
Prognostic and Therapeutic Role of CD15 and CD15s in Cancer

 , , ,
, , , 

 and
and 
Simple Summary
Abstract
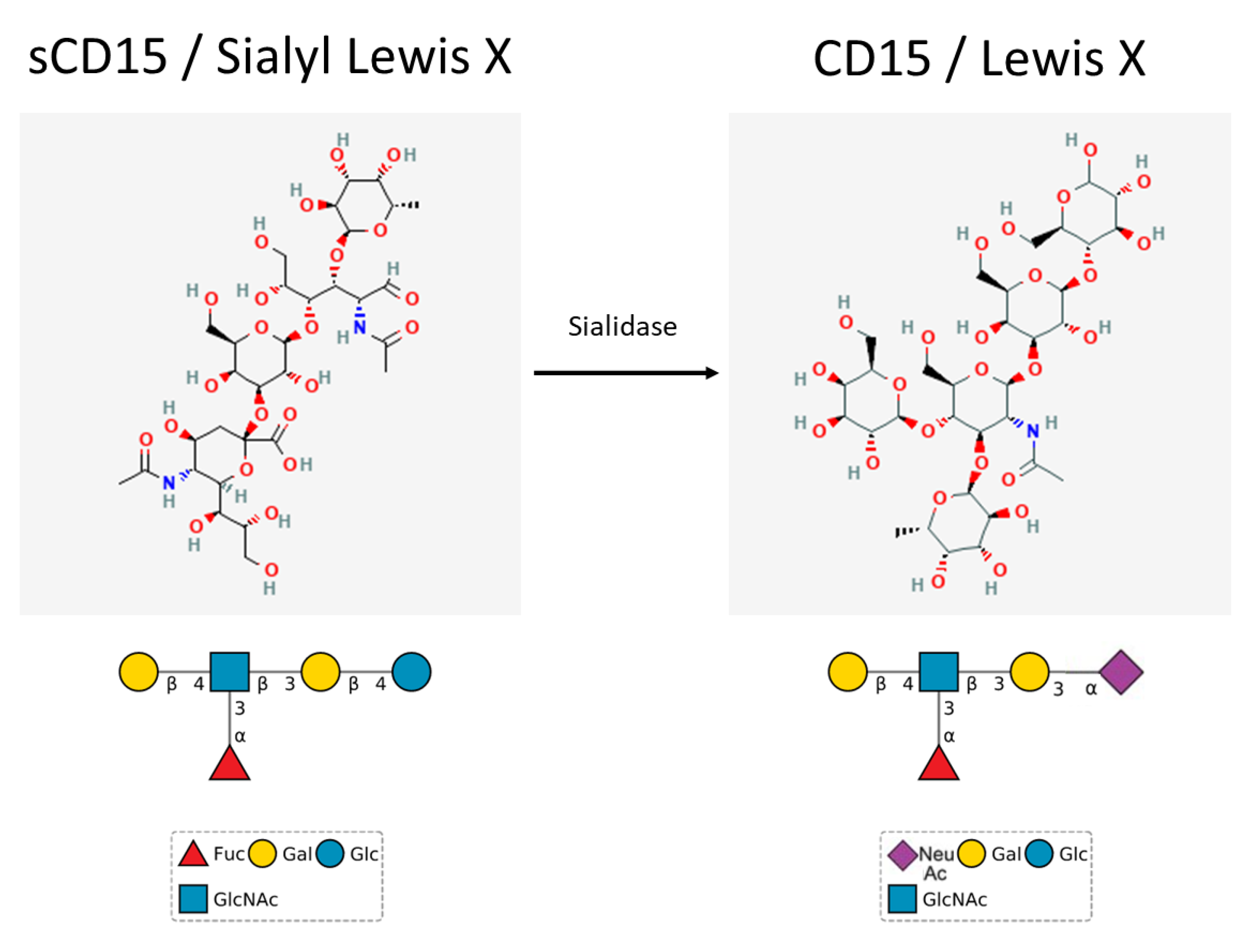
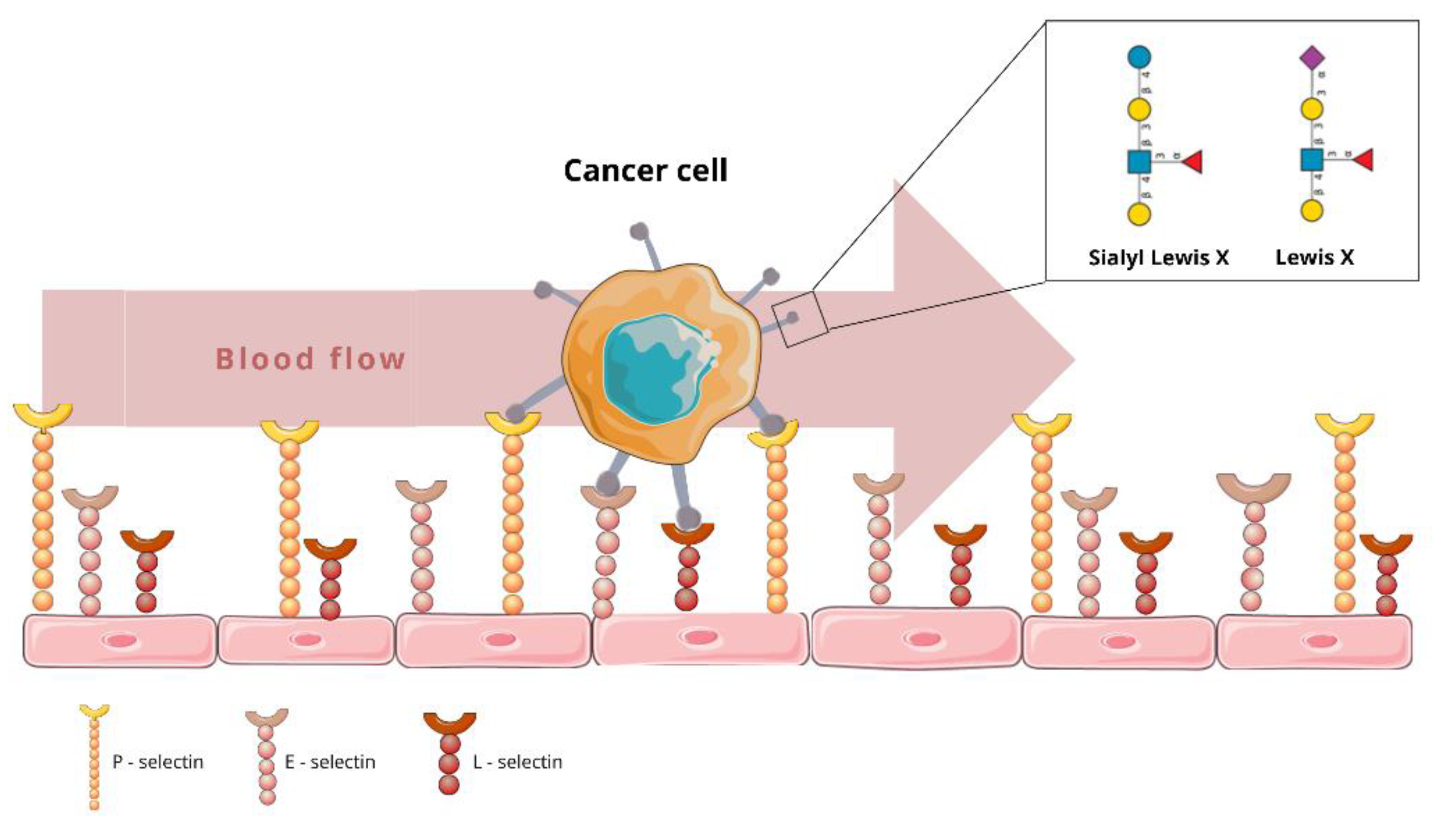
1. CD15 and CD15s: Expression, Structure and Homeostatic Function
2. Role of CD15 and CD15s in Neoplasms
3. Prognostic Significance of CD15 and CD15s Expression in Various Neoplasms
3.1. Gastrointestinal System Cancers
3.2. Lung Cancer
3.3. Breast Cancer
3.4. Haematological Malignancies
3.5. Gliomas
3.6. Urological Malignancies
4. Experimental Drugs Targeting CD15
5. Clinical Trials Concerning CD15 Expression
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nakayama, F.; Nishihara, S.; Iwasaki, H.; Kudo, T.; Okubo, R.; Kaneko, M.; Nakamura, M.; Karube, M.; Sasaki, K.; Narimatsu, H. CD15 Expression in Mature Granulocytes is Determined by α1,3-Fucosyltransferase IX, but in Promyelocytes and Monocytes by α1,3-Fucosyltransferase IV. J. Biol. Chem. 2001, 276, 16100–16106. [Google Scholar] [CrossRef] [PubMed]
- Capela, A.; Temple, S. LeX/ssea-1 is expressed by adult mouse CNS stem cells, identifying them as nonependymal. Neuron 2002, 35, 865–875. [Google Scholar] [CrossRef]
- Chivukula, M.; Dabbs, D.J. Immunocytology. Diagn. Immunohistochem. 2011, 3, 890–918. [Google Scholar] [CrossRef]
- Pilkington, G.; Jassam, S.; Maherally, Z.; Smith, J.; Fillmore, H. BM-26CD15 and E-selectin MEdiation of adhesion of non-small cell lung cancer cells to brain endothelium in lung-brain metastasis. Neuro. Oncol. 2014, 16, v26. [Google Scholar] [CrossRef]
- Silva, M.; Videira, P.A.; Sackstein, R. E-selectin ligands in the human mononuclear phagocyte system: Implications for infection, inflammation, and immunotherapy. Front. Immunol. 2018, 8, 1878. [Google Scholar] [CrossRef]
- Brazil, J.C.; Sumagin, R.; Cummings, R.D.; Louis, N.A.; Parkos, C.A. Targeting of Neutrophil Lewis X Blocks Transepithelial Migration and Increases Phagocytosis and Degranulation. Am. J. Pathol. 2016, 186, 297–311. [Google Scholar] [CrossRef]
- Gadhoum, S.Z.; Sackstein, R. CD15 expression in human myeloid cell differentiation is regulated by sialidase activity. Nat. Chem. Biol. 2008, 4, 751–757. [Google Scholar] [CrossRef]
- Payen, E.; Colomb, C.; Negre, O.; Beuzard, Y.; Hehir, K.; Leboulch, P. Lentivirus Vectors in β-Thalassemia. Methods Enzymol. 2012, 507, 109–124. [Google Scholar] [CrossRef]
- Ashwell, K.W.S.; Mai, J.K. Fetal Development of the Central Nervous System. Hum. Nerv. Syst. 2012, 31–79. [Google Scholar] [CrossRef]
- Miyara, M.; Chader, D.; Sage, E.; Sugiyama, D.; Nishikawa, H.; Bouvry, D.; Claër, L.; Hingorani, R.; Balderas, R.; Rohrer, J.; et al. Sialyl Lewis x (CD15s) identifies highly differentiated and most suppressive FOXP3high regulatory T cells in humans. Proc. Natl. Acad. Sci. USA 2015, 112, 7225–7230. [Google Scholar] [CrossRef]
- Paganuzzi, M.; Bobbio, B.; Marroni, P.; Filiberti, R.; Secco, G.B.; Grossi, C.E. Prognostic role of serum sialyl Lewisx (CD15s) in colorectal cancer. Oncology 2003, 65, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Klassen, H.J. Neural Flow Cytometry—A Historical Account from a Personal Perspective. Neural Surf. Antigens Basic Biol. Towar. Biomed. Appl. 2015, 2015, 167–173. [Google Scholar] [CrossRef]
- Martin, A.W. Immunohistology of Non-Hodgkin Lymphoma. Diagn. Immunohistochem. 2011, 156–188. [Google Scholar] [CrossRef]
- Dabelsteen, E. Cell surface carbohydrates as prognostic markers in human carcinomas. J. Pathol. 1996, 179, 358–369. [Google Scholar] [CrossRef]
- Sell, S. Cancer-associated carbohydrates identified by monoclonal antibodies. Hum. Pathol. 1990, 21, 1003–1019. [Google Scholar] [CrossRef]
- Elola, M.T.; Capurro, M.I.; Barrio, M.M.; Coombs, P.J.; Taylor, M.E.; Drickamer, K.; Mordoh, J. Lewis x Antigen Mediates Adhesion of Human Breast Carcinoma Cells to Activated Endothelium. Possible Involvement of the Endothelial Scavenger Receptor C-type Lectin. Breast Cancer Res. Treat. 2006, 101, 161–174. [Google Scholar] [CrossRef][Green Version]
- Ohana-Malka, O.; Benharroch, D.; Isakov, N.; Prinsloo, I.; Shubinsky, G.; Sacks, M.; Gopas, J. Selectins and anti-CD15 (Lewis x/a) antibodies transmit activation signals in Hodgkin’s lymphoma-derived cell lines. Exp. Hematol. 2003, 31, 1057–1065. [Google Scholar] [CrossRef]
- Fukushima, K. Expression of Lewis(x), sialylated Lewis(x), Lewis(a), and sialylated Lewis(a) antigens in human lung carcinoma. Tohoku J. Exp. Med. 1991, 163, 17–30. [Google Scholar] [CrossRef]
- Shi, Z.R.; McIntyre, L.J.; Knowles, B.B.; Solter, D.; Kim, Y.S. Expression of a Carbohydrate Differentiation Antigen, Stage-specific Embryonic Antigen 1, in Human Colonic Adenocarcinoma. Cancer Res. 1984, 44, 1142–1147. [Google Scholar]
- Laferrière, J.; Houle, F.; Huot, J. Regulation of the Metastatic Process by E-Selectin and Stress-Activated Protein Kinase-2/p38. Ann. N. Y. Acad. Sci. 2002, 973, 562–572. [Google Scholar] [CrossRef]
- Martín-Satué, M.; Marrugat, R.; Cancelas, J.A.; Blanco, J. Enhanced expression of alpha(1,3)-fucosyltransferase genes correlates with E-selectin-mediated adhesion and metastatic potential of human lung adenocarcinoma cells. Cancer Res. 1998, 58, 1544–1550. [Google Scholar] [PubMed]
- Takada, A.; Ohmori, K.; Yoneda, T.; Tsuyuoka, K.; Hasegawa, A.; Kiso, M.; Kannagi, R. Contribution of Carbohydrate Antigens Sialyl Lewis A and Sialyl Lewis X to Adhesion of Human Cancer Cells to Vascular Endothelium. Cancer Res. 1993, 53, 24. [Google Scholar]
- Numahata, K.; Satoh, M.; Handa, K.; Saito, S.; Ohyama, C.; Ito, A.; Takahashi, T.; Hoshi, S.; Orikasa, S.; Hakomori, S.I. Sialosyl-Le(x) expression defines invasive and metastatic properties of bladder carcinoma. Cancer 2002, 94, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, C.; Tsuboi, S.; Fukuda, M. Dual roles of sialyl Lewis X oligosaccharides in tumor metastasis and rejection by natural killer cells. EMBO J. 1999, 18, 1516–1525. [Google Scholar] [CrossRef]
- Irimura, T. Cancer metastasis determined by carbohydrate-mediated cell adhesion. Adv. Exp. Med. Biol. 1994, 353, 27–34. [Google Scholar] [CrossRef]
- Patel, T.P.; Goelz, S.E.; Lobb, R.R.; Parekh, R.B. Isolation and characterization of natural protein-associated carbohydrate ligands for E-selectin. Biochemistry 1994, 33, 14815–14824. [Google Scholar] [CrossRef]
- Mitsuoka, C.; Kawakami-Kimura, N.; Kasugai-Sawada, M.; Hiraiwa, N.; Toda, K.; Ishida, H.; Kiso, M.; Hasegawa, A.; Kannagi, R. Sulfated sialyl Lewis X, the putative L-selectin ligand, detected on endothelial cells of high endothelial venules by a distinct set of anti-sialyl Lewis X antibodies. Biochem. Biophys. Res. Commun. 1997, 230, 546–551. [Google Scholar] [CrossRef]
- Okamoto, T.; Yoneyama, M.S.; Hatakeyama, S.; Mori, K.; Yamamoto, H.; Koie, T.; Saitoh, H.; Yamaya, K.; Funyu, T.; Fukuda, M.; et al. Core2 O-glycan-expressing prostate cancer cells are resistant to NK cell immunity. Mol. Med. Rep. 2013, 7, 359–364. [Google Scholar] [CrossRef]
- Hanski, C.; Hanski, M.L.; Zimmer, T.; Ogorek, D.; Devine, P.; Riecken, E.O. Characterization of the major sialyl-Lex-positive mucins present in colon, colon carcinoma, and sera of patients with colorectal cancer. Cancer Res. 1995, 55, 928–933. [Google Scholar]
- Defendenti, C.; Atzeni, F.; Croce, A.M.; Mussani, E.; Saibeni, S.; Bollani, S.; Grosso, S.; Almasio, P.L.; Bruno, S.; Sarzi-Puttini, P. Morphological distribution of μ chains and cd15 receptors in colorectal polyp and adenocarcinoma specimens. BMC Clin. Pathol. 2013, 13, 8. [Google Scholar] [CrossRef]
- Zhou, J.; Nefedova, Y.; Lei, A.; Gabrilovich, D. Neutrophils and PMN-MDSC: Their biological role and interaction with stromal cells. Semin. Immunol. 2018, 35, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Tesi, R.J. MDSC; the Most Important Cell You Have Never Heard Of. Trends Pharmacol. Sci. 2019, 40, 4–7. [Google Scholar] [CrossRef]
- Seki-Soda, M.; Sano, T.; Ogawa, M.; Yokoo, S.; Oyama, T. CD15 + tumor infiltrating granulocytic cells can predict recurrence and their depletion is accompanied by good responses to S-1 with oral cancer. Head Neck 2021, 43, 2457–2467. [Google Scholar] [CrossRef] [PubMed]
- Pirillo, A.; Norata, G.D.; Catapano, A.L. LOX-1, OxLDL, and Atherosclerosis. Mediat. Inflamm. 2013, 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Wang, T.; Zheng, Q.; Tao, Y.; Dai, L.; Shen, H. Circulating CD15 + LOX-1 + PMN-MDSCs are a potential biomarker for the early diagnosis of non-small-cell lung cancer. Int. J. Clin. Pract. 2021, 75, e14317. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.X.; Liang, Y.; Gao, W. Clinicopathological and prognostic significance of sialyl Lewis X overexpression in patients with cancer: A meta-analysis. Onco. Targets. Ther. 2016, 9, 3113–3125. [Google Scholar] [CrossRef]
- Nakagoe, T.; Fukushima, K.; Sawai, T.; Tsuji, T.; Jibiki, M.-A.; Nanashima, A.; Tanaka, K.; Yamaguchi, H.; Yasutake, T.; Ayabe, H.; et al. Increased expression of sialyl Lewis(x) antigen as a prognostic factor in patients with stage 0, I, and II gastric cancer. Cancer Lett. 2002, 175, 213–221. [Google Scholar] [CrossRef]
- Futamura, N.; Nakamura, S.; Tatematsu, M.; Yamamura, Y.; Kannagi, R.; Hirose, H. Clinicopathologic significance of sialyl Le xexpression in advanced gastric carcinoma. Br. J. Cancer 2000, 83, 1681–1687. [Google Scholar] [CrossRef]
- Torrado, J.; Plummer, M.; Vivas, J.; Garay, J.; Lopez, G.; Peraza, S.; Carillo, E.; Oliver, W.; Muñoz, N. Lewis Antigen Alterations in a Population at High Risk of Stomach Cancer. Cancer Epidemiol. Prev. Biomark. 2000, 9, 9. [Google Scholar]
- Engel, U.; McCombs, R.; Stranahan, P.; Pettijohn, D.; Hage, E. Decrease in Le(x) expression in esophageal adenocarcinomas arising in Barrett’s epithelium. Cancer Epidemiol. Prev. Biomark. 1997, 6, 245–248. [Google Scholar]
- Faried, A.; Kimura, H.; Faried, L.S.; Usman, N.; Miyazaki, T.; Kato, H.; Yazawa, S.; Kuwano, H. Expression of carbohydrate antigens in human esophageal squamous cell carcinoma: Prognostic application and its diagnostic implications. Ann. Surg. Oncol. 2007, 14, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Nakamori, S.; Kameyama, M.; Imaoka, S.; Furukawa, H.; Ishikawa, O.; Sasaki, Y.; Kabuto, T.; Iwanaga, T.; Matsushita, Y.; Irimura, T. Increased Expression of Sialyl Lewisx Antigen Correlates with Poor Survival in Patients with Colorectal Carcinoma: Clinicopathological and Immunohistochemical Study. Cancer Res. 1993, 53, 3632–3637. [Google Scholar] [PubMed]
- Fukushi, Y.; Ohtani, H.; Orikasa, S. Expression of Lacto Series Type 2 Antigens in Human Renal Cell Carcinoma and Its Clinical Significance. JNCI J. Natl. Cancer Inst. 1989, 81, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, P.; Mann, B.; Mansmann, U.; Lövin, N.; Foss, H.-D.; Berger, G.; Scherübl, H.; Riecken, E.-O.; Buhr, H.J.; Hanski, C. Expression of SIALYL-Le(x) antigen defined by MAb AM-3 is an independent prognostic marker in colorectal carcinoma patients. J. Cancer 2000, 88, 281–286. [Google Scholar] [CrossRef]
- Schiffmann, L.; Schwarz, F.; Linnebacher, M.; Prall, F.; Pahnke, J.; Krentz, H.; Vollmar, B.; Klar, E. A novel sialyl LeX expression score as a potential prognostic tool in colorectal cancer. World J. Surg. Oncol. 2012, 10, 1–6. [Google Scholar] [CrossRef]
- Portela, S.V.; Martín, C.V.; Romay, L.M.; Cuevas, E.; Martín, E.G.; Briera, A.F. sLea and sLex expression in colorectal cancer: Implications for tumourigenesis and disease prognosis. Histol. Histopathol. 2011, 26, 1305–1316. [Google Scholar] [CrossRef]
- Jang, T.J.; Park, J.B.; Lee, J.I. The Expression of CD10 and CD15 Is Progressively Increased during Colorectal Cancer Development. Korean J. Pathol. 2013, 47, 340–347. [Google Scholar] [CrossRef]
- Yang, S.-L.; Luo, Y.-Y.; Chen, M.; Zhou, Y.-P.; Lu, F.-R.; Deng, D.-F.; Wu, Y.-R. A systematic review and meta-analysis comparing the prognosis of multicentric occurrence and vs. intrahepatic metastasis in patients with recurrent hepatocellular carcinoma after hepatectomy. HPB 2017, 19, 835–842. [Google Scholar] [CrossRef]
- Torii, A.; Nakayama, A.; Harada, A.; Nakao, A.; Nonami, T.; Sakamoto, J.; Watanabe, T.; Lto, M.; Takagi, H. Expression of the C D I 5 Antigen in Hepatocellular Carcinoma. Cancer 1993, 71, 3864–3867. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Shimada, M.; Takenaka, K.; Kajiyama, K.; Shirabe, K.; Sugimachi, K. The Sialyl Lewis X expression in hepatocarcinogenesis: Potential predictor for the emergence of hepatocellular carcinoma. Hepatogastroenterology 2002, 49, 213–217. [Google Scholar]
- Okada, Y.; Jin-No, K.; Ikeda, H.; Sakai, N.; Sotozono, M.-A.; Yonei, T.; Nakanishi, S.; Moriwaki, S.; Tsuji, T. Changes in the Expression of Sialyl-Lewisx, a Hepatic Necroinflammation-Associated Carbohydrate Neoantigen, in Human Hepatocellular Carcinomas. Cancer 1994, 73, 1811–1816. [Google Scholar] [CrossRef]
- Walter, D.; Herrmann, E.; Winkelmann, R.; Albert, J.G.; Liese, J.; Schnitzbauer, A.; Zeuzem, S.; Hansmann, M.L.; Peveling-Oberhag, J.; Hartmann, S. Role of CD15 expression in dysplastic and neoplastic tissue of the bile duct—A potential novel tool for differential diagnosis of indeterminate biliary stricture. Histopathology 2016, 69, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, H.; Kijima, H.; Dowaki, S.; Ohtani, Y.; Tobita, K.; Yamazaki, H.; Nakamura, M.; Ueyama, Y.; Tanaka, M.; Inokuchi, S.; et al. Clinicopathological significance of sialyl Lex expression in human gallbladder carcinoma. Oncol. Rep. 2004, 11, 1139–1143. [Google Scholar] [CrossRef]
- Comin, C.E.; Novelli, L.; Boddi, V.; Paglierani, M.; Dini, S. Calretinin, thrombomodulin, CEA, and CD15: A useful combination of immunohistochemical markers for differentiating pleural epithelial mesothelioma from peripheral pulmonary adenocarcinoma. Hum. Pathol. 2001, 32, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Mizuguchi, S.; Inoue, K.; Iwata, T.; Nishida, T.; Izumi, N.; Tsukioka, T.; Nishiyama, N.; Uenishi, T.; Suehiro, S. High serum concentrations of Sialyl Lewisx predict multilevel N2 disease in non-small-cell lung cancer. Ann. Surg. Oncol. 2006, 13, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Rahmathulla, G.; Toms, S.A.; Weil, R.J. The molecular biology of brain metastasis. J. Oncol. 2012, 2012, 723541. [Google Scholar] [CrossRef]
- Jassam, S.A.; Maherally, Z.; Ashkan, K.; Pilkington, G.J.; Fillmore, H.L. Fucosyltransferase 4 and 7 mediates adhesion of non-small cell lung cancer cells to brain-derived endothelial cells and results in modification of the blood-brain-barrier: In Vitro investigation of CD15 and CD15s in lung-to-brain metastasis. J. Neurooncol. 2019, 143, 405–415. [Google Scholar] [CrossRef]
- Mordoh, J.; Leis, S.; Bravo, A.I.; Podhajcer, O.L.; Ballare, C.; Capurro, M.; Kairiyama, C.; Bover, L. Description of a new monoclonal antibody, FC-2.15, reactive with human breast cancer and other human neoplasias. Int. J. Biol. Markers 1994, 9, 125–134. [Google Scholar] [CrossRef]
- Croce, M.V. An Introduction to the Relationship Between Lewis x and Malignancy Mainly Related to Breast Cancer and Head Neck Squamous Cell Carcinoma (HNSCC). Cancer Investig. 2021, 40, 173–183. [Google Scholar] [CrossRef]
- Sozzani, P.; Arisio, R.; Porpiglia, M.; Benedetto, C. Is Sialyl Lewis x antigen expression a prognostic factor in patients with breast cancer? Int. J. Surg. Pathol. 2008, 16, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, P.; Kadin, M.E. Immunohistology of Hodgkin Lymphoma. Diagn. Immunohistochem. 2011, 137–155. [Google Scholar] [CrossRef]
- Hsu, S.M.; Ho, Y.S.; Li, P.J.; Monheit, J.; Ree, H.J.; Sheibani, K.; Winberg, C.D. L&H variants of Reed-Sternberg cells express sialylated Leu M1 antigen. Am. J. Pathol. 1986, 122, 199. [Google Scholar] [PubMed]
- Benharroch, D.; Dima, E.; Levy, A.; Ohana-Malka, O.; Ariad, S.; Prinsloo, I.; Mejirovsky, E.; Sacks, M.; Gopas, J. Differential expression of sialyl and non-sialyl-CD15 antigens on Hodgkin-Reed-Sternberg cells: Significance in Hodgkin’s disease. Leuk. Lymphoma 2000, 39, 185–194. [Google Scholar] [CrossRef]
- Von Wasielewski, R.; Mengel, M.; Fischer, R.; Hansmann, M.L.; Hübner, K.; Franklin, J.; Tesch, H.; Paulus, U.; Werner, M.; Diehl, V.; et al. Classical Hodgkin’s disease. Clinical impact of the immunophenotype. Am. J. Pathol. 1997, 151, 1123. [Google Scholar]
- Pileri, S.A.; Ascani, S.; Leoncini, L.; Sabattini, E.; Zinzani, P.L.; Piccaluga, P.P.; Pileri, A.; Giunti, M.; Falini, B.; Bolis, G.B.; et al. Hodgkin’s lymphoma: The pathologist’s viewpoint. J. Clin. Pathol. 2002, 55, 162–176. [Google Scholar] [CrossRef]
- Ansell, S.M. Hodgkin Lymphoma: Diagnosis and Treatment. Mayo Clin. Proc. 2015, 90, 1574–1583. [Google Scholar] [CrossRef]
- Cozzolino, I.; Vitagliano, G.; Caputo, A.; Montella, M.; Franco, R.; Ciancia, G.; Selleri, C.; Zeppa, P. CD15, CD30, and PAX5 evaluation in Hodgkin’s lymphoma on fine-needle aspiration cytology samples. Diagn. Cytopathol. 2020, 48, 211–216. [Google Scholar] [CrossRef]
- Kosari, F.; Ghaffari, F. The Comparison Between Microwave and Autoclave as Antigen Retrieval Methods for Immunohistochemical Detection of CD15 and CD30 in Hodgkin’s Lymphoma. Iran. J. Pathol. 2018, 13, 390. [Google Scholar]
- Ball, E.D.; Selvaggi, K.; Hurd, D.; Herzig, R.; Clark, L.; Malley, V.; Persichetti, J.; de Magelhaus-Silverman, M. Phase I clinical trial of serotherapy in patients with acute myeloid leukemia with an immunoglobulin M monoclonal antibody to CD15. Clin. cancer Res. 1995, 1, 965–972. [Google Scholar]
- Wang, P.; Gong, S.; Liao, B.; Pan, J.; Wang, J.; Zou, D.; Zhao, L.; Xiong, S.; Deng, Y.; Yan, Q.; et al. HIF1α/HIF2α induces glioma cell dedifferentiation into cancer stem cells through Sox2 under hypoxic conditions. J. Cancer 2022, 13, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sheinfeld, J.; Reuter, V.E.; Sarkis, A.S.; Cordon-Cardo, C. Blood group antigens in normal and neoplastic urothelium. J. Cell. Biochem. 1992, 50, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Konety, B.R. Molecular markers in bladder cancer: A critical appraisal. Urol. Oncol. Semin. Orig. Investig. 2006, 24, 326–337. [Google Scholar] [CrossRef]
- Ezeabikwa, B.; Mondal, N.; Antonopoulos, A.; Haslam, S.M.; Matsumoto, Y.; Martin-Caraballo, M.; Lehoux, S.; Mandalasi, M.; Ishaque, A.; Heimburg-Molinaro, J.; et al. Major differences in glycosylation and fucosyltransferase expression in low-grade versus high-grade bladder cancer cell lines. Glycobiology 2021, 31, 1444–1463. [Google Scholar] [CrossRef] [PubMed]
- Sagerman, P.M.; Saigo, P.E.; Sheinfeld, J.; Charitonowics, E.; Cordon-Cardo, C. Enhanced detection of bladder cancer in urine cytology with Lewis X, M344 and 19A211 antigens. Acta Cytol. 1994, 38, 517–523. [Google Scholar] [PubMed]
- Golijanin, D.; Sherman, Y.; Shapiro, A.; Pode, D. Detection of bladder tumors by immunostaining of the Lewis X antigen in cells from voided urine. Urology 1995, 46, 173–177. [Google Scholar] [CrossRef]
- Pode, D.; Golijanin, D.; Sherman, Y.; Lebensart, P.; Shapiro, A. Immunostaining of Lewis X in cells from voided urine, cytopathology and ultrasound for noninvasive detection of bladder tumors. J. Urol. 1998, 159, 389–393. [Google Scholar] [CrossRef]
- Friedrich, M.G.; Hellstern, A.; Hautmann, S.H.; Graefen, M.; Conrad, S.; Huland, E.; Huland, H. Clinical use of urinary markers for the detection and prognosis of bladder carcinoma: A comparison of immunocytology with monoclonal antibodies against Lewis X and 486p3/12 with the BTA STAT and NMP22 tests. J. Urol. 2002, 168, 470–474. [Google Scholar] [CrossRef]
- Van Rhijn, B.W.G.; Van Der Poel, H.G.; Van Der Kwast, T.H. Urine markers for bladder cancer surveillance: A systematic review. Eur. Urol. 2005, 47, 736–748. [Google Scholar] [CrossRef]
- Jørgensen, T.; Berner, A.; Kaalhus, O.; Tveter, K.J.; Danielsen, H.E.; Bryne, M. Up-regulation of the oligosaccharide sialyl LewisX: A new prognostic parameter in metastatic prostate cancer. Cancer Res. 1995, 55, 1817–1819. [Google Scholar]
- Mårtensson, S.; Bigler, S.A.; Brown, M.; Lange, P.H.; Brawer, M.K.; Hakomori, S. itiroh Sialyl-Lewis(x) and related carbohydrate antigens in the prostate. Hum. Pathol. 1995, 26, 735–739. [Google Scholar] [CrossRef]
- Munkley, J. Glycosylation is a global target for androgen control in prostate cancer cells. Endocr. Relat. Cancer 2017, 24, R49–R64. [Google Scholar] [CrossRef] [PubMed]
- Cordon-Cardo, C.; Reuter, V.E.; Finstad, C.L.; Sheinfeld, J.; Lloyd, K.O.; Fair, W.R.; Melamed, M.R. Blood group-related antigens in human kidney: Modulation of Lewis determinants in renal cell carcinoma. Cancer Res. 1989, 49, 212–218. [Google Scholar]
- Røge, R.; Nielsen, S.; Vyberg, M. Carb-3 is the superior anti-CD15 monoclonal antibody for immunohistochemistry. Appl. Immunohistochem. Mol. Morphol. AIMM 2014, 22, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Ordóñez, N.G. The diagnostic utility of immunohistochemistry in distinguishing between mesothelioma and renal cell carcinoma: A comparative study. Hum. Pathol. 2004, 35, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.C.; Chen, P.C.H.; Ho, D.M.T. The diagnostic utility of MOC31, BerEP4, RCC marker and CD10 in the classification of renal cell carcinoma and renal oncocytoma: An immunohistochemical analysis of 328 cases. Histopathology 2004, 45, 452–459. [Google Scholar] [CrossRef] [PubMed]
- López, J.I.; Moreno, V.; García, H.; Antón, I.; Robles, A.; Oñate, J.M.; Baños, Á.; Escandón, J.; Ugalde, A. Renal cell carcinoma in young adults: A study of 130 cases and a review of previous series. Urol. Int. 2010, 84, 292–300. [Google Scholar] [CrossRef]
- Wu, C.-Y.; Huo, J.-P.; Zhang, X.-K.; Zhang, Y.-J.; Hu, W.-M.; Yang, P.; Lu, J.-B.; Zhang, Z.-L.; Cao, Y. Loss of CD15 expression in clear cell renal cell carcinoma is correlated with worse prognosis in Chinese patients. Jpn. J. Clin. Oncol. 2017, 47, 1182–1188. [Google Scholar] [CrossRef]
- Liebert, M.; Jaffe, R.; Taylor, R.J.; Ballou, B.T.; Solter, D.; Hakala, T.R. Detection of SSEA-1 on human renal tumors. Cancer 1987, 59, 1404–1408. [Google Scholar] [CrossRef]
- Koga, H.; Naito, S.; Nakashima, M.; Hasegawa, S.; Watanabe, T.; Kumazawa, J. A flow cytometric analysis of the expression of adhesion molecules on human renal cell carcinoma cells with different metastatic potentials. Eur. Urol. 1997, 31, 86–91. [Google Scholar] [CrossRef]
- Tozawa, K.; Okamoto, T.; Kawai, N.; Hashimoto, Y.; Hayashi, Y.; Kohri, K. Positive correlation between sialyl Lewis X expression and pathologic findings in renal cell carcinoma. Kidney Int. 2005, 67, 1391–1396. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kobayashi, M.; Morita, T. Significant Expression Patterns of Lewis X-related Antigens as a Prognostic Predictor of Low-stage Renal Cell Carcinomas. Anticancer Res. 2010, 30, 593–599. [Google Scholar] [PubMed]
- Kim, H.M.; Koo, J.S. Immunohistochemical Analysis of Cancer Stem Cell Marker Expression in Papillary Thyroid Cancer. Front. Endocrinol. 2019, 10, 523. [Google Scholar] [CrossRef] [PubMed]
- Franzoi, M.A.; Hortobagyi, G.N. Leptomeningeal carcinomatosis in patients with breast cancer. Crit. Rev. Oncol. Hematol. 2019, 135, 85–94. [Google Scholar] [CrossRef]
- Bidard, F.C.; Proudhon, C.; Pierga, J.Y. Circulating tumor cells in breast cancer. Mol. Oncol. 2016, 10, 418. [Google Scholar] [CrossRef]
- Cordone, I.; Masi, S.; Summa, V.; Carosi, M.; Vidiri, A.; Fabi, A.; Pasquale, A.; Conti, L.; Rosito, I.; Carapella, C.M.; et al. Overexpression of syndecan-1, MUC-1, and putative stem cell markers in breast cancer leptomeningeal metastasis: A cerebrospinal fluid flow cytometry study. Breast Cancer Res. 2017, 19, 46. [Google Scholar] [CrossRef]
- Jiang, C.-G.; Li, J.-B.; Liu, F.-R.; Wu, T.; Yu, M.; Xu, H.-M. Andrographolide inhibits the adhesion of gastric cancer cells to endothelial cells by blocking E-selectin expression. Anticancer Res. 2007, 27, 2439–2447. [Google Scholar]
- Lu, Y.; Lian, S.; Ye, Y.; Yu, T.; Liang, H.; Cheng, Y.; Xie, J.; Zhu, Y.; Xie, X.; Yu, S.; et al. S-Nitrosocaptopril prevents cancer metastasis in vivo by creating the hostile bloodstream microenvironment against circulating tumor cells. Pharmacol. Res. 2019, 139, 535–549. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Number | Condition or Disease | Therapy Protocol | Analysed Antigens | Short Description | Recruitment Status | Ref. |
|---|---|---|---|---|---|---|
| 40 | Metastatic renal cell carcinoma, renal cell carcinoma associated with Xp11.2 translocations/TFE3 gene fusions, stage III renal cell cancer AJCC v8, stage IV renal cell cancer AJCC v8, unresectable renal cell carcinoma | CD drug: Axitinib Biological: Nivolumab | CD15, CD45, CD11b, CD33, CD14, HLA-DR, CE4, CD3, CD24, FoxP3, CD8, CD69, CD38, PD1, CD244, TIM3, CD4 | Axitinib/nivolumab combination therapy vs. single-agent nivolumab for the treatment of TFE/translocation renal cell carcinoma (tRCC) across all age groups | Recruiting | NCT03595124 |
| 350 | Non-small cell lung cancer | Drug: Pembrolizumab + chemotherapy | CD15, PD-L1, CD8, FoxP3, PD1, CD163, | Prediction of response to treatment with pembrolizumab + chemotherapy in non-small cell lung cancer | Recruiting | NCT04589013 |
| 18 | Deep vein thrombosis, pulmonary embolism, cancer | Drug: Tinzaparin | CD15, CD24, CA19-9, TF, VEGF, TEPI | Thromboprophylaxis for patients undergoing surgical resection for colon cancer (PERI-OP) | Completed | NCT00967148 |
| 20 | Myelodysplastic syndromes, MDS/MPN crossover syndromes | Drug: 5-azacytidine Drug: Decitabine | CD15, CD11b, CD14 | 5-azacitidine and decitabine epigenetic therapy for myeloid malignancies | Recruiting | NCT04187703 |
| 260 | Acute myeloid leukemia, acute lymphoblastic leukemia, myelodysplastic syndrome | AlloHeme Test (ACROBAT) | CD15+, CD3+, CD33+, CD34+ | Assessment of chimerism and relapse post bone marrow/hematopoietic cell transplant (HCT) using AlloHeme test (ACROBAT) | Not yet recruiting | NCT04635384 |
| 100 | Colorectal carcinoma | Procedure: Fasting | CD15, CD3 CD4, CD8, CD19, CD45RA, CD62L, CD25, CD127, CD14, CD16, CD56, CD11b | Short-term fasting effects on chemotherapy toxicity and efficacy | Enrolling by invitation | NCT04247464 |
| 116 | Acute myeloid leukemia | Drug: Transplants from 8/8-matched unrelated donors Drug: Transplants from family-mismatched/haploidentical donors | CD15, CD33, CD3 | Transplantation from family-mismatched/haploidentical donors with matched unrelated donors in adult patients with acute myeloid leukemia | Unknown | NCT01751997 |
| 47 | Advanced melanoma, recurrent melanoma, stage III cutaneous melanoma AJCC v7, stage IIIA cutaneous melanoma AJCC v7, stage IIIB cutaneous melanoma AJCC v7, stage IIIC cutaneous melanoma AJCC v7, stage IV cutaneous melanoma AJCC v6 and v7, unresectable melanoma | Biological: Pembrolizumab Biological: Talimogene laherparepvec | CD15, PD-L1, PD-1, CD80, CD86, FoxP3, CD68, PG-M1, DAKO, CD14 | Talimogene laherparepvec (T-VEC) (NSC-785349) and MK-3475 (pembrolizumab) (NSC-776864) in patients with advanced melanoma who have progressed on anti-PD1/L1-based therapy | Active, not recruiting | NCT02965716 |
| 200 | Renal cell carcinoma, clear-cell metastatic renal cell carcinoma | Biological: Nivolumab/ipilimumab | CD15, HLA-DR, CD11b, CD14, CD33, FoxP3, CD25, CD45RA, CD127, slan, CD1c, CD11c, CD123, CD141, CD303, ICOS, PD-1, PD-L1, CTLA-4, CD27, CD28, CD45RA, CD45RO, CD57, CD95, CD69, CD25, CD107a, TNF-α, IL-4, IL-17, IL-10, | Tailored immunotherapy approach with nivolumab in subjects with metastatic or advanced renal cell carcinoma (TITAN-RCC) | Active, not recruiting | NCT02917772 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szlasa, W.; Wilk, K.; Knecht-Gurwin, K.; Gurwin, A.; Froń, A.; Sauer, N.; Krajewski, W.; Saczko, J.; Szydełko, T.; Kulbacka, J.; et al. Prognostic and Therapeutic Role of CD15 and CD15s in Cancer. Cancers 2022, 14, 2203. https://doi.org/10.3390/cancers14092203
Szlasa W, Wilk K, Knecht-Gurwin K, Gurwin A, Froń A, Sauer N, Krajewski W, Saczko J, Szydełko T, Kulbacka J, et al. Prognostic and Therapeutic Role of CD15 and CD15s in Cancer. Cancers. 2022; 14(9):2203. https://doi.org/10.3390/cancers14092203
Chicago/Turabian StyleSzlasa, Wojciech, Karol Wilk, Klaudia Knecht-Gurwin, Adam Gurwin, Anita Froń, Natalia Sauer, Wojciech Krajewski, Jolanta Saczko, Tomasz Szydełko, Julita Kulbacka, and et al. 2022. "Prognostic and Therapeutic Role of CD15 and CD15s in Cancer" Cancers 14, no. 9: 2203. https://doi.org/10.3390/cancers14092203
APA StyleSzlasa, W., Wilk, K., Knecht-Gurwin, K., Gurwin, A., Froń, A., Sauer, N., Krajewski, W., Saczko, J., Szydełko, T., Kulbacka, J., & Małkiewicz, B. (2022). Prognostic and Therapeutic Role of CD15 and CD15s in Cancer. Cancers, 14(9), 2203. https://doi.org/10.3390/cancers14092203