
Physical Activity Is Associated with Improved Overall Survival among Patients with Metastatic Colorectal Cancer

 , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Assessment of Mortality
2.3. Assessment of Physical Activity
2.4. Assessment of other Study Parameters
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
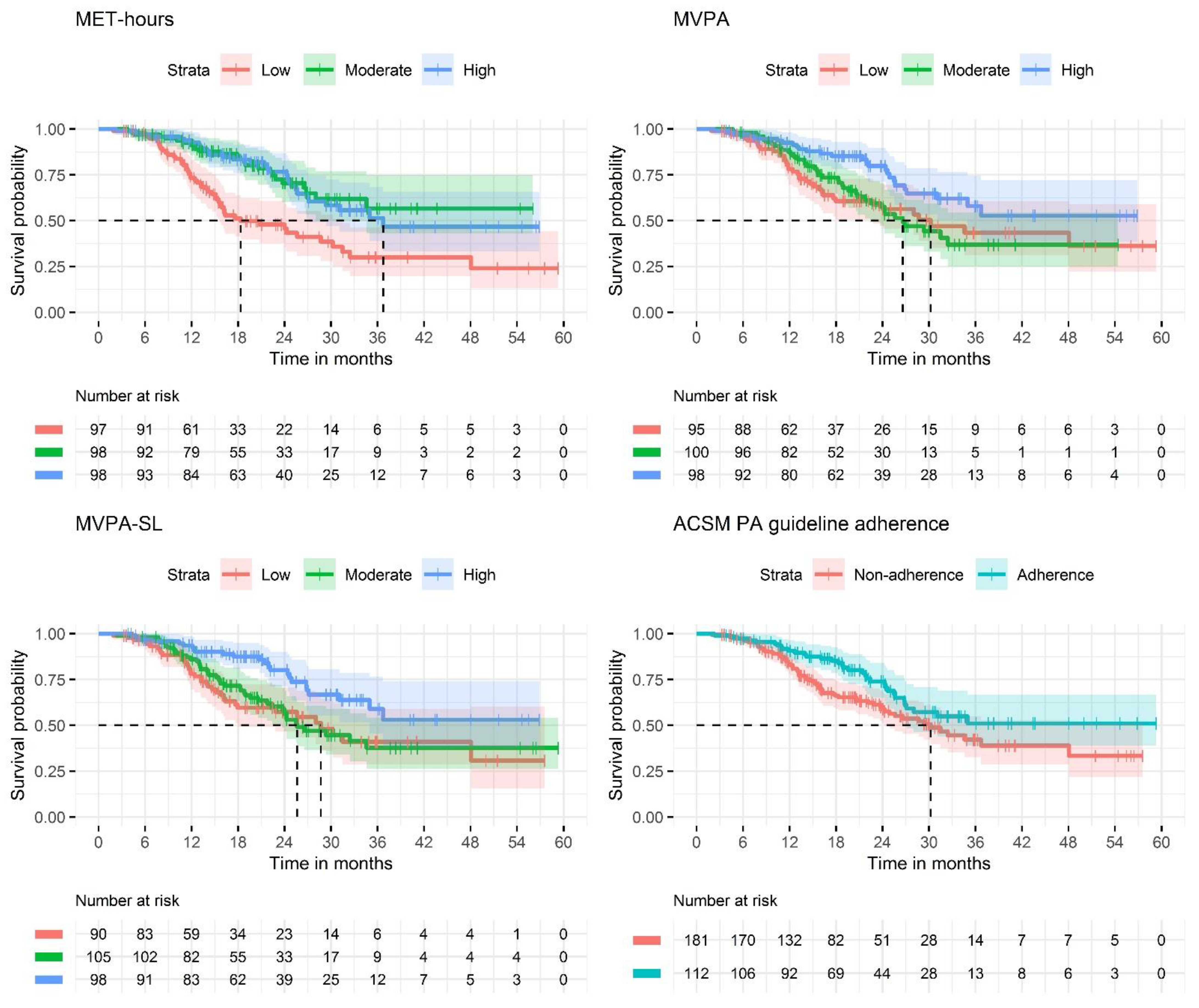
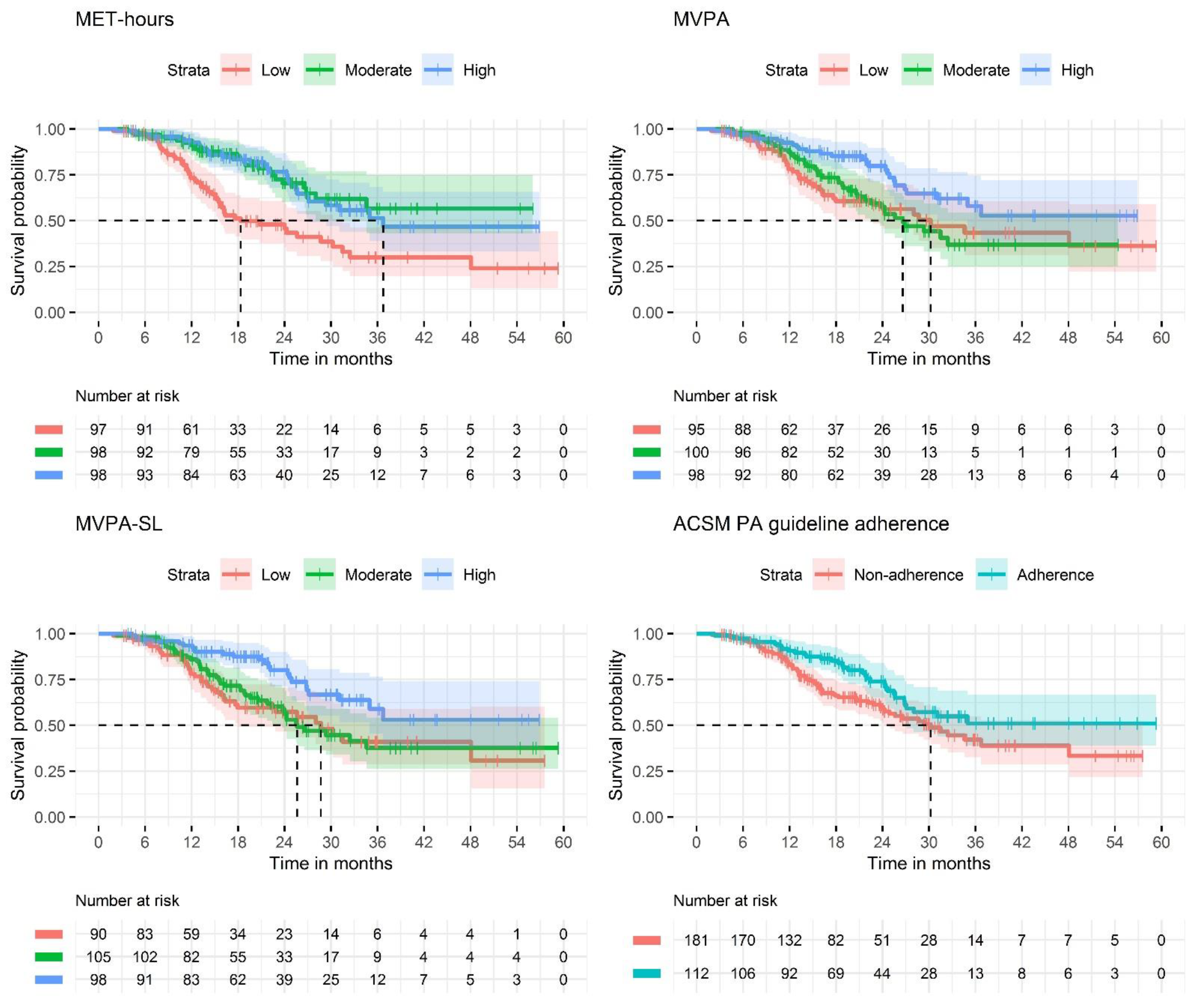
3.2. Associations of Physical Activity with OS
3.2.1. Metabolic Equivalent Task Hours
3.2.2. Moderate and Vigorous Physical Activity
3.2.3. Sport and Leisure Time Moderate and Vigorous Physical Activity
3.2.4. ACSM Physical Activity Guideline Adherence
3.2.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Characteristics | Study Sample (n = 293) | Dutch Population with mCRC between 2013-’17 (n = 15,341) | PLCRC PARTICIPANTS with mCRC between 2013-Aug’19 (n = 918) | Standardized Difference a Study Population vs. Dutch Population | Standardized Difference a Study Population vs. PLCRC Participants |
|---|---|---|---|---|---|
| Age in years, mean (SD) | 62.9 (10.6) | 68.4 (11.8) | 62.2 (11.0) | 0.491 | 0.065 |
| Sex | 0.222 | 0.115 | |||
| Male, n (%) | 197 (67.2) | 8669 (56.5) | 567 (61.2) | ||
| Female, n (%) | 96 (32.8) | 6672 (43.5) | 351 (38.2) | ||
| Primary tumor localization | 0.249 | 0.020 | |||
| Rectum, n (%) | 115 (39.2) | 4234 (27.6) | 354 (38.6) | ||
| Colon, n (%) | 178 (60.8) | 11,107 (72.4) | 564 (61.4) |
| Determinant (Median Hours/Week) | Events/ Total | Univariate Model | Adjusted Model a | Fully Adjusted Model b | |||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| MET | |||||||
| Continuous | 98/285 | 0.993 (0.990–0.997) | <0.001 | 0.994 (0.990–0.997) | <0.001 | 0.994 (0.990–0.997) | <0.001 |
| Low (33.3) | 48/95 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (90.3) | 22/95 | 0.348 (0.210–0.578) | <0.001 | 0.370 (0.218–0.628) | <0.001 | 0.413 (0.245–0.696) | <0.001 |
| High (166) | 28/95 | 0.388 (0.243–0.619) | <0.001 | 0.419 (0.256–0.686) | 0.001 | 0.419 (0.257–0.682) | <0.001 |
| MVPA | |||||||
| Continuous | 98/285 | 0.973 (0.954–0.993) | 0.007 | 0.972 (0.952–0.992) | 0.005 | 0.969 (0.950–0.989) | 0.003 |
| Low (0.6) | 35/92 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (7.5) | 40/98 | 0.988 (0.626–1.560) | 0.960 | 0.894 (0.551–1.449) | 0.649 | 0.867 (0.532–1.412) | 0.566 |
| High (21.5) | 23/95 | 0.476 (0.281–0.806) | 0.006 | 0.434 (0.248–0.759) | 0.003 | 0.416 (0.236–0.733) | 0.002 |
| MVPA-SL | |||||||
| Continuous | 98/285 | 0.963 (0.934–0.992) | 0.014 | 0.951 (0.920–0.983) | 0.003 | 0.952 (0.920–0.985) | 0.005 |
| Low (0.3) | 34/87 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (4.0) | 43/103 | 0.937 (0.597–1.469) | 0.776 | 0.720 (0.441–1.176) | 0.189 | 0.704 (0.433–1.144) | 0.156 |
| High (14.0) | 21/95 | 0.416 (0.241–0.717) | 0.002 | 0.332 (0.187–0.589) | <0.001 | 0.333 (0.185–0.599) | <0.001 |
| ACSM PA Guideline | |||||||
| Non-adherence | 67/176 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Adherence | 31/109 | 0.606 (0.396–0.928) | 0.021 | 0.628 (0.407–0.969) | 0.036 | 0.582 (0.374–0.906) | 0.016 |
References
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Colorectal Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. pp. 1–62. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Colorectal-cancer-report.pdf (accessed on 12 January 2022).
- Perera, P.S.; Thompson, R.L.; Wiseman, M.J. Recent Evidence for Colorectal Cancer Prevention Through Healthy Food, Nutrition, and Physical Activity: Implications for Recommendations. Curr. Nutr. Rep. 2012, 1, 44–54. [Google Scholar] [CrossRef]
- Johnson, C.M.; Wei, C.; Ensor, J.E.; Smolenski, D.J.; Amos, C.I.; Levin, B.; Berry, D.A. Meta-analyses of colorectal cancer risk factors. Cancer Causes Control 2013, 24, 1207–1222. [Google Scholar] [CrossRef]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and Risk of Colorectal Cancer: A Systematic Review of Prospective Studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robsahm, T.E.; Aagnes, B.; Hjartåker, A.; Langseth, H.; Bray, F.I.; Larsen, I.K. Body mass index, physical activity, and colorectal cancer by anatomical subsites: A systematic review and meta-analysis of cohort studies. Eur. J. Cancer Prev. 2013, 22, 492–505. [Google Scholar] [CrossRef] [PubMed]
- Je, Y.; Jeon, J.Y.; Giovannucci, E.L.; Meyerhardt, J.A. Association between physical activity and mortality in colorectal cancer: A meta-analysis of prospective cohort studies. Int. J. Cancer 2013, 133, 1905–1913. [Google Scholar] [CrossRef] [PubMed]
- Guetz, G.D.; Uzzan, B.; Bouillet, T.; Nicolas, P.; Chouahnia, K.; Zelek, L.; Morere, J.-F. Impact of Physical Activity on Cancer-Specific and Overall Survival of Patients with Colorectal Cancer. Gastroenterol. Res. Pract. 2013, 2013, 340851. [Google Scholar]
- Meyerhardt, J.A.; Giovannucci, E.L.; Holmes, M.D.; Chan, A.T.; Chan, J.A.; Colditz, G.; Fuchs, C.S. Physical Activity and Survival After Colorectal Cancer Diagnosis. J. Clin. Oncol. 2006, 24, 3527–3534. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Sato, K.; Niedzwiecki, D.; Ye, X.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Impact of physical activity after cancer diagnosis on survival in patients with recurrent colon cancer: Findings from CALGB 89803/alliance. Clin. Colorectal Cancer 2013, 12, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Lee, Y.; Jang, D.; Shin, A. Physical activity after colorectal cancer diagnosis and mortality in a nationwide retrospective cohort study. Cancers 2021, 13, 4804. [Google Scholar] [CrossRef]
- Schmid, D.; Leitzmann, M.F. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: A systematic review and meta-analysis. Ann. Oncol. 2014, 25, 1293–1311. [Google Scholar] [CrossRef]
- Walter, V.; Jansen, L.; Knebel, P.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H. Physical activity and survival of colorectal cancer patients: Population-based study from Germany. Int. J. Cancer 2017, 140, 1985–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, T.; Fritschi, L.; Platell, C.; Heyworth, J. Lifestyle factors associated with survival after colorectal cancer diagnosis. Br. J. Cancer 2013, 109, 814–822. [Google Scholar] [CrossRef] [Green Version]
- Haydon, A.M.M.; MacInnis, R.J.; English, D.R.; Giles, G.G. Effect of physical activity and body size on survival after diagnosis with colorectal cancer. Gut 2006, 55, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guercio, B.J.; Zhang, S.; Ou, F.; Venook, A.P.; Niedzwiecki, D.; Lenz, H.; Innocenti, F.; O’Neil, B.H.; Shaw, J.E.; Polite, B.N.; et al. Associations of physical activity with survival and progression in metastatic colorectal cancer: Results from Cancer and Leukemia Group B (Alliance)/SWOG 80405. J. Clin. Oncol. 2019, 37, 2620–2631. [Google Scholar] [CrossRef] [PubMed]
- Doyle, C.; Kushi, L.; Byers, T.; Courneya, K.S.; Demark-Wahnefried, W.; Grant, B.; McTiernan, A.; Rock, C.L.; Thompson, C.; Gansler, T.; et al. Nutrition and Physical Activity During and After Cancer Treatment: An American Cancer Society Guide for Informed Choices. CA Cancer J. Clin. 2006, 56, 323–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heywood, R.; McCarthy, A.L.; Skinner, T. Safety and feasibility of exercise interventions in patients with advanced cancer: A systematic review. Support. Care Cancer 2017, 25, 3031–3050. [Google Scholar] [CrossRef] [PubMed]
- Cheville, A.L.; Kollasch, J.; Vandenberg, J.; Shen, T.; Grothey, A.; Gamble, G.; Basford, J.R. A Home-Based Exercise Program to Improve Function, Fatigue, and Sleep Quality in Patients With Stage IV Lung and Colorectal Cancer: A Randomized Controlled Trial. J. Pain Symptom Manag. 2012, 45, 811–821. [Google Scholar] [CrossRef]
- Burbach, J.P.M.; Kurk, S.A.; Braak, R.R.J.C.V.D.; Dik, V.K.; May, A.M.; Meijer, G.A.; Punt, C.J.A.; Vink, G.R.; Los, M.; Hoogerbrugge, N.; et al. Prospective Dutch colorectal cancer cohort: An infrastructure for long-term observational, prognostic, predictive and (randomized) intervention research. Acta Oncol. 2016, 55, 1273–1280. [Google Scholar] [CrossRef] [Green Version]
- Austin, P.C. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Commun. Stat. Simul. Comput. 2009, 38, 1228–1234. [Google Scholar] [CrossRef]
- Wendel-Vos, G.C.W.; Schuit, A.J.; Saris, W.H.M.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weggemans, R.M.; Backx, F.J.G.; Borghouts, L.; Chinapaw, M.; Hopman, M.T.E.; Koster, A.; Kremers, S.; Van Loon, L.J.C.; May, A.; Mosterd, A.; et al. The 2017 Dutch Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. Released. IBM SPSS Statistics for Windows. Version 26.0. IBM Corp.: Armonk, NY, USA, 2019. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-26 (accessed on 12 January 2022).
- R Core Team. R: A Language and Environment for Statistical Computing. 2020. Available online: https://www.r-project.org/ (accessed on 12 January 2022).
- Therneau, T.M. A Package for Survival Analysis in R. 2021. Available online: https://cran.r-project.org/web/packages/survival/vignettes/survival.pdf (accessed on 12 January 2022).
- Kassambara, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using ‘ggplot2’. 2021. Available online: https://cran.r-project.org/web/packages/survminer/survminer.pdf (accessed on 12 January 2022).
- Derksen, J.W.G.; The PLCRC Study Group; Vink, G.R.; Elferink, M.A.G.; Roodhart, J.M.L.; Verkooijen, H.M.; van Grevenstein, W.M.U.; Siersema, P.D.; May, A.M.; Koopman, M. The Prospective Dutch Colorectal Cancer (PLCRC) cohort: Real-world data facilitating research and clinical care. Sci. Rep. 2021, 11, 3923. [Google Scholar] [CrossRef]
- Wolf, A.; MHunter, D.J.; Colditz, G.A.; Manson, J.A.; Stampfer, M.J.; Corsano, K.A.; Rosner, B.; Kriska, A.; Willett, W.C. Reproducibility and Validity of a Self-Administered Physical Activity Questionnaire. Int. J. Epidemiol. 1994, 23, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Cust, A.E.; Smith, B.J.; Chau, J.; van der Ploeg, H.P.; Friedenreich, C.M.; Armstrong, B.K.; Bauman, A. Validity and repeatability of the EPIC physical activity questionnaire: A validation study using accelerometers as an objective measure. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 33. [Google Scholar] [CrossRef] [Green Version]
- Hardikar, S.; Newcomb, P.A.; Campbell, P.T.; Win, A.; Lindor, N.M.; Buchanan, D.; Makar, K.W.; Jenkins, M.; Potter, J.; Phipps, A.I. Prediagnostic physical activity and colorectal cancer survival: Overall and stratified by tumor characteristics. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1130–1137. [Google Scholar] [CrossRef] [Green Version]
- Ratjen, I.; Schafmayer, C.; di Giuseppe, R.; Waniek, S.; Plachta-Danielzik, S.; Koch, M.; Burmeister, G.; Nöthlings, U.; Hampe, J.; Schlesinger, S.; et al. Postdiagnostic physical activity, sleep duration, and TV watching and all-cause mortality among long-term colorectal cancer survivors: A prospective cohort study. BMC Cancer 2017, 17, 701. [Google Scholar]
- Haftenberger, M.; Schuit, A.J.; Tormo, M.J.; Boeing, H.; Wareham, N.; Bueno-de-Mesquita, H.B.; Kumle, M.; Hjartåker, A.; Chirlaque, M.D.; Ardanaz, E.; et al. Physical activity of subjects aged 50–64 years involved in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002, 5, 1163–1177. [Google Scholar] [CrossRef]
- Ballard-Barbash, R.; Friedenreich, C.; Courneya, K.S.; Siddiqi, S.M.; McTiernan, A.; Alfano, C.M. Physical activity, biomarkers, and disease outcomes in cancer survivors: A systematic review. J. Natl. Cancer Inst. 2012, 104, 815–840. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.J.; Batehup, L.; Thomas, R. The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: A review of the literature. Br. J. Cancer 2011, 105, S52–S72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Waart, H.; Stuiver, M.M.; Van Harten, W.H.; Geleijn, E.; Kieffer, J.; Buffart, L.M.; De Maaker-Berkhof, M.; Boven, E.; Schrama, J.; Geenen, M.M. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: Results of the PACES randomized clinical trial. J. Clin. Oncol. 2015, 33, 1918–1927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renfro, L.A.; Loupakis, F.; Adams, R.; Seymour, M.T.; Heinemann, V.; Schmoll, H.-J.; Douillard, J.-Y.; I Hurwitz, H.; Fuchs, C.S.; Diaz-Rubio, E.; et al. Body mass index is prognostic in metastatic colorectal cancer: Pooled analysis of patients from first-line clinical trials in the ARCAD database. J. Clin. Oncol. 2016, 34, 144–150. [Google Scholar] [CrossRef] [PubMed]
| Characteristics | Low PA (n = 97) | Moderate PA (n = 98) | High PA (n = 98) | Total (n = 293) |
|---|---|---|---|---|
| Follow-up time in months, median (IQR) | 14.7 (10.6, 22.9) | 19.9 (13.0, 26.6) | 21.3 (15.8, 30.0) | 18.8 (12.4, 26.6) |
| MET-hours/week, median (p2.5, p97.5) | 33.1 (0, 60.9) | 89.9 (63.8, 119) | 166 (122, 303) | 90.0 (0, 281) |
| MVPA hours/week, median (p2.5, p97.5) | 1.50 (0, 13.7) | 6.8 (0, 25.4) | 19.9 (5.0, 60.6) | 7.5 (0, 47.4) |
| MVPA-SL hours/week, median (p2.5, p97.5) | 0 (0, 12.6) | 4.21 (0, 22.6) | 11.1 (1.0, 43.7) | 4.5 (0, 31.7) |
| Adheres to ACSM PA guideline, n (%) | 4 (4.1%) | 43 (43.9%) | 65 (66.3%) | 112 (38.2%) |
| Sex, n (%) | ||||
| Male | 67 (69.1%) | 64 (65.3%) | 66 (67.3%) | 197 (67.2%) |
| Female | 30 (30.9%) | 34 (34.7%) | 32 (32.7%) | 96 (32.8%) |
| Age in years, mean (SD) | 66.4 (10.4) | 62.1 (10.1) | 60.1 (10.3) | 62.9 (10.6) |
| BMI, mean (SD) | 25.5 (4.6) | 25.2 (3.6) | 25.8 (4.2) | 25.5 (4.2) |
| Missing | 5 (5.2%) | 6 (6.1%) | 6 (6.1%) | 17 (5.8%) |
| Location of primary tumor a | ||||
| Right | 33 (34.0%) | 28 (28.6%) | 22 (22.4%) | 83 (28.3%) |
| Left | 26 (26.8%) | 28 (28.6%) | 36 (36.7%) | 90 (30.7%) |
| Rectum | 36 (37.1%) | 41 (41.8%) | 38 (38.8%) | 115 (39.2%) |
| Other | 2 (2.1%) | 1 (1.0%) | 2 (2.0%) | 5 (1.7%) |
| Metastasis pattern | ||||
| Synchronous | 73 (75.3%) | 74 (75.5%) | 79 (80.6%) | 226 (77.1%) |
| Metachronous | 24 (24.7%) | 24 (24.5%) | 19 (19.4%) | 67 (22.9%) |
| Metastatic sites at diagnosis | ||||
| 1 | 54 (55.7%) | 67 (68.4%) | 58 (59.2%) | 179 (61.1%) |
| >1 | 43 (44.3%) | 31 (31.6%) | 40 (40.8%) | 114 (38.9%) |
| Liver only metastasis at diagnosis | ||||
| No | 65 (67.0%) | 50 (51.0%) | 57 (58.2%) | 172 (58.7%) |
| Yes | 32 (33.0%) | 48 (49.0%) | 41 (41.8%) | 121 (41.3%) |
| Surgery of primary tumor | ||||
| No | 39 (40.2%) | 24 (24.5%) | 32 (32.7%) | 95 (32.4%) |
| Yes, before metastasis | 22 (22.7%) | 21 (21.4%) | 17 (17.3%) | 60 (20.5%) |
| Yes, after metastasis | 36 (37.1%) | 53 (54.1%) | 49 (50.0%) | 138 (47.1%) |
| Metastasectomy, (any) | ||||
| No | 63 (64.9%) | 50 (51.0%) | 45 (45.9%) | 158 (53.9%) |
| Yes | 34 (35.1%) | 48 (49.0%) | 53 (54.1%) | 135 (46.1%) |
| Systemic therapy (after 1st metastasis) | ||||
| None | 27 (27.8%) | 29 (29.6%) | 25 (25.5%) | 81 (27.6%) |
| Fluoropyrimidines b | 68 (70.1%) | 68 (69.4%) | 72 (73.5%) | 209 (71.3%) |
| Oxaliplatin | 53 (54.6%) | 60 (61.2%) | 59 (60.2%) | 172 (58.7%) |
| Irinotecan | 27 (27.8%) | 23 (23.5%) | 21 (21.4%) | 71 (24.2%) |
| Other chemotherapy c | 6 (6.2%) | 4 (4.1%) | 2 (2.0%) | 12 (4.1%) |
| Bevacizumab | 50 (51.5%) | 52 (53.1%) | 52 (53.1%) | 154 (52.6%) |
| EGFR inhibitors d | 4 (4.1%) | 7 (7.1%) | 5 (5.1%) | 16 (5.5%) |
| Other targeted therapy e | 1 (1.0%) | 2 (2.0%) | 1 (1.0%) | 4 (1.4%) |
| Total days on treatment, median (IQR) | 169 (83, 324) | 223 (82, 370) | 215 (118, 471) | 211 (113, 416) |
| Determinant (Median Hours/Week) | Events/ Total | Univariate Model | Adjusted Model a | Fully Adjusted Model b | |||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| MET | |||||||
| Continuous | 106/293 | 0.994 (0.990–0.997) | <0.001 | 0.995 (0.991–0.998) | 0.001 | 0.995 (0.991–0.998) | <0.001 |
| Low (33.1) | 50/97 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (89.9) | 25/98 | 0.388 (0.240–0.628) | <0.001 | 0.448 (0.271–0.741) | 0.002 | 0.491 (0.299–0.807) | 0.005 |
| High (166) | 31/98 | 0.424 (0.271–0.666) | <0.001 | 0.491 (0.306–0.790) | 0.003 | 0.485 (0.303–0.778) | 0.003 |
| MVPA | |||||||
| Continuous | 106/293 | 0.976 (0.958–0.994) | 0.010 | 0.975 (0.957–0.994) | 0.010 | 0.973 (0.955–0.992) | 0.006 |
| Low (0.5) | 38/95 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (21.6) | 42/100 | 0.960 (0.617–1.491) | 0.855 | 0.916 (0.575–1.459) | 0.711 | 0.889 (0.556–1.423) | 0.625 |
| High (31.4) | 26/98 | 0.506 (0.307–0.834) | 0.008 | 0.491 (0.288–0.836) | 0.009 | 0.476 (0.278–0.816) | 0.007 |
| MVPA-SL | |||||||
| Continuous | 106/293 | 0.965 (0.938–0.993) | 0.015 | 0.955 (0.926–0.986) | 0.004 | 0.957 (0.927–0.988) | 0.007 |
| Low (0.0) | 37/90 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Moderate (4.2) | 45/105 | 0.909 (0.588–1.404) | 0.667 | 0.769 (0.480–1.230) | 0.273 | 0.737 (0.462–1.175) | 0.200 |
| High (14.0) | 24/98 | 0.446 (0.267–0.746) | 0.002 | 0.384 (0.223–0.661) | <0.001 | 0.389 (0.224–0.677) | <0.001 |
| ACSM PA Guideline | |||||||
| Non-adherence | 72/181 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Adherence | 34/112 | 0.628 (0.417–0.945) | 0.026 | 0.666 (0.439–1.009) | 0.055 | 0.629 (0.412–0.961) | 0.032 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smit, K.C.; Derksen, J.W.G.; Beets, G.L.O.; Belt, E.J.T.; Berbée, M.; Coene, P.P.L.O.; van Cruijsen, H.; Davidis, M.A.; Dekker, J.W.T.; van Dodewaard-de Jong, J.M.; et al. Physical Activity Is Associated with Improved Overall Survival among Patients with Metastatic Colorectal Cancer. Cancers 2022, 14, 1001. https://doi.org/10.3390/cancers14041001
Smit KC, Derksen JWG, Beets GLO, Belt EJT, Berbée M, Coene PPLO, van Cruijsen H, Davidis MA, Dekker JWT, van Dodewaard-de Jong JM, et al. Physical Activity Is Associated with Improved Overall Survival among Patients with Metastatic Colorectal Cancer. Cancers. 2022; 14(4):1001. https://doi.org/10.3390/cancers14041001
Chicago/Turabian StyleSmit, Karel C., Jeroen W. G. Derksen, Geerard L. O. Beets, Eric J. Th. Belt, Maaike Berbée, Peter Paul L. O. Coene, Hester van Cruijsen, Marjan A. Davidis, Jan Willem T. Dekker, Joyce M. van Dodewaard-de Jong, and et al. 2022. "Physical Activity Is Associated with Improved Overall Survival among Patients with Metastatic Colorectal Cancer" Cancers 14, no. 4: 1001. https://doi.org/10.3390/cancers14041001
APA StyleSmit, K. C., Derksen, J. W. G., Beets, G. L. O., Belt, E. J. T., Berbée, M., Coene, P. P. L. O., van Cruijsen, H., Davidis, M. A., Dekker, J. W. T., van Dodewaard-de Jong, J. M., Haringhuizen, A. W., Helgason, H. H., Hendriks, M. P., Hoekstra, R., de Hingh, I. H. J. T., IJzermans, J. N. M., Janssen, J. J. B., Konsten, J. L. M., Los, M., ... on behalf of the PLCRC Study Group. (2022). Physical Activity Is Associated with Improved Overall Survival among Patients with Metastatic Colorectal Cancer. Cancers, 14(4), 1001. https://doi.org/10.3390/cancers14041001