
Radiomics in Renal Cell Carcinoma—A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sources
2.2. Inclusion and Exclusion Criteria
- P (patients): Patients with benign or malign renal tumors;
- I (interventions): Radiomics or texture analysis;
- C (comparison): CT or MRI;
- O (outcome): Histologic subtyping (including differentiation of different RCC subtypes, differentiation and/or analysis of any benign and/or malign renal tumors, tumor grading, and any mutation analyses) and treatment response assessment.
2.3. Search Terms
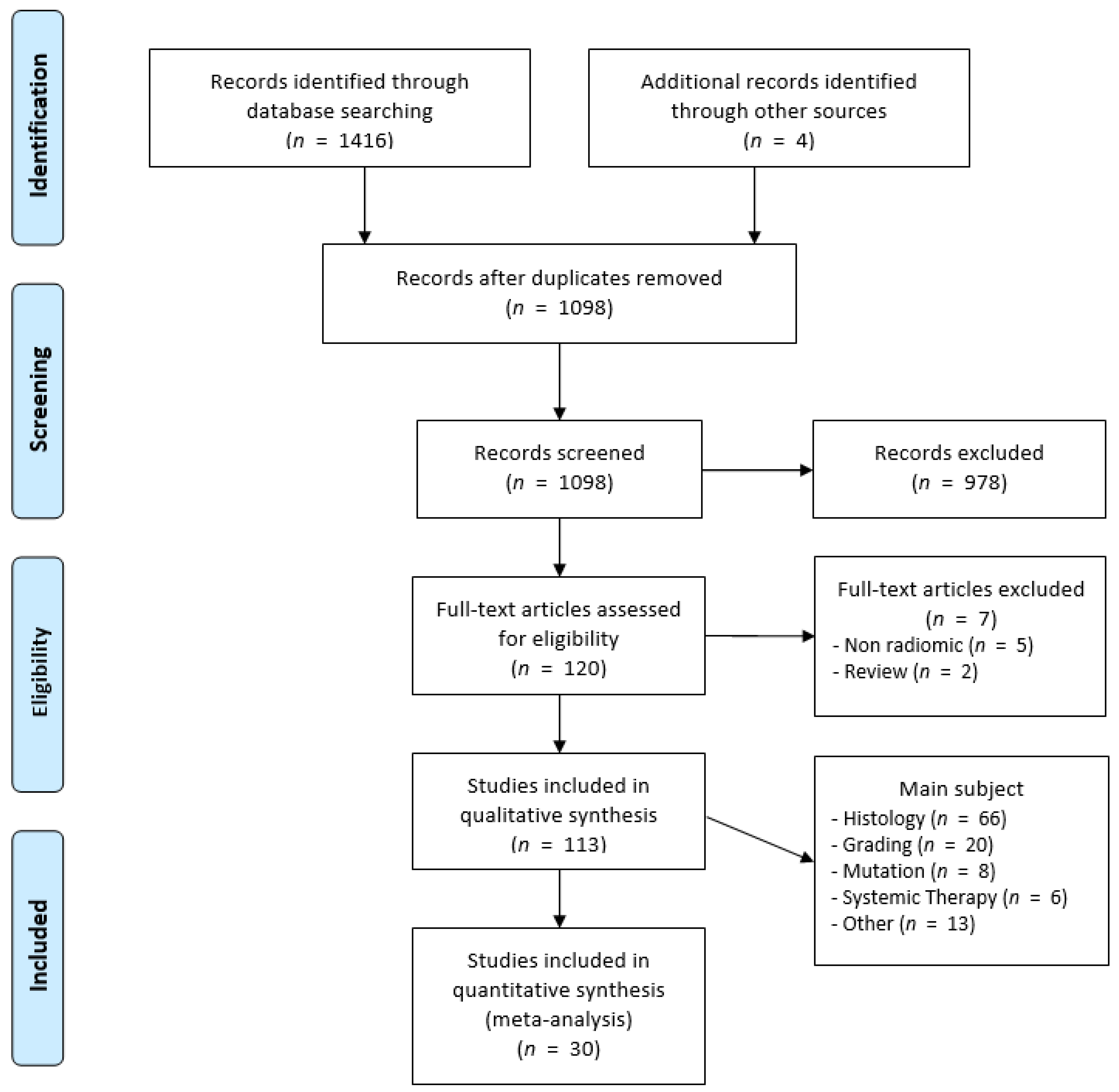
2.4. Study Selection
2.5. Quality Assessment
2.6. Meta-Analysis
- a meta-analysis of all studies investigating the use of radiomics to compare benign versus malign renal tumors;
- a meta-analysis of all studies investigating the use of radiomics for treatment response assessment of metastatic RCC with any ST.
2.7. Statistical Analysis
3. Results
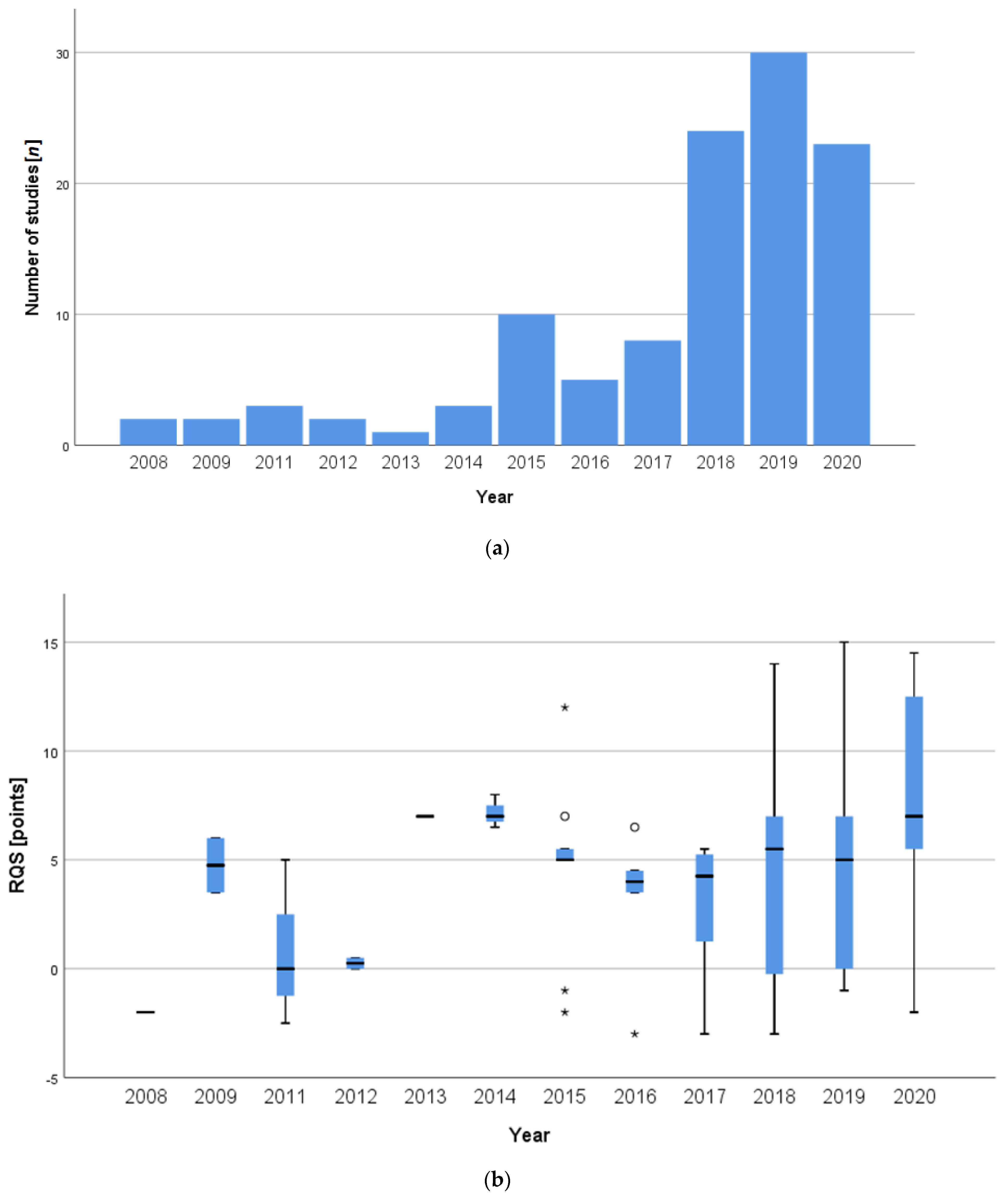
3.1. Included Studies
3.2. Quality Assessment
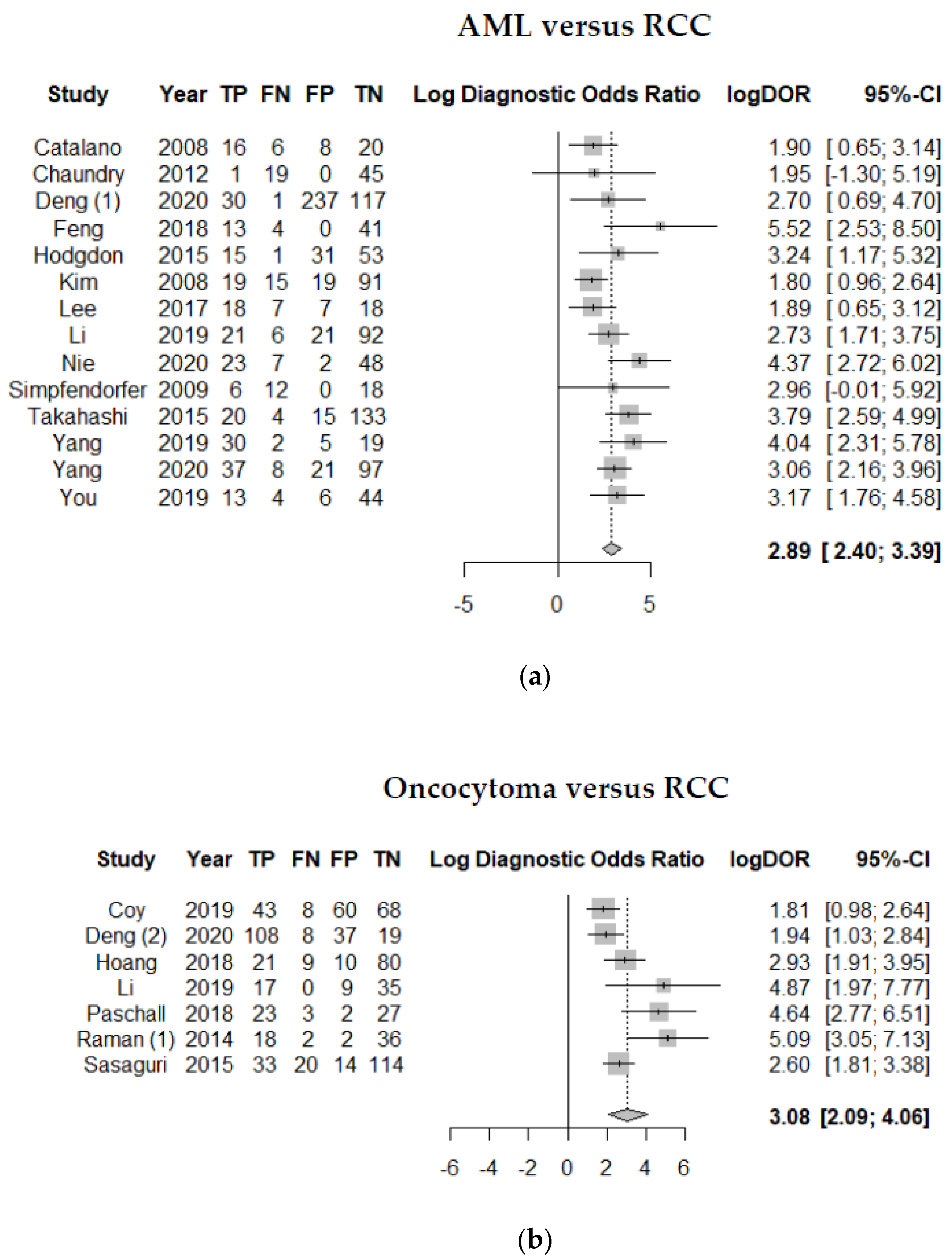
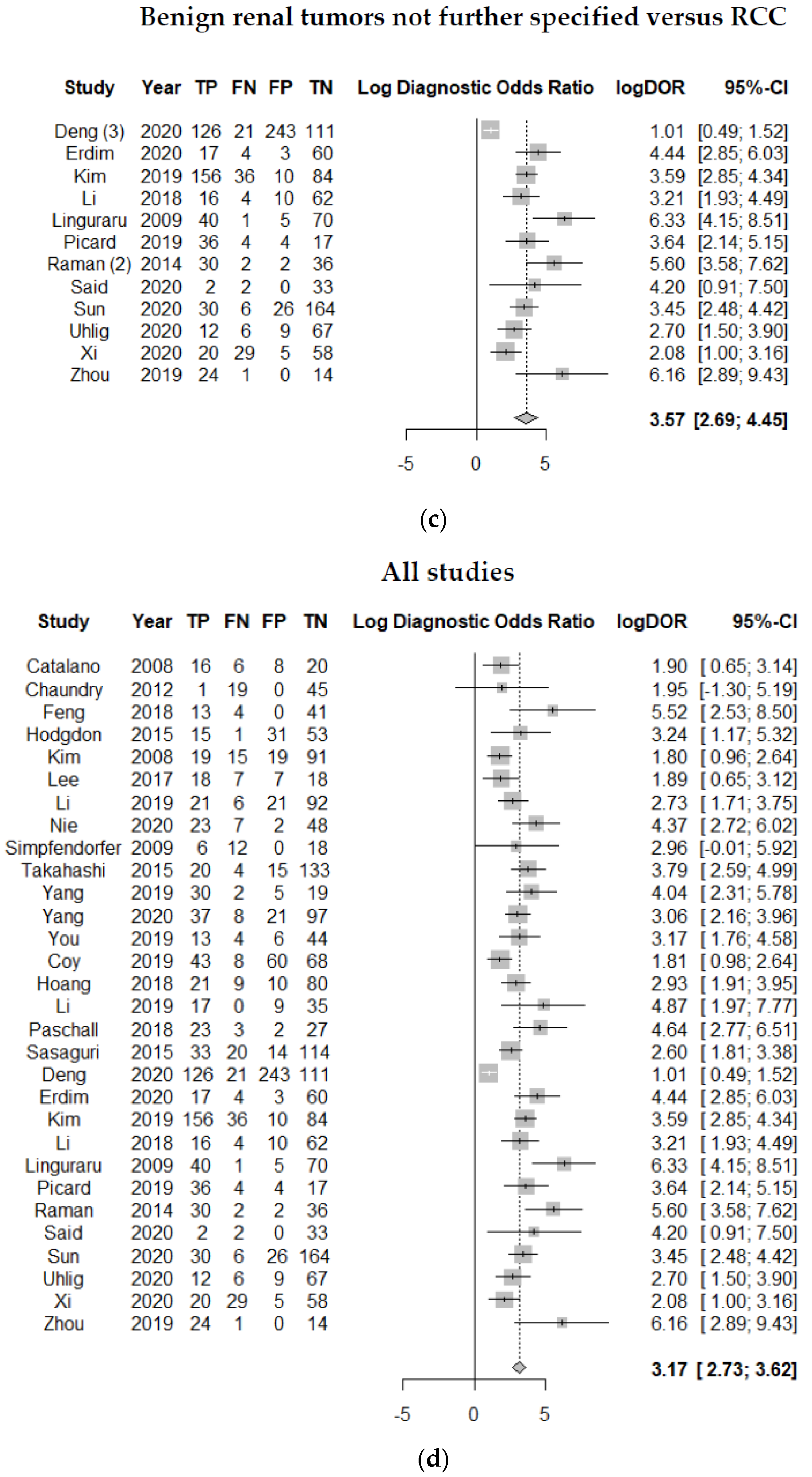
3.3. Differentiation of Benign and Malign Renal Tumors
3.4. Treatment Response Assessment
4. Discussion
4.1. Quality Assessment
4.2. Classification of Dignity of Renal Tumors
4.3. Treatment Response Assessment
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 729–762. [Google Scholar] [CrossRef] [PubMed]
- Mannil, M.; von Spiczak, J.; Manka, R.; Alkadhi, H. Texture Analysis and Machine Learning for Detecting Myocardial Infarction in Noncontrast Low-Dose Computed Tomography: Unveiling the Invisible. Investig. Radiol. 2018, 53, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Castellano, G.; Bonilha, L.; Li, L.M.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Tourassi, G.D. Journey toward computer-aided diagnosis: Role of image texture analysis. Radiology 1999, 213, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Bauman, T.M.; Potretzke, A.M.; Wright, A.J.; Knight, B.A.; Vetter, J.M.; Figenshau, R.S. Partial Nephrectomy for Presumed Renal-Cell Carcinoma: Incidence, Predictors, and Perioperative Outcomes of Benign Lesions. J. Endourol. 2017, 31, 412–417. [Google Scholar] [CrossRef]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef]
- Ursprung, S.; Beer, L.; Bruining, A.; Woitek, R.; Stewart, G.D.; Gallagher, F.A.; Sala, E. Radiomics of computed tomography and magnetic resonance imaging in renal cell carcinoma-a systematic review and meta-analysis. Eur. Radiol. 2020, 30, 3558–3566. [Google Scholar] [CrossRef] [PubMed]
- Antunes, J.; Viswanath, S.; Rusu, M.; Valls, L.; Hoimes, C.; Avril, N.; Madabhushi, A. Radiomics Analysis on FLT-PET/MRI for Characterization of Early Treatment Response in Renal Cell Carcinoma: A Proof-of-Concept Study. Transl. Oncol. 2016, 9, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.T.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane. Database. Syst. Rev. 2019, 10. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Kim, D.H.; Kim, H.S.; Park, S.Y.; Kim, J.Y.; Cho, S.J.; Shin, J.H.; Kim, J.H. Quality of science and reporting of radiomics in oncologic studies: Room for improvement according to radiomics quality score and TRIPOD statement. Eur. Radiol. 2020, 30, 523–536. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef]
- Deng, Y.; Soule, E.; Cui, E.; Samuel, A.; Shah, S.; Lall, C.; Sundaram, C.; Sandrasegaran, K. Usefulness of CT texture analysis in differentiating benign and malignant renal tumours. Clin. Radiol. 2020, 75, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Raman, S.P.; Chen, Y.; Schroeder, J.L.; Huang, P.; Fishman, E.K. CT texture analysis of renal masses: Pilot study using random forest classification for prediction of pathology. Acad. Radiol. 2014, 21, 1587–1596. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Lee, H.W.; Cho, H.W.; Joung, J.G.; Jeon, H.G.; Jeong, B.C.; Jeon, S.S.; Lee, H.M.; Nam, D.H.; Park, W.Y.; Kim, C.K. Integrative Radiogenomics Approach for Risk Assessment of Post-Operative Metastasis in Pathological T1 Renal Cell Carcinoma: A Pilot Retrospective Cohort Study. Cancers 2020, 12, 866. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Yu, D.; Ni, T.; Zhao, T.; Jin, Y.; Dong, E. Quantitative Analysis of Multiphase Contrast-Enhanced CT Images: A Pilot Study of Preoperative Prediction of Fat-Poor Angiomyolipoma and Renal Cell Carcinoma. AJR Am. J. Roentgenol. 2020, 214, 370–382. [Google Scholar] [CrossRef]
- Hosny, A.; Aerts, H.j.; Mak, R.H. Handcrafted versus deep learning radiomics for prediction of cancer therapy response. Lancet Digit. Health 2019, 1, e106–e107. [Google Scholar] [CrossRef]
- Sanders, G.D.; Neumann, P.J.; Basu, A. Recommendations for Conduct, Methodological Practices, and Reporting of Cost-effectiveness Analyses: Second Panel on Cost-Effectiveness in Health and Medicine. JAMA 2016, 316, 1093–1103. [Google Scholar] [CrossRef] [PubMed]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—“How-to” guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Sun, X.Y.; Feng, Q.-X.; Xu, X.; Zhang, J.; Zhu, F.-P.; Yang, Y.-H.; Zhang, Y.-D. Radiologic-Radiomic Machine Learning Models for Differentiation of Benign and Malignant Solid Renal Masses: Comparison With Expert-Level Radiologists. AJR Am. J. Roentgenol. 2020, 214, W44–W54. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, J.; Biggemann, L.; Nietert, M.M.; Beißbarth, T.; Lotz, J.; Kim, H.S.; Trojan, L.; Uhlig, A. Discriminating malignant and benign clinical T1 renal masses on computed tomography: A pragmatic radiomics and machine learning approach. Medicine (Baltimore) 2020, 99, e19725. [Google Scholar] [CrossRef] [PubMed]
- Picard, M.; Shah, N.; Flemming, B.; Kovacs, M.; Freeman, K.; Burchett, P.F.; Giovagnoli, D.A.; Hardie, A.D. Combined Qualitative and Quantitative Assessment of Low-Attenuation Renal Lesions Improves Identification of Renal Malignancy on Noncontrast Computed Tomography. J. Comput. Assist. Tomogr. 2019, 43, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Said, D.; Hectors, S.J.; Wilck, E.; Rosen, A.; Stocker, D.; Bane, O.; Beksaç, A.T.; Lewis, S.; Badani, K.; Taouli, B. Characterization of solid renal neoplasms using MRI-based quantitative radiomics features. Abdom. Radiol. 2020, 45, 2840–2850. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Takeuchi, M.; Sasaguri, K.; Leng, S.; Froemming, A.; Kawashima, A. CT negative attenuation pixel distribution and texture analysis for detection of fat in small angiomyolipoma on unenhanced CT. Abdom. Radiol. 2016, 41, 1142–1151. [Google Scholar] [CrossRef]
- Bharwani, N.; Miquel, M.E.; Powles, T.; Dilks, P.; Shawyer, A.; Sahdev, A.; Wilson, P.D.; Chowdhury, S.; Berney, D.M.; Rockall, A.G. Diffusion-weighted and multiphase contrast-enhanced MRI as surrogate markers of response to neoadjuvant sunitinib in metastatic renal cell carcinoma. Br. J. Cancer 2014, 110, 616–624. [Google Scholar] [CrossRef]
- Boos, J.; Revah, G.; Brook, O.R.l.; Rangaswamy, B.; Bhatt, R.S.; Brook, A.; Raptopoulos, V. Intensity Distribution Curve (Histogram) Analysis of Patients Undergoing Antiangiogenic Therapy for Metastatic Renal Cell Carcinoma. AJR Am. J. Roentgenol. 2017, 209, W85–W92. [Google Scholar] [CrossRef]
- Goh, V.; Ganeshan, B.; Nathan, P.; Juttla, J.K.; Vinayan, A.; Miles, K.A. Assessment of response to tyrosine kinase inhibitors in metastatic renal cell cancer: CT texture as a predictive biomarker. Radiology 2011, 261, 165–171. [Google Scholar] [CrossRef]
- Haider, M.A.; Vosough, A.; Khalvati, F.; Kiss, A.; Ganeshan, B.; Bjarnason, G.A. CT texture analysis: A potential tool for prediction of survival in patients with metastatic clear cell carcinoma treated with sunitinib. Cancer Imaging 2017, 17. [Google Scholar] [CrossRef]
- Osawa, T.; Takeuchi, A.; Kojima, T.; Shinohara, N.; Eto, M.; Nishiyama, H. Overview of current and future systemic therapy for metastatic renal cell carcinoma. Jpn. J. Clin. Oncol. 2019, 49, 395–403. [Google Scholar] [CrossRef]
- Fournier, L.; Costaridou, L.; Bidaut, L.; Michoux, N.; Lecouvet, F.E.; de Geus-Oei, L.-F.; Boellaard, R.; Oprea-Lager, D.E.; Obuchowski, N.A.; Caroli, A.; et al. Incorporating radiomics into clinical trials: Expert consensus on considerations for data-driven compared to biologically driven quantitative biomarkers. Eur. Radiol. 2021, 2021. [Google Scholar] [CrossRef]
- Gorin, M.A.; Rowe, S.P.; Baras, A.S.; Solnes, L.B.; Ball, M.W.; Pierorazio, P.M.; Pavlovich, C.P.; Epstein, J.I.; Javadi, M.S.; Allaf, M.E. Prospective Evaluation of 99mTc-sestamibi SPECT/CT for the Diagnosis of Renal Oncocytomas and Hybrid Oncocytic/Chromophobe Tumors. Eur Urol. 2016, 69, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.H.; Prezzi, D.; Kelly-Morland, C.; Goh, V. Imaging for the diagnosis and response assessment of renal tumours. World. J. Urol. 2018, 36, 1927–1942. [Google Scholar] [CrossRef]
- Sheikhbahaei, S.; Jones, C.S.; Porter, K.K.; Rowe, S.P.; Gorin, M.A.; Baras, A.S.; Pierorazio, P.M.; Ball, M.W.; Higuchi, T.; Johnson, P.T. Defining the Added Value of 99mTc-MIBI SPECT/CT to Conventional Cross-Sectional Imaging in the Characterization of Enhancing Solid Renal Masses. Clin. Nucl. Med. 2017, 42, e188–e193. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.M.; Solnes, L.B.; Rowe, S.P.; Gorin, M.A.; Sheikhbahaei, S.; Fung, G.; Frey, E.C.; Allaf, M.E.; Dy, Y.; Javadi, M.S. Use of quantitative SPECT/CT reconstruction in 99m Tc-sestamibi imaging of patients with renal masses. Ann. Nucl. Med. 2018, 32, 87–93. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Points | Average Score | |
|---|---|---|---|
| 1 | Image protocol quality | +1 if protocols are well-documented +1 if public protocol is used | 0.65 |
| 2 | Multiple segmentations | +1 if multiple segmentations are carried out (i.e., different physicians/algorithms/software) | 0.53 |
| 3 | Phantom study | +1 if phantom study is used on all scanners | 0.00 |
| 4 | Multiple time points | +1 if images are collected at additional time points | 0.07 |
| 5 | Feature reduction or adjustment for multiple testing | −3 if neither measure is implemented +3 if either measure is implemented | 0.69 |
| 6 | Multivariable analysis with non-radiomics features | +1 if multivariable analysis with non-radiomics features is carried out | 0.12 |
| 7 | Biological correlates | +1 if phenotypic differences are demonstrated | 0.96 |
| 8 | Cut-of-analyses | +1 if risk groups are determined by either the median, a previously published cut-off or if a continuous risk variable is reported | 0.09 |
| 9 | Discrimination statistics | +1 if a discrimination statistic and its statistical significance is reported (i.e., ROC curve, AUC) +1 if a resampling method technique is also applied (i.e., bootstrapping, cross-validation) | 1.21 |
| 10 | Calibration statistics | +1 if a calibration statistic and its statistical significance is reported (i.e. Calibration-in-the-large/slope) +1 if a resampling method technique is also applied (i.e., bootstrapping, cross-validation) | 0.02 |
| 11 | Prospective | +7 for prospective validation of a radiomics signature in an appropriate trial | 0.46 |
| 12 | Validation | −5 if validation is missing +2 if validation is based on a dataset from the same institute +3 if validation is based on a dataset from another institute +4 if validation is based on two datasets from two institutes +4 if study validates a previously published signature +5 of validation is based in three or more datasets from distinct institutes | −3.88 |
| 13 | Gold standard | +2 if comparison to the current gold standard is carried out | 1.91 |
| 14 | Potential clinical utility | +2 if a potential application in a clinical setting is reported | 2.00 |
| 15 | Cost-effectiveness analysis | +1 if the cost-effectiveness of the clinical application is reported | 0.00 |
| 16 | Open science and data | +1 if scans are open source +1 if region of interest (ROI) segmentations are open source +1 if code is open source +1 if representative segmentations and features are open source | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mühlbauer, J.; Egen, L.; Kowalewski, K.-F.; Grilli, M.; Walach, M.T.; Westhoff, N.; Nuhn, P.; Laqua, F.C.; Baessler, B.; Kriegmair, M.C. Radiomics in Renal Cell Carcinoma—A Systematic Review and Meta-Analysis. Cancers 2021, 13, 1348. https://doi.org/10.3390/cancers13061348
Mühlbauer J, Egen L, Kowalewski K-F, Grilli M, Walach MT, Westhoff N, Nuhn P, Laqua FC, Baessler B, Kriegmair MC. Radiomics in Renal Cell Carcinoma—A Systematic Review and Meta-Analysis. Cancers. 2021; 13(6):1348. https://doi.org/10.3390/cancers13061348
Chicago/Turabian StyleMühlbauer, Julia, Luisa Egen, Karl-Friedrich Kowalewski, Maurizio Grilli, Margarete T. Walach, Niklas Westhoff, Philipp Nuhn, Fabian C. Laqua, Bettina Baessler, and Maximilian C. Kriegmair. 2021. "Radiomics in Renal Cell Carcinoma—A Systematic Review and Meta-Analysis" Cancers 13, no. 6: 1348. https://doi.org/10.3390/cancers13061348
APA StyleMühlbauer, J., Egen, L., Kowalewski, K.-F., Grilli, M., Walach, M. T., Westhoff, N., Nuhn, P., Laqua, F. C., Baessler, B., & Kriegmair, M. C. (2021). Radiomics in Renal Cell Carcinoma—A Systematic Review and Meta-Analysis. Cancers, 13(6), 1348. https://doi.org/10.3390/cancers13061348