
How Immunotherapy Has Changed the Continuum of Care in Hepatocellular Carcinoma


 , ,
, ,  ,
, 


Abstract
Simple Summary
Abstract
1. Introduction
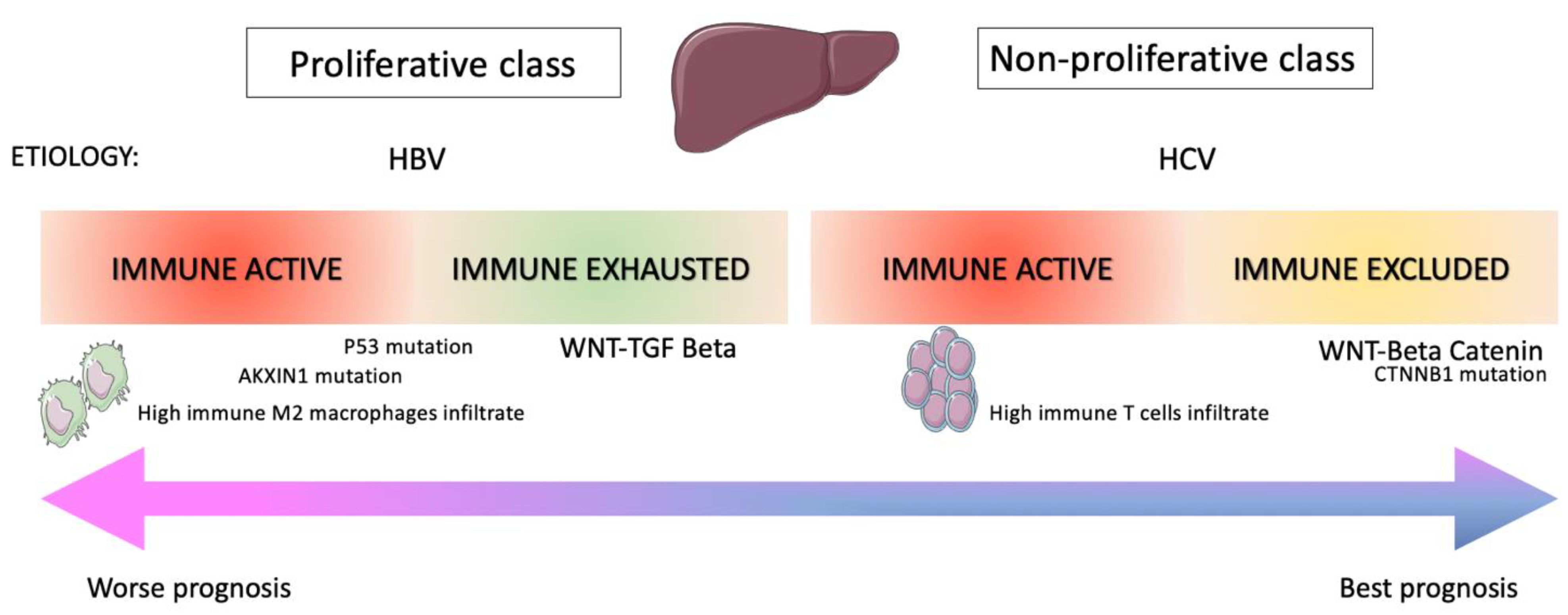
2. Immune Landscape of Hepatocarcinoma Disease
3. Clinical Evidence of Immune Checkpoint Inhibitors in Hepatocarcinoma
3.1. Nivolumab
3.2. Pembrolizumab
3.3. Atezolizumab
3.4. Anti-CTLA-4 Plus Anti-PD-1/PD-L1 Antibodies Combinations
4. Combining Immune Checkpoint Inhibitors with Targeted Agents
5. Same Approach in a Different Setting
6. Immunotherapy in Combination with Locoregional Treatment
7. Strategies beyond ICI
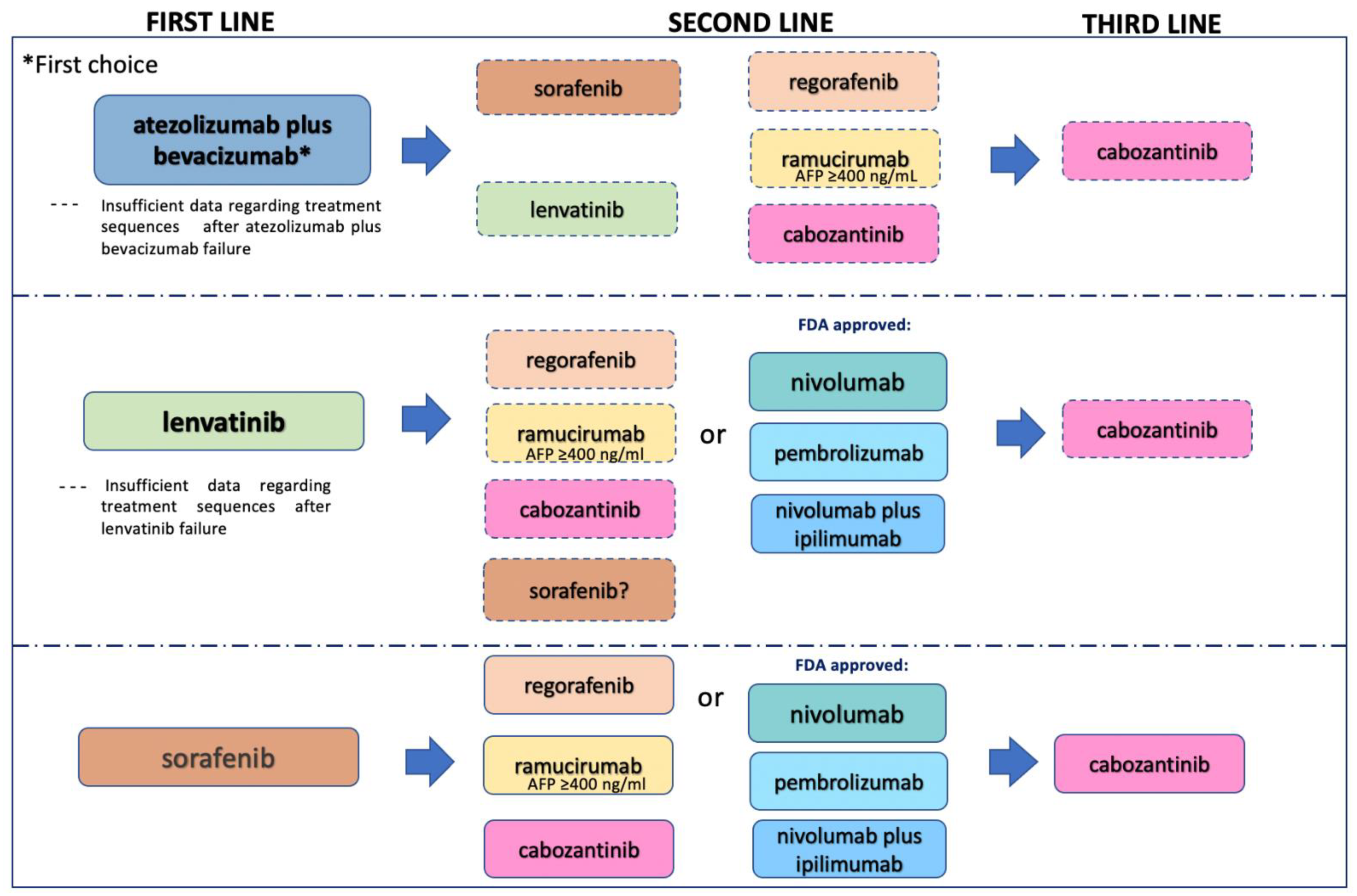
8. Correct Treatment Sequence after Implementation of ICI in the HCC Therapeutic Landscape
9. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Cariani, E.; Missale, G. Immune landscape of hepatocellular carcinoma microenvironment: Implications for prognosis and therapeutic applications. Liver Int. 2019, 39, 1608–1621. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC Staging Classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Saborowski, A. Current strategies for the treatment of intermediate and advanced hepatocellular carcinoma. Cancer Treat. Rev. 2020, 82, 101946. [Google Scholar] [CrossRef] [PubMed]
- Erstad, D.J.; Tanabe, K.K. Hepatocellular carcinoma: Early-stage management challenges. J. Hepatocell. Carcinoma 2017, 4, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Bagante, F.; Sahara, K.; Moris, D.; Hyer, J.M.; Wu, L.; Ratti, F.; Marques, H.P.; Soubrane, O.; Paredes, A.Z.; et al. Prognosis after Resection of Barcelona Clinic Liver Cancer (BCLC) Stage 0, A, and B Hepatocellular Carcinoma: A Comprehensive Assessment of the Current BCLC Classification. Ann. Surg. Oncol. 2019, 26, 3693–3700. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.-K.; Yen, C.-J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Nishida, N.; Kudo, M. Immunological Microenvironment of Hepatocellular Carcinoma and Its Clinical Implication. Oncology 2017, 92, 40–49. [Google Scholar] [CrossRef]
- Crispe, I.N. Hepatic T cells and liver tolerance. Nat. Rev. Immunol. 2003, 3, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, Y.; Shi, C.; Zhou, X.; Xu, K.; Jiao, D.; Sun, Z.; Han, X. A novel immune classification reveals distinct immune escape mechanism and genomic alterations: Implications for immunotherapy in hepatocellular carcinoma. J. Transl. Med. 2021, 19, 5. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Liu, S.; Zeng, S.; Shen, H. From bench to bed: The tumor immune microenvironment and current immunotherapeutic strategies for hepatocellular carcinoma. J. Exp. Clin. Cancer Res. 2019, 38, 396. [Google Scholar] [CrossRef] [PubMed]
- Kurebayashi, Y.; Ojima, H.; Tsujikawa, H.; Kubota, N.; Maehara, J.; Abe, Y.; Kitago, M.; Shinoda, M.; Kitagawa, Y.; Sakamoto, M. Landscape of immune microenvironment in hepatocellular carcinoma and its additional impact on histological and molecular classification. Hepatology 2018, 68, 1025–1041. [Google Scholar] [CrossRef] [PubMed]
- Kakumu, S.; Ito, S.; Ishikawa, T.; Mita, Y.; Tagaya, T.; Fukuzawa, Y.; Yoshioka, K. Decreased function of peripheral blood dendritic cells in patients with hepatocellular carcinoma with hepatitis B and C virus infection. J. Gastroenterol. Hepatol. 2000, 15, 431–436. [Google Scholar] [CrossRef]
- Chen, J.; Gingold, J.A.; Su, X. Immunomodulatory TGF-β Signaling in Hepatocellular Carcinoma. Trends Mol. Med. 2019, 25, 1010–1023. [Google Scholar] [CrossRef]
- Horst, A.K.; Kumashie, K.G.; Neumann, K.; Diehl, L.; Tiegs, G. Antigen presentation, autoantibody production, and therapeutic targets in autoimmune liver disease. Cell. Mol. Immunol. 2021, 18, 92–111. [Google Scholar] [CrossRef]
- Bai, J.; Liang, P.; Li, Q.; Feng, R.; Liu, J. Cancer Immunotherapy-Immune Checkpoint Inhibitors in Hepatocellular Carcinoma. Recent Patents Anti-Cancer Drug Discov. 2021, 16, 1. [Google Scholar] [CrossRef]
- He, S.; Jiang, W.; Fan, K.; Wang, X. The Efficacy and Safety of Programmed Death-1 and Programmed Death Ligand 1 Inhibitors for the Treatment of Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 881. [Google Scholar] [CrossRef]
- Federico, P.; Petrillo, A.; Giordano, P.; Bosso, D.; Fabbrocini, A.; Ottaviano, M.; Rosanova, M.; Silvestri, A.; Tufo, A.; Cozzolino, A.; et al. Immune Checkpoint Inhibitors in Hepatocellular Carcinoma: Current Status and Novel Perspectives. Cancers 2020, 12, 3025. [Google Scholar] [CrossRef]
- Yau, T.; Park, J.W.; Finn, R.S.; Cheng, A.L.; Mathurin, P.; Edeline, J.; Kudo, M.; Han, K.H.; Harding, J.J.; Merle, P.; et al. CheckMate 459: A randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann. Oncol. 2019, 30, v874–v875. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.-Y.; Breder, V.V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Results of KEYNOTE-240: Phase 3 study of pembrolizumab (Pembro) vs best supportive care (BSC) for second line therapy in advanced hepatocellular carcinoma (HCC). J. Clin. Oncol. 2019, 37, 4004. [Google Scholar] [CrossRef]
- Lee, M.S.; Ryoo, B.-Y.; Hsu, C.-H.; Numata, K.; Stein, S.; Verret, W.; Hack, S.P.; Spahn, J.; Liu, B.; Abdullah, H.; et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): An open-label, multicentre, phase 1b study. Lancet Oncol. 2020, 21, 808–820. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Lim, H.Y.; Kudo, M.; Breder, V.V.; Merle, P.; et al. IMbrave150: Updated overall survival (OS) data from a global, randomized, open-label phase III study of atezolizumab (atezo) + bevacizumab (bev) versus sorafenib (sor) in patients (pts) with unresectable hepatocellular carcinoma (HCC). J. Clin. Oncol. 2021, 39, 267. [Google Scholar] [CrossRef]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Caro, R.B.; Zurawski, B.; Kim, S.-W.; Costa, E.C.; Park, K.; Alexandru, A.; Lupinacci, L.; De la Mora, J.E.; et al. Nivolumab plus ipilimumab in advanced non–small-cell lung cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Sangro, B.; Gomez-Martin, C.; de la Mata, M.; Iñarrairaegui, M.; Garralda, E.; Barrera, P.; Riezu-Boj, J.-I.; Larrea, E.; Alfaro, C.; Sarobe, P.; et al. A clinical trial of CTLA-4 blockade with tremelimumab in patients with hepatocellular carcinoma and chronic hepatitis C. J. Hepatol. 2013, 59, 81–88. [Google Scholar] [CrossRef]
- Kelley, R.K.; Abou-Alfa, G.K.; Bendell, J.C.; Kim, T.-Y.; Borad, M.J.; Yong, W.-P.; Morse, M.; Kang, Y.; Rebelatto, M.; Makowsky, M.; et al. Phase I/II study of durvalumab and tremelimumab in patients with unresectable hepatocellular carcinoma (HCC): Phase I safety and efficacy analyses. J. Clin. Oncol. 2017, 35, 4073. [Google Scholar] [CrossRef]
- Kelley, R.K.; Sangro, B.; Harris, W.; Ikeda, M.; Okusaka, T.; Kang, Y.-K.; Qin, S.; Tai, D.W.-M.; Lim, H.Y.; Yau, T.; et al. Safety, Efficacy, and Pharmacodynamics of Tremelimumab Plus Durvalumab for Patients With Unresectable Hepatocellular Carcinoma: Randomized Expansion of a Phase I/II Study. J. Clin. Oncol. 2021, 39, 2991–3001. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Chan, S.L.; Furuse, J.; Galle, P.R.; Kelley, R.K.; Qin, S.; Armstrong, J.; Darilay, A.; Vlahovic, G.; Negro, A.; et al. A randomized, multicenter phase 3 study of durvalumab (D) and tremelimumab (T) as first-line treatment in patients with unresectable hepatocellular carcinoma (HCC): HIMALAYA study. J. Clin. Oncol. 2018, 36, TPS4144. [Google Scholar] [CrossRef]
- Morse, M.A.; Sun, W.; Kim, R.; He, A.R.; Abada, P.B.; Mynderse, M.; Finn, R.S. The Role of Angiogenesis in Hepatocellular Carcinoma. Clin. Cancer Res. 2019, 25, 912–920. [Google Scholar] [CrossRef]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Evoron, T.; Emarcheteau, E.; Epernot, S.; Ecolussi, O.; Etartour, E.; Etaieb, J.; Eterme, M. Control of the Immune Response by Pro-Angiogenic Factors. Front. Oncol. 2014, 4, 70. [Google Scholar] [CrossRef]
- Lin, C.-C.; Golan, T.; Corral, J.; Moreno, V.; Chung, H.; Wasserstrom, H.; Yang, J.; Mi, G.; Bang, Y.-J. Phase 1 study of ramucirumab (R) plus durvalumab (D) in patients (pts) with locally advanced and unresectable or metastatic gastrointestinal or thoracic malignancies (NCT02572687); Phase 1a results. Ann. Oncol. 2016, 27, viii1. [Google Scholar] [CrossRef][Green Version]
- Finn, R.S.; Ikeda, M.; Zhu, A.X.; Sung, M.W.; Baron, A.D.; Kudo, M.; Okusaka, T.; Kobayashi, M.; Kumada, H.; Kaneko, S.; et al. Phase Ib Study of Lenvatinib Plus Pembrolizumab in Patients With Unresectable Hepatocellular Carcinoma. J. Clin. Oncol. 2020, 38, 2960–2970. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Shen, J.; Gu, S.; Zhang, Y.; Wu, L.; Wu, J.; Shao, G.; Zhang, Y.; Xu, L.; Yin, T.; et al. Camrelizumab in Combination with Apatinib in Patients with Advanced Hepatocellular Carcinoma (RESCUE): A Nonrandomized, Open-label, Phase II Trial. Clin. Cancer Res. 2021, 27, 1003–1011. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, J.; Shen, J.; Gu, S.; Wu, L.; Wu, J.; Shao, G.; Zhang, Y.; Xu, L.; Yin, T.; et al. Update on overall survival (OS) of RESCUE: An open-label, phase 2 trial of camrelizumab (C) in combination with apatinib (A) in patients with advanced hepatocellular carcinoma (HCC). J. Clin. Oncol. 2021, 39, 4076. [Google Scholar] [CrossRef]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 2020, 69, 1492–1501. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.; Cole, T.; Bengsch, B.; Tait, P.; Sayed, A.; Abomeli, F.; Gramenitskaya, D.; Allara, E.; Thomas, R.; Ward, C.; et al. A phase Ib study of pembrolizumab following trans-arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): PETAL. Ann. Oncol. 2019, 30, v288. [Google Scholar] [CrossRef]
- Alisa, A.; Ives, A.; Pathan, A.A.; Navarrete, C.V.; Williams, R.; Bertoletti, A.; Behboudi, S. Analysis of CD4+ T-Cell Responses to a Novel α-Fetoprotein-Derived Epitope in Hepatocellular Carcinoma Patients. Clin. Cancer Res. 2005, 11, 6686–6694. [Google Scholar] [CrossRef]
- Sawada, Y.; Yoshikawa, T.; Nobuoka, D.; Shirakawa, H.; Kuronuma, T.; Motomura, Y.; Mizuno, S.; Ishii, H.; Nakachi, K.; Konishi, M.; et al. Phase I Trial of a Glypican-3–Derived Peptide Vaccine for Advanced Hepatocellular Carcinoma: Immunologic Evidence and Potential for Improving Overall Survival. Clin. Cancer Res. 2012, 18, 3686–3696. [Google Scholar] [CrossRef]
- Palmer, D.H.; Midgley, R.S.; Mirza, N.; Torr, E.E.; Ahmed, F.; Steele, J.C.; Steven, N.M.; Kerr, D.J.; Young, L.S.; Adams, D.H. A phase II study of adoptive immunotherapy using dendritic cells pulsed with tumor lysate in patients with hepatocellular carcinoma. Hepatology 2009, 49, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Heo, J.; Breitbach, C.J.; Moon, A.; Kim, C.W.; Patt, R.; Kim, M.K.; Lee, Y.K.; Oh, S.Y.; Woo, H.Y.; Parato, K.; et al. Sequential Therapy With JX-594, A Targeted Oncolytic Poxvirus, Followed by Sorafenib in Hepatocellular Carcinoma: Preclinical and Clinical Demonstration of Combination Efficacy. Mol. Ther. 2011, 19, 1170–1179. [Google Scholar] [CrossRef]
- Ady, J.W.; Heffner, J.; Mojica, K.; Johnsen, C.; Belin, L.J.; Love, D.; Chen, C.-T.; Pugalenthi, A.; Klein, E.; Chen, N.G.; et al. Oncolytic immunotherapy using recombinant vaccinia virus GLV-1h68 kills sorafenib-resistant hepatocellular carcinoma efficiently. Surgery 2014, 156, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Altomonte, J.; Marozin, S.; Schmid, R.M.; Ebert, O. Engineered Newcastle Disease Virus as an Improved Oncolytic Agent Against Hepatocellular Carcinoma. Mol. Ther. 2010, 18, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Badrinath, N.; Woo, H.Y.; Heo, J. Oncolytic Virus-Based Immunotherapies for Hepatocellular Carcinoma. Mediat. Inflamm. 2017, 2017, 5198798. [Google Scholar] [CrossRef]
- Park, B.-H.; Hwang, T.; Liu, T.-C.; Sze, D.Y.; Kim, J.-S.; Kwon, H.-C.; Oh, S.Y.; Han, S.-Y.; Yoon, J.-H.; Hong, S.-H.; et al. Use of a targeted oncolytic poxvirus, JX-594, in patients with refractory primary or metastatic liver cancer: A phase I trial. Lancet Oncol. 2008, 9, 533–542. [Google Scholar] [CrossRef]
- Efficace, F.; Vignetti, M. Quality of life and CAR-T cell therapy in children, adolescents, and young adults with haematological malignancies. Lancet Oncol. 2019, 20, 1625–1626. [Google Scholar] [CrossRef]
- Gao, H.; Li, K.; Tu, H.; Pan, X.; Jiang, H.; Shi, B.; Kong, J.; Wang, H.; Yang, S.; Gu, J.; et al. Development of T Cells Redirected to Glypican-3 for the Treatment of Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6418–6428. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Treatment (and Control) | Target | Setting/Target Patients | Start Date |
|---|---|---|---|---|
| NCT03638141 | durvalumab and tremelimumab + DEB-TACE | Anti-PD-L1+ anti-CTLA-4 | Intermediate stage/30 pts | 2 October 2019 |
| NCT04273100 | PD-1 mAb + Lenvatinib + TACE | Anti-PD-1+ MKI | Intermediate stage/56 pts | 14 November 2019 |
| NCT04522544 | Durvalumab and tremelimumab + SIRT or TACE | Anti-PD-L1+ anti-CTLA-4 | Intermediate stage/84 pts | 15 December 2020 |
| NCT04268888 | Nivolumab + TACE/TAE | Anti-PD-1 | Intermediate stage/522 pts | 8 May 2019 |
| EMERALD-1 (NCT03778957) | Durvalumab +TACE versus durvalumab and bevacizumab + TACE versus placebo + TACE | Anti-PD-L1, anti-PD-L1 + anti-VEGF | Locoregional HCC/710 | 30 November 2018 |
| LEAP012 (NCT04246177) | pembrolizumab + lenvatinib + TACE versus placebo + TACE | Anti-PD-1 + MKI | Intermediate stage /950 pts | 22 May 2020 |
| PETAL (NCT03397654) | Pembrolizumab following TACE | anti-PD-1 | Intermediate stage/26 pts | 28 January 2018 |
| NCT03316872 | Pembrolizumab + SBRT | Anti-PD-1 | 2nd line setting/30 pts | 15 February 2018 |
| NCT02837029 | nivolumab+ SIRT | Anti-PD-1 | Advanced HCC/27 pts | July 2016 |
| NCT03033446 in Asian patients | nivolumab + SIRT | Anti-PD-1 | Advanced HCC/40 pts | 20 December 2016 |
| NCT03380130 | nivolumab after SIRT | Anti-PD-1 | Advanced HCC/41 pts | 11 September 2017 |
| NCT02988440 | Sorafenib + spartalizumab | MKI + anti-PD-1 | Advanced HCC/20 pts | 20 April 2017 |
| NCT03347292 | Regorafenib + pembrolizumab | MKI + anti-PD-1 | 1st line setting/57 pts | 18 June 2018 |
| Regomune (NCT03475953) Expansion cohort D | Regorafenib + avelumab in solid tumors | MKI + anti-PD-1 | 2nd line setting/482 patients | 4 May 2018 |
| Checkmate 040NCT01658878 | Nivolumab; nivolumab + ipilimumab; Cabozantinib+ nivolumab; Cabozantinib + nivolumab + ipilimumab | Anti-PD-1, anti-PD-1+anti-CTLA-4; MKI + anti-PD-1; MKI + anti-PD-1 + anti-CTLA-4 | Advanced HCC: uninfected HCC pts, HCV-infected HCC pts, and HBV-infected pts 659 patients | 30 October 2012 |
| NCT03764293 | camrelizumab + apatinib versus sorafenib | MKI + anti-PD-1 | 1st line setting/510 pts | 10 June 2019 |
| COSMIC-312 (NCT03755791) | Cabozantinib atezolizumab versus sorafenib | MKI + anti-PD-L1 | 1st line setting/740 pts | 10 December 2018 |
| NCT03605706 | Camrelizumab + folfox | Anti-PD-1 | 1st line setting/396 pts | 31 May 2019 |
| HIMALAYA (NCT03298451) | Tremelimumab + durvalumab versus sorafenib | Anti-CTLA4 Ab + anti-PD-L1 | 1st line setting/1504 pts | 11 October 2017 |
| LEAP-002 (NCT03713593) | Lenvatinib plus pembrolizumab versus lenvatinib | MKI + anti-PD-1 versus MKI | 1st line setting/750 pts | 31 December 2018 |
| NCT03228667 | N-803 + Durvalumab + PD-L1 t-haNK | Anti-PD-1/PD-L1 | PD to ICIs/145 pts | 11 December 2018 |
| Study | Treatment (and Control) | Target | Setting/Target Patients | Start Date |
|---|---|---|---|---|
| EMERALD-2 (NCT03847428) | Durvalumab versus durvalumab + bevacizumab versus placebo | Anti-PD-L1 + anti-VEGF | Adjuvant setting/888 pts | 29 April 2019 |
| Keynote 937 (NCT03867084) | Pembrolizumab Versus placebo | Anti-PD-1 | Adjuvant setting/ CR after surgery or local ablation/950 pts | 28 May 2019 |
| Checkmate 9DX (NCT03383458) | Nivolumab versus placebo | Anti-PD-1 | Adjuvant setting/ CR after surgery or local ablation/530 pts | 18 April 2018 |
| IMbrave050 (NCT04102098) | Atezolizumab + bevacizumab versus active surveillance | Anti-PD-L1 + anti-VEGF | Adjuvant setting/662 pts | 31 December 2019 |
| Jupiter04 (NCT03859128) | Toripalimab versus placebo | Anti-PD-1 | Adjuvant setting/ CR after surgery/402 pts | 1 March 2019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, G.; Ciardiello, D.; Paragliola, F.; Nacca, V.; Santaniello, W.; Urraro, F.; Stanzione, M.; Niosi, M.; Dallio, M.; Federico, A.; et al. How Immunotherapy Has Changed the Continuum of Care in Hepatocellular Carcinoma. Cancers 2021, 13, 4719. https://doi.org/10.3390/cancers13184719
Martini G, Ciardiello D, Paragliola F, Nacca V, Santaniello W, Urraro F, Stanzione M, Niosi M, Dallio M, Federico A, et al. How Immunotherapy Has Changed the Continuum of Care in Hepatocellular Carcinoma. Cancers. 2021; 13(18):4719. https://doi.org/10.3390/cancers13184719
Chicago/Turabian StyleMartini, Giulia, Davide Ciardiello, Fernando Paragliola, Valeria Nacca, Walter Santaniello, Fabrizio Urraro, Maria Stanzione, Marco Niosi, Marcello Dallio, Alessandro Federico, and et al. 2021. "How Immunotherapy Has Changed the Continuum of Care in Hepatocellular Carcinoma" Cancers 13, no. 18: 4719. https://doi.org/10.3390/cancers13184719
APA StyleMartini, G., Ciardiello, D., Paragliola, F., Nacca, V., Santaniello, W., Urraro, F., Stanzione, M., Niosi, M., Dallio, M., Federico, A., Selvaggi, F., Della Corte, C. M., Napolitano, S., Ciardiello, F., & Martinelli, E. (2021). How Immunotherapy Has Changed the Continuum of Care in Hepatocellular Carcinoma. Cancers, 13(18), 4719. https://doi.org/10.3390/cancers13184719