

Magnetic Resonance Imaging-Based Predictive Models for Clinically Significant Prostate Cancer: A Systematic Review

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Evidence Acquisition
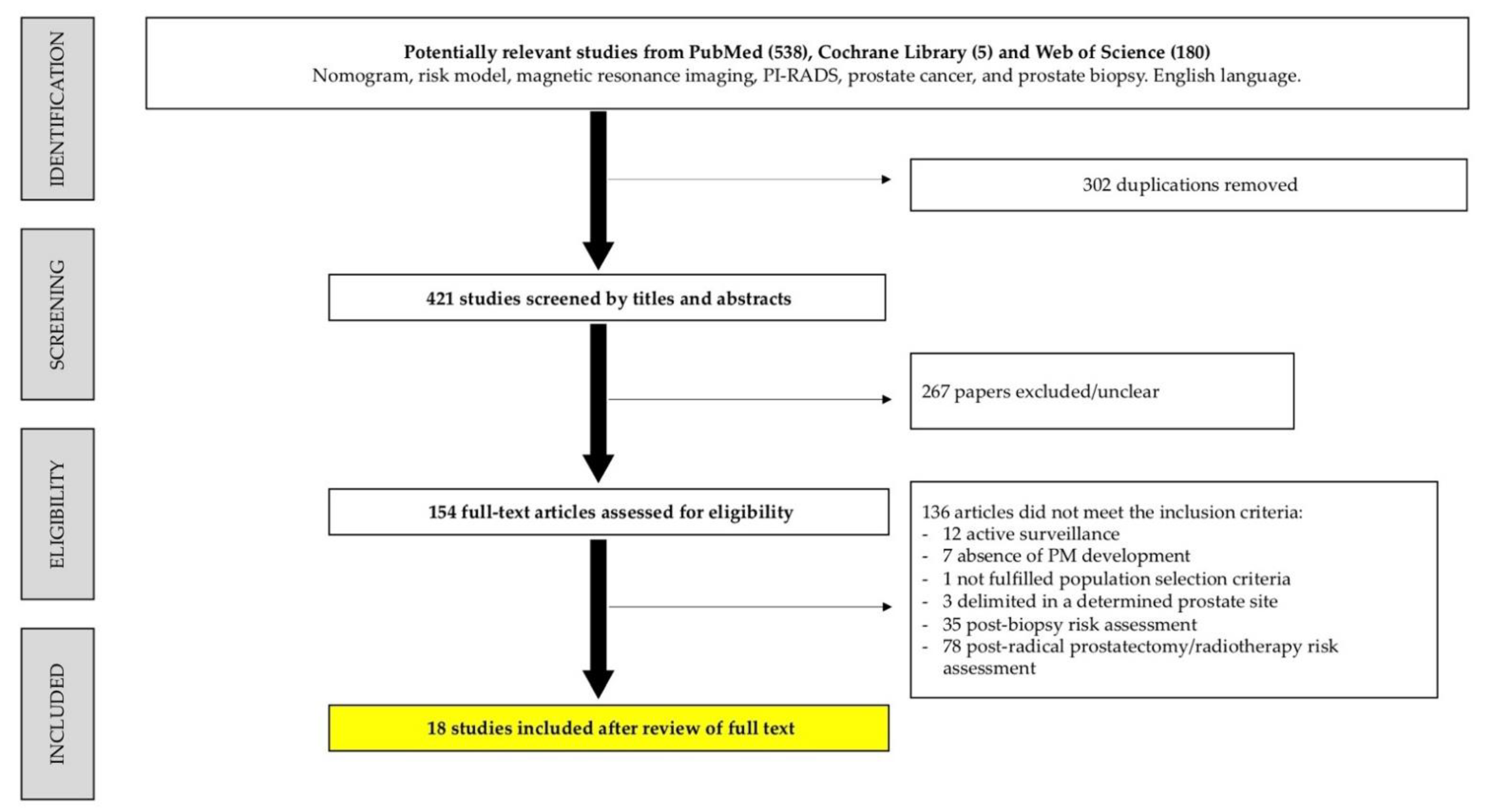
2.1. Search Strategy
2.2. Eligible Criteria
2.3. Study Selection
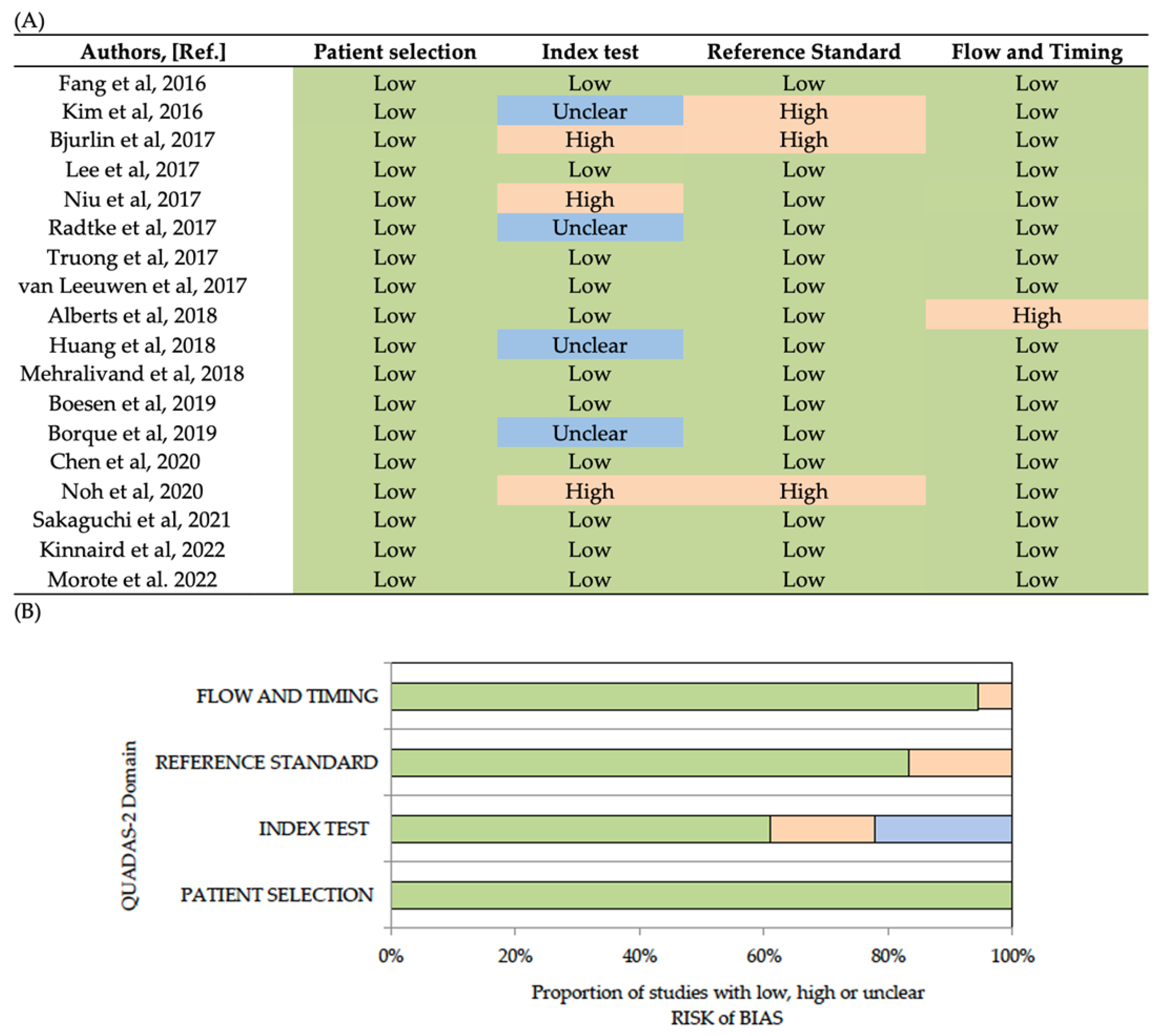
2.4. Quality Assessment
3. Synthesis of the Evid
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Correction Statement
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Drazer, M.W.; Huo, D.; Eggener, S.E. National Prostate Cancer Screening Rates after the 2012 US Preventive Services Task Force Recommendation Discouraging Prostate-Specific Antigen-Based Screening. J. Clin. Oncol. 2015, 33, 2416–2423. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Matoso, A.; Epstein, J.I. Defining Clinically Significant Prostate Cancer on the Basis of Pathological Findings. Histopathology 2019, 74, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Schoots, I.G.; Padhani, A.R.; Rouvière, O.; Barentsz, J.O.; Richenberg, J. Analysis of Magnetic Resonance Imaging-Directed Biopsy Strategies for Changing the Paradigm of Prostate Cancer Diagnosis. Eur. Urol. Oncol. 2020, 3, 32–41. [Google Scholar] [CrossRef]
- Drost, F.J.H.; Osses, D.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Roobol, M.J.; Schoots, I.G. Prostate Magnetic Resonance Imaging, with or Without Magnetic Resonance Imaging-Targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-Analysis. Eur. Urol. 2020, 77, 78–94. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Omer, A.; Harriss, E.; Davies, L.; Kasivisvanathan, V.; Punwani, S.; Moore, C.M.; Kastner, C.; Barrett, T.; Van Den Bergh, R.C.; et al. Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in the Detection of Clinically Significant Prostate Cancer in the Prostate Imaging Reporting and Data System Era: A Systematic Review and Meta-Analysis. Eur. Urol. 2020, 78, 402–414. [Google Scholar] [CrossRef]
- Moldovan, P.C.; Van den Broeck, T.; Sylvester, R.; Marconi, L.; Bellmunt, J.; van den Bergh, R.C.N.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Fossati, N.; et al. What Is the Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-Analysis from the European Association of Urology Prostate Cancer Guidelines Panel. Eur. Urol. 2017, 72, 250–266. [Google Scholar] [CrossRef]
- Mazzone, E.; Stabile, A.; Pellegrino, F.; Basile, G.; Cignoli, D.; Cirulli, G.O.; Sorce, G.; Barletta, F.; Scuderi, S.; Bravi, C.A.; et al. Positive Predictive Value of Prostate Imaging Reporting and Data System Version 2 for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Oncol. 2021, 4, 697–713. [Google Scholar] [CrossRef]
- Becerra, M.F.; Atluri, V.S.; Bhattu, A.S.; Punnen, S. Serum and Urine Biomarkers for Detecting Clinically Significant Prostate Cancer. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Celma, A.; Diaz, F.; Regis, L.; Roche, S.; Mast, R.; Semidey, M.E.; de Torres, I.M.; Planas, J.; Trilla, E. Prostatic-Specific Antigen Density Behavior According to Multiparametric Magnetic Resonance Imaging Result. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Schoots, I.G.; Roobol, M.J. Multivariate Risk Prediction Tools Including MRI for Individualized Biopsy Decision in Prostate Cancer Diagnosis: Current Status and Future Directions. World J. Urol. 2020, 38, 517–529. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Kattan, M.W. Nomograms for Prostate Cancer. BJU Int. 2006, 98, 39–46. [Google Scholar] [CrossRef]
- Borque-Fernando, Á.; Esteban, L.M.; Celma, A.; Roche, S.; Planas, J.; Regis, L.; de Torres, I.; Semidey, M.E.; Trilla, E.; Morote, J. How to Implement Magnetic Resonance Imaging before Prostate Biopsy in Clinical Practice: Nomograms for Saving Biopsies. World J. Urol. 2020, 38, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Borque-Fernando, A.; Triquell, M.; Celma, A.; Regis, L.; Escobar, M.; Mast, R.; de Torres, I.M.; Semidey, M.E.; Abascal, J.M.; et al. The Barcelona Predictive Model of Clinically Significant Prostate Cancer. Cancers 2022, 14, 1589. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, A.; Brisbane, W.; Kwan, L.; Priester, A.; Chuang, R.; Barsa, D.E.; Delfin, M.; Sisk, A.; Margolis, D.; Felker, E.; et al. A Prostate Cancer Risk Calculator (PCRC-MRI): Use of Clinical and Magnetic Resonance Imaging Data to Predict Biopsy Outcome in North American Men. Can. Urol. Assoc. J. 2021, 16, 161–166. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Altman, D.G.; Booth, A.; et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (Prisma-p) 2015: Elaboration and Explanation. BMJ 2015, 349, 1–25. [Google Scholar] [CrossRef]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a Knowledge Representation for Clinical Questions. AMIA Annu. Symp. Proc./AMIA Symp. 2006, 359–363. [Google Scholar]
- Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; Whiting, P.F.; Rutjes, A.W.S.S.; Westwood, M.E.; Mallet, S.; Deeks, J.J.; Reitsma, J.B.; et al. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar]
- Fang, D.; Zhao, C.; Ren, D.; Yu, W.; Wang, R.; Wang, H.; Li, X.; Yin, W.; Yu, X.; Yang, K.; et al. Could Magnetic Resonance Imaging Help to Identify the Presence of Prostate Cancer Before Initial Biopsy? The Development of Nomogram Predicting the Outcomes of Prostate Biopsy in the Chinese Population. Ann. Surg. Oncol. 2016, 23, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Weaver, J.K.; Shetty, A.S.; Vetter, J.M.; Andriole, G.L.; Strope, S.A. Magnetic Resonance Imaging Provides Added Value to the Prostate Cancer Prevention Trial Risk Calculator for Patients With Estimated Risk of High-Grade Prostate Cancer Less Than or Equal to 10%. Urology 2017, 102, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Bjurlin, M.A.; Rosenkrantz, A.B.; Sarkar, S.; Lepor, H.; Huang, W.C.; Huang, R.; Venkataraman, R.; Taneja, S.S. Prediction of Prostate Cancer Risk Among Men Undergoing Combined MRI-Targeted and Systematic Biopsy Using Novel Pre-Biopsy Nomograms That Incorporate MRI Findings. Urology 2018, 112, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Liyanage, S.H.; Wulaningsih, W.; Wolfe, K.; Carr, T.; Younis, C.; van Hemelrijck, M.; Popert, R.; Acher, P. Toward an MRI-Based Nomogram for the Prediction of Transperineal Prostate Biopsy Outcome: A Physician and Patient Decision Tool. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 664.e11–664.e18. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.K.; Li, J.; Das, S.K.; Xiong, Y.; Yang, C.B.; Peng, T. Developing a Nomogram Based on Multiparametric Magnetic Resonance Imaging for Forecasting High-Grade Prostate Cancer to Reduce Unnecessary Biopsies within the Prostate-Specific Antigen Gray Zone. BMC Med. Imaging 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Radtke, J.P.; Wiesenfarth, M.; Kesch, C.; Freitag, M.T.; Alt, C.D.; Celik, K.; Distler, F.; Roth, W.; Wieczorek, K.; Stock, C.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for Advanced Risk Modeling of Prostate Cancer—Patient-Tailored Risk Stratification Can Reduce Unnecessary Biopsies. Eur. Urol. 2017, 72, 888–896. [Google Scholar] [CrossRef]
- Truong, M.; Wang, B.; Gordetsky, J.B.; Nix, J.W.; Frye, T.P.; Messing, E.M.; Thomas, J.V.; Feng, C.; Rais-Bahrami, S. Multi-Institutional Nomogram Predicting Benign Prostate Pathology on Magnetic Resonance/Ultrasound Fusion Biopsy in Men with a Prior Negative 12-Core Systematic Biopsy. Cancer 2018, 124, 278–285. [Google Scholar] [CrossRef]
- Van Leeuwen, P.J.; Hayen, A.; Thompson, J.E.; Moses, D.; Shnier, R.; Böhm, M.; Abuodha, M.; Haynes, A.M.; Ting, F.; Barentsz, J.; et al. A Multiparametric Magnetic Resonance Imaging-Based Risk Model to Determine the Risk of Significant Prostate Cancer Prior to Biopsy. BJU Int. 2017, 120, 774–781. [Google Scholar] [CrossRef]
- Alberts, A.R.; Roobol, M.J.; Verbeek, J.F.M.; Schoots, I.G.; Chiu, P.K.; Osses, D.F.; Tijsterman, J.D.; Beerlage, H.P.; Mannaerts, C.K.; Schimmöller, L.; et al. Prediction of High-Grade Prostate Cancer Following Multiparametric Magnetic Resonance Imaging: Improving the Rotterdam European Randomized Study of Screening for Prostate Cancer Risk Calculators. Eur. Urol. 2019, 75, 310–318. [Google Scholar] [CrossRef]
- Huang, C.; Song, G.; Wang, H.; Ji, G.; Li, J.; Chen, Y.; Fan, Y.; Fang, D.; Xiong, G.; Xin, Z.; et al. MultiParametric Magnetic Resonance Imaging-Based Nomogram for Predicting Prostate Cancer and Clinically Significant Prostate Cancer in Men Undergoing Repeat Prostate Biopsy. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef]
- Mehralivand, S.; Shih, J.H.; Rais-Bahrami, S.; Oto, A.; Bednarova, S.; Nix, J.W.; Thomas, J.V.; Gordetsky, J.B.; Gaur, S.; Harmon, S.A.; et al. A Magnetic Resonance Imaging–Based Prediction Model for Prostate Biopsy Risk Stratification. JAMA Oncol. 2018, 4, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Boesen, L.; Thomsen, F.B.; Nørgaard, N.; Løgager, V.; Balslev, I.; Bisbjerg, R.; Thomsen, H.S.; Jakobsen, H. A Predictive Model Based on Biparametric Magnetic Resonance Imaging and Clinical Parameters for Improved Risk Assessment and Selection of Biopsy-Naïve Men for Prostate Biopsies. Prostate Cancer Prostatic Dis. 2019, 22, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Yang, Y.; Peng, T.; Yu, X.; Deng, H.; Guo, Z. The Prediction Value of PI-RADS v2 Score in High-Grade Prostate Cancer: A Multicenter Retrospective Study. Int. J. Med. Sci. 2020, 17, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Noh, T.I.; Hyun, C.W.; Kang, H.E.; Jin, H.J.; Tae, J.H.; Shim, J.S.; Kang, S.G.; Sung, D.J.; Cheon, J.; Lee, J.G.; et al. A Predictive Model Based on Bi-Parametric Magnetic Resonance Imaging and Clinical Parameters for Clinically Significant Prostate Cancer in the Korean Population. Cancer Res. Treat. 2021, 53, 1148–1155. [Google Scholar] [CrossRef]
- Sakaguchi, K.; Hayashida, M.; Tanaka, N.; Oka, S.; Urakami, S. A Risk Model for Detecting Clinically Significant Prostate Cancer Based on Bi-Parametric Magnetic Resonance Imaging in a Japanese Cohort. Sci. Rep. 2021, 11, 18829. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Renson, A.; Rais-Bahrami, S.; Truong, M.; Rosenkrantz, A.B.; Huang, R.; Taneja, S.S. Predicting Benign Prostate Pathology on Magnetic Resonance Imaging/Ultrasound Fusion Biopsy in Men with a Prior Negative 12-Core Systematic Biopsy: External Validation of a Prognostic Nomogram. Eur. Urol. Focus. 2019, 5, 815–822. [Google Scholar] [CrossRef]
- Chen, R.; Verbeek, J.F.M.; Yang, Y.; Song, Z.; Sun, Y.; Roobol, M.J. Comparing the Prediction of Prostate Biopsy Outcome Using the Chinese Prostate Cancer Consortium (CPCC) Risk Calculator and the Asian Adapted Rotterdam European Randomized Study of Screening for Prostate Cancer (ERSPC) Risk Calculator in Chinese and Europ. World J. Urol. 2021, 39, 73–80. [Google Scholar] [CrossRef]
- De Nunzio, C.; Lombardo, R.; Baldassarri, V.; Cindolo, L.; Bertolo, R.; Minervini, A.; Sessa, F.; Muto, G.; Bove, P.; Vittori, M.; et al. Rotterdam Mobile Phone App Including MRI Data for the Prediction of Prostate Cancer: A Multicenter External Validation. Eur. J. Surg. Oncol. 2021, 47, 2640–2645. [Google Scholar] [CrossRef]
- Remmers, S.; Kasivisvanathan, V.; Verbeek, J.F.M.; Moore, C.M.; Roobol, M.J. Reducing Biopsies and Magnetic Resonance Imaging Scans During the Diagnostic Pathway of Prostate Cancer: Applying the Rotterdam Prostate Cancer Risk Calculator to the PRECISION Trial Data. Eur. Urol. Open Sci. 2022, 36, 1–8. [Google Scholar] [CrossRef]
- Louie, K.S.; Seigneurin, A.; Cathcart, P.; Sasieni, P. Do Prostate Cancer Risk Models Improve the Predictive Accuracy of PSA Screening? A Meta-Analysis. Ann. Oncol. 2015, 26, 848–864. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Carroll, P.R.; Eggener, S.; Fulgham, P.F.; Margolis, D.J.; Pinto, P.A.; Rosenkrantz, A.B.; Rubenstein, J.N.; Rukstalis, D.B.; Taneja, S.S.; et al. Update of the Standard Operating Procedure on the Use of Multiparametric Magnetic Resonance Imaging for the Diagnosis, Staging and Management of Prostate Cancer. J. Urol. 2020, 203, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Sherrer, R.L.; Glaser, Z.A.; Gordetsky, J.B.; Nix, J.W.; Porter, K.K.; Rais-Bahrami, S. Comparison of Biparametric MRI to Full Multiparametric MRI for Detection of Clinically Significant Prostate Cancer. Prostate Cancer Prostatic Dis. 2019, 22, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.K.; King, A.; Galgano, S.J.; Sherrer, R.L.; Gordetsky, J.B.; Rais-Bahrami, S. Financial Implications of Biparametric Prostate MRI. Prostate Cancer Prostatic Dis. 2020, 23, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Tamada, T.; Kido, A.; Yamamoto, A.; Takeuchi, M.; Miyaji, Y.; Moriya, T.; Sone, T. Comparison of Biparametric and Multiparametric MRI for Clinically Significant Prostate Cancer Detection With PI-RADS Version 2.1. J. Magn. Reson. Imaging 2021, 53, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic Performance of Prostate Imaging Reporting and Data System Version 2 for Detection of Prostate Cancer: A Systematic Review and Diagnostic Meta-Analysis. Eur. Urol. 2017, 72, 177–188. [Google Scholar] [CrossRef]
- Radtke, J.P.; Giganti, F.; Wiesenfarth, M.; Stabile, A.; Marenco, J.; Orczyk, C.; Kasivisvanathan, V.; Nyarangi-Dix, J.N.; Schütz, V.; Dieffenbacher, S.; et al. Prediction of Significant Prostate Cancer in Biopsy-Naïve Men: Validation of a Novel Risk Model Combining MRI and Clinical Parameters and Comparison to an ERSPC Risk Calculator and PI-RADS. PLoS ONE 2019, 14, e0221350. [Google Scholar] [CrossRef]
- Osses, D.F.; Roobol, M.J.; Schoots, I.G. Prediction Medicine: Biomarkers, Risk Calculators and Magnetic Resonance Imaging as Risk Stratification Tools in Prostate Cancer Diagnosis. Int. J. Mol. Sci. 2019, 20, 1637. [Google Scholar] [CrossRef]
- Ilic, D.; Djulbegovic, M.; Jung, J.H.; Hwang, E.C.; Zhou, Q.; Cleves, A.; Agoritsas, T.; Dahm, P. Prostate Cancer Screening with Prostate-Specific Antigen (PSA) Test: A Systematic Review and Meta-Analysis. BMJ 2018, 362, k3519. [Google Scholar] [CrossRef]
- Vickers, A.J.; Cronin, A.M.; Roobol, M.J.; Hugosson, J.; Jones, J.S.; Clinic, C.; Kattan, M.W.; Klein, E.; Hamdy, F.; Neal, D.; et al. Cancer Risk: The Prostate Biopsy Collaborative Group. Clin. Cancer Res. 2011, 16, 4374–4381. [Google Scholar] [CrossRef]
- Massanova, M.; Robertson, S.; Barone, B.; Dutto, L.; Caputo, V.F.; Bhatt, J.R.; Ahmad, I.; Bada, M.; Obeidallah, A.; Crocetto, F. The Comparison of Imaging and Clinical Methods to Estimate Prostate Volume: A Single-Centre Retrospective Study. Urol. Int. 2021, 105, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Nordström, T.; Akre, O.; Aly, M.; Grönberg, H.; Eklund, M. Prostate-Specific Antigen (PSA) Density in the Diagnostic Algorithm of Prostate Cancer. Prostate Cancer Prostatic Dis. 2018, 21, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Boyle, H.J.; Alibhai, S.; Decoster, L.; Efstathiou, E.; Fizazi, K.; Mottet, N.; Oudard, S.; Payne, H.; Prentice, M.; Puts, M.; et al. Updated Recommendations of the International Society of Geriatric Oncology on Prostate Cancer Management in Older Patients. Eur. J. Cancer 2019, 116, 116–136. [Google Scholar] [CrossRef] [PubMed]
- Cui, T.; Kovell, R.C.; Terlecki, R.P. Is It Time to Abandon the Digital Rectal Examination? Lessons from the PLCO Cancer Screening Trial and Peer-Reviewed Literature. Curr. Med. Res. Opin. 2016, 32, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Okotie, O.T.; Roehl, K.A.; Han, M.; Loeb, S.; Gashti, S.N.; Catalona, W.J. Characteristics of Prostate Cancer Detected by Digital Rectal Examination Only. Urology 2007, 70, 1117–1120. [Google Scholar] [CrossRef]
- Gandaglia, G.; Leni, R.; Bray, F.; Fleshner, N.; Freedland, S.J.; Kibel, A.; Stattin, P.; Van Poppel, H.; La Vecchia, C. Epidemiology and Prevention of Prostate Cancer. Eur. Urol. Oncol. 2021, 4, 877–892. [Google Scholar] [CrossRef]
- Evans, S.; Metcalfe, C.; Ibrahim, F.; Persad, R.; Ben-Shlomo, Y. Investigating Black-White Differences in Prostate Cancer Prognosis: A Systematic Review and Meta-Analysis. Int. J. Cancer 2008, 123, 430–435. [Google Scholar] [CrossRef]
- Dess, R.T.; Hartman, H.E.; Mahal, B.A.; Soni, P.D.; Jackson, W.C.; Cooperberg, M.R.; Amling, C.L.; Aronson, W.J.; Kane, C.J.; Terris, M.K.; et al. Association of Black Race with Prostate Cancer-Specific and Other-Cause Mortality. JAMA Oncol. 2019, 5, 975–983. [Google Scholar] [CrossRef]
- Pradere, B.; Veeratterapillay, R.; Dimitropoulos, K.; Yuan, Y.; Omar, M.I.; MacLennan, S.; Cai, T.; Bruyère, F.; Bartoletti, R.; Köves, B.; et al. Nonantibiotic Strategies for the Prevention of Infectious Complications Following Prostate Biopsy: A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 653–663. [Google Scholar] [CrossRef]
- Tu, X.; Liu, Z.; Chang, T.; Qiu, S.; Xu, H.; Bao, Y.; Yang, L.; Wei, Q. Transperineal Magnetic Resonance Imaging–Targeted Biopsy May Perform Better Than Transrectal Route in the Detection of Clinically Significant Prostate Cancer: Systematic Review and Meta-Analysis. Clin. Genitourin. Cancer 2019, 17, e860–e870. [Google Scholar] [CrossRef]
- Khoo, C.C.; Eldred-Evans, D.; Peters, M.; van Son, M.; van Rossum, P.S.N.; Connor, M.J.; Hosking-Jervis, F.; Tanaka, M.B.; Reddy, D.; Bass, E.; et al. A Comparison of Prostate Cancer Detection between Visual Estimation (Cognitive Registration) and Image Fusion (Software Registration) Targeted Transperineal Prostate Biopsy. J. Urol. 2021, 205, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Bass, E.J.; Pantovic, A.; Connor, M.; Gabe, R.; Padhani, A.R.; Rockall, A.; Sokhi, H.; Tam, H.; Winkler, M.; Ahmed, H.U. A Systematic Review and Meta-Analysis of the Diagnostic Accuracy of Biparametric Prostate MRI for Prostate Cancer in Men at Risk. Prostate Cancer Prostatic Dis. 2021, 24, 596–611. [Google Scholar] [CrossRef] [PubMed]
- JLH van Leenders, G.; van der Kwast, T.H.; Grignon, D.J.; Evans, A.J.; Kristiansen, G.; Kweldam, C.F.; Litjens, G.; McKenney, J.K.; Melamed, J.; Mottet, N.; et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2020, 44, 87–99. [Google Scholar] [CrossRef]
- Liu, C.; Liu, S.L.; Wang, Z.X.; Yu, K.; Feng, C.X.; Ke, Z.; Wang, L.; Zeng, X.Y. Using the Prostate Imaging Reporting and Data System Version 2 (PI-RIDS v2) to Detect Prostate Cancer Can Prevent Unnecessary Biopsies and Invasive Treatment. Asian. J. Androl. 2018, 20, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Andras, I.; Cata, E.D.; Serban, A.; Kadula, P.; Telecan, T.; Buzoianu, M.; Bungardean, M.; Stanca, D.V.; Coman, I.; Crisan, N. Combined Systematic and Mri-Us Fusion Prostate Biopsy Has the Highest Grading Accuracy When Compared to Final Pathology. Medicina 2021, 57, 519. [Google Scholar] [CrossRef] [PubMed]
- Wynants, L.; Van Smeden, M.; McLernon, D.J.; Timmerman, D.; Steyerberg, E.W.; Van Calster, B. Three Myths about Risk Thresholds for Prediction Models. BMC Med. 2019, 17, 192. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Van Calster, B.; Steyerberg, E.W. Net Benefit Approaches to the Evaluation of Prediction Models, Molecular Markers, and Diagnostic Tests. BMJ 2016, 352, 3–7. [Google Scholar] [CrossRef]
- Püllen, L.; Radtke, J.P.; Wiesenfarth, M.; Roobol, M.J.; Verbeek, J.F.M.; Wetter, A.; Guberina, N.; Pandey, A.; Hüttenbrink, C.; Tschirdewahn, S.; et al. External Validation of Novel Magnetic Resonance Imaging-Based Models for Prostate Cancer Prediction. BJU Int. 2020, 125, 407–416. [Google Scholar] [CrossRef]
- Saba, K.; Wettstein, M.S.; Lieger, L.; Hötker, A.M.; Donati, O.F.; Moch, H.; Ankerst, D.P.; Poyet, C.; Sulser, T.; Eberli, D.; et al. External Validation and Comparison of Prostate Cancer Risk Calculators Incorporating Multiparametric Magnetic Resonance Imaging for Prediction of Clinically Significant Prostate Cancer. J. Urol. 2020, 203, 719–726. [Google Scholar] [CrossRef]
- Ankerst, D.P.; Straubinger, J.; Selig, K.; Guerrios, L.; De Hoedt, A.; Hernandez, J.; Liss, M.A.; Leach, R.J.; Freedland, S.J.; Kattan, M.W.; et al. A Contemporary Prostate Biopsy Risk Calculator Based on Multiple Heterogeneous Cohorts. Eur. Urol. 2018, 74, 197–203. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; de Cobelli, O.; Musi, G.; del Giudice, F.; Carrieri, G.; Busetto, G.M.; Falagario, U.G.; Sciarra, A.; Maggi, M.; Crocetto, F.; et al. Radiomics in Prostate Cancer: An up-to-Date Review. Ther. Adv. Urol. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Seetharaman, A.; Bhattacharya, I.; Chen, L.C.; Kunder, C.A.; Shao, W.; Soerensen, S.J.C.; Wang, J.B.; Teslovich, N.C.; Fan, R.E.; Ghanouni, P.; et al. Automated Detection of Aggressive and Indolent Prostate Cancer on Magnetic Resonance Imaging. Med. Phys. 2021, 48, 2960–2972. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, I.; Seetharaman, A.; Kunder, C.; Shao, W.; Chen, L.C.; Soerensen, S.J.C.; Wang, J.B.; Teslovich, N.C.; Fan, R.E.; Ghanouni, P.; et al. Selective Identification and Localization of Indolent and Aggressive Prostate Cancers via CorrSigNIA: An MRI-Pathology Correlation and Deep Learning Framework: CorrSigNIA: An MRI-Pathology Correlation and Deep Learning Framework. Med. Image Anal. 2022, 75, 102288. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Bao, M.L.; Wu, C.J.; Zhang, J.; Zhang, Y.D.; Shi, H. bin A Radiomics Machine Learning-Based Redefining Score Robustly Identifies Clinically Significant Prostate Cancer in Equivocal PI-RADS Score 3 Lesions. Abdom. Radiol. 2020, 45, 4223–4234. [Google Scholar] [CrossRef]
- Brancato, V.; Aiello, M.; Basso, L.; Monti, S.; Palumbo, L.; di Costanzo, G.; Salvatore, M.; Ragozzino, A.; Cavaliere, C. Evaluation of a Multiparametric MRI Radiomic-Based Approach for Stratification of Equivocal PI-RADS 3 and Upgraded PI-RADS 4 Prostatic Lesions. Sci. Rep. 2021, 11, 643. [Google Scholar] [CrossRef]
- Wang, J.; Wu, C.J.; Bao, M.L.; Zhang, J.; Wang, X.N.; Zhang, Y.D. Machine Learning-Based Analysis of MR Radiomics Can Help to Improve the Diagnostic Performance of PI-RADS v2 in Clinically Relevant Prostate Cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef]
- Soerensen, S.J.C.; Fan, R.E.; Seetharaman, A.; Chen, L.; Shao, W.; Bhattacharya, I.; Kim, Y.H.; Sood, R.; Borre, M.; Chung, B.I.; et al. Deep Learning Improves Speed and Accuracy of Prostate Gland Segmentations on Magnetic Resonance Imaging for Targeted Biopsy. J. Urol. 2021, 206, 604–612. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, W.; Yue, X.; Shen, J.; Gao, C.; Pang, P.; Cui, F.; Xu, M. Development of a Novel, Multi-Parametric, MRI-Based Radiomic Nomogram for Differentiating Between Clinically Significant and Insignificant Prostate Cancer. Front. Oncol. 2020, 10, 888. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Authors, Year [Ref.] | Biopsy Status | MRI/T | PI-RADS Version | Biopsy Approach | Systematic Biopsy | Guided Biopsy | Type of GB | csPCa Definition |
|---|---|---|---|---|---|---|---|---|
| Fang et al., 2016 [21] | 984/0 | mp/1.5–3 | 1 | TR | 12 | NA/≥3 | NA | GS ≥ 3+4 |
| Kim et al., 2016 [22] | 185/154 | mp/3 | 1–2 | TR | 12 | NA/≥4 | Cog/Soft | GS ≥ 3+4 |
| Bjurlin et al., 2017 [23] | 288/171 | mp/3 | 1 | TR | 12 | 1–4/≥3 | Soft | GS ≥ 3+4 |
| Lee et al., 2017 [24] | 484/131 | bp/1.5 | 1 | TP | 24–40 * | 2–4/≥3 | Cog | GS≥7 or MCCL≥ 6 mm |
| Niu et al., 2017 [25] | 151/0 | mp/3 | 2 | TR | 12 | 1/≥3 | Cog | GS ≥ 3+4 |
| Radtke et al., 2017 [26] | 670/489 | mp/3 | 1 | TP | 24 * | 2–4/≥2 | Soft | GS ≥ 3+4 |
| Truong et al., 2017 [27] | 0/285 | mp/3 | 2 | TR | 12–24 * | 2/≥3 | Soft | GS ≥ 3+4 |
| van Leeuwen et al., 2017 [28] | 344/49 | mp/1.5–3 | 1 | TP | 30 * | 2/≥3 | Soft/Cog | GS≥ 7/> 5% G4 or MLCL≥ 20%/7 mm |
| Alberts et al., 2018 [29] | 504/457 | mp-bp/3 | 1–2 | TR | 12 | NA/≥3 | In bore/Cog/Soft | GS ≥ 3+4 |
| Huang et al., 2018 [30] | 0/231 | mp/1.5–3 | 2 | TR | 12 | 2/≥4 | NA | GS ≥ 3+4 |
| Mehralivand et al., 2018 [31] | 179/221 | mp/NA | 2 | TR | 12 | 2/≥3 | Soft | GS ≥ 3+4 |
| Boesen et al., 2019 [32] | 876/0 | bp/3 | 2 | TR | 10 | 2/≥3 | Cog | GG ≥ 2 |
| Borque et al., 2019 [15] | 163/183 | mp/3 | 2 | TR | 12 | 2/≥3 | Cog | GG ≥ 2 |
| Chen et al., 2020 [33] | 316 | mp/NA | 2 | NA | NA | NA | NA | GS ≥ 3+4 |
| Noh et al., 2020 [34] | 215/85 | bp/3 | 2 | TP | 24–20 * | 2–10/≥3 | Cog | GS ≥ 3+4 |
| Sakaguchi et al., 2021 [35] | 773/0 | bp/1.5–3 | 2 | TR | 8–14 | 2–4/≥3 | Cog | GG3 or MCCL≥ 6 mm |
| Kinnaird et al., 2022 [17] | 1449/905 | mp/3 | 2 | TR | 12 | 2–3/≥3 | Cog | GG ≥ 2 |
| Morote et al. 2022 [16] | 1098/388 | mp/3 | 2 | TR | 12 | 2–4/≥3 | Cog | GG ≥ 2 |
| Authors, [Ref.] | Age | PCa FH | DRE | Biopsy Status | Ethnicity | PSA | PSAD | PV |
|---|---|---|---|---|---|---|---|---|
| Fang et al., 2016 [21] | Y | N | Y | N | N | Y | N | Y |
| Kim et al., 2016 [22] | Y | Y | Y | Y | Y | Y | N | N |
| Bjurlin et al., 2017 [23] | Y | N | N | N | N | N | Y | N |
| Lee et al., 2017 [24] | Y | N | N | Y | N | N | Y | N |
| Niu et al., 2017 [25] | Y | N | N | N | N | N | Y | N |
| Radtke et al., 2017 [26] | Y | N | Y | N | N | Y | N | Y |
| Truong et al., 2017 [27] | Y | N | N | N | N | Y | N | Y |
| van Leeuwen et al., 2017 [28] | Y | N | Y | N | N | Y | N | Y |
| Alberts et al., 2018 [29] | Y | N | Y | N | N | Y | N | Y |
| Huang et al., 2018 [30] | Y | N | Y | N | N | Y | N | Y |
| Mehralivand et al., 2018 [31] | N | N | Y | Y | Y | Y | N | N |
| Boesen et al., 2019 [32] | Y | N | Y | N | N | N | Y | N |
| Borque et al., 2019 [15] | Y | N | Y | Y | N | N | Y | N |
| Chen et al., 2020 [33] | N | N | N | N | N | Y | N | Y |
| Noh et al., 2020 [34] | Y | N | N | N | N | N | Y | N |
| Sakaguchi et al., 2021 [35] | Y | N | N | N | N | Y | N | Y |
| Kinnaird et al., 2022 [17] | Y | N | Y | Y | Y | Y | Y | Y |
| Morote et al. 2022 [16] | Y | Y | Y | Y | N | Y | N | Y |
| Authors, [Ref.] | n | Repeat Biopsy | csPCa | Sen. | Spe. | Avoided Biopsies | Cut-Off | AUROC | DCA | CUC |
|---|---|---|---|---|---|---|---|---|---|---|
| Fang et al., 2016 [21] | 894 | 0 | 24.4 | 95 | 38 | 19.8 | 30 | 0.87 | 5 | NA |
| Kim et al., 2016 [22] | 339 | 35.4 | 34.0 | 95 | 20 | 15.1 | NA | 0.78 | NA | NA |
| Bjurlin et al., 2017 [23] | 288 | 0 | 33.6 | 95 | 56 | 42.2 | NA | 0.91 | NA | NA |
| Bjurlin et al., 2017 [23] | 171 | 100 | 18.1 | 95 | 40 | 33.9 | NA | 0.86 | NA | NA |
| Lee et al., 2017 [24] | 615 | 21.3 | 38.5 | 97.5 | 54.8 | 34.6 | 30 | 0.92 | NA | NA |
| Niu et al., 2017 [25] | 151 | 0 | 21.0 | 87.3 | 78.4 | 64.9 | 36 | 0.85 | NA | NA |
| Radtke et al., 2017 [26] | 660 | 0 | NA | 95 | 35 | NA | NA | 0.83 | 16 | NA |
| Radtke et al., 2017 [26] | 335 | 100 | NA | 95 | 25.5 | NA | NA | 0.81 | 12 | NA |
| Truong et al., 2017 [27] | 285 | 100 | 38.9 | 94.7 | 57.5 | 36.5 | 40 | 0.83 | 1 | NA |
| van Leeuwen et al., 2017 [28] | 393 | 12.5 | 37.9 | 93.9 | NA | 34.4 | 12.5 | 0.88 | 4 | NA |
| Alberts et al., 2018 [29] | 504 | 0 | 42.0 | 92 | NA | 24.0 | 15 | 0.84 | 10 | NA |
| Alberts et al., 2018 [29] | 504 | 100 | 29.0 | 95 | NA | 41.0 | 15 | 0.85 | 5 | NA |
| Huang et al., 2018 [30] | 231 | 100 | 25.5 | 95 | 63 | 48.0 | 21 | 0.92 | 10 | NA |
| Mehralivand et al., 2018 [31] | 400 | 55.2 | 48.3 | 96 | 54 | 30.0 | 15 | 0.84 | 10 | NA |
| Boesen et al., 2019 [32] | 876 | 0 | 40.0 | 96 | 60 | 38.0 | 15 | 0.89 | 5 | NA |
| Borque et al., 2019 [15] | 346 | 53.0 | 32.6 | 95 | 51 | 30.0 | 10 | 0.88 | 0.88 | Y |
| Chen et al., 2020 [33] | 257 | NA | 59.2 | 95 | 40 | 19.0 | NA | 0.84 | NA | NA |
| Noh et al., 2020 [34] | 300 | 28.3 | 34.0 | 95 | 52 | 30.1 | 10 | 0.86 | 10 | NA |
| Sakaguchi et al., 2021 [35] | 773 | 0 | 44.3 | 95 | 73 | 43.0 | 15 | 0.86 | 5 | NA |
| Kinnaird et al., 2022 [17] | 1885 | 62.0 | 40.0 | 95 | 32 | 21.2 | NA | 0.84 | NA | NA |
| Morote et al. 2022 [16] | 1486 | 26.1 | 36.9 | 95 | 56 | 40.0 | 15 | 0.90 | 12 | Y |
| AUROC for csPCa | |||
|---|---|---|---|
| Authors, Year [Ref.] | MRI Setting Alone | Clinical Predictors Predictive Model | MRI-Based Predictive Model |
| Fang et al., 2016 [21] | NA | BN: 0.85 PNPB: NA Both status: NA | BN: 0.872 PNPB: NA Both status: NA |
| Kim et al., 2016 [22] | NA | BN: 0.60 PNPB: 0.63 Both status: 0.60 | BN: 0.72 PNPB: 0.61 Both status: 0.69 |
| Bjurlin et al., 2017 [23] | NA | NA | BN: 0.84 PNPB: 0.87 Both status: NA |
| Lee et al., 2017 [24] | NA | NA | BN: NA PNPB: NA Both status: 0.92 |
| Niu et al., 2017 [25] | BN: 0.76 PNPB: NA Both status: NA | NA | BN: 0.85 PNPB: NA Both status: NA |
| Radtke et al., 2017 [26] | BN: 0.76 PNPB: 0.78 Both status: NA | BN: 0.81 PNPB: 0.66 Both status: NA | BN: 0.83 PNPB: 0.81 Both status: NA |
| Truong et al., 2017 [27] | NA | NA | NA |
| van Leeuwen et al., 2017 [28] | NA | BN: NA PNPB: NA Both status: 0.797 | BN: NA PNPB: NA Both status: 0.897 |
| Alberts et al., 2018 [29] | NA | BN: 0.76 PNPB: 0.74 Both status: NA | BN: 0.84 PNPB: 0.85 Both status: NA |
| Huang et al., 2018 [30] | NA | NA | BN: NA PNPB: 0.927 Both status: NA |
| Mehralivand et al., 2018 [31] | NA | BN: NA PNPB: NA Both status: 0.72 | BN: NA PNPB: NA Both status: 0.84 |
| Boesen et al., 2019 [32] | BN: 0.83 PNPB: NA Both status: NA | BN: 0.85 PNPB: NA Both status: NA | BN: 0.89 PNPB: NA Both status: NA |
| Borque et al., 2019 [15] | NA | NA | BN: NA PNPB: NA Both status: 0.856 |
| Chen et al., 2020 [33] | 0.869 | NA | 0.84 |
| Noh et al., 2020 [34] | BN: 0.801 PNPB: NA Both status: NA | BN: 0.795 PNPB: NA Both status: NA | BN: 0.861 PNPB: NA Both status: NA |
| Sakaguchi et al., 2021 [35] | BN: 0.822 PNPB: NA Both status: NA | NA | BN: 0.862 PNPB: NA Both status: NA |
| Kinnaird et al., 2022 [17] | BN: NA PNPB: NA Both status: 0.760 | BN: NA PNPB: NA Both status: 0.707 | BN: NA PNPB: NA Both status: 0.843 |
| Morote et al. 2022 [17] | BN: NA PNPB: NA Both status: 0.842 | NA | BN: NA PNPB: NA Both status: 0.987 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triquell, M.; Campistol, M.; Celma, A.; Regis, L.; Cuadras, M.; Planas, J.; Trilla, E.; Morote, J. Magnetic Resonance Imaging-Based Predictive Models for Clinically Significant Prostate Cancer: A Systematic Review. Cancers 2022, 14, 4747. https://doi.org/10.3390/cancers14194747
Triquell M, Campistol M, Celma A, Regis L, Cuadras M, Planas J, Trilla E, Morote J. Magnetic Resonance Imaging-Based Predictive Models for Clinically Significant Prostate Cancer: A Systematic Review. Cancers. 2022; 14(19):4747. https://doi.org/10.3390/cancers14194747
Chicago/Turabian StyleTriquell, Marina, Miriam Campistol, Ana Celma, Lucas Regis, Mercè Cuadras, Jacques Planas, Enrique Trilla, and Juan Morote. 2022. "Magnetic Resonance Imaging-Based Predictive Models for Clinically Significant Prostate Cancer: A Systematic Review" Cancers 14, no. 19: 4747. https://doi.org/10.3390/cancers14194747
APA StyleTriquell, M., Campistol, M., Celma, A., Regis, L., Cuadras, M., Planas, J., Trilla, E., & Morote, J. (2022). Magnetic Resonance Imaging-Based Predictive Models for Clinically Significant Prostate Cancer: A Systematic Review. Cancers, 14(19), 4747. https://doi.org/10.3390/cancers14194747