
Are Wellness Visits a Possible and Effective Cure for the Increasing Cancer Burden in Poland? Example of Women’s Preventive Services in the U.S.

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
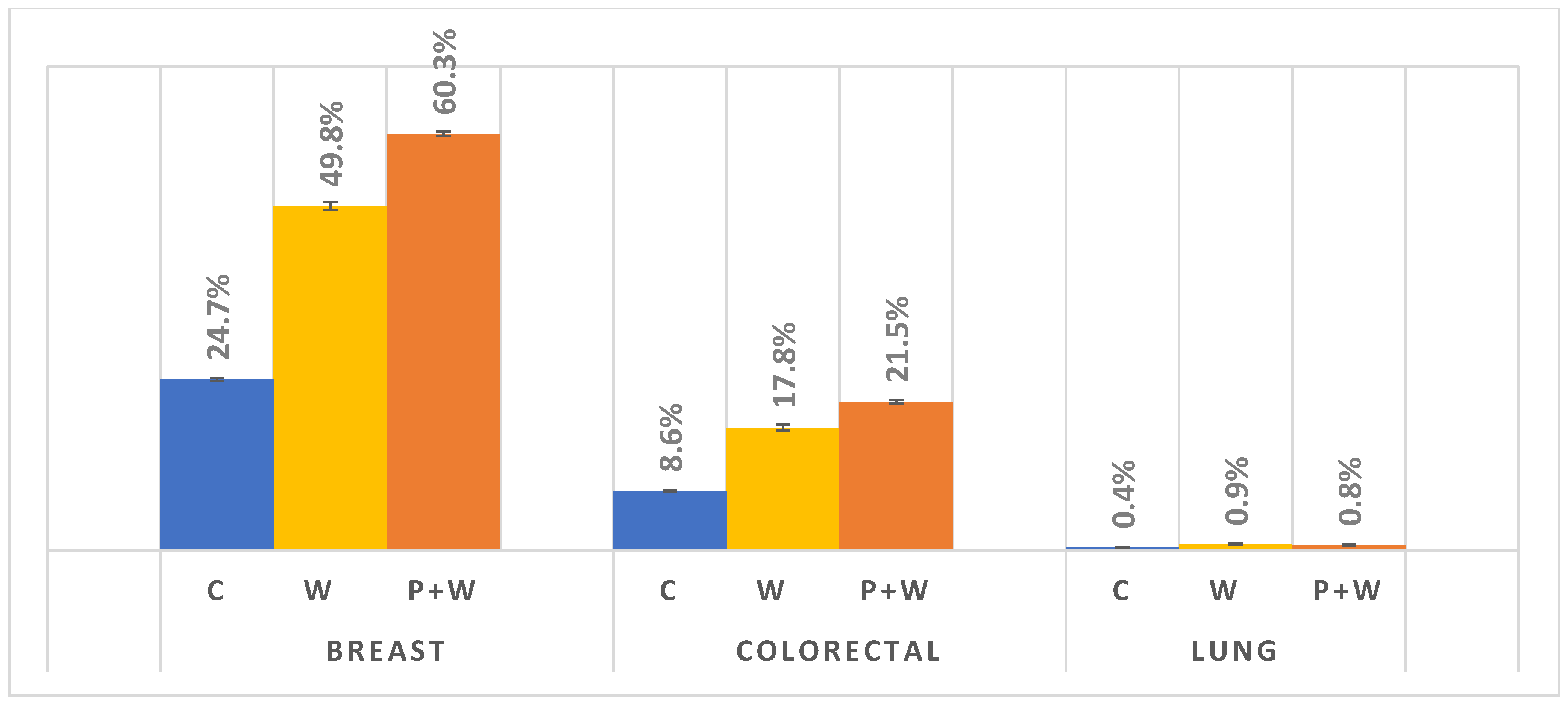
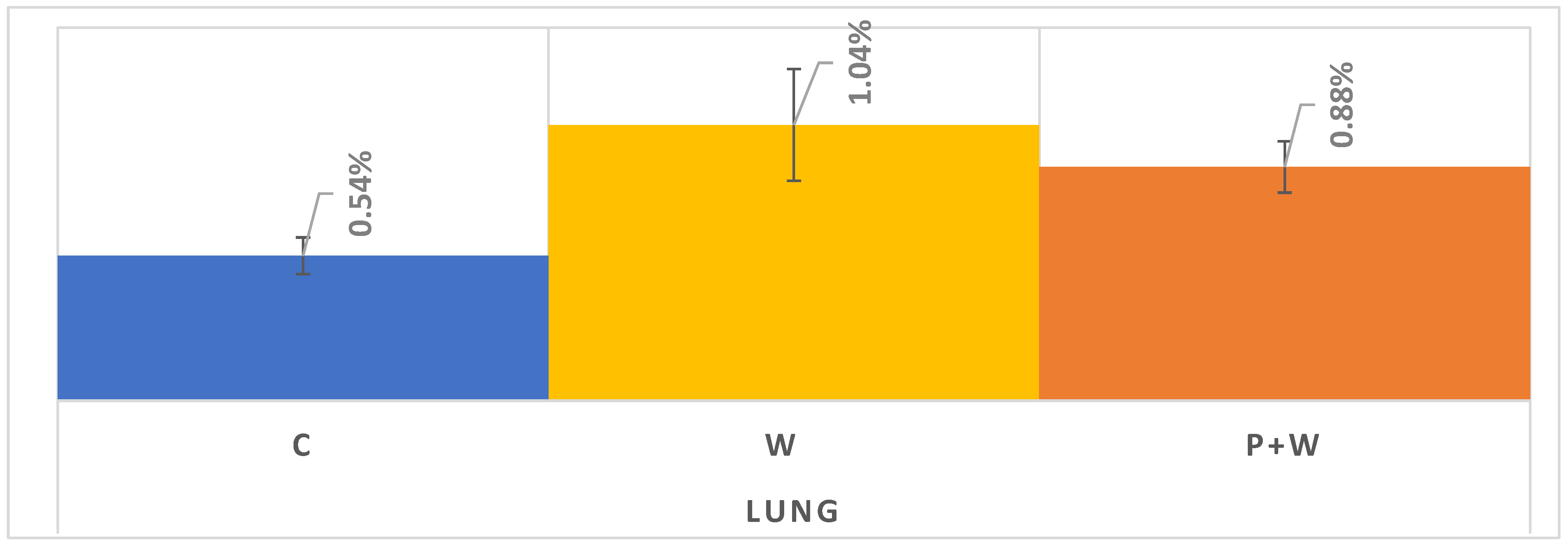
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
The Patient Protection and Affordable Care Act: PUBLIC LAW 111–148
- A
- A health risk assessment completed prior to or as part of the visit
- A.
- Establishment of (or update to) the individual’s medical and family history
- B.
- [Reviewing] A list of current providers and suppliers that are regularly involved in providing medical care to the individual (including a list of all prescribed medications)
- C.
- A measurement of height, weight, body mass index (or waist circumference, if appropriate), blood pressure, and other routine measurements
- D.
- Detection of any cognitive impairment
- E.
- The establishment of, or an update to, the following:
- i.
- A screening schedule for the next 5 to 10 years, as appropriate, based on recommendations of the United States Preventive Services Task Force and the Advisory Committee on Immunization Practices, and the individual’s health status, screening history, and age-appropriate preventive services covered under this title.
- ii.
- A list of risk factors and conditions for which primary, secondary, or tertiary prevention interventions are recommended or are underway, including any mental health conditions or any such risk factors or conditions that have been identified through an initial preventive physical examination (as described under subsection (ww)(1)), and a list of treatment options and their associated risks and benefits.
- F.
- The furnishing of personalized health advice and a referral, as appropriate, to health education or preventive counseling services or programs aimed at reducing identified risk factors and improving self-management, or community-based lifestyle interventions to reduce health risks and promote self-management and wellness, including weight loss, physical activity, smoking cessation, fall prevention, and nutrition.
Appendix B
Other Preventive Visits:
|
Other Wellness Visits:
|
Vaccinations:
|
Screening Events:
|
HCPCS Codes to Identify Screening and Preventive Services
- The source for “Other Preventive Visits” codes was the AMA CPT 2016 Manual.
- Primary source for vaccinations was the CDC Immunization Information Systems (IIS): (https://www2a.cdc.gov/vaccines/iis/iisstandards/vaccines.asp), accessed on 11 April 2022.
- Primary source for other screening events was the Medicare Learning Network Preventive Services Chart: (https://www.cms.gov/Medicare/Prevention/PrevntionGenInfo/medicare-preventive-services/MPS-QuickReferenceChart-1.html), accessed on 11 April 2022.
- CRC screening codes were supplemented with additional codes from KP Hedis Insight (https://provider.ghc.org/open/providerCommunications/hedisInsight/index.jhtml), accessed on 11 April 2022.
- Breast cancer screening codes were supplemented with internal expert review, accessed on 11 April 2022.
References
- Didkowska, J.; Wojciechowska, U.; Olasek, P.; Caetano dos Santos, F.; Michałek, I. Cancer in Poland in 2019; National Cancer Registry: Warsaw, Poland, 2021; ISSN1 0867-8251. Available online: http://onkologia.org.pl/wp-content/uploads/Nowotwory_2019.pdf (accessed on 20 February 2022)ISSN2 0867-8251.
- Koczkodaj, P.; Didkowska, J. Tobacco attributable Disability-Adjusted Life Years (DALYs) burden in Poland and Hungary: The role of women. Tob. Induc. Dis. 2021, 19, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Sulkowska, U.; Michałek, I.M.; Didkowska, J.; Koczkodaj, P. Lung cancer and breast cancer mortality trends among 45–74-year-old European women. Nowotw. J. Oncol. 2021, 71, 185–196. [Google Scholar] [CrossRef]
- Eurostat, Smoking Prevalence by Sex (Source: DG SANTE). Available online: https://ec.europa.eu/eurostat/databrowser/view/sdg_03_30/default/table?lang=en (accessed on 20 February 2022).
- Chief Sanitary Inspectorate, Report from a Nationwide Survey on Attitudes Towards Tobacco Smoking. 2019. Available online: https://gis.gov.pl/wp-content/uploads/2018/04/Postawy-Polak%C3%B3w-do-palenia-tytoniu_Raport-Kantar-Public-dla-GIS_2019.pdf (accessed on 21 February 2022).
- OECD. State of Health in the EU Poland Country Health Profile 2019. Available online: https://ec.europa.eu/health/sites/default/files/state/docs/2019_chp_poland_english.pdf (accessed on 23 February 2022).
- Koczkodaj, P.; Sulkowska, U.; Mańczuk, M.; Cedzynska, M.; Przepiórka, I.; Ciuba, A.; Przewoźniak, K.; Didkowska, J. Estimated cancer burden attributable to the alcohol consumption in Poland in 2016. Nowotw. J. Oncol. 2019, 69, 179–181. [Google Scholar] [CrossRef]
- The State Agency for the Prevention of Alcohol-Related Problems in Poland (PARPA). Research and Statistical Information, Statistics. Available online: http://www.parpa.pl/index.php/badania-i-informacje-statystyczne/statystyki (accessed on 23 February 2022).
- Drygas, W.; Gajewska, M.; Zdrojewski, T. Insufficient Level of Physical Activity in Poland as a Threat and a Challenge to Public Health. Report of the Public Health Committee of the Polish Academy of Sciences; National Institute of Public Health—National Institute of Hygiene: Warsaw, Poland, 2021; ISBN 978-83-65870-35-3. [Google Scholar]
- Eurostat. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Overweight_and_obesity_-_BMI_statistics#Obesity_in_the_EU:_gender_differences (accessed on 24 February 2022).
- National Health Fund in Poland, Data on Cancer Screenings Performance (1 February 2022). Available online: https://www.nfz.gov.pl/dla-pacjenta/programy-profilaktyczne/dane-o-realizacji-programow/ (accessed on 21 February 2022).
- Koczkodaj, P.; Kamiński, M.; Ciuba, A.; Didkowska, J. Cancer screening coverage in Poland—From bad to better to the worst during the SARS-CoV-2 pandemic. Arch. Med. Sci. 2021, 17, 1132–1133. [Google Scholar] [CrossRef] [PubMed]
- The Patient Protection and Affordable Care Act: Public Law. 111–148. pp. 435–436. Available online: https://www.govinfo.gov/content/pkg/PLAW-111publ148/pdf/PLAW-111publ148.pdf (accessed on 3 March 2022).
- Manchikanti, L.; Ii, S.H.; Benyamin, R.M.; Hirsch, J.A. Evolution of US Health Care Reform. Pain Physician 2017, 20, 107–110. [Google Scholar] [CrossRef]
- Camacho, F.; Yao, N.A.; Anderson, R. The Effectiveness of Medicare Wellness Visits in Accessing Preventive Screening. J. Prim. Care Community Health 2017, 8, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Lechowski, Ł.; Jasion, A. Spatial Accessibility of Primary Health Care in Rural Areas in Poland. Int. J. Environ. Res. Public Health 2021, 18, 9282. [Google Scholar] [CrossRef] [PubMed]
- Yao, N.; Alcalá, H.E.; Anderson, R.; Balkrishnan, R. Cancer Disparities in Rural Appalachia: Incidence, Early Detection, and Survivorship. J. Rural Health 2016, 33, 375–381. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2019, 396, 1223–1249. [Google Scholar] [CrossRef]
- Sahar, L.; Msc, V.L.D.W.; Bsc, K.K.L.; Fedewa, S.A.; Rosenthal, L.; Kazerooni, E.A.; Dyer, D.S.; Smith, R.A. Geographic access to lung cancer screening among eligible adults living in rural and urban environments in the United States. Cancer 2022, 128, 1584–1594. [Google Scholar] [CrossRef] [PubMed]
- Appalachian Regional Commission. County Economic Status and Distressed Areas in Appalachia. Available online: https://www.arc.gov/appalachian_region/CountyEconomicStatusandDistressedAreasinAppalachia.asp (accessed on 23 March 2022).
- Centers for Disease Control and Prevention. NCHS Urban-Rural Classification Scheme for Counties. Available online: https://www.cdc.gov/nchs/data_access/urban_rural.htm (accessed on 23 March 2022).
- National Cancer Institute. NCI Comorbidity Index Overview. Available online: https://healthcaredelivery.cancer.gov/seermedicare/considerations/comorbidity.html (accessed on 23 March 2022).
- Galvin, S.L.; Grandy, R.; Woodall, T.; Parlier, A.B.; Thach, S.; Landis, S.E. Improved Utilization of Preventive Services Among Patients Following Team-Based Annual Wellness Visits. North Carol. Med. J. 2017, 78, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.T.; Webel, B.K.; Donahue, E.E.; Richards, A.; Sabo, R.T.; Brooks, E.M.; Kashiri, P.L.; Huffstetler, A.N.; Santana, S.; Harris, L.M.; et al. Understanding the Value of the Wellness Visit: A Descriptive Study. Am. J. Prev. Med. 2021, 61, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health in Poland, Prophylaxis 40 Plus (Profilaktyka 40 Plus). Available online: https://www.gov.pl/web/zdrowie/profilaktyka-40-plus (accessed on 30 March 2022).
- Ganguli, I.; Souza, J.; McWilliams, J.M.; Mehrotra, A. Trends in Use of the US Medicare Annual Wellness Visit, 2011–2014. JAMA 2017, 317, 2233–2235. [Google Scholar] [CrossRef] [PubMed]
- The Seym of the Republic of Poland, Answer of the Minister of Health to a Parliamentary Question, 6 March 2019. Available online: https://orka2.sejm.gov.pl/INT8.nsf/klucz/ATTBAUCXZ/%24FILE/i29778-o1.pdf (accessed on 30 March 2022).
- Chien, S.-Y.; Chuang, M.-C.; Chen, I.-P.; Yu, P.H. Primary Drivers of Willingness to Continue to Participate in Community-Based Health Screening for Chronic Diseases. Int. J. Environ. Res. Public Health 2019, 16, 1645. [Google Scholar] [CrossRef] [PubMed]
- Economic Research Service. U.S. Department of Agriculture. Employment & Education. Available online: https://www.ers.usda.gov/topics/rural-economy-population/employment-education/rural-education/ (accessed on 30 March 2022).
- Ombudsman for Patients’ Rights Statements. Available online: https://www.gov.pl/web/rpp/przedmiot-wiedza-o-zdrowiu---wystapienie-rzecznika-praw-pacjenta-do-ministra-zdrowia-i-ministra-edukacji (accessed on 30 March 2022).
- Unanue-Arza, S.; Solís-Ibinagagoitia, M.; Díaz-Seoane, M.; Mosquera-Metcalfe, I.; Idigoras, I.; Bilbao, I.; Portillo, I. Inequalities and risk factors related to non-participation in colorectal cancer screening programmes: A systematic review. Eur. J. Public Health 2020, 31, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Force, U.P.S.T.; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; et al. Screening for Lung Cancer. JAMA 2021, 325, 962–970. [Google Scholar] [CrossRef]
- Rzyman, W.; Szurowska, E.; Adamek, M. Implementation of lung cancer screening at the national level: Polish example. Transl. Lung Cancer Res. 2019, 8 (Suppl. 1), S95–S105. [Google Scholar] [CrossRef] [PubMed]
- Rzyman, W.; Didkowska, J.; Dziedzic, R.; Grodzki, T.; Orłowski, T.; Szurowska, E.; Langfort, R.; Biernat, W.; Kowalski, D.; Dyszkiewicz, W.; et al. Consensus Statement on a Screening Programme for the Detection of Early Lung Cancer in Poland. Adv. Respir. Med. 2018, 86, 53–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Number of Beneficiaries in the Years 2014–2018: 2,869,072 | |||
|---|---|---|---|
| Beneficiaries with Wellness Visits (W): 788,779 | Beneficiaries without Wellness Visits: 2,080,293 | ||
| Characteristic of beneficiares | Number | Characteristic of beneficiaries | Number |
| Beneficiaries enrolled in FFS Medicare +/− 1 year from a candidate’s reference day | 532,201 | Beneficiaries enrolled in FFS Medicare +/− 1 year during time window 2016–2017 | 715,210 |
| Beneficiaries with no additional W during a reference time window 2016–2017 | 514,321 | Beneficiaries without 90 days lookback for related preventive services or screenings (P) before reference | 350,854 |
| Beneficiaries with reference days only after 1 January 2016 | 302,397 | ||
| Beneficiaries aged 65–79 at reference day | 229,792 | Beneficiaries aged 65–79 at reference day | 197,360 |
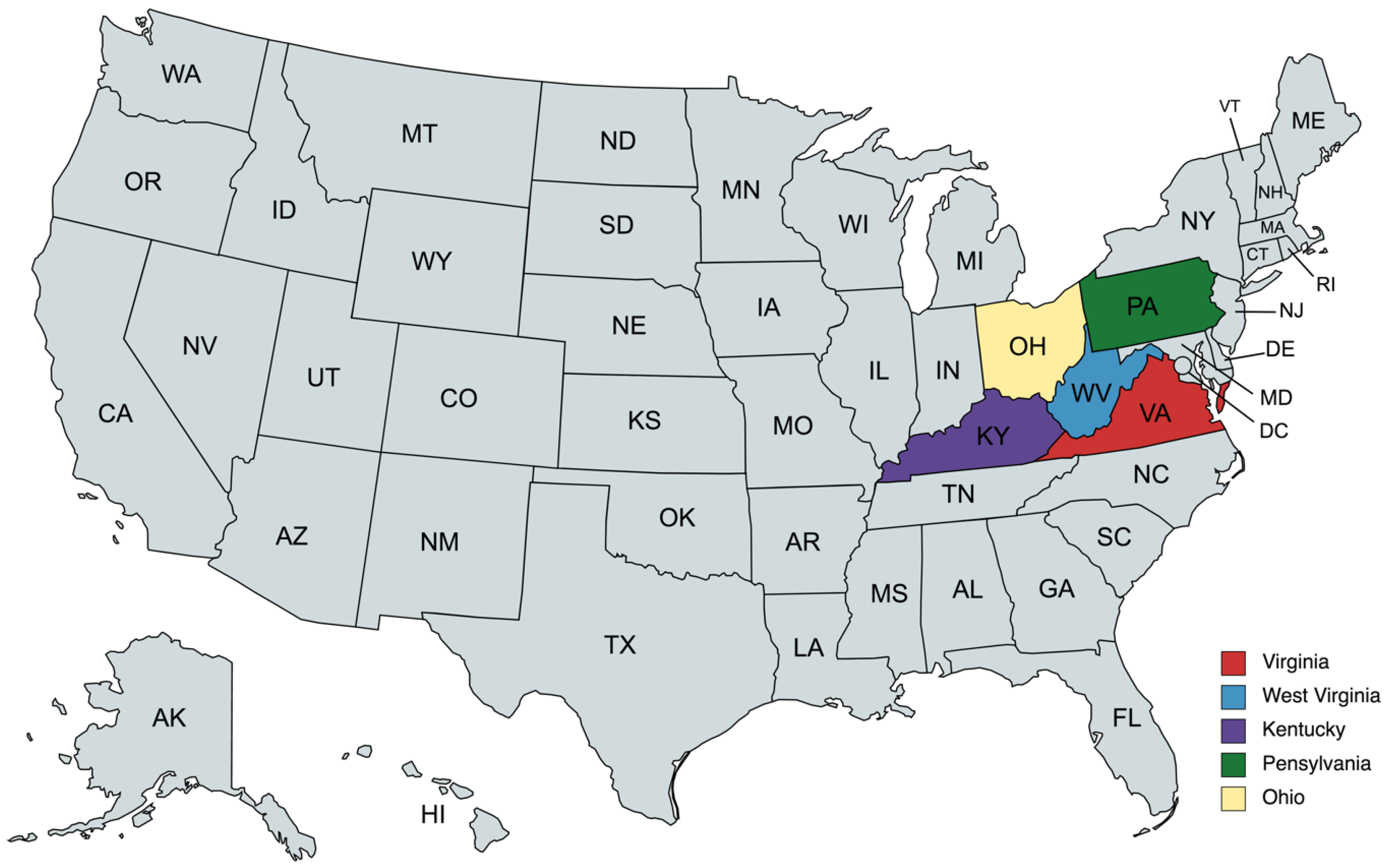
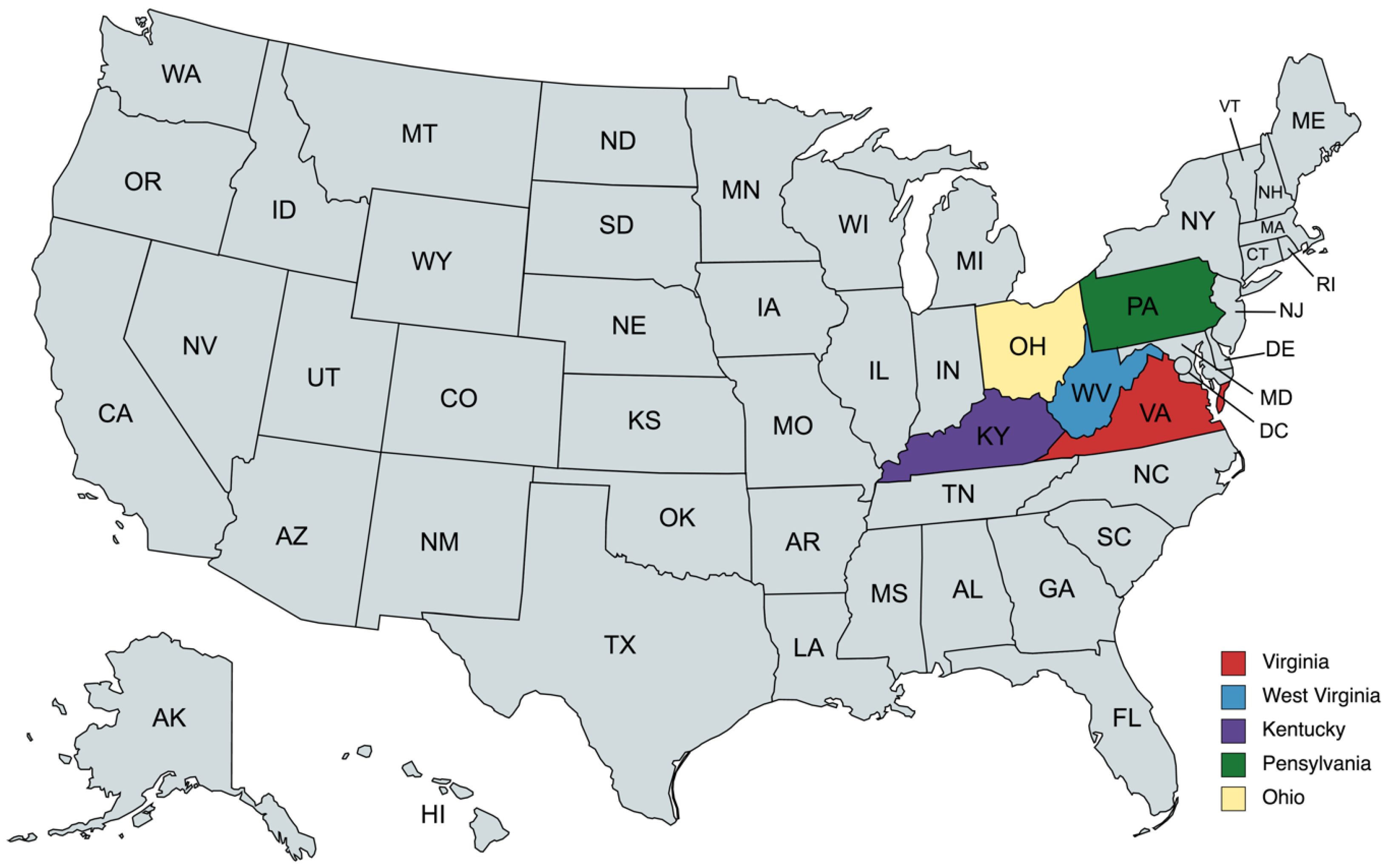
| Beneficiaries restricted to 5-states study region at reference | 185,176 | ||
| ↓FINAL SAMPLE↓ | |||
| W only | 35,847 | Control group (C) (after restricting beneficiaries to 5-state study region at reference) | 168,516 |
| Previous related preventive services or screenings (P) + W | 149,329 | ||
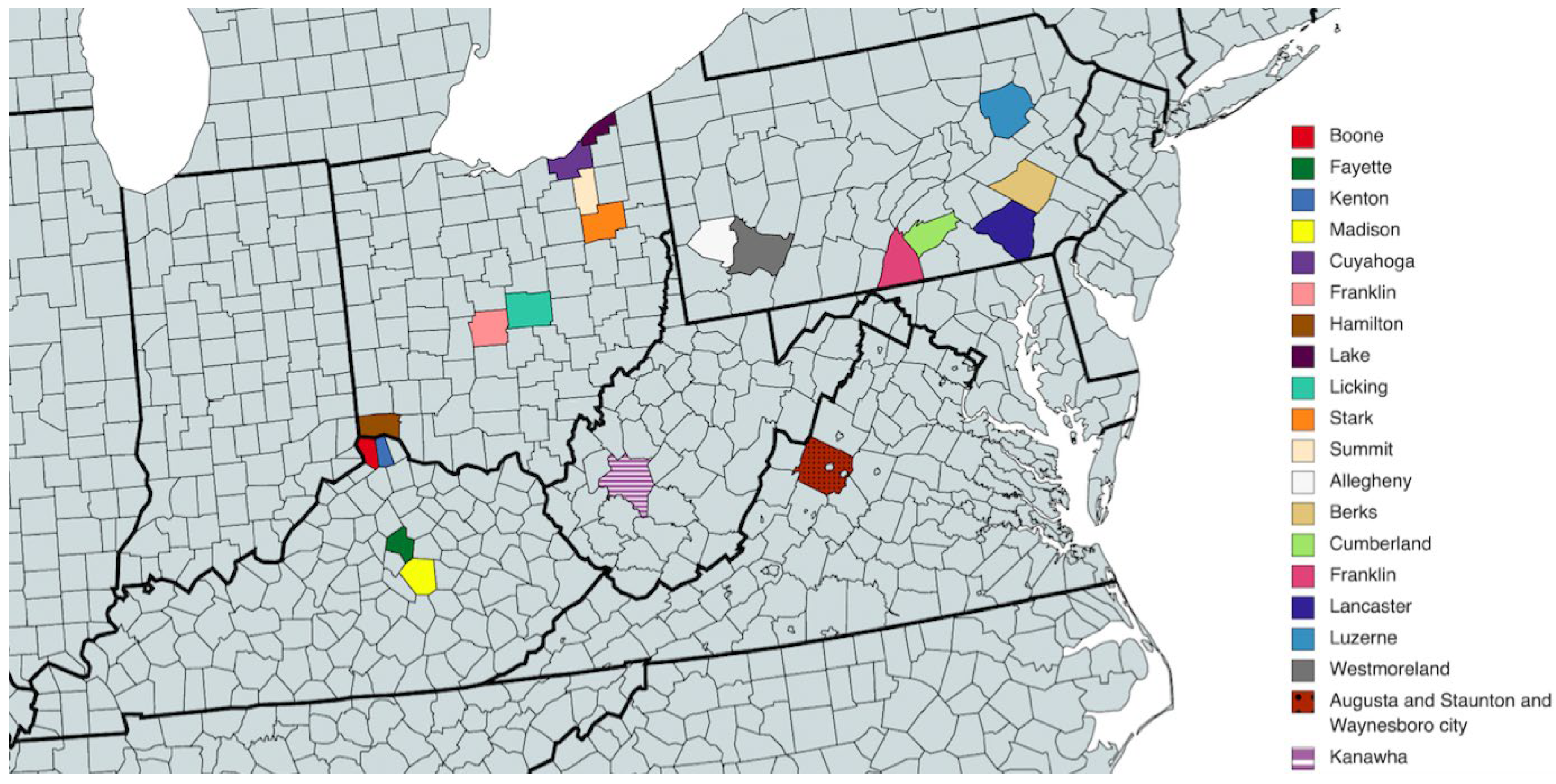
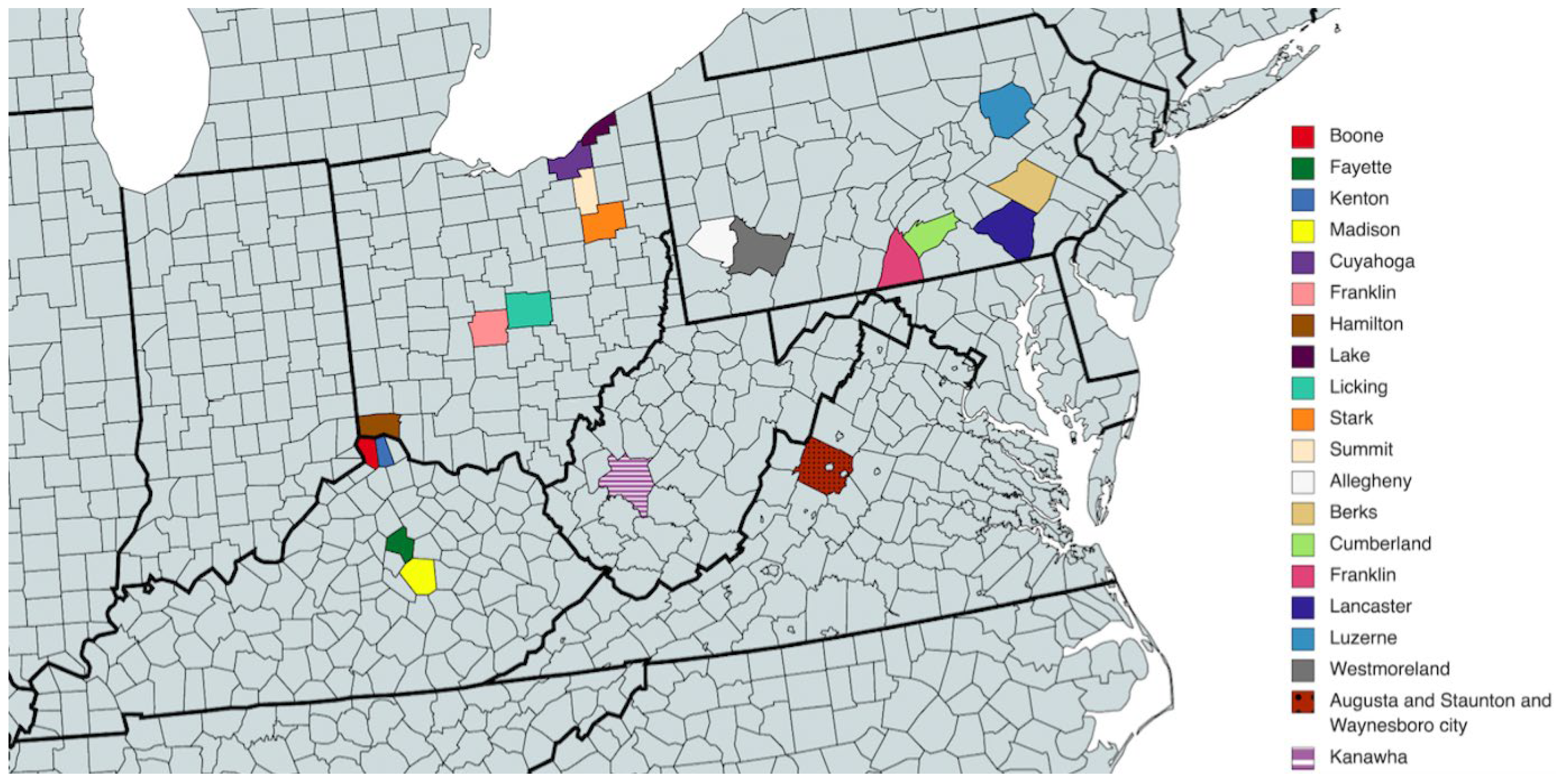
| LUNG CANCER SAMPLE (20 CHOSEN COUNTIES) | |||
| W only | 9467 | Control group (C) | 43,739 |
| Previous related preventive services or screenings (P) + W | 40,119 | ||
| Year | 2021 | 2022 | ||||||
|---|---|---|---|---|---|---|---|---|
| Month | Jul | Aug | Sept | Oct | Nov | Dec | Jan | Feb |
| Cytology (%) | 12.98 | 12.90 | 12.82 | 12.77 | 12.65 | 12.56 | 12.60 | 12.10 |
| Mammography (%) | 33.98 | 34.25 | 34.52 | 34.73 | 34.90 | 35.14 | 35.31 | 33.21 |
| Year | Number of Sent Invitations | % of Women Who Conducted Screening after Receiving an Invitation | ||
|---|---|---|---|---|
| Mammography | Cytology | Mammography | Cytology | |
| 2009 | 1,130,217 | 1,595,311 | 26.83 | 13.18 |
| 2010 | 2,419,462 | 3,202,921 | 26.59 | 11.73 |
| 2011 | 2,536,771 | 3,357,113 | 29.68 | 12.70 |
| 2012 | 2,690,028 | 3,413,678 | 26.07 | 9.68 |
| 2013 | 2,603,090 | 3,220,579 | 24.04 | 9.87 |
| 2014 | 2,749,920 | 3,348,593 | 21.42 | 9.20 |
| 2015 | 2,970,912 | 3,432,764 | 21.13 | 9.52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koczkodaj, P.; Camacho, F.; Batten, G.P.; Anderson, R.T. Are Wellness Visits a Possible and Effective Cure for the Increasing Cancer Burden in Poland? Example of Women’s Preventive Services in the U.S. Cancers 2022, 14, 4296. https://doi.org/10.3390/cancers14174296
Koczkodaj P, Camacho F, Batten GP, Anderson RT. Are Wellness Visits a Possible and Effective Cure for the Increasing Cancer Burden in Poland? Example of Women’s Preventive Services in the U.S. Cancers. 2022; 14(17):4296. https://doi.org/10.3390/cancers14174296
Chicago/Turabian StyleKoczkodaj, Paweł, Fabian Camacho, George P. Batten, and Roger T. Anderson. 2022. "Are Wellness Visits a Possible and Effective Cure for the Increasing Cancer Burden in Poland? Example of Women’s Preventive Services in the U.S." Cancers 14, no. 17: 4296. https://doi.org/10.3390/cancers14174296
APA StyleKoczkodaj, P., Camacho, F., Batten, G. P., & Anderson, R. T. (2022). Are Wellness Visits a Possible and Effective Cure for the Increasing Cancer Burden in Poland? Example of Women’s Preventive Services in the U.S. Cancers, 14(17), 4296. https://doi.org/10.3390/cancers14174296