
Multidimensional Diffusion Magnetic Resonance Imaging for Characterization of Tissue Microstructure in Breast Cancer Patients: A Prospective Pilot Study

 ,
,  , ,
, ,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MRI Examination Protocol
2.3. Image Assessment and Data Collection
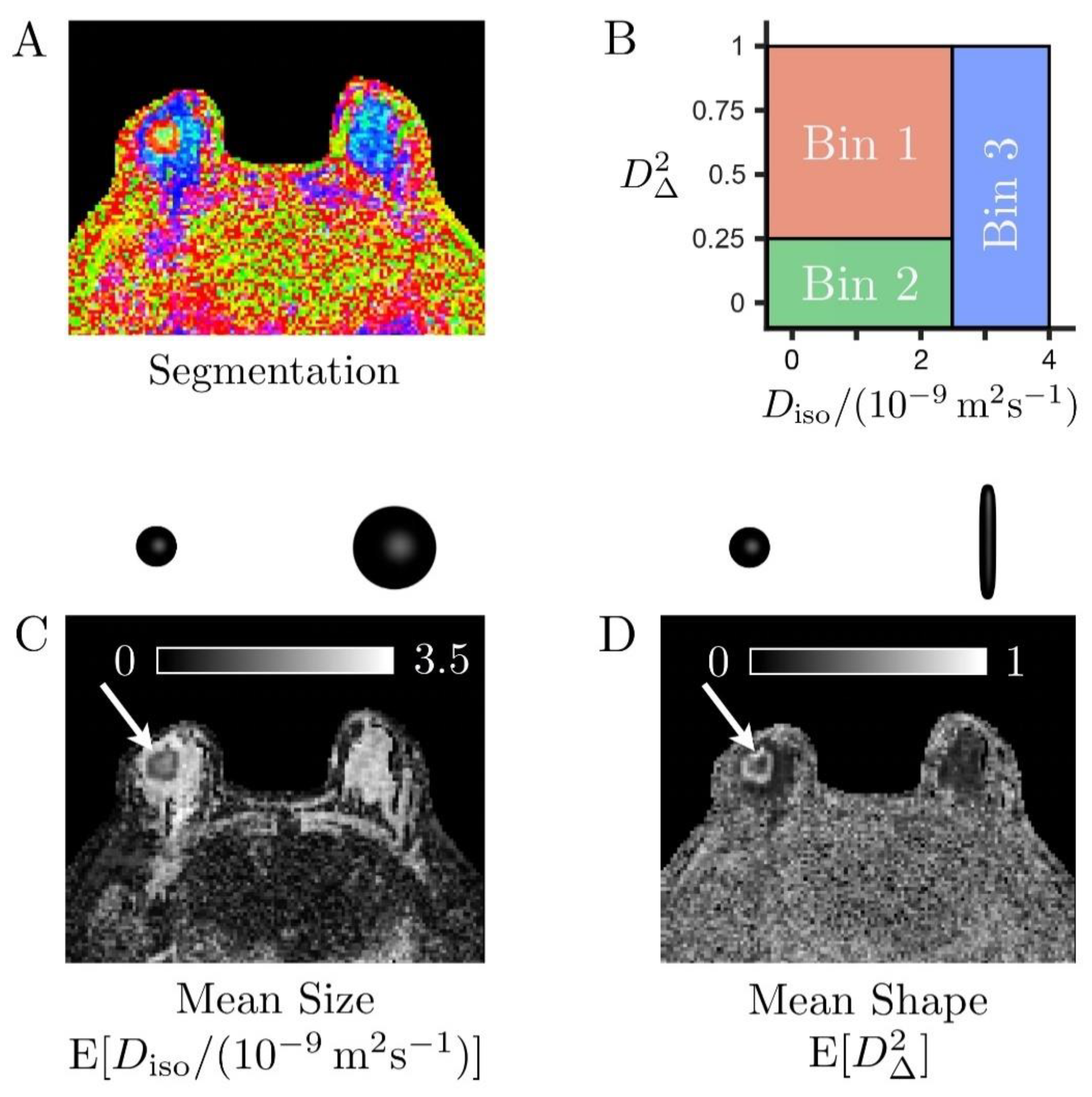
2.4. Diffusion Tensor Distributions (DTDs) and DTD-Derived Maps
- -
- Bin 1 within and
- -
- Bin 2 within and ,
- -
- Bin 3 within and
2.5. Quantitative Analysis of the Maps
2.6. Statistical Analysis
3. Results
3.1. Patient Cohort and Lesion Characteristics
3.2. Diffusion Tensor Distributions (DTDs) Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Partridge, S.C.; Nissan, N.; Rahbar, H.; Bs, A.E.K.; Sigmund, E.E. Diffusion-weighted breast MRI: Clinical applications and emerging techniques. J. Magn. Reson. Imaging 2017, 45, 337–355. [Google Scholar] [CrossRef]
- Basser, P.J. Inferring microstructural features and the physiological state of tissues from diffusion-weighted images. NMR Biomed. 1995, 8, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Basser, P.J.; Pierpaolib, C. Microstructural and Physiological Features of Tissues Elucidated by Quantitative-Diffusion-Tensor MRI. J. Magn. Reson. Ser. B 1996, 111, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, D. Apparent Diffusion Coefficient and Beyond: What Diffusion MR Imaging Can Tell Us about Tissue Structure. Radiology 2013, 268, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR imaging of intravoxel incoherent motions: Application to diffusion and perfusion in neurologic disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef]
- Bokacheva, L.; Kaplan, J.B.; Giri, D.D.; Patil, S.; Gnanasigamani, M.; Nyman, C.G.; Deasy, J.O.; Morris, E.A.; Thakur, S.B. Intravoxel incoherent motion diffusion-weighted MRI at 3.0 T differentiates malignant breast lesions from benign lesions and breast parenchyma. J. Magn. Reson. Imaging 2014, 40, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Cho, G.Y.; Gennaro, L.; Sutton, E.J.; Zabor, E.C.; Zhang, Z.; Giri, D.; Moy, L.; Sodickson, D.K.; Morris, E.A.; Sigmund, E.E.; et al. Intravoxel incoherent motion (IVIM) histogram biomarkers for prediction of neoadjuvant treatment response in breast cancer patients. Eur. J. Radiol. Open 2017, 4, 101–107. [Google Scholar] [CrossRef]
- Basser, P.; Mattiello, J.; LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef]
- Pierpaoli, C.; Jezzard, P.; Basser, P.J.; Barnett, A.; Chiro, G.D. Diffusion tensor MR imaging of the human brain. Radiology 1996, 201, 637–648. [Google Scholar] [CrossRef]
- Tournier, J.-D.; Mori, S.; Leemans, A. Diffusion tensor imaging and beyond. Magn. Reson. Med. 2011, 65, 1532–1556. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A.; Ramani, A.; Lu, H.; Kaczynski, K. Diffusional kurtosis imaging: The quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn. Reson. Med. 2005, 53, 1432–1440. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010, 23, 698–710. [Google Scholar] [CrossRef]
- Camps-Herrero, J. Diffusion-weighted imaging of the breast: Current status as an imaging biomarker and future role. BJR Open 2019, 1, 20180049. [Google Scholar] [CrossRef]
- Zhou, W.-P.; Zan, X.-Y.; Hu, X.-Y.; Liu, X.; Sudarshan, S.K.P.; Yang, S.-D.; Guo, Y.-J.; Fang, X.-M. Characterization of breast lesions using diffusion kurtosis model-based imaging: An initial experience. J. X-Ray Sci. Technol. 2020, 28, 157–169. [Google Scholar] [CrossRef]
- Partridge, S.C.; Ziadloo, A.; Murthy, R.; White, S.W.; Peacock, S.; Eby, P.R.; DeMartini, W.B.; Lehman, C.D. Diffusion tensor MRI: Preliminary anisotropy measures and mapping of breast tumors. J. Magn. Reson. Imaging 2010, 31, 339–347. [Google Scholar] [CrossRef]
- Wu, N.; Li, G.; Zhang, J.; Chang, S.; Hu, J.; Dai, Y. Characterization of Breast Tumors Using Diffusion Kurtosis Imaging (DKI). PLoS ONE 2014, 9, e113240. [Google Scholar] [CrossRef]
- Huang, Y.; Lin, Y.; Hu, W.; Ma, C.; Lin, W.; Wang, Z.; Liang, J.; Ye, W.; Zhao, J.; Wu, R. Diffusion Kurtosis at 3.0T as an In Vivo Imaging Marker for Breast Cancer Characterization: Correlation with Prognostic Factors. J. Magn. Reson. Imaging 2019, 49, 845–856. [Google Scholar] [CrossRef]
- Xu, J.; Jiang, X.; Li, H.; Arlinghaus, L.R.; McKinley, E.T.; Devan, S.P.; Hardy, B.M.; Xie, J.; Kang, H.; Chakravarthy, A.B.; et al. Magnetic resonance imaging of mean cell size in human breast tumors. Magn. Reson. Med. 2020, 83, 2002–2014. [Google Scholar] [CrossRef]
- Xu, J.; Jiang, X.; Devan, S.P.; Arlinghaus, L.R.; McKinley, E.T.; Xie, J.; Zu, Z.; Wang, Q.; Chakravarthy, A.B.; Wang, Y.; et al. MRI-cytometry: Mapping nonparametric cell size distributions using diffusion MRI. Magn. Reson. Med. 2021, 85, 748–761. [Google Scholar] [CrossRef]
- Lasič, S.; Szczepankiewicz, F.; Eriksson, S.; Nilsson, M.; Topgaard, D. Microanisotropy imaging: Quantification of microscopic diffusion anisotropy and orientational order parameter by diffusion MRI with magic-angle spinning of the q-vector. Front. Phys. 2014, 2, 2. [Google Scholar] [CrossRef]
- Topgaard, D. Multidimensional diffusion MRI. J. Magn. Reson. 2017, 275, 98–113. [Google Scholar] [CrossRef]
- Westin, C.-F.; Knutsson, H.; Pasternak, O.; Szczepankiewicz, F.; Özarslan, E.; van Westen, D.; Mattisson, C.; Bogren, M.; O’Donnell, L.J.; Kubicki, M.; et al. Q-space trajectory imaging for multidimensional diffusion MRI of the human brain. NeuroImage 2016, 135, 345–362. [Google Scholar] [CrossRef]
- Andrew, E.R.; Bradbury, A.W.; Eades, R.G. Removal of Dipolar Broadening of Nuclear Magnetic Resonance Spectra of Solids by Specimen Rotation. Nature 1959, 183, 1802–1803. [Google Scholar] [CrossRef]
- Schmidt-Rohr, K.; Spiess, H.W. Multidimensional Solid-State NMR and Polymers; Academic Press: London, UK, 1994. [Google Scholar]
- Eriksson, S.; Lasič, S.; Nilsson, M.; Westin, C.-F.; Topgaard, D. NMR diffusion-encoding with axial symmetry and variable anisotropy: Distinguishing between prolate and oblate microscopic diffusion tensors with unknown orientation distribution. J. Chem. Phys. 2015, 142, 104201. [Google Scholar] [CrossRef] [PubMed]
- Szczepankiewicz, F.; Westin, C.-F.; Nilsson, M. Gradient waveform design for tensor-valued encoding in diffusion MRI. J. Neurosci. Methods 2021, 348, 109007. [Google Scholar] [CrossRef]
- Topgaard, D. Advanced Diffusion Encoding Methods in MRI; Royal Society of Chemistry: Croydon, UK, 2020. [Google Scholar]
- Ning, L.; Szczepankiewicz, F.; Nilsson, M.; Rathi, Y.; Westin, C.-F. Probing tissue microstructure by diffusion skewness tensor imaging. Sci. Rep. 2021, 11, 135. [Google Scholar] [CrossRef]
- Szczepankiewicz, F.; Sjölund, J.; Ståhlberg, F.; Lätt, J.; Nilsson, M. Tensor-valued diffusion encoding for diffusional variance decomposition (DIVIDE): Technical feasibility in clinical MRI systems. PLoS ONE 2019, 14, e0214238. [Google Scholar] [CrossRef] [PubMed]
- Szczepankiewicz, F.; Lasič, S.; van Westen, D.; Sundgren, P.C.; Englund, E.; Westin, C.-F.; Ståhlberg, F.; Lätt, J.; Topgaard, D.; Nilsson, M. Quantification of microscopic diffusion anisotropy disentangles effects of orientation dispersion from microstructure: Applications in healthy volunteers and in brain tumors. NeuroImage 2015, 104, 241–252. [Google Scholar] [CrossRef]
- Szczepankiewicz, F.; van Westen, D.; Englund, E.; Westin, C.-F.; Ståhlberg, F.; Lätt, J.; Sundgren, P.C.; Nilsson, M. The link between diffusion MRI and tumor heterogeneity: Mapping cell eccentricity and density by diffusional variance decomposition (DIVIDE). NeuroImage 2016, 142, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Szczepankiewicz, F.; Brabec, J.; Taylor, M.; Westin, C.; Golby, A.; Van Westen, D.; Sundgren, P.C. Tensor-valued diffusion MRI in under 3 minutes: An initial survey of microscopic anisotropy and tissue heterogeneity in intracranial tumors. Magn. Reson. Med. 2020, 83, 608–620. [Google Scholar] [CrossRef]
- Lampinen, B.; Zampeli, A.; Björkman-Burtscher, I.M.; Szczepankiewicz, F.; Källén, K.; Strandberg, M.C.; Nilsson, M. Tensor-valued diffusion MRI differentiates cortex and white matter in malformations of cortical development associated with epilepsy. Epilepsia 2020, 61, 1701–1713. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.W.; Lasič, S.; Lundell, H.; Nilsson, M.; Topgaard, D.; Sellebjerg, F.; Szczepankiewicz, F.; Siebner, H.R.; Blinkenberg, M.; Dyrby, T.B. Disentangling white-matter damage from physiological fibre orientation dispersion in multiple sclerosis. Brain Commun. 2020, 2, 2. [Google Scholar] [CrossRef]
- Kamiya, K.; Kamagata, K.; Ogaki, K.; Hatano, T.; Ogawa, T.; Takeshige-Amano, H.; Murata, S.; Andica, C.; Murata, K.; Feiweier, T.; et al. Brain White-Matter Degeneration Due to Aging and Parkinson Disease as Revealed by Double Diffusion Encoding. Front. Neurosci. 2020, 14, 584510. [Google Scholar] [CrossRef]
- Topgaard, D. Diffusion tensor distribution imaging. NMR Biomed. 2019, 32, e4066. [Google Scholar] [CrossRef] [PubMed]
- Basser, P.J.; Pajevic, S. A normal distribution for tensor-valued random variables: Applications to diffusion tensor MRI. IEEE Trans. Med. Imaging 2003, 22, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Jian, B.; Vemuri, B.C.; Özarslan, E.; Carney, P.R.; Mareci, T.H. A novel tensor distribution model for the diffusion-weighted MR signal. NeuroImage 2007, 37, 164–176. [Google Scholar] [CrossRef] [PubMed]
- de Almeida Martins, J.P.; Tax, C.M.W.; Szczepankiewicz, F.; Jones, D.K.; Westin, C.-F.; Topgaard, D. Transferring principles of solid-state and Laplace NMR to the field of in vivo brain MRI. Magn. Reson. 2020, 1, 27–43. [Google Scholar] [CrossRef]
- de Almeida Martins, J.P.; Topgaard, D. Multidimensional correlation of nuclear relaxation rates and diffusion tensors for model-free investigations of heterogeneous anisotropic porous materials. Sci. Rep. 2018, 8, 2488. [Google Scholar] [CrossRef]
- Reymbaut, A.; Critchley, J.; Durighel, G.; Sprenger, T.; Sughrue, M.; Bryskhe, K.; Topgaard, D. Toward nonparametric diffusion-characterization of crossing fibers in the human brain. Magn. Reson. Med. 2021, 85, 2815–2827. [Google Scholar] [CrossRef] [PubMed]
- Breast Imaging Reporting and Data System, 5th ed.; ACR BI-RADS® Atlas; American College of Radiology: Reston, VA, USA, 2013; Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads (accessed on 30 March 2021).
- Elston, C.; Ellis, I. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Conturo, T.E.; McKinstry, R.C.; Akbudak, E.; Robinson, B.H. Encoding of anisotropic diffusion with tetrahedral gradients: A general mathematical diffusion formalism and experimental results. Magn. Reson. Med. 1996, 35, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Reymbaut, A.; Mezzani, P.; de Almeida Martins, J.P.; Topgaard, D. Accuracy and precision of statistical descriptors obtained from multidimensional diffusion signal inversion algorithms. NMR Biomed. 2020, 33, e4267. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.L.; Hanson, R.J. Solving Least Squares Problems; Prentice-Hall: Englewood Cliffs, NJ, USA, 1974. [Google Scholar]
- Efron, B. Bootstrap Methods: Another Look at the Jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- De Kort, D.W.; Van Duynhoven, J.P.M.; Hoeben, F.J.M.; Janssen, H.M.; Van As, H. NMR Nanoparticle Diffusometry in Hydrogels: Enhancing Sensitivity and Selectivity. Anal. Chem. 2014, 86, 9229–9235. [Google Scholar] [CrossRef]
- Pas, K.; Komlosh, M.E.; Perl, D.P.; Basser, P.J.; Benjamini, D. Retaining information from multidimensional correlation MRI using a spectral regions of interest generator. Sci. Rep. 2020, 10, 3246. [Google Scholar] [CrossRef]
- Slator, P.J.; Hutter, J.; Marinescu, R.V.; Palombo, M.; Young, A.L.; Jackson, L.H.; Ho, A.; Chappell, L.C.; Rutherford, M.; Hajnal, J.V.; et al. InSpect: INtegrated SPECTral Component Estimation and Mapping for Multi-contrast Microstructural MRI. In Information Processing in Medical Imaging. IPMI 2019; Chung, A., Gee, J., Yushkevich, P., Bao, S., Eds.; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; Volume 11492, pp. 755–766. [Google Scholar]
- Nilsson, M.; Szczepankiewicz, F.; Van Westen, D.; Hansson, O. Extrapolation-Based References Improve Motion and Eddy-Current Correction of High B-Value DWI Data: Application in Parkinson’s Disease Dementia. PLoS ONE 2015, 10, e0141825. [Google Scholar] [CrossRef]
- Baltzer, P.; Mann, R.M.; Iima, M.; Sigmund, E.E.; Clauser, P.; Gilbert, F.J.; Martincich, L.; Partridge, S.C.; Patterson, A.; Pinker, K.; et al. Diffusion-weighted imaging of the breast—A consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur. Radiol. 2020, 30, 1436–1450. [Google Scholar] [CrossRef] [PubMed]
- Jiang, R.; Ma, Z.; Dong, H.; Sun, S.; Zeng, X.; Li, X. Diffusion tensor imaging of breast lesions: Evaluation of apparent diffusion coefficient and fractional anisotropy and tissue cellularity. Br. J. Radiol. 2016, 89, 20160076. [Google Scholar] [CrossRef]
- Çakır, Ö.; Arslan, A.; Inan, N.; Anik, Y.; Sarisoy, T.; Gümüştaş, S.; Akansel, G. Comparison of the diagnostic performances of diffusion parameters in diffusion weighted imaging and diffusion tensor imaging of breast lesions. Eur. J. Radiol. 2013, 82, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Nissan, N.; Furman-Haran, E.; Feinberg-Shapiro, M.; Grobgeld, D.; Eyal, E.; Zehavi, T.; Degani, H. Tracking the Mammary Architectural Features and Detecting Breast Cancer with Magnetic Resonance Diffusion Tensor Imaging. J. Vis. Exp. 2014, e52048. [Google Scholar] [CrossRef]
- Plaza, M.J.; Morris, E.A.; Thakur, S.B. Diffusion tensor imaging in the normal breast: Influences of fibroglandular tissue composition and background parenchymal enhancement. Clin. Imaging 2016, 40, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Eyal, E.; Shapiro-Feinberg, M.; Furman-Haran, E.; Grobgeld, D.; Golan, T.; Itzchak, Y.; Catane, R.; Papa, M.; Degani, H. Parametric Diffusion Tensor Imaging of the Breast. Investig. Radiol. 2012, 47, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Li, Z.; Wu, Z.; Zheng, Y.; Zeng, S.; E, L.; Liang, J. Diagnostic Performance of Diffusion Tensor Imaging for Characterizing Breast Tumors: A Comprehensive Meta-Analysis. Front. Oncol. 2019, 9, 1229. [Google Scholar] [CrossRef]
- Tagliafico, A.; Rescinito, G.; Monetti, F.; Villa, A.; Chiesa, F.; Fisci, E.; Pace, D.; Calabrese, M. Diffusion tensor magnetic resonance imaging of the normal breast: Reproducibility of DTI-derived fractional anisotropy and apparent diffusion coefficient at 3.0 T. Radiol. Med. 2012, 117, 992–1003. [Google Scholar] [CrossRef]
- Mukherjee, P.; Berman, J.I.; Chung, S.W.; Hess, C.P.; Henry, R.G. Diffusion Tensor MR Imaging and Fiber Tractography: Theoretic Underpinnings. AJNR Am. J. Neuroradiol. 2008, 29, 632–641. [Google Scholar] [CrossRef]
- Soares, J.M.; Marques, P.; Alves, V.; Sousa, N. A hitchhiker’s guide to diffusion tensor imaging. Front. Neurosci. 2013, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Meyer, H.J.; Wienke, A. Can apparent diffusion coefficient (ADC) distinguish breast cancer from benign breast findings? A meta-analysis based on 13 847 lesions. BMC Cancer 2019, 19, 955. [Google Scholar] [CrossRef] [PubMed]
- Bickel, H.; Pinker, K.; Polanec, S.; Magometschnigg, H.; Wengert, G.; Spick, C.; Bogner, W.; Bago-Horvath, Z.; Helbich, T.H.; Baltzer, P. Diffusion-weighted imaging of breast lesions: Region-of-interest placement and different ADC parameters influence apparent diffusion coefficient values. Eur. Radiol. 2017, 27, 1883–1892. [Google Scholar] [CrossRef]
- Arponent, O.; Sudah, M.; Masarwah, A.; Taina, M.; Rautiainen, S.; Könönen, M.; Sironen, R.; Kosma, V.-M.; Sutela, A.; Hakumäki, J.; et al. Diffusion-Weighted Imaging in 3.0 Tesla Breast MRI: Diagnostic Performance and Tumor Characterization Using Small Subregions vs. Whole Tumor Regions of Interest. PLoS ONE 2015, 10, e0138702. [Google Scholar] [CrossRef]
- Luo, J.; Hippe, D.S.; Rahbar, H.; Parsian, S.; Rendi, M.H.; Partridge, S.C. Diffusion tensor imaging for characterizing tumor microstructure and improving diagnostic performance on breast MRI: A prospective observational study. Breast Cancer Res. 2019, 21, 102. [Google Scholar] [CrossRef]
- Lundell, H.; Nilsson, M.; Dyrby, T.B.; Parker, G.J.M.; Cristinacce, P.L.H.; Zhou, F.-L.; Topgaard, D.; Lasič, S. Multidimensional diffusion MRI with spectrally modulated gradients reveals unprecedented microstructural detail. Sci. Rep. 2019, 9, 9026. [Google Scholar] [CrossRef] [PubMed]
- O’Flynn, E.A.M.; Morgan, V.A.; Giles, S.L.; DeSouza, N.M. Diffusion weighted imaging of the normal breast: Reproducibility of apparent diffusion coefficient measurements and variation with menstrual cycle and menopausal status. Eur. Radiol. 2012, 22, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Ko, E.S.; Kim, R.B.; Han, B.-K.; Nam, S.J.; Shin, J.H.; Hahn, S.Y. Effect of menstrual cycle and menopausal status on apparent diffusion coefficient values and detectability of invasive ductal carcinoma on diffusion-weighted MRI. Breast Cancer Res. Treat. 2015, 149, 751–759. [Google Scholar] [CrossRef]
- Fanariotis, M.; Tsougos, I.; Vlychou, M.; Fezoulidis, I.; Vassiou, K. Contrast-enhanced and unenhanced diffusion-weighted imaging of the breast at 3 T. Clin. Radiol. 2018, 73, 928–935. [Google Scholar] [CrossRef]
- Janka, R.; Hammon, M.; Geppert, C.; Nothhelfer, A.; Uder, M.; Wenkel, E. Diffusion-Weighted MR Imaging of Benign and Malignant Breast Lesions Before and After Contrast Enhancement. RöFo 2014, 186, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.; Laio, A. Clustering by fast search and find of density peaks. Science 2014, 344, 1492–1496. [Google Scholar] [CrossRef] [PubMed]
- Reymbaut, A.; de Almeida Martins, J.P.; Tax, C.M.W.; Szczepankiewicz, F.; Jones, D.K.; Topgaard, D. Resolving orientation-specific diffusion-relaxation features via Monte-Carlo density-peak clustering in heterogeneous brain tissue. arXiv 2020, arXiv:2004.08626. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequences | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Series descriptor | 3D axial T2 | 3D axial T1 | 3D axial DISCO | 2D axial DWI | 2D axial MDD DWI |
| Sequence type | Fast-Spin Echo | Gradient-Echo VIBRANT | Gradient-Echo | Spin-Echo EPI | Spin-Echo EPI |
| Field of view (cm) | 34–38 | 34–38 | 34–38 | 34–38 | 34–38 |
| Slice thickness (mm) | 3 | 1.1 | 1.1 | 3.9 | 3.9 |
| Gap (mm) | 3 | 0 | 0 | 0 | 2.7 |
| Fat saturation | Yes | No | Yes | Yes | Yes |
| TE (ms) | Minimum | Minimum | Minimum | Minimum | 98 |
| TR (ms) | 2500–6000 | 4–4.5 | 4–4.5 | 2000–6000 | 2700–5000 |
| Matrix size (mm) | 512 × 512 | 512 × 512 | 512 × 512 | 256 × 256 | 128 × 128 |
| Flip angle | 111 | 10 | 12 | 90 | 90 |
| Direction | ALL | ALL | |||
| Number of directions | 3 | 43 | |||
| b-values (s/mm2) | 0, 800 | 100, 700, 1400, 2000 | |||
| Frequency direction | A/P | A/P | A/P | A/P | A/P |
| Scan time (min:sec) | 2:32 | 1:30 | 5–6 1 | 4:02 | 4:12 |
| Feature | Value |
|---|---|
| Patients (n = 16) | |
| Mean patient age in years (SD) | 51.1 (13.5) |
| Menopausal status | |
| Pre-menopausal | 8 (50%) |
| Post-menopausal | 8 (50%) |
| Breast type | |
| Almost entirely fatty | 1 (6.25%) |
| Scattered FGT | 3 (18.25%) |
| Heterogeneous FGT | 8 (50%) |
| Extreme FGT | 4 (25%) |
| Breast tumors (n = 16) | |
| Size in mm (SD) | 30 (17.5) |
| Lesion type on DCE-MRI | |
| Mass | 12 (75%) |
| NME | 2 (12.5%) |
| Mixed | 2 (12.5%) |
| Histopathology | |
| IDC | 8 (50%) |
| ILC | 1 (6.25%) |
| DCIS | 2 (12.5%) |
| IDCs with extensive DCIS component | 5 (31.25%) |
| Metrics | Tumors | FGT | p-Value |
|---|---|---|---|
| Mean diffusion tensor size (E[Diso]) | 1.43 (0.54) | 2.33 (0.22) | <0.001 |
| Variance of diffusion tensor sizes (V[Diso]) | 0.73 (0.19) | 0.97 (0.33) | 0.06 |
| Mean diffusion tensor shape (E[D∆2]) | 0.47 (0.15) | 0.27 (0.11) | <0.001 |
| Fractional anisotropy (FA) | 0.39 (0.07) | 0.32 (0.08) | 0.02 |
| Orientational order parameter (OP) | 0.38 (0.16) | 0.38 (0.17) | 0.71 |
| Signal fraction of bin 1 (fbin1) | 0.53 (0.27) | 0.17 (0.14) | <0.001 |
| Signal fraction of bin 2 (fbin2) | 0.23 (0.11) | 0.22 (0.07) | 0.40 |
| Signal fraction of bin 3 (fbin3) | 0.29 (0.19) | 0.62 (0.10) | <0.001 |
| Metrics | Invasive Tumors | DCIS and IDCs with Extensive DCIS Component | p-Value |
|---|---|---|---|
| Mean diffusion tensor size (E[Diso]) | 1.22 (0.32) | 1.72 (0.66) | 0.05 |
| Variance of diffusion tensor sizes (V[Diso]) | 0.68 (0.16) | 0.79 (0.22) | 0.24 |
| Mean diffusion tensor shape (E[D∆2]) | 0.53 (0.10) | 0.4 (0.18) | 0.11 |
| Fractional anisotropy (FA) | 0.38 (0.07) | 0.4 (0.08) | 0.45 |
| Orientational order parameter (OP) | 0.35 (0.15) | 0.43 (0.17) | 0.20 |
| Signal fraction of bin 1 (fbin1) | 0.64 (0.13) | 0.4 (0.25) | 0.03 |
| Signal fraction of bin 2 (fbin2) | 0.24 (0.12) | 0.21 (0.11) | 0.15 |
| Signal fraction of bin 3 (fbin3) | 0.18 (0.08) | 0.42 (0.21) | 0.03 |
| Metrics | Premenopausal | Postmenopausal | p-Value |
|---|---|---|---|
| Mean diffusion tensor size (E[Diso]) | 2.35 (0.22) | 2.31 (0.23) | 0.96 |
| Variance of diffusion tensor sizes (V[Diso]) | 0.88 (0.3) | 1.06 (0.36) | 0.42 |
| Mean diffusion tensor shape (E[D∆2]) | 0.25 (0.09) | 0.29 (0.13) | 0.71 |
| Fractional anisotropy (FA) | 0.3 (0.07) | 0.33 (0.09) | 0.37 |
| Orientational order parameter (OP) | 0.36 (0.18) | 0.4 (0.18) | 0.42 |
| Signal fraction of bin 1 (fbin1) | 0.14 (0.11) | 0.20 (0.17) | 0.42 |
| Signal fraction of bin 2 (fbin2) | 0.23 (0.08) | 0.21 (0.06) | 0.96 |
| Signal fraction of bin 3 (fbin3) | 0.63 (0.11) | 0.61 (0.10) | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naranjo, I.D.; Reymbaut, A.; Brynolfsson, P.; Lo Gullo, R.; Bryskhe, K.; Topgaard, D.; Giri, D.D.; Reiner, J.S.; Thakur, S.B.; Pinker-Domenig, K. Multidimensional Diffusion Magnetic Resonance Imaging for Characterization of Tissue Microstructure in Breast Cancer Patients: A Prospective Pilot Study. Cancers 2021, 13, 1606. https://doi.org/10.3390/cancers13071606
Naranjo ID, Reymbaut A, Brynolfsson P, Lo Gullo R, Bryskhe K, Topgaard D, Giri DD, Reiner JS, Thakur SB, Pinker-Domenig K. Multidimensional Diffusion Magnetic Resonance Imaging for Characterization of Tissue Microstructure in Breast Cancer Patients: A Prospective Pilot Study. Cancers. 2021; 13(7):1606. https://doi.org/10.3390/cancers13071606
Chicago/Turabian StyleNaranjo, Isaac Daimiel, Alexis Reymbaut, Patrik Brynolfsson, Roberto Lo Gullo, Karin Bryskhe, Daniel Topgaard, Dilip D. Giri, Jeffrey S. Reiner, Sunitha B. Thakur, and Katja Pinker-Domenig. 2021. "Multidimensional Diffusion Magnetic Resonance Imaging for Characterization of Tissue Microstructure in Breast Cancer Patients: A Prospective Pilot Study" Cancers 13, no. 7: 1606. https://doi.org/10.3390/cancers13071606
APA StyleNaranjo, I. D., Reymbaut, A., Brynolfsson, P., Lo Gullo, R., Bryskhe, K., Topgaard, D., Giri, D. D., Reiner, J. S., Thakur, S. B., & Pinker-Domenig, K. (2021). Multidimensional Diffusion Magnetic Resonance Imaging for Characterization of Tissue Microstructure in Breast Cancer Patients: A Prospective Pilot Study. Cancers, 13(7), 1606. https://doi.org/10.3390/cancers13071606