
Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors
 , ,
, ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
- (1).
- The patient was initially diagnosed with a pathologically confirmed NSCLC between 1 January 2020 and 31 December 2021 at the Sankt Clara Hospital in Basel (Switzerland);
- (2).
- The patient underwent an FDG-PET/CT scan performed at the Sankt Clara Hospital in Basel (Switzerland) for staging before any treatment with regards to the proven NSCLC;
- (3).
- The patient was over the age of 18 years at the date of NSCLC diagnosis;
- (4).
- The patient consented to the use of their clinical data for research purposes.
2.2. Baseline Characteristics
2.3. FDG-PET/CT Acquisition
2.4. Primary Tumor Segmentation
2.4.1. Metabolic Features
2.4.2. Morphological Features
2.5. Long-Term Response Assessment
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Primary Tumor Segmentation
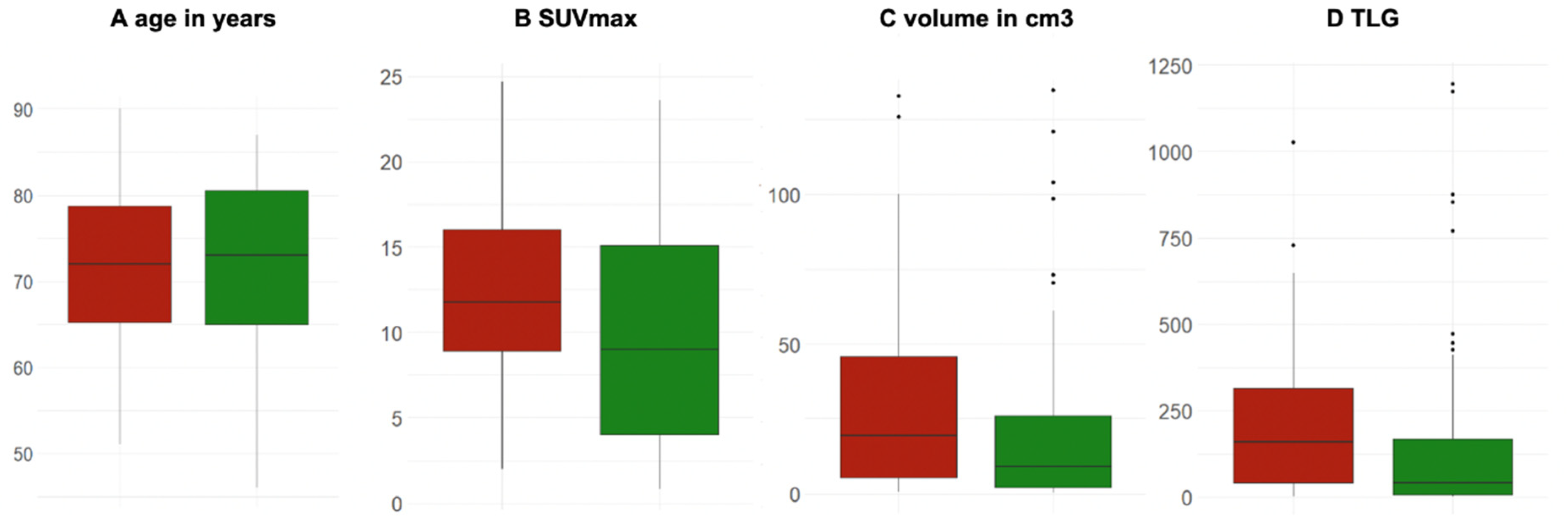
3.2.1. Metabolic Features of Primary Tumor
3.2.2. Morphological Features of Primary Tumor
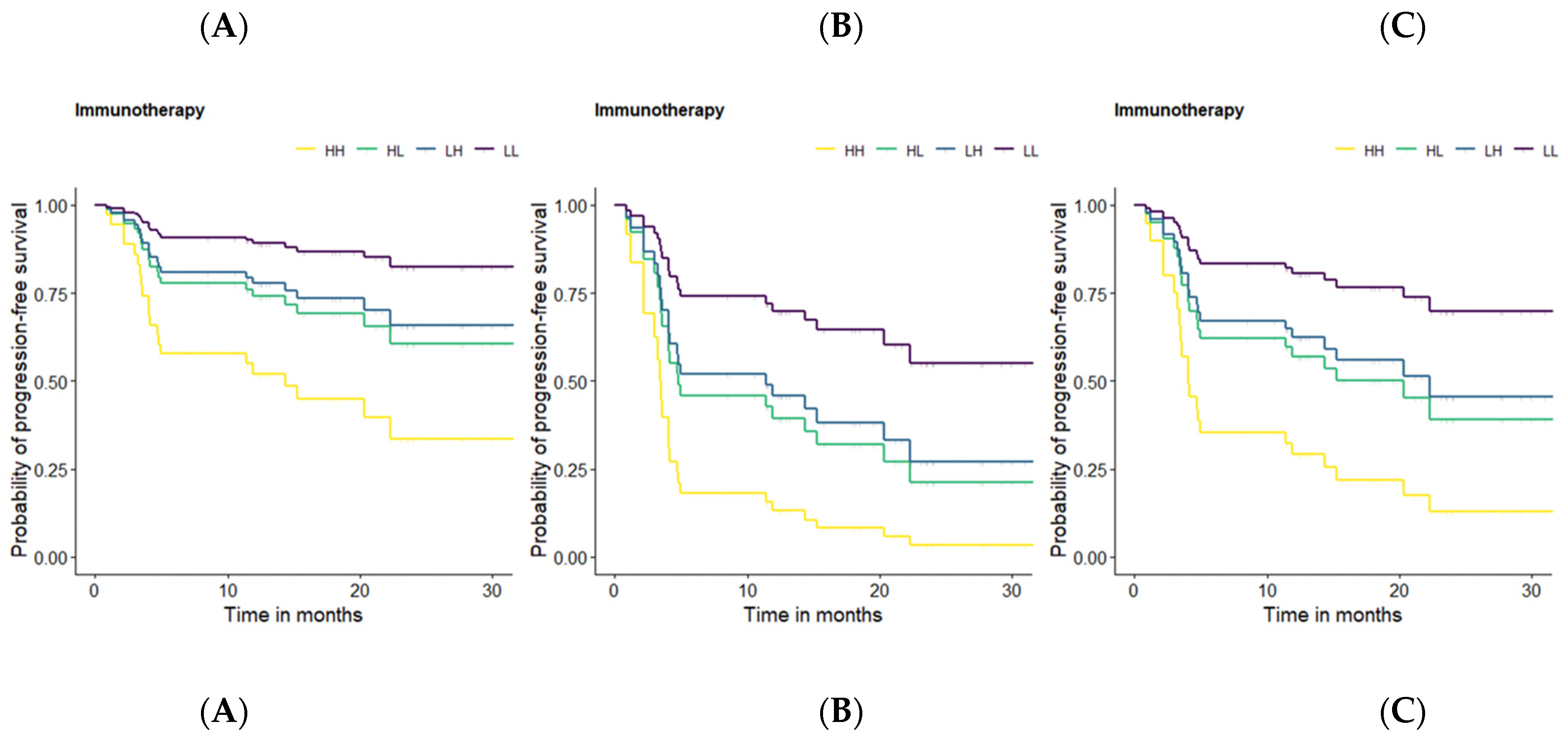
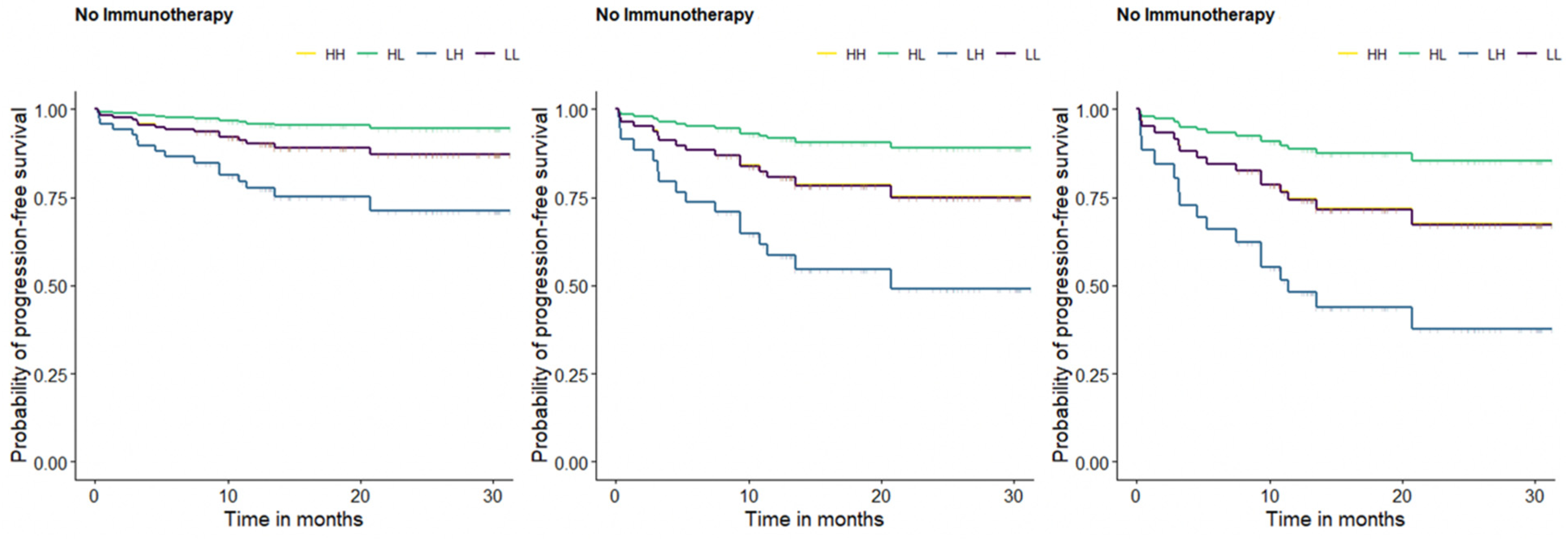
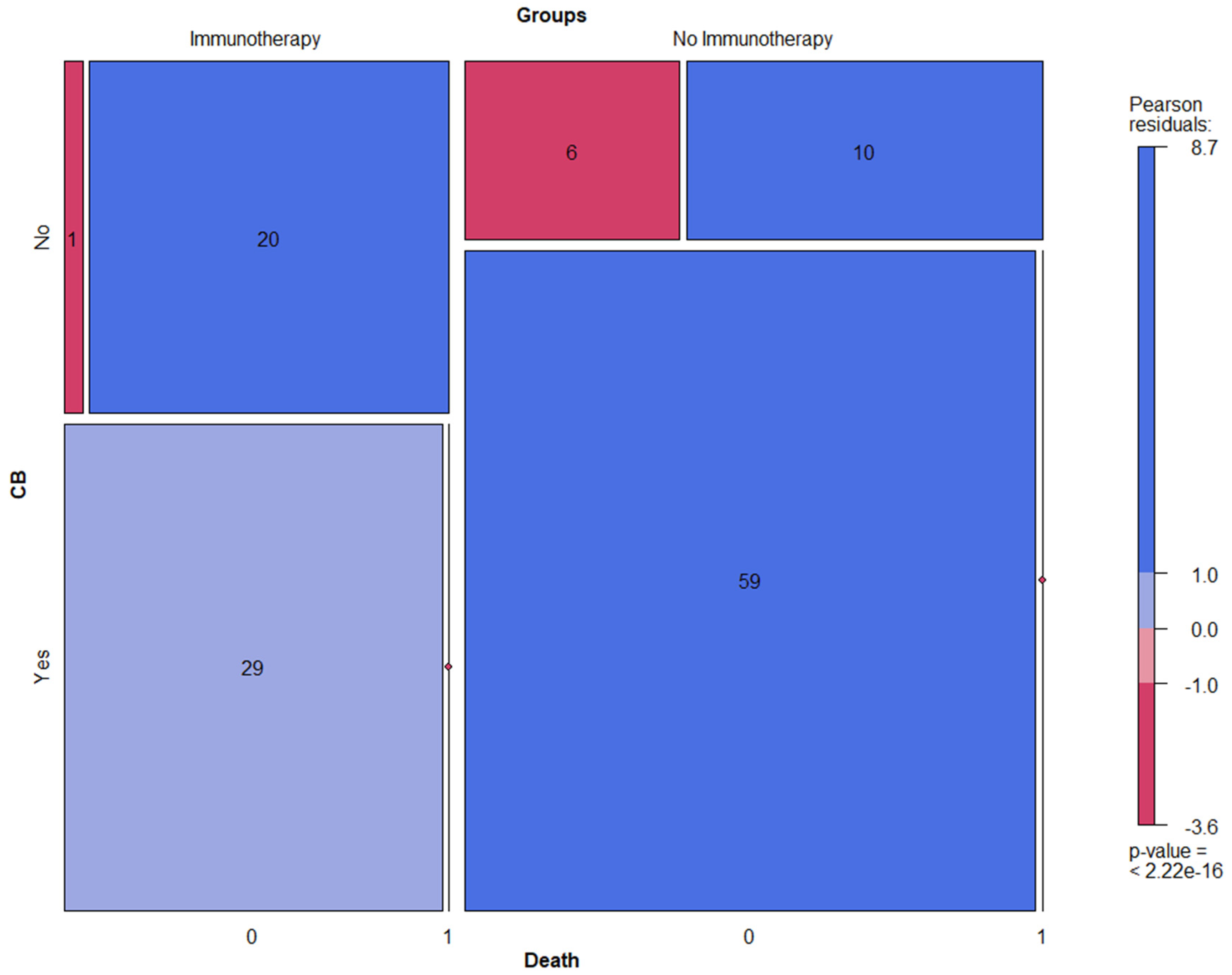
3.3. Long-Term Response Assessment
3.4. Prediction Model for Durable Treatment Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations (In Order of Appearance)
| NSCLC | Nonsmall cell lung cancer |
| SCLC | Small cell lung cancer |
| ICI | Immune checkpoint inhibitors |
| CTLA-4 | Cytotoxic T lymphocyte-associated molecule-4 |
| PD-1 | Programmed cell death receptor-1 |
| PD-L | Programmed cell death ligand-1 |
| IRAEs | Immune-related adverse events |
| TMB | Tumor mutational burden |
| TME | Tumor microenvironment |
| FDG-PET/CT | 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomography/computed tomography |
| GCP | Good clinical practice |
| EKNZ | Ethikkommission Nordwest- und Zentralschweiz |
| BMI | Body mass index |
| kg/m2 | Kilograms per squared meter |
| AJCC | American Joint Committee on Cancer |
| GE | General Electric |
| mmol/L | Millimoles per liter |
| IQR | Interquantile range |
| MBq | Megabecquerel |
| DLP | Dose length product |
| mGy/cm | Milligray per cm |
| 3D | Three-dimensional |
| TOF | Time-of-flight |
| AW | Advanced workstation |
| SUVmax | Standardized uptake value maximum |
| SUVmean | Standardized uptake value mean |
| MTV | Metabolic tumor volume |
| TLG | Total lesion glycolysis |
| VOI | Volume of interest |
| OSEM | Ordered subset expectation maximization |
| UL | Upper lobe |
| LL | Lower lobe |
| ML | Middle lobe |
| OS | Overall survival |
| PFS | Progression-free survival |
| CB | Clinical benefit |
| SD | Standard deviation |
| HR | Hazard ratio |
| CI | Confidence interval |
References
- Carter, B.W.; Halpenny, D.F.; Ginsberg, M.S.; Papadimitrakopoulou, V.A.; de Groot, P.M. Immunotherapy in Non-Small Cell Lung Cancer Treatment: Current Status and the Role of Imaging. J. Thorac. Imaging 2017, 32, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Polverari, G.; Ceci, F.; Bertaglia, V.; Reale, M.L.; Rampado, O.; Gallio, E.; Passera, R.; Liberini, V.; Scapoli, P.; Arena, V.; et al. 18F-FDG Pet Parameters and Radiomics Features Analysis in Advanced Nsclc Treated with Immunotherapy as Predictors of Therapy Response and Survival. Cancers 2020, 12, E1163. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Qin, C.; Hu, H.; Liu, T.; He, Y.; Guo, H.; Yan, H.; Zhang, J.; Tang, S.; Zhou, H. Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer: Progress, Challenges, and Prospects. Cells 2022, 11, 320. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Su, D.; Wang, J.; Cheng, Z.; Chin, Y.; Chen, L.; Chan, C.; Zhang, R.; Gao, T.; Ben, X.; et al. Predictive Value of Baseline Metabolic Tumor Volume for Non-Small-Cell Lung Cancer Patients Treated with Immune Checkpoint Inhibitors: A Meta-Analysis. Front. Oncol. 2022, 12, 951557. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Liang, H.; Zhong, W.; Zhao, J.; Chen, M.; Zhu, Z.; Xu, Y.; Wang, M. Prognostic Impact of Maximum Standardized Uptake Value on 18 F-FDG PET/CT Imaging of the Primary Lung Lesion on Survival in Advanced Non-Small Cell Lung Cancer: A Retrospective Study. Thorac. Cancer 2021, 12, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, N.; Wu, Z.; Pan, N.; Shen, X.; Liu, T.; Wei, F.; You, J.; Xu, W.; Ren, X. New Insight on the Correlation of Metabolic Status on 18F-FDG PET/CT with Immune Marker Expression in Patients with Non-Small Cell Lung Cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1127–1136. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Z. The History and Advances in Cancer Immunotherapy: Understanding the Characteristics of Tumor-Infiltrating Immune Cells and Their Therapeutic Implications. Cell Mol. Immunol. 2020, 17, 807–821. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus Docetaxel for Previously Treated, PD-L1-Positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010): A Randomised Controlled Trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Kudura, K.; Dimitriou, F.; Basler, L.; Förster, R.; Mihic-Probst, D.; Kutzker, T.; Dummer, R.; Mangana, J.; Burger, I.A.; Kreissl, M.C. Prediction of Early Response to Immune Checkpoint Inhibition Using FDG-PET/CT in Melanoma Patients. Cancers 2021, 13, 3830. [Google Scholar] [CrossRef]
- Kudura, K.; Nussbaumer, L.; Foerster, R.; Basler, L. Inflammatory Blood Parameters as Biomarkers for Response to Immune Checkpoint Inhibition in Metastatic Melanoma Patients. Biomedicines 2022, 10, 2135. [Google Scholar] [CrossRef] [PubMed]
- Chardin, D.; Paquet, M.; Schiappa, R.; Darcourt, J.; Bailleux, C.; Poudenx, M.; Sciazza, A.; Ilie, M.; Benzaquen, J.; Martin, N.; et al. Baseline Metabolic Tumor Volume as a Strong Predictive and Prognostic Biomarker in Patients with Non-Small Cell Lung Cancer Treated with PD1 Inhibitors: A Prospective Study. J. Immunother. Cancer 2020, 8, e000645. [Google Scholar] [CrossRef]
- Liao, X.; Liu, M.; Wang, R.; Zhang, J. Potentials of Non-Invasive 18F-FDG PET/CT in Immunotherapy Prediction for Non–Small Cell Lung Cancer. Front. Genet. 2022, 12, 810011. [Google Scholar] [CrossRef] [PubMed]
- Galvano, A.; Gristina, V.; Malapelle, U.; Pisapia, P.; Pepe, F.; Barraco, N.; Castiglia, M.; Perez, A.; Rolfo, C.; Troncone, G.; et al. The Prognostic Impact of Tumor Mutational Burden (TMB) in the First-Line Management of Advanced Non-Oncogene Addicted Non-Small-Cell Lung Cancer (NSCLC): A Systematic Review and Meta-Analysis of Randomized Controlled Trials. ESMO Open 2021, 6, 100124. [Google Scholar] [CrossRef] [PubMed]
- Monaco, L.; Gemelli, M.; Gotuzzo, I.; Bauckneht, M.; Crivellaro, C.; Genova, C.; Cortinovis, D.; Zullo, L.; Ammoni, L.; Bernasconi, D.; et al. Metabolic Parameters as Biomarkers of Response to Immunotherapy and Prognosis in Non-Small Cell Lung Cancer (NSCLC): A Real World Experience. Cancers 2021, 13, 1634. [Google Scholar] [CrossRef] [PubMed]
- Kandathil, A.; Kay, F.U.; Butt, Y.M.; Wachsmann, J.W.; Subramaniam, R.M. Role of FDG PET/CT in the Eighth Edition of TNM Staging of Non-Small Cell Lung Cancer. Radiographics 2018, 38, 2134–2149. [Google Scholar] [CrossRef]
- Lang, D.; Ritzberger, L.; Rambousek, V.; Horner, A.; Wass, R.; Akbari, K.; Kaiser, B.; Kronbichler, J.; Lamprecht, B.; Gabriel, M. First-Line Pembrolizumab Mono- or Combination Therapy of Non-Small Cell Lung Cancer: Baseline Metabolic Biomarkers Predict Outcomes. Cancers 2021, 13, 6096. [Google Scholar] [CrossRef]
- Seban, R.-D.; Assie, J.-B.; Giroux-Leprieur, E.; Massiani, M.-A.; Soussan, M.; Bonardel, G.; Chouaid, C.; Playe, M.; Goldfarb, L.; Duchemann, B.; et al. FDG-PET Biomarkers Associated with Long-Term Benefit from First-Line Immunotherapy in Patients with Advanced Non-Small Cell Lung Cancer. Ann. Nucl. Med. 2020, 34, 968–974. [Google Scholar] [CrossRef]
- Im, H.-J.; Bradshaw, T.; Solaiyappan, M.; Cho, S.Y. Current Methods to Define Metabolic Tumor Volume in Positron Emission Tomography: Which One Is Better? Nucl. Med. Mol. Imaging 2018, 52, 5–15. [Google Scholar] [CrossRef]
- Andraos, T.Y.; Halmos, B.; Cheng, H.; Huntzinger, C.; Shirvani, S.M.; Ohri, N. Disease Burden on PET Predicts Outcomes for Advanced NSCLC Patients Treated with First-Line Immunotherapy. Clin. Lung Cancer 2022, 23, 291–299. [Google Scholar] [CrossRef]
- Castello, A.; Rossi, S.; Toschi, L.; Lopci, E. Impact of Antibiotic Therapy and Metabolic Parameters in Non-Small Cell Lung Cancer Patients Receiving Checkpoint Inhibitors. J. Clin. Med. 2021, 10, 1251. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Calabrò, D.; Conci, N.; Argalia, G.; Marchese, P.V.; Fabbri, F.; Fragomeno, B.; Ricci, D.; Fanti, S.; Ambrosini, V.; et al. Baseline Total Metabolic Tumour Volume on 2-Deoxy-2-[18F]Fluoro-d-Glucose Positron Emission Tomography-Computed Tomography as a Promising Biomarker in Patients with Advanced Non-Small Cell Lung Cancer Treated with First-Line Pembrolizumab. Eur. J. Cancer 2021, 150, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Eude, F.; Guisier, F.; Salaün, M.; Thiberville, L.; Pressat-Laffouilhere, T.; Vera, P.; Decazes, P. Prognostic Value of Total Tumour Volume, Adding Necrosis to Metabolic Tumour Volume, in Advanced or Metastatic Non-Small Cell Lung Cancer Treated with First-Line Pembrolizumab. Ann. Nucl. Med. 2022, 36, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Kaira, K.; Yamaguchi, O.; Mouri, A.; Shiono, A.; Miura, Y.; Murayama, Y.; Kobayashi, K.; Kagamu, H.; Kuji, I. Potential of FDG-PET as Prognostic Significance after Anti-PD-1 Antibody against Patients with Previously Treated Non-Small Cell Lung Cancer. J. Clin. Med. 2020, 9, 725. [Google Scholar] [CrossRef] [PubMed]
- Icht, O.; Domachevsky, L.; Groshar, D.; Dudnik, E.; Rotem, O.; Allen, A.M.; Peled, N.; Reinhorn, D.; Jacobi, O.; Shochat, T.; et al. Lower Tumor Volume Is Associated with Increased Benefit from Immune Checkpoint Inhibitors in Patients with Advanced Non-Small-Cell Lung Cancer. Asia-Pac. J. Clin. Oncol. 2021, 17, e125–e131. [Google Scholar] [CrossRef] [PubMed]
- Kazuhiro, K.; Kawanaka, Y.; Komoto, H.; Minami, T.; Yokoi, T.; Kuribayashi, K.; Kijima, T.; Nakamura, A.; Hashimoto, M.; Kondo, N.; et al. The Utility of 68F-FDG PET/CT for Evaluation of Tumor Response to Immune Checkpoint Inhibitor Therapy and Prognosis Prediction in Patients with Non-Small-Cell Lung Cancer. Hell. J. Nucl. Med. 2021, 24, 186–198. [Google Scholar] [CrossRef]
- Seban, R.-D.; Mezquita, L.; Berenbaum, A.; Dercle, L.; Botticella, A.; Le Pechoux, C.; Caramella, C.; Deutsch, E.; Grimaldi, S.; Adam, J.; et al. Baseline Metabolic Tumor Burden on FDG PET/CT Scans Predicts Outcome in Advanced NSCLC Patients Treated with Immune Checkpoint Inhibitors. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1147–1157. [Google Scholar] [CrossRef]
- Vekens, K.; Everaert, H.; Neyns, B.; Ilsen, B.; Decoster, L. The Value of 18F-FDG PET/CT in Predicting the Response to PD-1 Blocking Immunotherapy in Advanced NSCLC Patients with High-Level PD-L1 Expression. Clin. Lung Cancer 2021, 22, 432–440. [Google Scholar] [CrossRef]
- Yamaguchi, O.; Kaira, K.; Hashimoto, K.; Mouri, A.; Shiono, A.; Miura, Y.; Murayama, Y.; Kobayashi, K.; Kagamu, H.; Kuji, I. Tumor Metabolic Volume by 18F-FDG-PET as a Prognostic Predictor of First-Line Pembrolizumab for NSCLC Patients with PD-L1 ≥ 50. Sci. Rep. 2020, 10, 14990. [Google Scholar] [CrossRef]
- Berghmans, T.; Dusart, M.; Paesmans, M.; Hossein-Foucher, C.; Buvat, I.; Castaigne, C.; Scherpereel, A.; Mascaux, C.; Moreau, M.; Roelandts, M.; et al. Primary Tumor Standardized Uptake Value (SUVmax) Measured on Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) Is of Prognostic Value for Survival in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review and Meta-Analysis (MA) by the European Lung Cancer Working Party for the IASLC Lung Cancer Staging Project. J. Thorac. Oncol. 2008, 3, 6–12. [Google Scholar] [CrossRef]
- Na, F.; Wang, J.; Li, C.; Deng, L.; Xue, J.; Lu, Y. Primary Tumor Standardized Uptake Value Measured on F18-Fluorodeoxyglucose Positron Emission Tomography Is of Prediction Value for Survival and Local Control in Non-Small-Cell Lung Cancer Receiving Radiotherapy: Meta-Analysis. J. Thorac. Oncol. 2014, 9, 834–842. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Baseline Characteristics | |
|---|---|
| Age median ± SD in years (IQR) | 72.0 ± 9.5 (65.0–80.0) |
| Gender | |
| Male | 64 (51.2%) |
| Female | 61 (48.8%) |
| BMI median ± SD in kg/m2 (IQR) | 24.8 ± 5.9 (22.3–29.0) |
| Histopathological subtype of NSCLC | |
| Adenocarcinoma | 59 (47.2%) |
| Squamous cell carcinoma | 31 (24.8%) |
| Large cell carcinoma | 17 (13.6%) |
| Neuroendocrine tumor | 15 (12.0%) |
| Not specific | 3 (2.4%) |
| PD-L1 expression | |
| >50% | 24 (19.2%) |
| 1–50% | 18 (14.4%) |
| <1% | 57 (45.6%) |
| Not available | 26 (20.8%) |
| Distant metastases | |
| On a patient level, in total | 125 (100%) |
| No distant metastasis | 79 (63.2%) |
| One distant metastasis | 33 (26.4%) |
| Two or more distant metastases | 13 (10.4%) |
| On a metastasis level, in total | 81 (100%) |
| Liver | 8 (9.9%) |
| Lung | 14 (17.3%) |
| Pleura | 13 (16.0%) |
| Bone | 17 (21.0%) |
| Suprarenal gland | 12 (14.8%) |
| Kidney | 1 (1.2%) |
| Soft tissue | 8 (9.9%) |
| Brain | 1 (1.2%) |
| Lymph node | 7 (8.6%) |
| Clinical staging (AJCC 8th edition) | |
| I | 29 (23.2%) |
| II | 7 (5.6%) |
| III | 43 (34.4%) |
| IV | 46 (36.8%) |
| Treatment regimen | |
| First-line ICI | 25 (20.0%) |
| Second-line ICI | 25 (20.0%) |
| No treatment with ICI | 75 (60.0%) |
| 2. Primary Tumor Segmentation | |
|---|---|
| a. Metabolic features of primary tumor | |
| SUVmax median ± SD (IQR) | 10.1 ± 6.0 (5.8–15.4) |
| SUVmean median ± SD (IQR) | 6.1 ± 3.5 (3.4–8.7) |
| MTV median ± SD (IQR) | 13.5 ± 30.7 (3.5–36.0) |
| TLG median ± SD (IQR) | 71.4 ± 247.7 (14.9–275.1) |
| b. Morphological features of primary tumor | |
| Volume median ± SD in cm3 (IQR) | 13.7 ± 30.7 (3.5–35.8) |
| Anatomical site (lung lobe UL/LL/ML and side R/L) | |
| ULR | 41 (32.8%) |
| LLR | 21 (16.8%) |
| ML | 14 (11.2%) |
| ULL | 32 (25.6%) |
| LLL | 13 (10.4%) |
| Two lobes | 4 (3.2%) |
| Localization of primary tumor within the lobe lung | |
| Central | 59 (47.2%) |
| Peripheral | 56 (44.8%) |
| Extensive (central & peripheral) | 10 (8.0%) |
| Morphology | |
| Solid | 108 (86.4%) |
| Subsolid | 7 (5.6%) |
| Mixed (solid/subsolid) | 8 (6.4%) |
| Cystic | 2 (1.6%) |
| Margin | |
| Sharp | 13 (10.4%) |
| Irregular | 96 (76.8%) |
| Spiculated | 16 (12.8%) |
| Lymphangiosis carcinomatosa | |
| Yes | 25 (20.0%) |
| No | 100 (80.0%) |
| 3.Long-Term Response Assessment | |
|---|---|
| Follow-up median ± SD in months (IQR) | 18.93 ± 6.98 (13.37–25.97) |
| OS median ± SD in months (IQR) | 14.80 ± 8.68 (10.73–23.93) |
| PFS median ± SD in months (IQR) | 14.03 ± 9.02 (9.37–23.60) |
| CB | |
| Yes | 88 (70.4%) |
| No | 37 (29.6%) |
| Death | |
| Yes | 30 (24.0%) |
| No | 95 (76.0%) |
| Immunotherapy | No Immunotherapy | |||||||
|---|---|---|---|---|---|---|---|---|
| OS | PFS | OS | PFS | |||||
| HR (CI) | p-Value | HR (CI) | p-Value | HR (CI) | p-Value | HR (CI) | p-Value | |
| Age | 0.92 (0.86, 0.98) | <0.01 | 0.92 (0.86, 0.98) | 0.01 | 1.02 (0.96, 1.09) | 0.49 | 1.03 (0.97, 1.10) | 0.28 |
| SUVmax | 1.36 (1.14, 1.64) | <0.01 | 1.30 (1.10, 1.54) | <0.01 | 1.05 (0.92, 1.19) | 0.45 | 1.08 (0.98, 1.24) | 0.23 |
| Volume | 1.07 (1.03, 1.12) | <0.01 | 1.06 (1.02–1.11) | <0.01 | 1.05 (0.99, 1.11) | 0.11 | 1.04 (1.00, 1.09) | 0.06 |
| TLG | 0.99 (0.98, 1.00) | <0.01 | 0.99 (0.99, 1.00 | <0.01 | 0.99 (0.99, 1.00) | 0.20 | 0.99 (0.99, 1.00) | 0.09 |
| Lymphangiosis | 4.03 (1.06, 17.51) | 0.04 | 4.53 (1.13, 18.20) | 0.03 | 1.70 (0.43 6.71) | 0.45 | 1.69 (0.45, 6.30) | 0.44 |
| Stage IV | 6.13 (1.10, 34.20) | 0.04 | 6.89 (1.20, 39.56) | 0.03 | 3.87 (0.72, 20.69) | 0.11 | 4.07 (0.84, 19.69) | 0.08 |
| Immunotherapy | No Immunotherapy | |||||||
|---|---|---|---|---|---|---|---|---|
| OS | PFS | OS | PFS | |||||
| SUVmax | ≤15.05 15.60 | >15.05 13.54 | ≤15.05 14.95 | >15.05 13.11 | ≤14.36 17.57 | >14.36 17.44 | ≤14.36 17.20 | >14.36 14.77 |
| Volume | ≤26.94 16.46 | >26.94 13.15 | ≤26.94 15.94 | >26.94 12.45 | ≤24.24 18.34 | >24.24 15.31 | ≤24.24 17.12 | >24.24 14.98 |
| Lymphangiosis | No 15.32 | Yes 14.40 | No 14.70 | Yes 13.89 | No 18.27 | Yes 13.21 | No 17.37 | Yes 11.82 |
| Clinical stage IV | No 17.69 | Yes 13.16 | No 16.62 | Yes 12.91 | No 18.45 | Yes 12.72 | No 17.39 | Yes 12.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kudura, K.; Ritz, N.; Kutzker, T.; Hoffmann, M.H.K.; Templeton, A.J.; Foerster, R.; Kreissl, M.C.; Antwi, K. Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors. Cancers 2022, 14, 6095. https://doi.org/10.3390/cancers14246095
Kudura K, Ritz N, Kutzker T, Hoffmann MHK, Templeton AJ, Foerster R, Kreissl MC, Antwi K. Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors. Cancers. 2022; 14(24):6095. https://doi.org/10.3390/cancers14246095
Chicago/Turabian StyleKudura, Ken, Nando Ritz, Tim Kutzker, Martin H. K. Hoffmann, Arnoud J. Templeton, Robert Foerster, Michael C. Kreissl, and Kwadwo Antwi. 2022. "Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors" Cancers 14, no. 24: 6095. https://doi.org/10.3390/cancers14246095
APA StyleKudura, K., Ritz, N., Kutzker, T., Hoffmann, M. H. K., Templeton, A. J., Foerster, R., Kreissl, M. C., & Antwi, K. (2022). Predictive Value of Baseline FDG-PET/CT for the Durable Response to Immune Checkpoint Inhibition in NSCLC Patients Using the Morphological and Metabolic Features of Primary Tumors. Cancers, 14(24), 6095. https://doi.org/10.3390/cancers14246095