial germ cell tumors. J. Cancer Res. Clin. Oncol. 2023, 149, 791–802. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Number | Final Diagnosis | Sex | Age of Dx of PST (Years) | Growth Hormone | Gonadal Axis | Thyroid Axis | Adrenal Axis | Central Diabetes Insipidus | CPP | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient with Oncological Diagnosis | At Dx | Pre Tx | Last FU | At Dx | Pre Tx | Last FU | At Dx | Pre Tx | Last FU | At Dx | Pre Tx | Last FU | At Dx | Pre Tx | Last FU | At Dx | |||
| 1 | Germinoma | F | 10.3 | ↓ | ↓ | ↓ | Unknown | ↓ | Normal | Normal | Normal | Normal | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 3 | Germinoma | F | 5.9 | ↓ | ↓ | ↓ | Unknown | Unknown | Normal | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 4 | Germinoma | M | 16.5 | ↓ | ↓ | Unknown | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 8 | NGGCT | M | 8.2 | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | Normal | ↓ | ↓ | ↓ | ↓ | ↓ | Yes | Yes | Yes | No |
| 9 | LCH | F | 5.2 | Normal | Normal | ↓ | Normal | Normal | Normal | Normal | Normal | ↓ | Normal | Normal | Normal | Yes | Yes | Yes | No |
| 10 | Germinoma | F | 9.4 | ↓ | ↓ | ↓ | Unknown | Unknown | Unknown | ↓ | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 13 | Germinoma | M | 14.6 | Normal | Unknown | Unknown | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 14 | NGGCT | M | 9.5 | Normal | Normal | ↓ | Unknown | ↓ | Unknown | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | Yes | Yes | Yes | No |
| 16 | Germinoma | M | 13.4 | ↓ | ↓ | ↓ | ↓ | ↓ | Normal | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | Yes | Yes | Yes | No |
| 20 | Germinoma | F | 12 | ↓ | ↓ | Unknown | Normal | ↓ | ↓ | ↓ | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 24 | Germinoma | M | 10.9 | ↓ | ↓ | ↓ | Normal | Normal | Normal | ↓ | ↓ | ↓ | ↓ | ↓ | Normal | Yes | Yes | Yes | No |
| 25 | Germinoma | F | 12.2 | ↓ | ↓ | Unknown | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | Yes | Yes | Yes | No |
| 26 | Germinoma | M | 15.4 | ↓ | ↓ | Normal | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Normal | ↓ | ↓ | Yes | Yes | Yes | No |
| 28 | Germinoma | M | 14.1 | ↓ | ↓ | ↓ | ↓ | ↓ | Normal | Normal | Normal | Normal | ↓ | ↓ | ↓ | Yes | Yes | Yes | No |
| Patient Number | Final Diagnosis | Sex | Age of Dx of PST (Years) | Growth Hormone | Gonadal Axis | Thyroid Axis | Adrenal Axis | Central Diabetes Insipidus | CPP | ||||||||||
| Patient with Non-Oncological Diagnosis | At Dx | Last FU | At Dx | Last FU | At Dx | Last FU | At Dx | Last FU | At Dx | Last FU | At Dx | ||||||||
| 2 | Idiopathic | F | 10.9 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Yes | Yes | No | |||||
| 5 | Idiopathic | M | 15.6 | ↓ | ↓ | ↓ | ↓ | Normal | Normal | Normal | Normal | No | No | No | |||||
| 6 | Idiopathic | F | 10.4 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 7 | Idiopathic | F | 15 | ↓ | ↓ | ↓ | ↓ | Normal | Normal | Normal | Normal | Yes | Yes | No | |||||
| 11 | Idiopathic | F | 3.8 | Normal | ↓ | Normal | Normal | Normal | Normal | Normal | Normal | Yes | Yes | No | |||||
| 12 | Idiopathic | F | 5.6 | Unknown | ↓ | Normal | Normal | Normal | Normal | Normal | Normal | Yes | Yes | No | |||||
| 15 | Idiopathic | F | 13.8 | Normal | Normal | Normal | Normal | Normal | Normal | ↓ | Normal | No | No | No | |||||
| 17 | Idiopathic | F | 8.8 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 18 | Idiopathic | F | 11.6 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 19 | Idiopathic | F | 9.7 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 21 | Idiopathic | F | 9.7 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 22 | Idiopathic | F | 7.3 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
| 23 | Idiopathic | F | 16.2 | ↓ | ↓ | ↓ | ↓ | Normal | Normal | Normal | Normal | No | No | No | |||||
| 27 | Idiopathic | M | 13.5 | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | No | No | Yes | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.W.T.; Poon, S.W.Y.; Cheung, C.; Wong, C.K.C.; Shing, M.M.K.; Chow, T.T.W.; Lee, S.L.K.; Pang, G.S.W.; Kwan, E.Y.W.; Poon, G.W.K.; et al. Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening. Cancers 2023, 15, 3935. https://doi.org/10.3390/cancers15153935
Li MWT, Poon SWY, Cheung C, Wong CKC, Shing MMK, Chow TTW, Lee SLK, Pang GSW, Kwan EYW, Poon GWK, et al. Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening. Cancers. 2023; 15(15):3935. https://doi.org/10.3390/cancers15153935
Chicago/Turabian StyleLi, Mario W. T., Sarah W. Y. Poon, Claudia Cheung, Chris K. C. Wong, Matthew M. K. Shing, Terry T. W. Chow, Samantha L. K. Lee, Gloria S. W. Pang, Elaine Y. W. Kwan, Grace W. K. Poon, and et al. 2023. "Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening" Cancers 15, no. 15: 3935. https://doi.org/10.3390/cancers15153935
APA StyleLi, M. W. T., Poon, S. W. Y., Cheung, C., Wong, C. K. C., Shing, M. M. K., Chow, T. T. W., Lee, S. L. K., Pang, G. S. W., Kwan, E. Y. W., Poon, G. W. K., Yau, H.-C., Tung, J. Y. L., & Liu, A. P. Y. (2023). Incidence and Predictors for Oncologic Etiologies in Chinese Children with Pituitary Stalk Thickening. Cancers, 15(15), 3935. https://doi.org/10.3390/cancers15153935