
Prospective Real-World Gynaecological Cancer Clinical Registry with Associated Biospecimens: A Collaborative Model to Promote Translational Research between GEICO and the Spanish Biobank Network

 ,
,  , , ,
, , ,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The GEICO VCR Design
2.2. The GEICO VCR Development Strategy
2.3. Clinical Data and Biological Sample Collection Process
2.4. Biobank Network Mode of Operation
2.5. Commitment to Patients
3. Results
3.1. VCR Recruitment and Clinical Data
3.2. Model Operating Policy
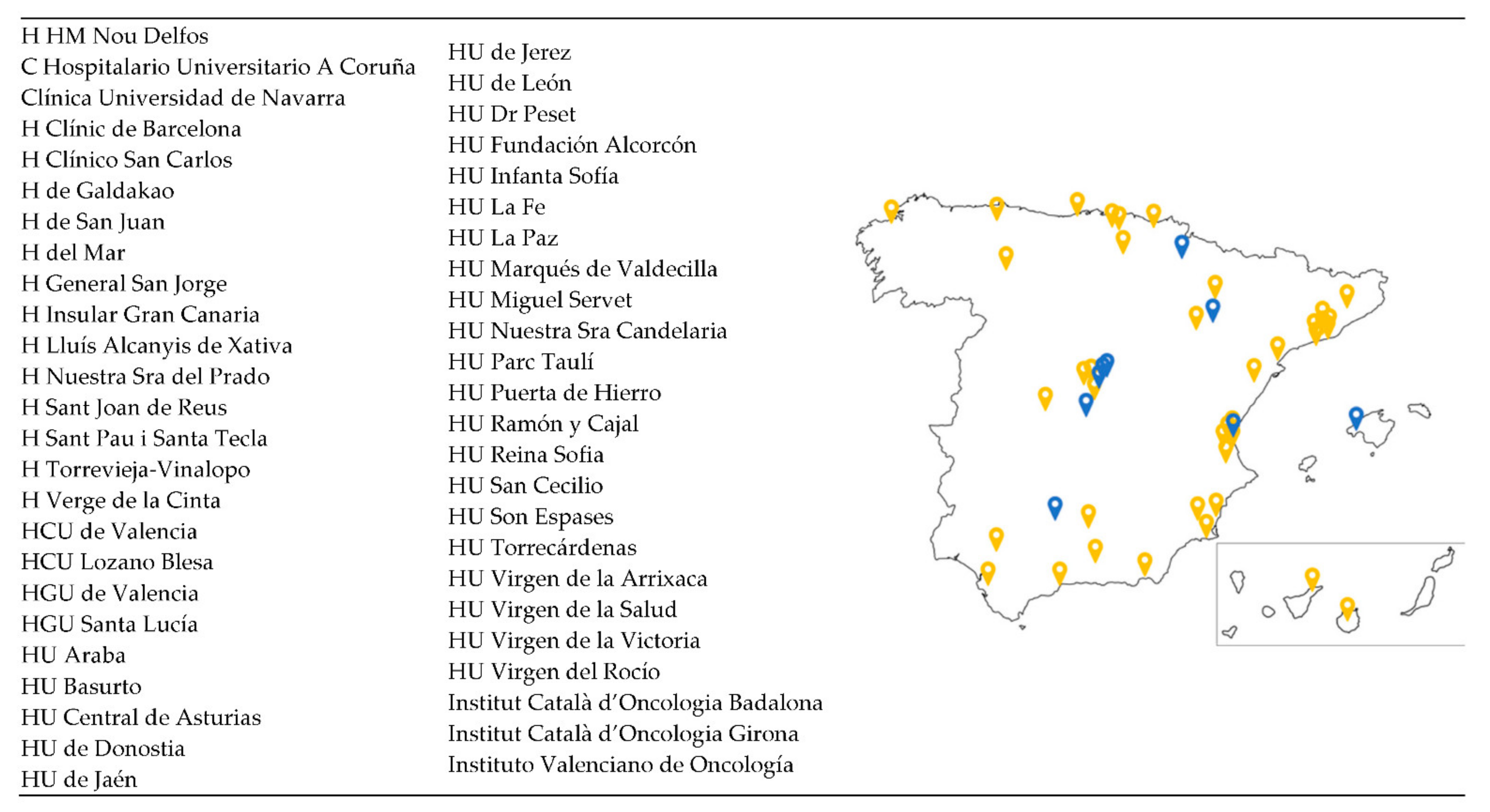
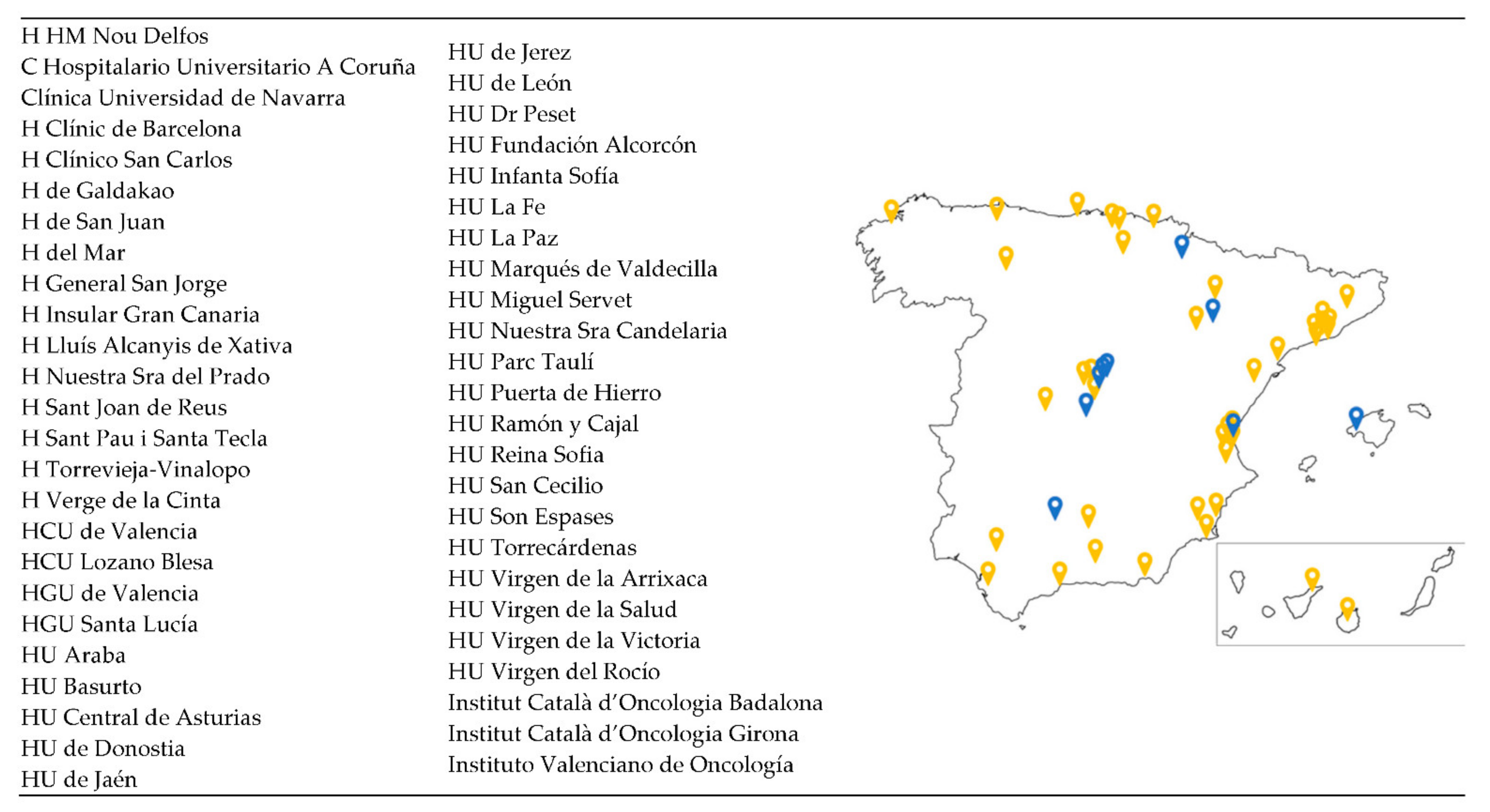
- Participation in the GEICO VCR is voluntary. All GEICO centres and researchers were invited to join the VCR, but only those who expressed their interest in participating were activated. To date, there are 49 centres involved (30 fully activated for recruitment). The target is to activate at least a total of 60 sites;
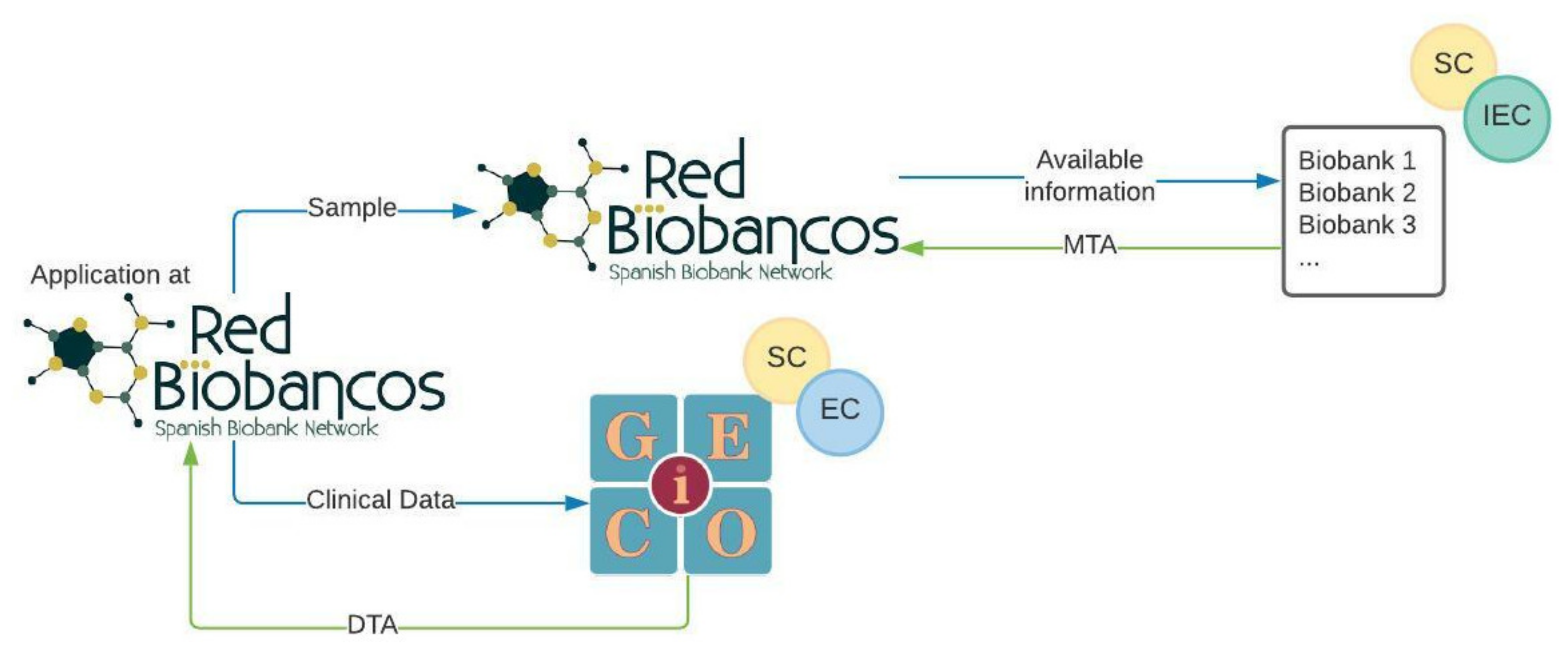
- Both GEICO and RNBB maintain their independence in terms of functioning. This is the reason why patients sign two informed consents: the one to provide clinical data for the VCR and the one to give biospecimens for the biobank. This implies that there might be patients who provide data without samples and vice versa;
- Each centre coordinates the collection of data and biospecimens. Each local GEICO investigator coordinates with the biobank manager the type of biological samples to be collected according to the biobank’s capabilities. At least an FFPE tumour block is recommended;
- Biobanks will charge investigators the cost of handling the samples to cover expenses. This will be done for each application and will affect only those sample types that are selected. The invoice for this service is provided once the samples are delivered to the investigator. Biobanks might apply different fees depending on the type of applicant (public, private, pharma, etc.) and are agreed with the investigator prior to signing the MTA;
- GEICO will not receive any financial income for providing data. The only expected return for GEICO is of scientific and academic nature. GEICO has developed a publication policy to compensate the efforts of investigators in maintaining the VCR updated, which is mainly based on co-authorships for publications originating from the results of the investigations. This aspect is discussed with the investigator and defined in the DTA.
3.3. Patient Participation
4. Discussion
4.1. The Importance of High-Quality Clinical Data and Biospecimens
4.2. The TCGA Experience
4.3. The Advantages of the VCR-Biobank Experience
4.4. Multidisciplinary International Collaboration: The Path towards Effective Personalised Medicine
4.5. Limitations of the Approach
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Husson, O.; de Rooij, B.H.; Kieffer, J.; Oerlemans, S.; Mols, F.; Aaronson, N.K.; van der Graaf, W.T.A.; van de Poll-Franse, L.V. The EORTC QLQ-C30 Summary Score as Prognostic Factor for Survival of Patients with Cancer in the ‘Real-World’: Results from the Population-Based PROFILES Registry. Oncologist 2020, 25, e722–e732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanetti, R.; Sacchetto, L.; Coebergh, J.W.; Rosso, S. To accelerate cancer prevention in Europe: Challenges for cancer registries. Eur. J. Cancer 2018, 104, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Heriot, N.; Brand, A.; Cohen, P.; Hegarty, S.; Hyde, S.; Leung, Y.; Zalcberg, J.R.; Rome, R. Developing an Australian multi-module clinical quality registry for gynaecological cancers: A protocol paper. BMJ Open 2020, 10, e034579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ringborg, U. Translational cancer research—A coherent cancer research continuum. Mol. Oncol. 2019, 13, 517–520. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.N.; Karvonen, C.; Graham, K.; Weinfeld, M.; Joy, A.A.; Koebel, M.; Morris, D.; Robson, P.J.; Johnston, R.N.; Brockton, N.T. Biobanking in the Twenty-First Century: Driving Population Metrics into Biobanking Quality. Adv. Exp. Med. Biol. 2015, 864, 95–114. [Google Scholar] [CrossRef]
- Arias-Diaz, J.; Martín-Arribas, M.C.; del Pozo, J.G.; Alonso, C. Spanish regulatory approach for biobanking. Eur. J. Hum. Genet. 2013, 21, 708–712. [Google Scholar] [CrossRef] [Green Version]
- Caenazzo, L.; Tozzo, P.; Borovecki, A. Ethical governance in biobanks linked to electronic health records. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4182–4188. [Google Scholar]
- Annaratone, L.; De Palma, G.; Bonizzi, G.; Sapino, A.; Botti, G.; Berrino, E.; Mannelli, C.; Arcella, P.; Di Martino, S.; Steffan, A.; et al. Basic principles of biobanking: From biological samples to precision medicine for patients. Virchows Arch. 2021, 479, 233. [Google Scholar] [CrossRef]
- Kinkorová, J.; Topolčan, O. Biobanks in Horizon 2020: Sustainability and attractive perspectives. EPMA J. 2018, 9, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Riegman, P.H.J.; Morente, M.M.; Betsou, F.; de Blasio, P.; Geary, P. Biobanking for better healthcare. Mol. Oncol. 2008, 2, 213–222. [Google Scholar] [CrossRef] [Green Version]
- Meir, K.; Gaffney, E.F.; Simeon-Dubach, D.; Ravid, R.; Watson, P.H.; Schacter, B.; Manuel, M.; Morente and the Marble Arch International Working Group on Biobanking. The human face of biobank networks for translational research. Biopreserv. Biobank. 2011, 9, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Morente, M.M.; Cereceda, L.; Luna-Crespo, F.; Artiga, M.J. Managing a biobank network. Biopreserv. Biobank. 2011, 9, 187–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devereux, L.; Watson, P.H.; Mes-Masson, A.-M.; Crespo, F.D.L.; Thomas, G.; Pitman, H.; Speirs, V.; Hall, A.G.; Bollinger, N.; Posada, M.; et al. A Review of International Biobanks and Networks: Success Factors and Key Benchmarks-A 10-Year Retrospective Review. Biopreserv. Biobank. 2019, 17, 512–519. [Google Scholar] [CrossRef] [PubMed]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef] [PubMed]
- Tewari, K.S.; Sill, M.W.; Long, H.J., III; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; et al. Improved survival with bevacizumab in advanced cervical cancer. N. Engl. J. Med. 2014, 370, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, R.E. Biobanking: The foundation of personalized medicine. Curr. Opin. Oncol. 2011, 23, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.; Tighe, A.; Golder, A.; Littler, S.; Bakker, B.; Moralli, D.; Baker, S.M.; Donaldson, I.J.; Spierings, D.C.J.; Wardenaar, R.; et al. A living biobank of ovarian cancer ex vivo models reveals profound mitotic heterogeneity. Nat. Commun. 2020, 11, 822. [Google Scholar] [CrossRef]
- Le Page, C.; Rahimi, K.; Köbel, M.; Tonin, P.N.; Meunier, L.; Portelance, L.; Bernard, M.; Nelson, B.H.; Bernardini, M.Q.; Bartlett, J.M.S.; et al. Characteristics and outcome of the COEUR Canadian validation cohort for ovarian cancer biomarkers. BMC Cancer 2018, 18, 347. [Google Scholar] [CrossRef]
- De Gregorio, A.; Nagel, G.; Möller, P.; Rempen, A.; Schlicht, E.; Fritz, S.; Flock, F.; Kühn, T.; Thiel, F.; Felberbaum, R.; et al. Feasibility of a large multi-center translational research project for newly diagnosed breast and ovarian cancer patients with affiliated biobank: The BRandO biology and outcome (BiO)-project. Arch. Gynecol. Obstet. 2020, 301, 273–281. [Google Scholar] [CrossRef]
- Adishesh, M.; Hapangama, D.K. Enriching Personalized Endometrial Cancer Research with the Harmonization of Biobanking Standards. Cancers 2019, 11, 1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, I.; Churruca, C.M.; Redondo, A.; Santaballa, A.; Calvo, E.; Ojeda, B.; Del Campo, J.M.; Laínez, N.; García-Martínez, E.; Romeo, M.; et al. Early stage ovarian cancer clinical behavior according to FIGO 2014 Staging changes with a focus on IC subtype: Data from prospective GEICO registry. J. Clin. Oncol. 2015, 33, 5554. [Google Scholar] [CrossRef]
- Leskela, S.; Romero, I.; Cristobal, E.; Pérez-Mies, B.; Rosa-Rosa, J.M.; Gutierrez-Pecharroman, A.; Caniego-Casas, T.; Santón, A.; Ojeda, B.; López-Reig, R.; et al. Mismatch Repair Deficiency in Ovarian Carcinoma: Frequency, Causes, and Consequences. Am. J. Surg. Pathol. 2020, 44, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Simeon-Dubach, D.; Watson, P. Biobanking 3.0: Evidence based and customer focused biobanking. Clin. Biochem. 2014, 47, 300–308. [Google Scholar] [CrossRef]
- Compton, C. Getting to personalized cancer medicine: Taking out the garbage. Cancer 2007, 110, 1641–1643. [Google Scholar] [CrossRef]
- Hutter, C.; Zenklusen, J.C. The Cancer Genome Atlas: Creating Lasting Value beyond Its Data. Cell 2018, 173, 283–285. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef]
- Lehmann, S.; Guadagni, F.; Moore, H.; Ashton, G.; Barnes, M.; Benson, E.; Clements, J.; Koppandi, I.; Coppola, D.; Demiroglu, S.Y.; et al. Standard preanalytical coding for biospecimens: Review and implementation of the Sample PREanalytical Code (SPREC). Biopreserv. Biobank. 2012, 10, 366–374. [Google Scholar] [CrossRef]
- Moore, H.M.; Kelly, A.B.; Jewell, S.D.; McShane, L.M.; Clark, D.P.; Greenspan, R.; Hayes, D.F.; Hainaut, P.; Kim, P.; Mansfield, E.; et al. Biospecimen reporting for improved study quality (BRISQ). J. Proteome Res. 2011, 10, 3429–3438. [Google Scholar] [CrossRef]
- Te Yang, H.; Shah, R.H.; Tegay, D.; Onel, K. Precision oncology: Lessons learned and challenges for the future. Cancer Manag. Res. 2019, 11, 7525–7536. [Google Scholar] [CrossRef] [Green Version]
- Esteva-Socias, M.; Artiga, M.-J.; Bahamonde, O.; Belar, O.; Bermudo, R.; Castro, E.; Escámez, T.; Fraga, M.; Jauregui-Mosquera, L.; Novoa, I.; et al. In search of an evidence-based strategy for quality assessment of human tissue samples: Report of the tissue Biospecimen Research Working Group of the Spanish Biobank Network. J. Transl. Med. 2019, 17, 370. [Google Scholar] [CrossRef] [PubMed]
- Ferdyn, K.; Gleńska-Olender, J.; Witoń, M.; Zagórska, K.; Kozera, Ł.; Chróścicka, A.; Matera-Witkiewicz, A. Quality Management System in the BBMRI.pl Consortium: Status Before the Formation of the Polish Biobanking Network. Biopreserv. Biobank. 2019, 17, 401–409. [Google Scholar] [CrossRef] [Green Version]
- Horizon Europe, Work Programme 2021–2022. 2021. Available online: https://ec.europa.eu/info/funding-tenders/opportunities/docs/2021-2027/horizon/wp-call/2021-2022/wp-1-general-introduction_horizon-2021-2022_en.pdf (accessed on 17 December 2021).
- Kaye, J.; Heeney, C.; Hawkins, N.; de Vries, J.; Boddington, P. Data sharing in genomics—Re-shaping scientific practice. Nat. Rev. Genet. 2009, 10, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Golubnitschaja, O.; Epma; Costigliola, V. General report & recommendations in predictive, preventive and personalised medicine 2012: White paper of the European Association for Predictive, Preventive and Personalised Medicine. EPMA J. 2012, 3, 14–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Data | Site Patient ID Date of birth Date of registration Date of informed consent | Consent to transfer data to third parties Willingness to be informed about findings Participation in Clinical Trials |
| Diagnosis | Date of diagnosis Ovarian cancer (Epithelial malignant, Non-epithelial malignant, Borderline, Non-malignant) - Epithelial malignant (Serous, Endometrioid, Mucinous, Clear cell, Mullerian/carcinosarcoma, Other), - Differentiation grade - Non-epithelial malignant (Granulosa, Yolk sac, Germinal, Brenner, Other) - Borderline (Serous, Endometrioid, Other) - Non-malignant (Cyst, Endometriosis, Other) | Endometrial cancer (Endometrioid serous/carcinosarcoma, Sarcoma, Other) Cervical cancer (Squamous carcinoma, Adenocarcinoma, Sarcoma, Other) Secondary malignancy Germline: BRCA1/2 alterations Somatic: BRCA1/2 and HRD alterations Federation Internationale de Gynecolgie et d’Obstetrique (FIGO) stage according to 2014 classification Biopsy number |
| Primary surgery | Tumour type (Primary, Recurrent) Surgery type (Palliative, Laparoscopy, Laparotomy) | ECOG status CA-125 Residual tumour mass |
| Chemotherapy | Drug name Start and end dates | Maintenance |
| Biobank | Availability of sample in biobank Biobank code | Availability of sample in Pathological Anatomy Service |
| Recurrence | Yes/No | Recurrence dates |
| Follow-up | Date of last follow up | Death (Date, Cause) |
| Biobank/Institution | Region | FFPE Block | Plasma | Serum | Buffy Coat | Ascitic Fluid | Other |
|---|---|---|---|---|---|---|---|
| HCU San Carlos | Comunidad de Madrid | ✓ | ✓ | ✓ | ✓ | ||
| HU Son Espases | Baleares | ✓ | * | ||||
| H U Reina Sofía | Andalucía | ✓ | ✓ | ✓ | ✓ | ** | |
| HU Virgen de la Salud | Castilla la Mancha | ✓ | ✓ | ✓ | * | ||
| HU Miguel Servet | Aragón | ✓ | ✓ | ✓ | ✓ | PBMC in DMSO | |
| CUN | Navarra | ✓ | ✓ | ✓ | ✓ | * | |
| IVO | Comunidad Valenciana | ✓ | ✓ | ✓ | ✓ | *** | * |
| HU Ramón y Cajal | Comunidad de Madrid | ✓ | ✓ | ✓ | ✓ | * | |
| HU Infanta Sofía | Comunidad de Madrid | ✓ | ✓ | ✓ | ✓ | ||
| Hospital del Mar | Cataluña | ✓ | ✓ | ✓ | ✓ | ||
| HU La Fe | Comunidad Valenciana | ✓ | ✓ | ✓ | ✓ | ||
| H CU de Valencia | Comunidad Valenciana | ✓ | ✓ | ✓ | ✓ | * | |
| ICO Girona | Cataluña | ✓ | ✓ | ✓ | ✓ | ||
| HU La Paz | Comunidad de Madrid | ✓ | ✓ | ✓ | ✓ | ||
| HU Marqués de Valdecilla | Cantabria | ✓ | ✓ | ✓ | ✓ | ||
| CHUAC | Galicia | ✓ | ✓ | ✓ | ✓ | ||
| Parc Taulí Hospital Universitari | Cataluña | ✓ | ✓ | ✓ | ✓ | ||
| HU Central de Asturias | Asturias | ✓ | ✓ | ✓ | ✓ | * | |
| ICO Badalona | Cataluña | ✓ | ✓ | ✓ | ✓ | * | |
| HU Jaén | Andalucía | ✓ | |||||
| HU Virgen del Rocío | Andalucía | ✓ | |||||
| HU Virgen de la Victoria | Andalucía | ✓ | |||||
| HU Torrecárdenas | Andalucía | ✓ | ✓ | ✓ | ✓ | *** | |
| HU de Jerez | Andalucía | ✓ | |||||
| HCU San Cecilio | Andalucía | ✓ | |||||
| H Galdakao | País Vasco | ✓ | ✓ | ✓ | ✓ | ||
| HU Basurto | País Vasco | ✓ | ✓ | ✓ | ✓ |
| Age Group (Years) | Diagnosis | ||||
|---|---|---|---|---|---|
| 30–50 | 85 | Borderline | 15 | ||
| 51–70 | 204 | Epithelial malignant | 307 | ||
| 17–90 | 85 | Non-epithelial malignant | 2 | ||
| ECOG status (initial diagnosis) | FIGO stages | ||||
| 0 | 158 | IA IB IC IC1 IC2 IC3 IIA IIB | 36 4 5 19 12 9 11 11 | IIA IIIA1 IIIA2 IIIB IIIC IVA IVB | 11 10 2 14 111 16 62 |
| 1 | 97 | ||||
| 2 | 15 | ||||
| 3 | 1 | ||||
| 4 | 2 | ||||
| NA | 24 | ||||
| HRD alteration | |||||
| Yes | 7 | ||||
| No | 5 | ||||
| Unknown | 82 | ||||
| Clinical Trial Involvements | |||
|---|---|---|---|
| Yes | 44 | No | 323 |
| Primary tumour surgery | Primary tumour surgery (technique) | ||
| Diagnostic (only biopsy) Interval debulking Palliative Primary cytoreduction Secondary cytoreduction NA | 41 55 4 183 1 13 | Laparoscopy | 60 |
| Laparotomy | 198 | ||
| NA | 39 | ||
| Residual tumour mass (primary) [cm] | |||
| >1 | 46 | ||
| 0 | 184 | ||
| 0.1–1 | 20 | ||
| NA | 47 | ||
| Chemotherapy | |||
| Bevacizumab | 41 | Paclitaxel | 222 |
| Carboplatin | 258 | PLD | 13 |
| Cisplatin | 1 | Others | 23 |
| Gemcitabine | 1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Guerrero, J.A.; Mendiola, M.; Pérez-Fidalgo, J.A.; Romero, I.; Torres, A.; Recalde, D.; Molina, E.; Gómez-Raposo, C.; Levin, A.M.; Herrero, A.; et al. Prospective Real-World Gynaecological Cancer Clinical Registry with Associated Biospecimens: A Collaborative Model to Promote Translational Research between GEICO and the Spanish Biobank Network. Cancers 2022, 14, 1965. https://doi.org/10.3390/cancers14081965
López-Guerrero JA, Mendiola M, Pérez-Fidalgo JA, Romero I, Torres A, Recalde D, Molina E, Gómez-Raposo C, Levin AM, Herrero A, et al. Prospective Real-World Gynaecological Cancer Clinical Registry with Associated Biospecimens: A Collaborative Model to Promote Translational Research between GEICO and the Spanish Biobank Network. Cancers. 2022; 14(8):1965. https://doi.org/10.3390/cancers14081965
Chicago/Turabian StyleLópez-Guerrero, José Antonio, Marta Mendiola, José Alejandro Pérez-Fidalgo, Ignacio Romero, Ana Torres, Delia Recalde, Elena Molina, César Gómez-Raposo, Ana M. Levin, Ana Herrero, and et al. 2022. "Prospective Real-World Gynaecological Cancer Clinical Registry with Associated Biospecimens: A Collaborative Model to Promote Translational Research between GEICO and the Spanish Biobank Network" Cancers 14, no. 8: 1965. https://doi.org/10.3390/cancers14081965
APA StyleLópez-Guerrero, J. A., Mendiola, M., Pérez-Fidalgo, J. A., Romero, I., Torres, A., Recalde, D., Molina, E., Gómez-Raposo, C., Levin, A. M., Herrero, A., Alarcón, J., Esteban, C., Marquina, G., Rubio, M. J., Guerra, E., Sánchez-Lorenzo, L., Gálvez-Montosa, F., de Juan, A., Churruca, C., ... González-Martín, A. (2022). Prospective Real-World Gynaecological Cancer Clinical Registry with Associated Biospecimens: A Collaborative Model to Promote Translational Research between GEICO and the Spanish Biobank Network. Cancers, 14(8), 1965. https://doi.org/10.3390/cancers14081965