
Surgical Interest of an Accurate Real-World Prediction of Primary Systemic Therapy Response in HER2 Breast Cancers

 ,
,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- Inclusion criteria: women over 18 years of age, with HER2 immunophenotype BC [10], who received PST (chemotherapy with Trastuzumab with or without Pertuzumab), and subsequently underwent surgery. HER2 status was determined by immune-histochemistry (IHC) using the HER2 polyclonal antibody (DAKO HercepTest) and in situ hybridization by FISH when 2+. Scoring was performed using the current American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines [11].
- Exclusion criteria: patients diagnosed with BC subtypes other than HER2, who underwent primary surgical treatment, who were metastatic, who were males, or who were under 18 years.
3. Results
3.1. Clinical Features
3.2. Percutaneous Biopsy Histopathological Features
3.3. Radiological Response after PST
3.4. Surgical Approach
3.5. Histopathological Features Surgical Specimen
3.5.1. Patients without Initial Axillary Involvement-cN0
3.5.2. Patients with Positive Initial Axillary Involvement—cN1-3
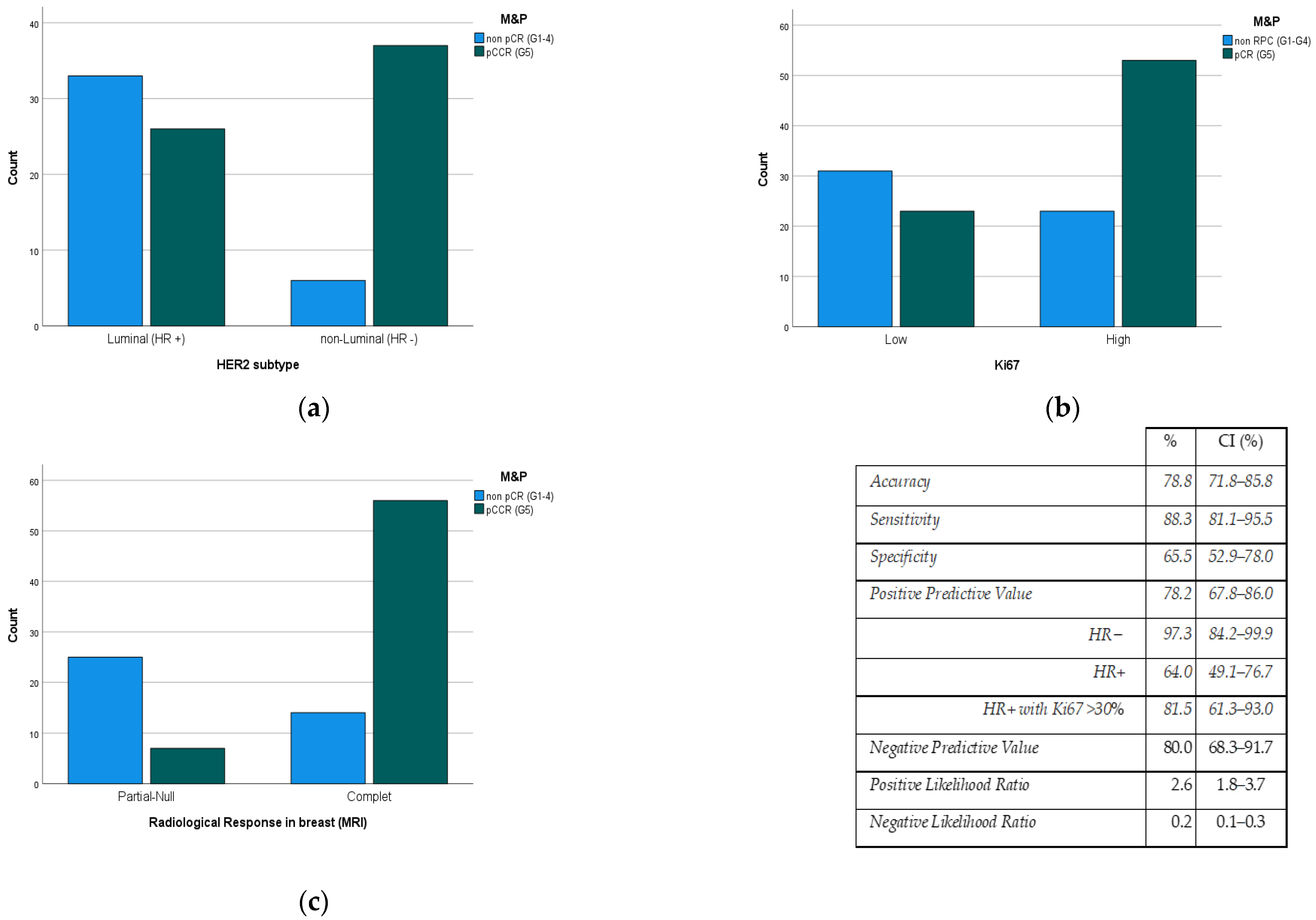
3.6. Relationship between Variables and the Degree of Response by the M&P System
- ER and PR negative status showed higher rates (p < 0.001) of pCR (83.0%/41.8%) than the luminal HER2 subtype (Figure 2a).
- Ki67 Proliferation Index value is directly related (p < 0.006) to the pCR rate (Figure 2b).
- The degree of radiological response had a predictive positive value (PPV) of 78.2% to the pCR rate (p < 0.001) (Figure 2c).
3.7. Relationship between Pathological Response in the Breast and the Axilla
3.8. Multivariate Analysis
4. Discussion
4.1. Clinical Features
4.2. Percutaneous Biopsy Histopathological Features
4.3. Radiological Response after PST
4.4. Surgical Approach
4.5. Histopathological Features of the Surgical Specimen
4.6. Relationship between Pathological Response in Breast and Axilla
4.7. Relationship between Variables and Degree of M&P Response
- HER2 subtype. Our pCR rate was higher than that of Novoa et al. [3], but only in non-luminal HER2 tumors (RH negative). This has been seen in other series [18,26] and is collected in the meta-analyses of Cortazar or Broglio [24,27], which may be due to a cross-resistance between the HER2 and estrogen receptors pathways, which will confer some resistance to therapies aimed at each of them [28].
- KI67. In our study, the value of Ki67 is directly related to the degree of pathological response in the breast (p = 0.001), in the sense that most patients with high Ki67 achieved pCR. There are numerous studies [5,18,31] with similar conclusions, although the problem of this marker is related to its low reproducibility.
- Radiological response after PST. In the daily clinic, MRI is accepted as the gold standard for predicting the degree of response to PST [9], although its PPV does not exceed 80%. Therefore, it would be very useful to have other variables that improve it. In our study, we found that variables such as Ki67 (high) and HER2 subtype (non-luminal HER2) improve the response predictability by up to almost 100%.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, Y.; Wu, S.; Xing, H.; Han, M.; Li, J.; Liu, Y. Development and Validation of a Novel Model for Predicting Prognosis of Non-PCR Patients After Neoadjuvant Therapy for Breast Cancer. Front. Oncol. 2021, 11, 675533. [Google Scholar] [CrossRef] [PubMed]
- Ates, O.; Oksuzoglu, O.B.; Aktas, B.Y.; Karadag, I.; Esen, S.; Karakaya, S.; Uncu, D.; Erol, C.; Gurbuz, M.; Yalcin, B.; et al. Evaluation of Factors Predicting Pathologic Complete Response in Locally Advanced HER2 Positive Breast Cancer Treated with Neoadjuvant Pertuzumab, Trastuzumab and Chemotherapy; Real Life Data. J. BUON 2021, 26, 1398–1404. [Google Scholar] [PubMed]
- Novoa, S.A. Terapia Sistémica Primaria En Cáncer de Mama HER2 Positivo: Factores Pronósticos y Predictores de Respuesta, Datos de Eficacia, Cardiotoxicidad y Seguimiento a Largo Plazo. Ph.D. Thesis, Universidade da Coruña, A Coruña, Spain, 2019. [Google Scholar]
- Carey, L.A.; Dees, E.C.; Sawyer, L.; Gatti, L.; Moore, D.T.; Collichio, F.; Ollila, D.W.; Sartor, C.I.; Graham, M.L.; Perou, C.M. The Triple Negative Paradox: Primary Tumor Chemosensitivity of Breast Cancer Subtypes. Clin. Cancer Res. 2007, 13, 2329–2334. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Konecny, G.E.; Paepke, S.; von Minckwitz, G. Current and Future Role of Neoadjuvant Therapy for Breast Cancer. Breast Edinb. Scotl. 2014, 23, 526–537. [Google Scholar] [CrossRef]
- Chen, J.; Colosimo, M.; Lim, E. The Management of HER2-Positive Early Breast Cancer: Current and Future Therapies. Asia Pac. J. Clin. Oncol. 2021, 17, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Mao, C.; Jiang, W.; Huang, J.; Wang, M.; Yan, X.; Yang, Z.; Wang, D.; Zhang, X.; Shen, J. Quantitative Parameters of Diffusion Spectrum Imaging: HER2 Status Prediction in Patients with Breast Cancer. Front. Oncol. 2022, 12, 194. [Google Scholar] [CrossRef]
- Marinovich, M.L.; Houssami, N.; MacAskill, P.; Sardanelli, F.; Irwig, L.; Mamounas, E.P.; Minckwitz, G.V.; Brennan, M.E.; Ciatto, S. Meta-Analysis of Magnetic Resonance Imaging in Detecting Residual Breast Cancer after Neoadjuvant Therapy. J. Natl. Cancer Inst. 2013, 105, 321–333. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Albain, K.S.; André, F.; Bergh, J.; et al. Personalizing the Treatment of Women with Early Breast Cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 142, 1364–1382. [Google Scholar] [CrossRef]
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thurlimann, B.; Senn, H.-J.; Members, P.; Andre, F.; et al. Tailoring Therapies-Improving the Management of Early Breast Cancer: St GallenInternational Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A New Histological Grading System to Assess Response of Breast Cancers to Primary Chemotherapy: Prognostic Significance and Survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef]
- Symmans, W.F.; Peintinger, F.; Hatzis, C.; Rajan, R.; Kuerer, H.; Valero, V.; Assad, L.; Poniecka, A.; Hennessy, B.; Green, M.; et al. Measurement of Residual Breast Cancer Burden to Predict Survival after Neoadjuvant Chemotherapy. J. Clin. Oncol. 2007, 25, 4414–4422. [Google Scholar] [CrossRef]
- Sataloff, D.M.; Mason, B.A.; Prestipino, A.J.; Seinige, U.L.; Lieber, C.P.; Baloch, Z. Pathologic Response to Induction Chemotherapy in Locally Advanced Carcinoma of the Breast: A Determinant of Outcome. J. Am. Coll. Surg. 1995, 180, 297–306. [Google Scholar]
- Katayama, A.; Miligy, I.M.; Shiino, S.; Toss, M.S.; Eldib, K.; Kurozumi, S.; Quinn, C.M.; Badr, N.; Murray, C.; Provenzano, E.; et al. Predictors of Pathological Complete Response to Neoadjuvant Treatment and Changes to Post-Neoadjuvant HER2 Status in HER2-Positive Invasive Breast Cancer. Mod. Pathol. Off. J. U. S. Can. Acad. Pathol. Inc. 2021, 34, 1271–1281. [Google Scholar] [CrossRef]
- Prete, S.D.; Caraglia, M.; Luce, A.; Montella, L.; Galizia, G.; Sperlongano, P.; Cennamo, G.; Lieto, E.; Capasso, E.; Fiorentino, O.; et al. Clinical and Pathological Factors Predictive of Response to Neoadjuvant Chemotherapy in Breast Cancer: A Single Center Experience. Oncol. Lett. 2019, 18, 3873–3879. [Google Scholar] [CrossRef] [PubMed]
- Vega, I.S.; Zenteno, J.S.; Fernandez, F.B.; Cosmelli, F.R.; Chavez, R.L.; Manzur, B.C. Predictors of Pathologic Complete Response to Neoadjuvant Treatment in HER2-Overexpressing Breast Cancer: A Retrospective Analysis Using Real-World Data. Ecancermedicalscience 2022, 16, 1338. [Google Scholar] [CrossRef]
- Woolf, D.K.; Padhani, A.R.; Makris, A. Magnetic Resonance Imaging, Digital Mammography, and Sonography: Tumor Characteristics and Tumor Biology in Primary Setting. J. Natl. Cancer Inst. Monogr. 2015, 2015, 15–20. [Google Scholar] [CrossRef]
- Mazari, F.A.K.; Sharma, N.; Dodwell, D.; Horgan, K. Human Epidermal Growth Factor 2–Positive Breast Cancer with Mammographic Microcalcification: Relationship to Pathologic Complete Response after Neoadjuvant Chemotherapy. Radiology 2018, 288, 366–374. [Google Scholar] [CrossRef]
- Kim, E.Y.; Do, S.I.; Yun, J.S.; Park, Y.L.; Park, C.H.; Moon, J.H.; Youn, I.; Choi, Y.J.; Ham, S.Y.; Kook, S.H. Preoperative Evaluation of Mammographic Microcalcifications after Neoadjuvant Chemotherapy for Breast Cancer. Clin. Radiol. 2020, 75, 641.e19–641.e27. [Google Scholar] [CrossRef]
- Minckwitz, G.V.; Untch, M.; Nüesch, E.; Loibl, S.; Kaufmann, M.; Kümmel, S.; Fasching, P.A.; Eiermann, W.; Blohmer, J.U.; Costa, S.D.; et al. Impact of Treatment Characteristics on Response of Different Breast Cancer Phenotypes: Pooled Analysis of the German Neo-Adjuvant Chemotherapy Trials. Breast Cancer Res. Treat. 2011, 125, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Buzdar, A.U.; Ibrahim, N.K.; Francis, D.; Booser, D.J.; Thomas, E.S.; Theriault, R.L.; Pusztai, L.; Green, M.C.; Arun, B.K.; Giordano, S.H.; et al. Significantly Higher Pathologic Complete Remission Rate after Neoadjuvant Therapy with Trastuzumab, Paclitaxel, and Epirubicin Chemotherapy: Results of a Randomized Trial in Human Epidermal Growth Factor Receptor 2-Positive Operable Breast Cancer. J. Clin. Oncol. 2005, 23, 3676–3685. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological Complete Response and Long-Term Clinical Benefit in Breast Cancer: The CTNeoBC Pooled Analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Schmidt, H.; Zhaveri, S.; Valente, C.; Pisapati, K.; Pickholz, E.; Weltz, S.; Nayak, A.; Oza, T.; Corben, A.; Weltz, C.; et al. Response in Breast vs Axilla after Neoadjuvant Treatment and Implications for Nonoperative Management of Invasive Breast Cancer. Breast J. 2021, 27, 120–125. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.H.; Roman, L.; Tseng, L.M.; Liu, M.C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.A.; et al. Efficacy and Safety of Neoadjuvant Pertuzumab and Trastuzumab in Women with Locally Advanced, Inflammatory, or Early HER2-Positive Breast Cancer (NeoSphere): A Randomised Multicentre, Open-Label, Phase 2 Trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Broglio, K.R.; Quintana, M.; Foster, M.; Olinger, M.; McGlothlin, A.; Berry, S.M.; Boileau, J.F.; Brezden-Masley, C.; Chia, S.; Dent, S.; et al. Association of Pathologic Complete Response to Neoadjuvant Therapy in HER2-Positive Breast Cancer with Long-Term Outcomes Ameta-Analysis. JAMA Oncol. 2016, 2, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Eiermann, W.; Semiglazov, V.; Manikhas, A.; Lluch, A.; Tjulandin, S.; Zambetti, M.; Vazquez, F.; Byakhow, M.; Lichinitser, M.; et al. Neoadjuvant Chemotherapy with Trastuzumab Followed by Adjuvant Trastuzumab versus Neoadjuvant Chemotherapy Alone, in Patients with HER2-Positive Locally Advanced Breast Cancer (the NOAH Trial): A Randomised Controlled Superiority Trial with a Parallel HER. Lancet 2010, 375, 377–384. [Google Scholar] [CrossRef]
- Hellyer, N.J.; Kim, M.S.; Koland, J.G. Heregulin-Dependent Activation of Phosphoinositide 3-Kinase and Akt via the ErbB2/ErbB3 Co-Receptor. J. Biol. Chem. 2001, 276, 42153–42161. [Google Scholar] [CrossRef]
- Loibl, S.; Bruey, J.; Minckwitz, G.V.; Huober, J.B.; Press, M.F.; Darb-Esfahani, S.; Solbach, C.; Denkert, C.; Tesch, H.; Holms, F.; et al. Validation of P95 as a Predictive Marker for Trastuzumab-Based Therapy in Primary HER2-Positive Breast Cancer: A Translational Investigation from the Neoadjuvant GeparQuattro Study. J. Clin. Oncol. 2011, 29, 530. [Google Scholar] [CrossRef]
- Yerushalmi, R.; Woods, R.; Ravdin, P.M.; Hayes, M.M.; Gelmon, K.A. Ki67 in Breast Cancer: Prognostic and Predictive Potential. Lancet Oncol. 2010, 11, 174–183. [Google Scholar] [CrossRef]
- Prat, A.; Guarneri, V.; Pascual, T.; Brasó-Maristany, F.; Sanfeliu, E.; Paré, L.; Schettini, F.; Martínez, D.; Jares, P.; Griguolo, G.; et al. Development and Validation of the New HER2DX Assay for Predicting Pathological Response and Survival Outcome in Early-Stage HER2-Positive Breast Cancer. EBioMedicine 2022, 75, 103801. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.W.; Ellis, I.O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-term Follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Chang, J.; Powles, T.J.; Allred, D.C.; Ashley, S.E.; Clark, G.M.; Makris, A.; Assersohn, L.; Gregory, R.K.; Osborne, C.K.; Dowsett, M. Biologic Markers as Predictors of Clinical Outcome from Systemic Therapy for Primary Operable Breast Cancer. J. Clin. Oncol. 1999, 17, 3058–3063. [Google Scholar] [CrossRef]
- Hwang, H.W.; Jung, H.; Hyeon, J.; Park, Y.H.; Ahn, J.S.; Im, Y.H.; Nam, S.J.; Kim, S.W.; Lee, J.E.; Yu, J.H.; et al. A Nomogram to Predict Pathologic Complete Response (PCR) and the Value of Tumor-Infiltrating Lymphocytes (TILs) for Prediction of Response to Neoadjuvant Chemotherapy (NAC) in Breast Cancer Patients. Breast Cancer Res. Treat. 2019, 173, 255–266. [Google Scholar] [CrossRef]
- Minckwitz, G.V.; Sinn, H.P.; Raab, G.; Loibl, S.; Blohmer, J.U.; Eidtmann, H.; Hilfrich, J.; Merkle, E.; Jackisch, C.; Costa, S.D.; et al. Clinical Response after Two Cycles Compared to HER2, Ki-67, P53, and Bcl-2 in Independently Predicting a Pathological Complete Response after Preoperative Chemotherapy in Patients with Operable Carcinoma of the Breast. Breast Cancer Res. 2008, 10, 1–11. [Google Scholar] [CrossRef]
- Arnould, L.; Arveux, P.; Couturier, J.; Gelly-Marty, M.; Loustalot, C.; Ettore, F.; Sagan, C.; Antoine, M.; Penault-Llorca, F.; Vasseur, B.; et al. Pathologic Complete Response to Trastuzumab-Based Neoadjuvant Therapy Is Related to the Level of HER-2 Amplification. Clin. Cancer Res. 2007, 13, 6404–6409. [Google Scholar] [CrossRef] [PubMed]
- Orrù, S.; Pascariello, E.; Sotgiu, G.; Piras, D.; Saderi, L.; Muroni, M.R.; Carru, C.; Arru, C.; Mocci, C.; Pinna, G.; et al. Prognostic Role of Androgen Receptor Expression in HER2+ Breast Carcinoma Subtypes. Biomedicines 2022, 10, 164. [Google Scholar] [CrossRef]
- Li, Q.; Xiao, Q.; Li, J.; Wang, Z.; Wang, H.; Gu, Y. Value of Machine Learning with Multiphases CE-MRI Radiomics for Early Prediction of Pathological Complete Response to Neoadjuvant Therapy in HER2-Positive Invasive Breast Cancer. Cancer Manag. Res. 2021, 13, 5053–5062. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | M&P 1–4 | M&P 5 (pCR) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Min | Max | Mean | SD | Min | Max | Mean | SD | Min | Max | p | |
| Age at diagnosis (y) | 132 | 52.9 | 13.3 | 24 | 81 | 53.2 | 13.2 | 25 | 79 | 52.6 | 13.5 | 24 | 81 | 0.812 |
| n | Median | IQR | Min | Max | Median | IQR | Min | Max | Median | IQR | Min | Max | p | |
| MRI Main tumoral size (mm) | 132 | 29.5 | 20.0–40.0 | 9 | 100 | 28.0 | 20–40 | 11 | 110 | 30.0 | 20–40 | 11 | 100 | 0.805 |
| MRI Total tumoral size (mm) | 132 | 35.0 | 25.0–60.0 | 9 | 110 | 32.0 | 22–60 | 9 | 100 | 38.0 | 26–56 | 11 | 110 | 0.615 |
| Ki67 (%) | 130 | 37.5 | 25.0–51.3 | 4 | 95 | 30.0 | 24.8–40 | 5 | 90 | 40.0 | 30–60 | 4 | 95 | 0.006 |
| Pathological tumoral size (mm) | 132 | 0.0 | 0.0–8.8 | 0 | 70 | 11.0 | 5–17 | 0.1 | 70 | 0.0 | 0.0–0.0 | 0 | 15 | 0.000 |
| Radiologic Response Rate (%) | 132 | 100.0 | 95.0–100.0 | −10 | 100 | 95.0 | 70–100 | −10 | 100 | 100.0 | 100–100 | 0 | 100 | <0.001 |
| RCB (Pathologic response) | 102 | 0.0 | 0.0–1.5 | 0 | 4.9 | 1.673 | 1.3–3.2 | 0.7 | 4.9 | 0.000 | 0.0–0.0 | 0 | 0 | <0.001 |
| All Patients | M&P 1–4 | M&P 5 (pCR) | |||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p-Value | |
| cT | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| 1b | 1 | 0.8 | 1 | 1.8 | 0 | 0.0 | 0.510 |
| 1c | 35 | 26.5 | 15 | 27.3 | 20 | 26.0 | |
| 2 | 79 | 59.8 | 30 | 54.5 | 49 | 63.6 | |
| 3 | 17 | 12.9 | 9 | 16.4 | 8 | 10.4 | |
| Focality | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| Unifocal | 80 | 60.6 | 36 | 65.5 | 44 | 57.1 | 0.335 |
| Multifocal-multicentric | 52 | 39.4 | 19 | 34.5 | 33 | 42.9 | |
| Clinical node status (cN) | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| N0 | 74 | 56.8 | 30 | 54.5 | 45 | 58.4 | 0.564 |
| N1 | 30 | 22.0 | 14 | 25.5 | 15 | 19.5 | |
| N2 | 26 | 19.7 | 11 | 20.0 | 15 | 19.5 | |
| N3 | 2 | 1.5 | 0 | 0.0 | 2 | ||
| Histology of the tumor | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| Ductal | 123 | 93.2 | 49 | 89.1 | 74 | 96.1 | 0.115 |
| Other | 9 | 6.8 | 6 | 10.9 | 3 | 3.9 | |
| Histological grade | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| G1–G2 | 58 | 38.6 | 29 | 52.7 | 29 | 37.7 | 0.086 |
| G3 | 74 | 56.1 | 26 | 47.3 | 48 | 62.3 | |
| Ki67 value | 130 | 100.0 | 54 | 100.0 | 76 | 100.0 | |
| Low (≤30%) | 54 | 41.6 | 31 | 22.2 | 23 | 30.2 | <0.001 |
| High (>30%) | 76 | 58.5 | 23 | 42.6 | 53 | 69.7 | |
| HER2 positive subtype | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| HR− (non-luminal) | 53 | 40.2 | 9 | 16.4 | 44 | 57.1 | <0.001 |
| HR+ (luminal) | 79 | 59.8 | 46 | 83.6 | 33 | 42.9 | |
| Radiological response after PST | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| Complete | 87 | 65.9 | 19 | 34.5 | 68 | 88.3 | <0.001 |
| Partial-Null | 45 | 34.1 | 36 | 64.5 | 9 | 11.7 | |
| Sentinel Node Biopsy | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| No | 23 | 17.4 | 16 | 29.1 | 7 | 9.1 | 0.003 |
| Yes | 109 | 82.6 | 39 | 70.9 | 70 | 90.9 | |
| positive sentinel node | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| 0 | 95 | 87.2 | 29 | 74.4 | 66 | 94.3 | 0.01 |
| 1 | 13 | 11.9 | 9 | 23.1 | 4 | 5.7 | |
| 2 | 1 | 0.9 | 1 | 2.6 | 0 | 0.0 | |
| >2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Axillary involvement degree | 14 | 100.0 | 10 | 100.0 | 4 | 100.0 | |
| Macrometastases 1 | 7 | 50.0 | 7 | 70.0 | 0 | 0.0 | |
| Macrometastases | 7 | 50.0 | 3 | 30.0 | 4 | 100.0 | |
| TAD | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| No | 120 | 90.9 | 51 | 92.7 | 69 | 90.9 | 0.539 |
| Yes | 12 | 9.1 | 4 | 7.3 | 8 | 9.1 | |
| ALND | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| No | 87 | 65.9 | 28 | 50.9 | 59 | 76.6 | 0.02 |
| Yes | 45 | 34.1 | 27 | 49.1 | 18 | 23.4 | |
| positive lymph nodes | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| 0 | 24 | 53.3 | 9 | 33.3 | 15 | 83.3 | 0.008 |
| 1–3 | 14 | 31.1 | 11 | 40.7 | 3 | 16.7 | |
| 4–9 | 4 | 8.9 | 4 | 14.8 | 0 | 0.0 | |
| >9 | 3 | 6.7 | 3 | 11.1 | 0 | 0.0 | |
| Pathologic response in breast (M&P) | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| G1 | 6 | 4.5 | 55 | 41.7 | |||
| G2 | 0 | 0.0 | |||||
| G3 | 25 | 18.9 | |||||
| G4 | 24 | 18.2 | |||||
| G5 | 77 | 58.3 | 77 | 58.3 | |||
| Pathologic response (RCB) | 132 | 100.0 | 55 | 100.0 | 77 | 100.0 | |
| pCR | 59 | 57.8 | 0 | 0.0 | 59 | 76.6 | |
| I | 13 | 12.7 | 11 | 20.0 | 2 | 2.6 | |
| II | 23 | 22.5 | 21 | 38.2 | 2 | 2.6 | |
| III | 7 | 6.9 | 7 | 12.7 | 0 | 0.0 | |
| Pathologic response in axilla (Sataloff) | 64 | 100.0 | 31 | 100.0 | 33 | 100.0 | |
| N-A | 22 | 37.9 | 2 | 6.5 | 20 | 60.6 | <0.001 |
| N-B | 14 | 20.7 | 6 | 19.4 | 8 | 24.2 | |
| N-C | 22 | 31.0 | 18 | 58.1 | 4 | 12.1 | |
| N-D | 6 | 10.3 | 5 | 16.1 | 1 | 3.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Méndez, J.I.; Horstmann, M.; Méndez, N.; Frías, L.; Moreno, E.; Yébenes, L.; Roca, M.J.; Hernández, A.; Martí, C. Surgical Interest of an Accurate Real-World Prediction of Primary Systemic Therapy Response in HER2 Breast Cancers. Cancers 2023, 15, 2757. https://doi.org/10.3390/cancers15102757
Sánchez-Méndez JI, Horstmann M, Méndez N, Frías L, Moreno E, Yébenes L, Roca MJ, Hernández A, Martí C. Surgical Interest of an Accurate Real-World Prediction of Primary Systemic Therapy Response in HER2 Breast Cancers. Cancers. 2023; 15(10):2757. https://doi.org/10.3390/cancers15102757
Chicago/Turabian StyleSánchez-Méndez, Jose Ignacio, Mónica Horstmann, Nieves Méndez, Laura Frías, Elisa Moreno, Laura Yébenes, Mᵃ José Roca, Alicia Hernández, and Covadonga Martí. 2023. "Surgical Interest of an Accurate Real-World Prediction of Primary Systemic Therapy Response in HER2 Breast Cancers" Cancers 15, no. 10: 2757. https://doi.org/10.3390/cancers15102757
APA StyleSánchez-Méndez, J. I., Horstmann, M., Méndez, N., Frías, L., Moreno, E., Yébenes, L., Roca, M. J., Hernández, A., & Martí, C. (2023). Surgical Interest of an Accurate Real-World Prediction of Primary Systemic Therapy Response in HER2 Breast Cancers. Cancers, 15(10), 2757. https://doi.org/10.3390/cancers15102757