
Limited Changes in Lifestyle Behaviours after Non-Muscle Invasive Bladder Cancer Diagnosis

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
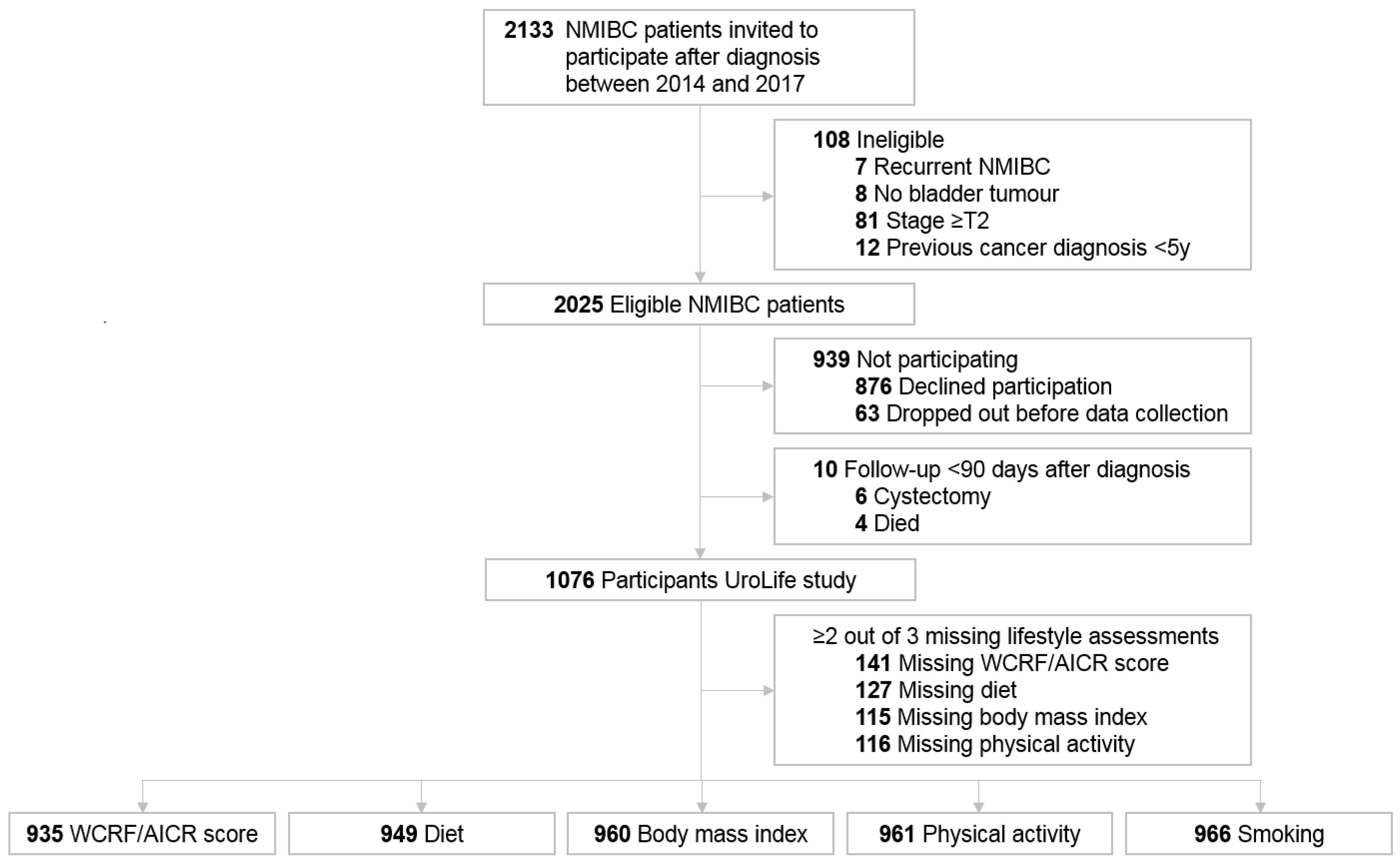
2.1. Study Population
2.2. Data Collection
2.3. WCRF/AICR Recommendations Adherence Score
2.4. Statistical Analyses
3. Results
3.1. Study Population
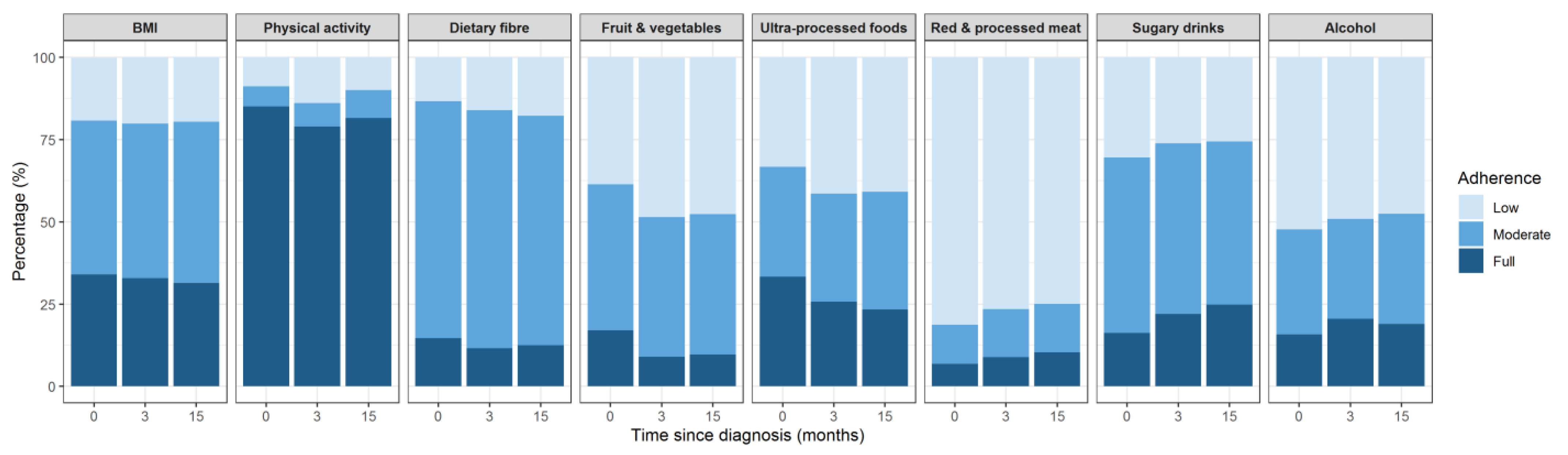
3.2. Adherence to WCRFF/AICR Recommendations
3.3. Lifestyle Changes
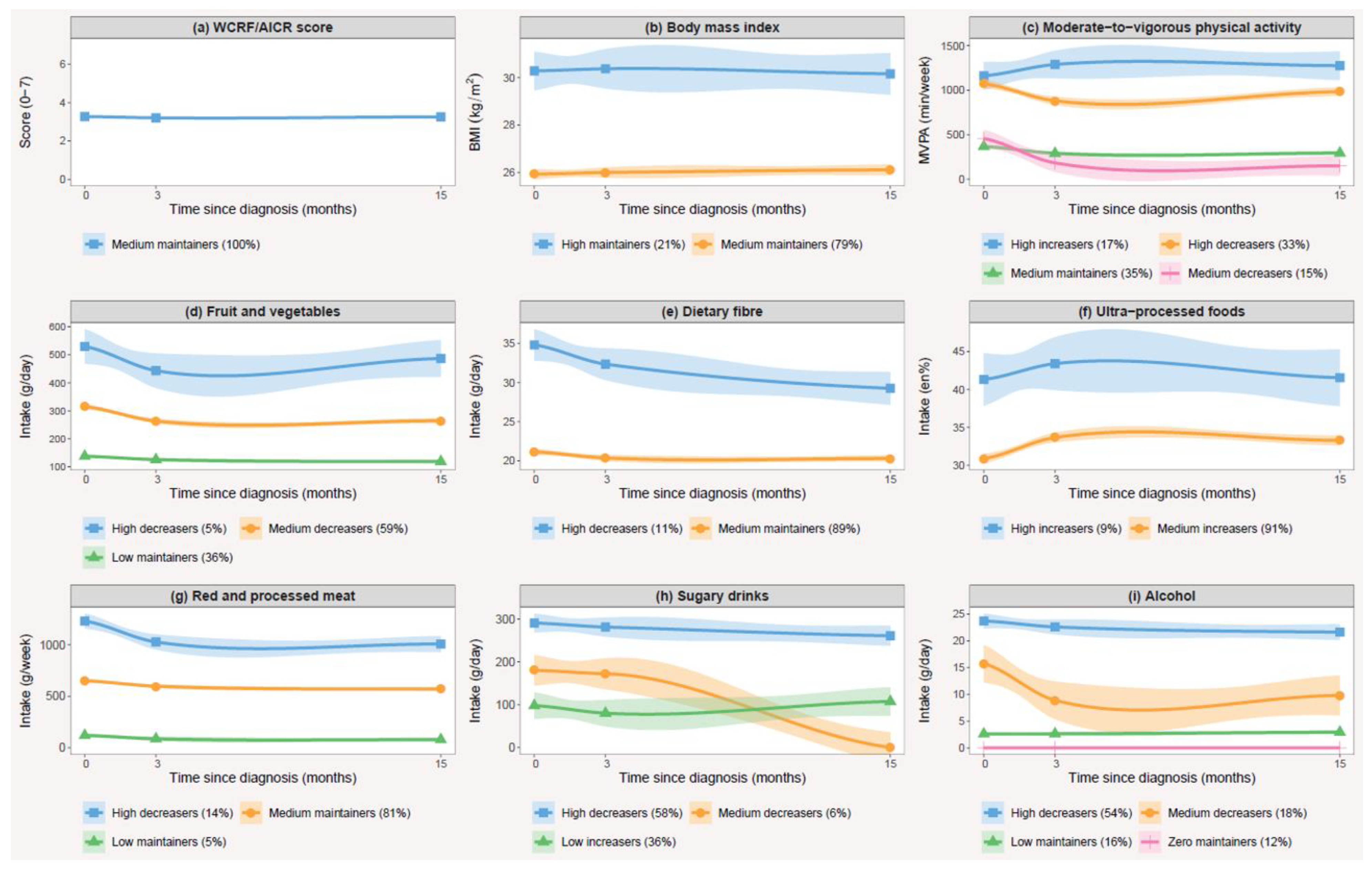
3.4. Trajectories of Change and Their Correlates
3.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.; Luengo-Fernandez, R.; Sullivan, R.; Witjes, J.A. Economic Burden of Bladder Cancer Across the European Union. Eur. Urol. 2016, 69, 438–447. [Google Scholar] [CrossRef] [Green Version]
- Mossanen, M.; Gore, J.L. The burden of bladder cancer care: Direct and indirect costs. Curr. Opin. Urol. 2014, 24, 487–491. [Google Scholar] [CrossRef]
- Williams, S.B.; Howard, L.E.; Foster, M.L.; Klaassen, Z.; Sieluk, J.; De Hoedt, A.M.; Freedland, S.J. Estimated Costs and Long-term Outcomes of Patients With High-Risk Non–Muscle-Invasive Bladder Cancer Treated With Bacillus Calmette-Guérin in the Veterans Affairs Health System. JAMA Netw. Open 2021, 4, e213800. [Google Scholar] [CrossRef]
- Zuniga, K.B.; Graff, R.E.; Feiger, D.B.; Meng, M.V.; Porten, S.P.; Kenfield, S.A. Lifestyle and Non-muscle Invasive Bladder Cancer Recurrence, Progression, and Mortality: Available Research and Future Directions. Bladder Cancer 2020, 6, 9–23. [Google Scholar] [CrossRef] [Green Version]
- Kwan, M.L.; Garren, B.; Nielsen, M.E.; Tang, L. Lifestyle and nutritional modifiable factors in the prevention and treatment of bladder cancer. Urol. Oncol. 2018, 37, 380–386. [Google Scholar] [CrossRef]
- Mehra, K.; Berkowitz, A.; Sanft, T. Diet, Physical Activity, and Body Weight in Cancer Survivorship. Med Clin. 2017, 101, 1151–1165. [Google Scholar] [CrossRef]
- World Cancer Research Fund; American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective; Continuous Update Project Expert Report; World Cancer Research Fund: London, UK, 2018; Available online: https://www.wcrf.org/diet-and-cancer/ (accessed on 3 March 2021).
- Tollosa, D.N.; Tavener, M.; Hure, A.; James, E.L. Adherence to multiple health behaviours in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. Res. Pract. 2019, 13, 327–343. [Google Scholar] [CrossRef]
- Westhoff, E.; Kampman, E.; Aben, K.K.; Hendriks, I.G.; Witjes, J.A.; Kiemeney, L.A.; Vrieling, A. Low awareness, adherence, and practice but positive attitudes regarding lifestyle recommendations among non-muscle-invasive bladder cancer patients. Urol. Oncol. 2019, 37, 573.e1–573.e8. [Google Scholar] [CrossRef]
- Chung, J.; Kulkarni, G.S.; Bender, J.; Breau, R.H.; Guttman, D.; Maganti, M.; Matthew, A.; Morash, R.; Papadakos, J.; Jones, J.M. Modifiable lifestyle behaviours impact the health-related quality of life of bladder cancer survivors. BJU Int. 2020, 125, 836–842. [Google Scholar] [CrossRef]
- Fassier, P.; Zelek, L.; Lecuyer, L.; Bachmann, P.; Touillaud, M.; Druesne-Pecollo, N.; Galan, P.; Cohen, P.; Hoarau, H.; Latino-Martel, P.; et al. Modifications in dietary and alcohol intakes between before and after cancer diagnosis: Results from the prospective population-based NutriNet-Sante cohort. Int. J. Cancer. 2017, 141, 457–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, Y.Y.; Ho, S.C.; Cheng, A.; Kwok, C.; Lee, C.I.; Cheung, K.L.; Lee, R.; Loong, H.H.F.; He, Y.Q.; Yeo, W. Adherence to the World Cancer Research Fund/American Institute for Cancer Research Guideline Is Associated With Better Health-Related Quality of Life Among Chinese Patients With Breast Cancer. J. Natl. Compr. Cancer Netw. 2018, 16, 275–285. [Google Scholar] [CrossRef] [PubMed]
- van Zutphen, M.; Boshuizen, H.C.; Kok, D.E.; van Baar, H.; Geijsen, A.; Wesselink, E.; Winkels, R.M.; van Halteren, H.K.; de Wilt, J.H.W.; Kampman, E.; et al. Colorectal cancer survivors only marginally change their overall lifestyle in the first 2 years following diagnosis. J. Cancer Surviv. Res. Pract. 2019, 13, 956–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velentzis, L.S.; Keshtgar, M.R.; Woodside, J.V.; Leathem, A.J.; Titcomb, A.; Perkins, K.A.; Mazurowska, M.; Anderson, V.; Wardell, K.; Cantwell, M.M. Significant changes in dietary intake and supplement use after breast cancer diagnosis in a UK multicentre study. Breast Cancer Res. Treat. 2011, 128, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.; Steptoe, A.; Wardle, J. Is a cancer diagnosis a trigger for health behaviour change? Findings from a prospective, population-based study. Br. J. Cancer 2013, 108, 2407–2412. [Google Scholar] [CrossRef] [Green Version]
- Karlsen, R.V.; Bidstrup, P.E.; Christensen, J.; Larsen, S.B.; Tjønneland, A.; Dalton, S.O.; Johansen, C. Men with cancer change their health behaviour: A prospective study from the Danish diet, cancer and health study. Br. J. Cancer 2012, 107, 201–206. [Google Scholar] [CrossRef]
- Tollosa, D.N.; Holliday, E.; Hure, A.; Tavener, M.; James, E.L. A 15-year follow-up study on long-term adherence to health behaviour recommendations in women diagnosed with breast cancer. Breast Cancer Res. Treat. 2020, 182, 727–738. [Google Scholar] [CrossRef]
- Shi, Z.; Rundle, A.; Genkinger, J.M.; Cheung, Y.K.; Ergas, I.J.; Roh, J.M.; Kushi, L.H.; Kwan, M.L.; Greenlee, H. Distinct trajectories of fruits and vegetables, dietary fat, and alcohol intake following a breast cancer diagnosis: The Pathways Study. Breast Cancer Res. Treat. 2020, 179, 229–240. [Google Scholar] [CrossRef]
- de Goeij, L.; Westhoff, E.; Witjes, J.A.; Aben, K.K.; Kampman, E.; Kiemeney, L.A.; Vrieling, A. The UroLife study: Protocol for a Dutch prospective cohort on lifestyle habits in relation to non-muscle-invasive bladder cancer prognosis and health-related quality of life. BMJ Open 2019, 9, e030396. [Google Scholar] [CrossRef]
- Siebelink, E.; Geelen, A.; de Vries, J.H. Self-Reported energy intake by FFQ compared with actual energy intake to maintain body weight in 516 adults. Br. J. Nutr. 2011, 106, 274–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, J.H.; de Groot, L.C.; van Staveren, W.A. Dietary assessment in elderly people: Experiences gained from studies in the Netherlands. Eur. J. Clin. Nutr. 2009, 63 (Suppl. 1), S69–S74. [Google Scholar] [CrossRef] [PubMed]
- Streppel, M.T.; de Vries, J.H.; Meijboom, S.; Beekman, M.; de Craen, A.J.; Slagboom, P.E.; Feskens, E.J. Relative validity of the food frequency questionnaire used to assess dietary intake in the Leiden Longevity Study. Nutr. J. 2013, 12, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Public Health and the Environment (RIVM); Netherlands Nutrition Center. Dutch Food Composition (NEVO) Table 2011; Netherlands Nutrition Center: The Hague, The Netherlands, 2011. [Google Scholar]
- de Hollander, E.L.; Zwart, L.; de Vries, S.I.; Wendel-Vos, W. The SQUASH was a more valid tool than the OBiN for categorizing adults according to the Dutch physical activity and the combined guideline. J. Clin. Epidemiol. 2012, 65, 73–81. [Google Scholar] [CrossRef]
- Wagenmakers, R.; van den Akker-Scheek, I.; Groothoff, J.W.; Zijlstra, W.; Bulstra, S.K.; Kootstra, J.W.; Wendel-Vos, G.C.; van Raaij, J.J.; Stevens, M. Reliability and validity of the short questionnaire to assess health-enhancing physical activity (SQUASH) in patients after total hip arthroplasty. BMC Musculoskelet. Disord. 2008, 9, 141. [Google Scholar] [CrossRef] [Green Version]
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and relative validity of the short questionnaire to assess health-enhancing physical activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- Weggemans, R.M.; Backx, F.J.G.; Borghouts, L.; Chinapaw, M.; Hopman, M.T.E.; Koster, A.; Kremers, S.; van Loon, L.J.C.; May, A.; Mosterd, A.; et al. The 2017 Dutch Physical Activity Guidelines. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 58. [Google Scholar] [CrossRef]
- Sangha, O.; Stucki, G.; Liang, M.H.; Fossel, A.H.; Katz, J.N. The Self-Administered Comorbidity Questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003, 49, 156–163. [Google Scholar] [CrossRef]
- Shams-White, M.M.; Brockton, N.T.; Mitrou, P.; Romaguera, D.; Brown, S.; Bender, A.; Kahle, L.L.; Reedy, J. Operationalizing the 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Cancer Prevention Recommendations: A Standardized Scoring System. Nutrients 2019, 11, 1572. [Google Scholar] [CrossRef] [Green Version]
- Shams-White, M.M.; Romaguera, D.; Mitrou, P.; Reedy, J.; Bender, A.; Brockton, N.T. Further Guidance in Implementing the Standardized 2018 World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) Score. Cancer Epidemiol. Biomark. Prev. 2020, 29, 889–894. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The star shines bright. World Nutr. 2016, 7, 28–38. [Google Scholar]
- Lennon, H.; Kelly, S.; Sperrin, M.; Buchan, I.; Cross, A.J.; Leitzmann, M.; Cook, M.B.; Renehan, A.G. Framework to construct and interpret latent class trajectory modelling. BMJ Open 2018, 8, e020683. [Google Scholar] [CrossRef] [PubMed]
- van de Schoot, R.; Sijbrandij, M.; Winter, S.D.; Depaoli, S.; Vermunt, J.K. The GRoLTS-Checklist: Guidelines for Reporting on Latent Trajectory Studies. Struct. Equ. Model. Multidiscip. J. 2017, 24, 451–467. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 22 March 2021).
- Tjon, A.J.S.; Pannekoek, S.; Kampman, E.; Hoedjes, M. Adherence to Diet and Body Weight Recommendations among Cancer Survivors after Completion of Initial Cancer Treatment: A Systematic Review of the Literature. Nutr. Cancer 2019, 71, 367–374. [Google Scholar] [CrossRef]
- Breedveld-Peters, J.J.L.; Koole, J.L.; Müller-Schulte, E.; van der Linden, B.W.A.; Windhausen, C.; Bours, M.J.L.; van Roekel, E.H.; Weijenberg, M.P. Colorectal cancers survivors’ adherence to lifestyle recommendations and cross-sectional associations with health-related quality of life. Br. J. Nutr. 2018, 120, 188–197. [Google Scholar] [CrossRef]
- Ghelfi, F.; Tieri, M.; Gori, S.; Nicolis, F.; Petrella, M.C.; Filiberti, A.; Apolone, G.; Titta, L. Do cancer patients change their diet in the e-health information era? A review of the literature and a survey as a proposal for the Italian population. Food Res. Int. 2018, 104, 59–68. [Google Scholar] [CrossRef]
- Westmaas, J.L.; Newton, C.C.; Stevens, V.L.; Flanders, W.D.; Gapstur, S.M.; Jacobs, E.J. Does a Recent Cancer Diagnosis Predict Smoking Cessation? An Analysis From a Large Prospective US Cohort. J. Clin. Oncol. 2015, 33, 1647–1652. [Google Scholar] [CrossRef]
- van Osch, F.H.M.; Jochems, S.H.J.; Reulen, R.C.; Pirrie, S.J.; Nekeman, D.; Wesselius, A.; James, N.D.; Wallace, D.M.A.; Cheng, K.K.; van Schooten, F.J.; et al. The association between smoking cessation before and after diagnosis and non-muscle-invasive bladder cancer recurrence: A prospective cohort study. Cancer Causes Control 2018, 29, 675–683. [Google Scholar] [CrossRef] [Green Version]
- Winters, B.R.; Wen, L.; Holt, S.K.; Dash, A.; Gore, J.L.; Schade, G.R.; Wright, J.L. Does the Diagnosis of Bladder Cancer Lead to Higher Rates of Smoking Cessation? Findings from the Medicare Health Outcomes Survey. J. Urol. 2019, 202, 241–246. [Google Scholar] [CrossRef]
- Brunet, J.; Amireault, S.; Chaiton, M.; Sabiston, C.M. Identification and prediction of physical activity trajectories in women treated for breast cancer. Ann. Epidemiol. 2014, 24, 837–842. [Google Scholar] [CrossRef]
- Fleming, S.; Jones, T.; Janda, M.; Vagenas, D.; Ward, L.; Reul-Hirche, H.; Sandler, C.; Obermair, A.; Hayes, S. Physical activity trajectories following gynecological cancer: Results from a prospective, longitudinal cohort study. Int. J. Gynecol. Cancer 2020, 30, 1784. [Google Scholar] [CrossRef] [PubMed]
- Lucas, A.R.; Levine, B.J.; Avis, N.E. Posttreatment trajectories of physical activity in breast cancer survivors. Cancer 2017, 123, 2773–2780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Z.; Rundle, A.; Genkinger, J.M.; Cheung, Y.K.; Ergas, I.J.; Roh, J.M.; Kushi, L.H.; Kwan, M.L.; Greenlee, H. Distinct trajectories of moderate to vigorous physical activity and sedentary behavior following a breast cancer diagnosis: The Pathways Study. J. Cancer Surviv. Res. Pract. 2020, 14, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.; Hoekstra, T. Classifying developmental trajectories over time should be done with great caution: A comparison between methods. J. Clin. Epidemiol. 2012, 65, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Herle, M.; Micali, N.; Abdulkadir, M.; Loos, R.; Bryant-Waugh, R.; Hübel, C.; Bulik, C.M.; De Stavola, B.L. Identifying typical trajectories in longitudinal data: Modelling strategies and interpretations. Eur. J. Epidemiol. 2020, 35, 205–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hattori, A.; Sturm, R. The obesity epidemic and changes in self-report biases in BMI. Obesity 2013, 21, 856–860. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Philipps, V.; Liquet, B. Estimation of Extended Mixed Models Using Latent Classes and Latent Processes: The R Package lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef] [Green Version]
- van der Nest, G.; Lima Passos, V.; Candel, M.J.J.M.; van Breukelen, G.J.P. An overview of mixture modelling for latent evolutions in longitudinal data: Modelling approaches, fit statistics and software. Adv. Life Course Res. 2020, 43, 100323. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| 2018 WCRF/AICR Recommendations | Operationalization of Recommendations | Score | Adherence | |
|---|---|---|---|---|
| n | % | |||
| 1. Be a healthy weight | Body mass index (kg/m2) b | |||
| 18.5 to <25 | 1 | 318 | 34 | |
| 25 to <30 | 0.5 | 438 | 47 | |
| <18.5 or ≥30 | 0 | 179 | 19 | |
| 2. Be physically active | Moderate-to-vigorous physical activity c (min/week) | |||
| ≥150 | 1 | 779 | 85 | |
| 75 to 150 | 0.5 | 57 | 6 | |
| <75 | 0 | 81 | 9 | |
| 3. Eat a diet rich in wholegrains, vegetables, fruit, and beans | Fruit and vegetables (g/day) d | |||
| ≥400 | 0.5 | 158 | 17 | |
| 200 to <400 | 0.25 | 413 | 44 | |
| <200 | 0 | 360 | 39 | |
| Total dietary fibre (g/day) | ||||
| ≥30 | 0.5 | 137 | 15 | |
| 15 to <30 | 0.25 | 669 | 72 | |
| <15 | 0 | 125 | 13 | |
| 4. Limit consumption of “fast foods” and other processed foods high in fat, starches or sugars | Percent of total kcal from ultra-processed foods (en%) e | |||
| Tertile 1 < 26.6 | 1 | 310 | 33 | |
| Tertile 2 26.6 to <36.2 | 0.5 | 311 | 33 | |
| Tertile 3 ≥ 36.2 | 0 | 310 | 33 | |
| 5. Limit consumption of red and processed meat | Red (g/week) and processed meat (g/week) f | |||
| Red meat ≤ 500 and processed meat < 21 | 1 | 63 | 7 | |
| Red meat ≤ 500 and processed meat 21 to <100 | 0.5 | 111 | 12 | |
| Red meat > 500 or processed meat ≥ 100 | 0 | 757 | 81 | |
| 6. Limit consumption of sugar sweetened drinks | Sugary drinks (g/day) g | |||
| 0 | 1 | 151 | 16 | |
| >0 to ≤250 | 0.5 | 496 | 53 | |
| >250 | 0 | 284 | 31 | |
| 7. Limit alcohol consumption | Ethanol (g/day) h | |||
| 0 | 1 | 147 | 16 | |
| >0 to ≤10 | 0.5 | 297 | 32 | |
| >10 | 0 | 487 | 52 | |
| Characteristics a | Overall n = 1076 | Included b n = 935 | Excluded b n = 141 |
|---|---|---|---|
| Age at diagnosis, median (IQR), y | 65.9 (61.0–72.0) | 66.2 (61.0–72.0) | 63.9 (58.0–72.0) |
| Male, n (%) | 860 (80) | 747 (80) | 113 (80) |
| Educational level, n (%) c | |||
| Low | 531 (49) | 450 (48) | 81 (57) |
| Medium | 280 (26) | 248 (27) | 32 (23) |
| High | 257 (24) | 236 (25) | 21 (15) |
| Work status, n (%) | |||
| Employed | 326 (30) | 277 (30) | 49 (35) |
| (Early) retirement | 638 (59) | 567 (61) | 71 (50) |
| Unemployed | 19 (2) | 19 (2) | 0 (0) |
| Occupationally disabled | 49 (5) | 42 (5) | 7 (5) |
| Different | 36 (3) | 30 (3) | 6 (4) |
| Living situation, n (%) | |||
| With partner | 763 (71) | 675 (72) | 88 (62) |
| With partner and kids | 139 (13) | 120 (13) | 19 (14) |
| Alone with or without kids | 153 (14) | 128 (14) | 25 (18) |
| Different | 13 (1) | 11 (1) | 2 (1) |
| Body mass index, median (IQR), kg/m2 | 26.3 (24.3–29.0) | 26.3 (24.3–29.0) | 26.0 (24.8–29.1) |
| Body mass index, n (%) | |||
| Underweight | 10 (1) | 8 (1) | 2 (1) |
| Normal weight | 353 (33) | 319 (34) | 34 (24) |
| Overweight | 513 (48) | 437 (47) | 76 (54) |
| Obese | 190 (18) | 171 (18) | 19 (14) |
| Smoking status before diagnosis, n (%) | |||
| Never | 188 (18) | 168 (18) | 20 (14) |
| Former | 625 (58) | 552 (59) | 73 (52) |
| Current | 256 (24) | 215 (23) | 41 (29) |
| WCRF/AICR score, median (IQR), 0–7 | 3.3 (2.8–3.8) | 3.3 (2.8–3.8) | 2.8 (2.5–3.5) |
| Presence of comorbidities, n (%) | |||
| 0 | 164 (15) | 139 (15) | 25 (18) |
| 1 | 269 (25) | 238 (25) | 31 (22) |
| ≥2 | 620 (58) | 553 (59) | 67 (48) |
| Stage, n (%) | |||
| Ta | 812 (76) | 706 (76) | 106 (75) |
| T1 | 236 (22) | 204 (22) | 32 (23) |
| Tis | 28 (3) | 25 (3) | 3 (2) |
| Grade, n (%) | |||
| 1 | 242 (23) | 207 (22) | 35 (25) |
| 2 | 525 (49) | 454 (49) | 71 (50) |
| 3 | 306 (28) | 271 (29) | 35 (25) |
| Lifestyle Behaviour | n | Baseline a | 3 Months after Diagnosis a | 15 Months after Diagnosis a | Change b | Effect Size b,c | p Trend d |
|---|---|---|---|---|---|---|---|
| WCRF/AICR score | 935 | 3.3 (3.2, 3.3) | 3.2 (3.1, 3.3) | 3.3 (3.2, 3.3) | 0.0 (−0.1, 0.0) | −0.04 (−0.15, 0.06) | 0.96 |
| BMI (kg/m2) | 960 | 26.8 (26.6, 27.1) | 26.9 (26.7, 27.2) | 26.9 (26.6, 27.2) | 0.1 (0.0, 0.2) | 0.14 (−0.07, 0.35) | 0.31 |
| Physical activity (min/week) | 961 | 750 (708, 792) | 637 (595, 679) | 665 (620, 709) | −85 (−136, −35) | −0.19 (−0.29, −0.10) | 0.01 |
| Fruit and vegetables (g/day) | 949 | 261 (253, 271) | 223 (214, 231) | 224 (215, 234) | −38 (−48, −27) | −0.46 (−0.57, −0.35) | <0.001 |
| Dietary fibre (g/day) | 949 | 22.6 (22.2, 23.1) | 21.7 (21.2, 22.2) | 21.3 (20.8, 21.7) | −1.4 (−1.9, −0.9) | −0.34 (−0.45, −0.23) | <0.001 |
| Ultra-processed foods (en%) e | 949 | 31.8 (31.2, 32.5) | 34.5 (33.8, 35.2) | 34.0 (33.3, 34.8) | 2.2 (1.4, 2.9) | 0.38 (0.28, 0.50) | <0.001 |
| Red and processed meat (g/week) | 949 | 704 (681, 727) | 634 (611, 656) | 608 (586, 630) | −96 (−121, −71) | −0.49 (−0.60, −0.38) | <0.001 |
| Sugary drinks (g/day) | 949 | 215 (197, 234) | 202 (184, 221) | 187 (169, 205) | −28 (−50, −7) | −0.15 (−0.25, −0.05) | <0.01 |
| Alcohol (g/day) | 949 | 16.1 (14.9, 17.3) | 14.3 (13.1, 15.4) | 13.9 (12.8, 14.9) | −2.3 (−3.2, −1.3) | −0.27 (−0.37, −0.18) | <0.001 |
| Smoking (%) | 966 | 23.2 (20.5, 25.8) | 16.3 (14.0, 18.7) | 15.0 (12.6, 17.5) | −8.1 (−12, −4.5) | −0.44 (−0.65, −0.24) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beeren, I.; Goeij, L.d.; Dandis, R.; Vidra, N.; Zutphen, M.v.; Witjes, J.A.; Kampman, E.; Kiemeney, L.A.L.M.; Vrieling, A. Limited Changes in Lifestyle Behaviours after Non-Muscle Invasive Bladder Cancer Diagnosis. Cancers 2022, 14, 960. https://doi.org/10.3390/cancers14040960
Beeren I, Goeij Ld, Dandis R, Vidra N, Zutphen Mv, Witjes JA, Kampman E, Kiemeney LALM, Vrieling A. Limited Changes in Lifestyle Behaviours after Non-Muscle Invasive Bladder Cancer Diagnosis. Cancers. 2022; 14(4):960. https://doi.org/10.3390/cancers14040960
Chicago/Turabian StyleBeeren, Ivy, Liesbeth de Goeij, Rana Dandis, Nikoletta Vidra, Moniek van Zutphen, J. Alfred Witjes, Ellen Kampman, Lambertus A. L. M. Kiemeney, and Alina Vrieling. 2022. "Limited Changes in Lifestyle Behaviours after Non-Muscle Invasive Bladder Cancer Diagnosis" Cancers 14, no. 4: 960. https://doi.org/10.3390/cancers14040960
APA StyleBeeren, I., Goeij, L. d., Dandis, R., Vidra, N., Zutphen, M. v., Witjes, J. A., Kampman, E., Kiemeney, L. A. L. M., & Vrieling, A. (2022). Limited Changes in Lifestyle Behaviours after Non-Muscle Invasive Bladder Cancer Diagnosis. Cancers, 14(4), 960. https://doi.org/10.3390/cancers14040960