
Effect of Transarterial Chemoembolization on ALBI Grade in Intermediate-Stage Hepatocellular Carcinoma: Criteria for Unsuitable Cases Selection

 , and
, and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Transarterial Chemoembolization
2.3. Definitions
2.4. Follow-Up and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of the BCLC-B HCC Patients
3.2. Incidence of Acute and Chronic ALBI-Grade Migration after TACE
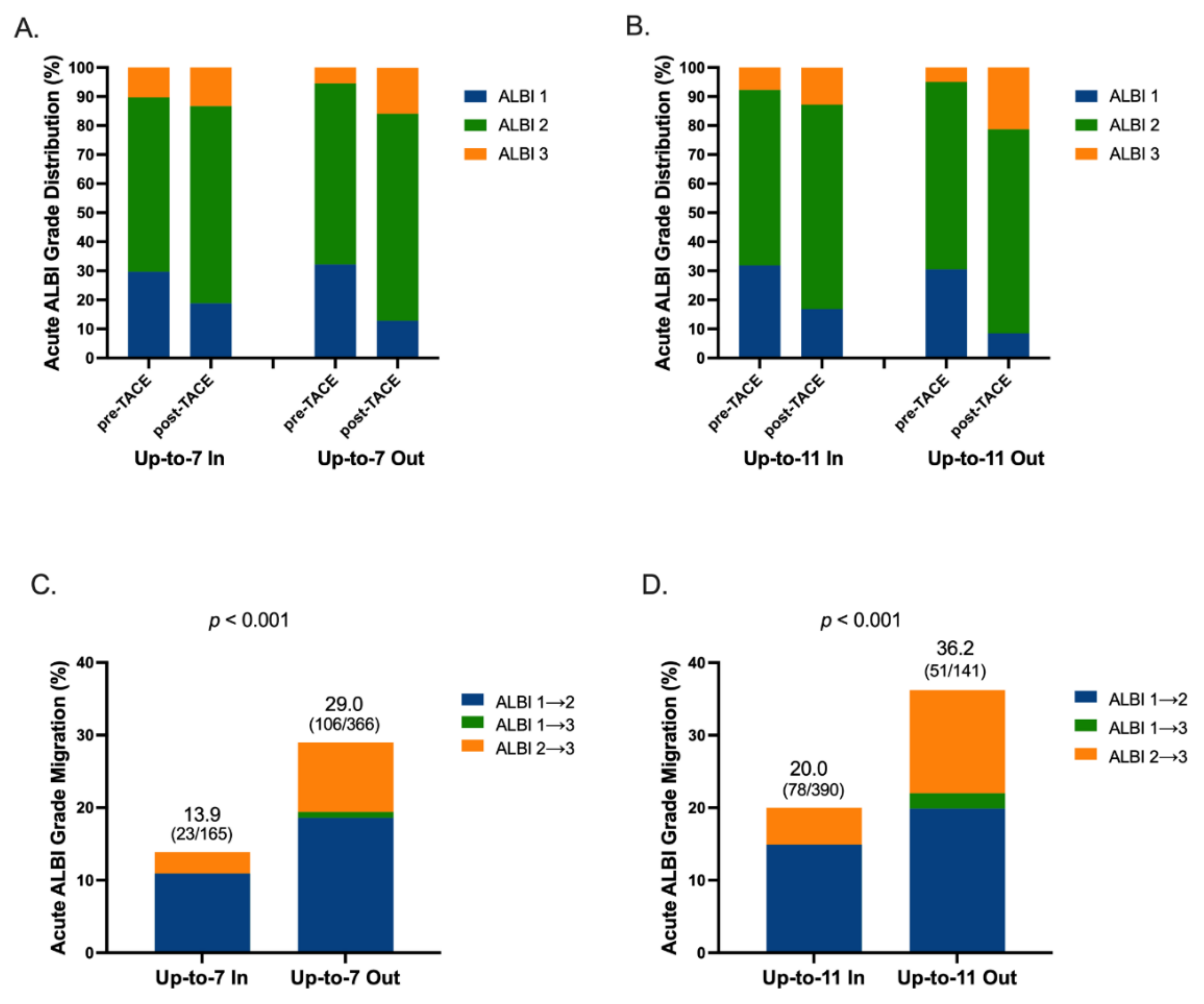
3.3. Distribution of ALBI Grade before and after TACE in Acute Phase by Different Tumor Size plus Tumor Number Criteria
3.4. Factors Associated with ALBI-Grade Migration in Acute Phase
3.5. Incidence of HBV Reactivation and HCV Hepatitis Flare after TACE
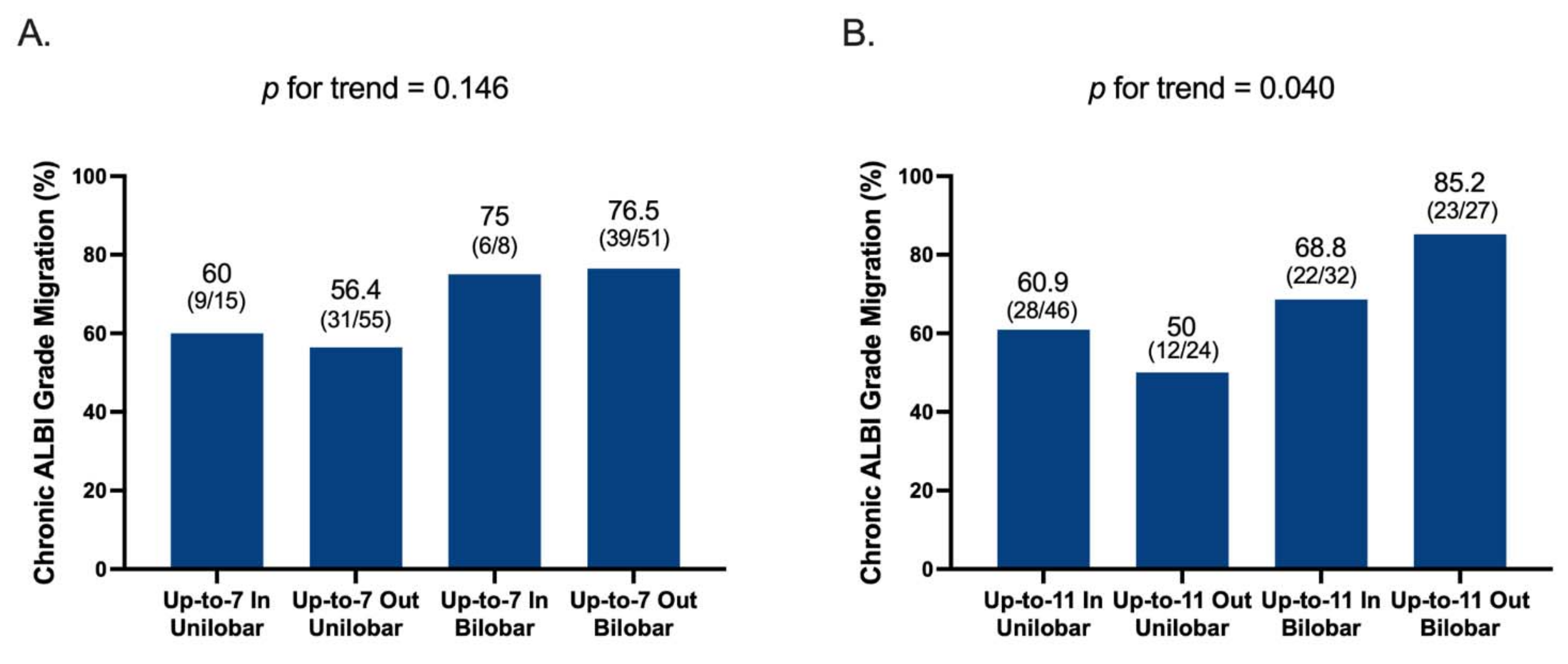
3.6. Factors of Chronic ALBI-Grade Migration in Patients with Acute ALBI Migration after TACE
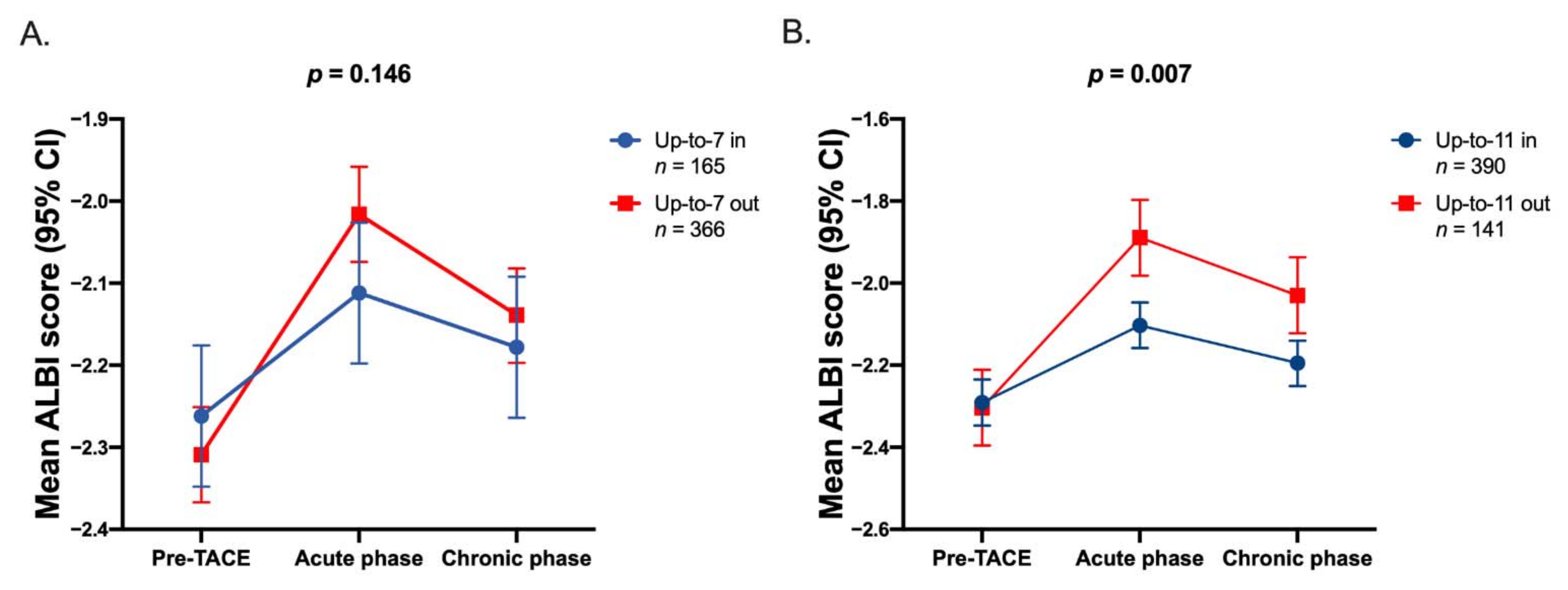
3.7. Dynamic Changes of ALBI Score after TACE
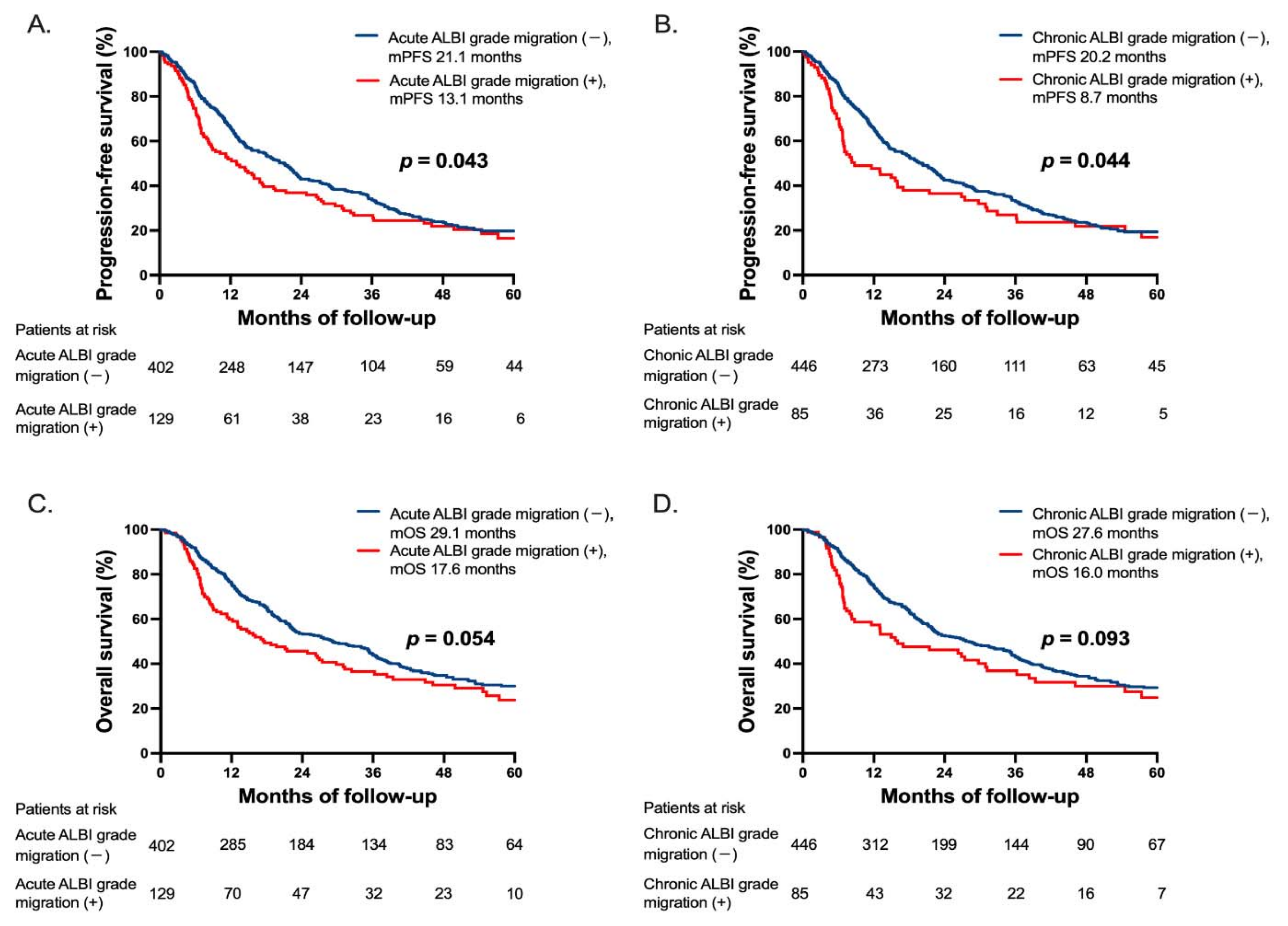
3.8. Progression-Free and Overall Survival Stratified by ALBI-Grade Migration
3.9. Prognostic Factors Associated with PFS and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villanueva, A. Hepatocellular carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ducreux, M.; Lencioni, R.; Di Bisceglie, A.; Galle, P.; Dufour, J. European Association for the Study of the Liver: European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar]
- Lo, C.-M.; Ngan, H.; Tso, W.-K.; Liu, C.-L.; Lam, C.-M.; Poon, R.T.-P.; Fan, S.-T.; Wong, J. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002, 35, 1164–1171. [Google Scholar] [CrossRef]
- Llovet, J.M.; Real, M.I.; Montaña, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Solà, R.; et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomised controlled trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef]
- Cammà, C.; Schepis, F.; Orlando, A.; Albanese, M.; Shahied, L.; Trevisani, F.; Andreone, P.; Craxi, A.; Cottone, M. Transarterial chemoembolization for unresectable hepatocellular carcinoma: Meta-analysis of randomized controlled trials. Radiology 2002, 224, 47–54. [Google Scholar] [CrossRef]
- Llovet, J.M.; Bruix, J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 2003, 37, 429–442. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-H.; Chen, C.-H.; Chang, T.-T.; Chen, S.-C.; Chiang, J.-H.; Lee, H.-S.; Lin, P.-W.; Huang, G.-T.; Sheu, J.-C.; Tsai, H.-M.; et al. The role of transcatheter arterial embolization for patients with unresectable hepatocellular carcinoma: A nationwide, multicentre study evaluated by cancer stage. Aliment. Pharmacol. Ther. 2005, 21, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-H.; Wu, J.-C.; Chen, S.-C.; Chen, C.-H.; Chiang, J.-H.; Huo, T.-I.; Lee, P.-C.; Chang, F.-Y.; Lee, S.-D. Survival benefit of transcatheter arterial chemoembolization in patients with hepatocellular carcinoma larger than 10 cm in diameter. Aliment. Pharmacol. Ther. 2005, 23, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.M.; Piscaglia, F.; Raoul, J.L.; Sangro, B.; Bolondi, L. Heterogeneity of patients with intermediate (BCLC B) hepatocellular carcinoma: Proposal for a subclassification to facilitate treatment decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef]
- Ha, Y.; Shim, J.H.; Kim, S.O.; Kim, K.M.; Lim, Y.S.; Lee, H.C. Clinical appraisal of the recently proposed Barcelona Clinic Liver Cancer stage B subclassification by survival analysis. J. Gastroenterol. Hepatol. 2014, 29, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, K.; Arii, S.; Ikai, I.; Omata, M.; Okita, K.; Ichida, T.; Matsuyama, Y.; Nakanuma, Y.; Kojiro, M.; Makuuchi, M.; et al. Prospective cohort study of transarterial chemoembolization for unresectable hepatocellular carcinoma in 8510 patients. Gastroenterology 2006, 131, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A changing paradigm for the treatment of intermediate-stage hepatocellular carcinoma: Asia-Pacific primary liver cancer expert consensus statements. Liver Cancer 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2008, 10, 35–43. [Google Scholar] [CrossRef]
- Giannini, E.G.; Moscatelli, A.; Pellegatta, G.; Vitale, A.; Farinati, F.; Ciccarese, F.; Piscaglia, F.; Rapaccini, G.L.; Di Marco, M.; Caturelli, E.; et al. Application of the intermediate-stage subclassification to patients with untreated hepatocellular carcinoma. Off. J. Am. Coll. Gastroenterol. 2016, 111, 70–77. [Google Scholar] [CrossRef]
- Weinmann, A.; Koch, S.; Sprinzl, M.; Kloeckner, R.; Schulze-Bergkamen, H.; Düber, C.; Lang, H.; Otto, G.; Wörns, M.A.; Galle, P.R. Survival analysis of proposed BCLC-B subgroups in hepatocellular carcinoma patients. Liver Int. 2015, 35, 591–600. [Google Scholar] [CrossRef]
- Biolato, M.; Gallusi, G.; Iavarone, M.; Cabibbo, G.; Racco, S.; De Santis, A.; Della Corte, C.; Maida, M.; Attili, A.F.; Sangiovanni, A.; et al. Prognostic ability of BCLC-B subclassification in patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Ann. Hepatol. 2018, 17, 110–118. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B stage hepatocellular carcinoma and treatment strategies: Proposal of modified Bolondi’s subclassification (Kinki criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef]
- Kim, J.H.; Shim, J.H.; Lee, H.C.; Sung, K.-B.; Ko, H.-K.; Ko, G.-Y.; Gwon, D.I.; Kim, J.W.; Lim, Y.-S.; Park, S.H. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017, 37, 1861–1868. [Google Scholar] [CrossRef]
- Kimura, H.; Ohkawa, K.; Miyazaki, M.; Sakakibara, M.; Imanaka, K.; Tamura, T.; Sueyoshi, H.; Takada, R.; Fukutake, N.; Uehara, H.; et al. Subclassification of patients with intermediate-stage (Barcelona Clinic Liver Cancer stage-B) hepatocellular carcinoma using the up-to-seven criteria and serum tumor markers. Hepatol. Int. 2017, 11, 105–114. [Google Scholar] [CrossRef]
- Lee, I.; Hung, Y.; Liu, C.; Lee, R.; Su, C.; Huo, T.; Li, C.; Chao, Y.; Lin, H.; Hou, M.; et al. A new ALBI-based model to predict survival after transarterial chemoembolization for BCLC stage B hepatocellular carcinoma. Liver Int. 2019, 39, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xia, D.; Bai, W.; Wang, E.; Sun, J.; Huang, M.; Mu, W.; Yin, G.; Li, H.; Zhao, H.; et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicentre observational study. J. Hepatol. 2019, 70, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach—The ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.-C.; Chen, Y.-T.; Chao, Y.; Huo, T.-I.; Li, C.-P.; Su, C.-W.; Lee, M.-H.; Hou, M.-C.; Lee, F.-Y.; Lin, H.-C.; et al. Validation of the albumin-bilirubin grade-based integrated model as a predictor for sorafenib-failed hepatocellular carcinoma. Liver Int. 2017, 38, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.-C.; Chao, Y.; Chen, M.-H.; Lan, K.-H.; Lee, C.-J.; Lee, I.-C.; Chen, S.-C.; Hou, M.-C.; Huang, Y.-H. Predictors of response and survival in immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. Cancers 2020, 12, 182. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.; Yuen, M.-F.; Hui, C.-K.; Tso, W.-K.; Lai, C.-L. A prospective study regarding the complications of transcatheter intraarterial lipiodol chemoembolization in patients with hepatocellular carcinoma. Cancer 2002, 94, 1747–1752. [Google Scholar] [CrossRef]
- Sun, Z.; Li, G.; Ai, X.; Luo, B.; Wen, Y.; Zhao, Z.; Dong, S.; Guan, J. Hepatic and biliary damage after transarterial chemoembolization for malignant hepatic tumors: Incidence, diagnosis, treatment, outcome and mechanism. Crit. Rev. Oncol. 2011, 79, 164–174. [Google Scholar] [CrossRef]
- Malagari, K.; Chatzimichael, K.; Alexopoulou, E.; Kelekis, A.; Hall, B.; Dourakis, S.; Delis, S.; Gouliamos, A.; Kelekis, D. Transarterial chemoembolization of unresectable hepatocellular carcinoma with drug eluting beads: Results of an open-label study of 62 patients. Cardiovasc. Interv. Radiol. 2007, 31, 269–280. [Google Scholar] [CrossRef]
- Min, Y.W.; Kim, J.; Kim, S.; Sung, Y.K.; Lee, J.H.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Koh, K.C.; Paik, S.W.; et al. Risk factors and a predictive model for acute hepatic failure after transcatheter arterial chemoembolization in patients with hepatocellular carcinoma. Liver Int. 2013, 33, 197–202. [Google Scholar] [CrossRef]
- Huang, Y.S.; Chiang, J.H.; Wu, J.C.; Chang, F.Y.; Lee, S.D. Risk of hepatic failure after transcatheter arterial chemoembolization for hepatocellular carcinoma: Predictive value of the monoethylglycinexylidide test. Am. J. Gastroenterol. 2002, 97, 1223–1227. [Google Scholar] [CrossRef]
- Marelli, L.; Stigliano, R.; Triantos, C.; Senzolo, M.; Cholongitas, E.; Davies, N.; Tibballs, J.; Meyer, T.; Patch, D.W.; Burroughs, A.K. Transarterial therapy for hepatocellular carcinoma: Which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc. Interv. Radiol. 2006, 30, 6–25. [Google Scholar] [CrossRef]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J. Hepatol. 2016, 66, 338–346. [Google Scholar] [CrossRef]
- Hung, Y.W.; Lee, I.C.; Chi, C.T.; Lee, R.C.; Liu, C.A.; Chiu, N.C.; Hwang, H.E.; Chao, Y.; Hou, M.C.; Huang, Y.H. Redefining tumor burden in patients with intermediate-stage hepatocellular carcinoma: The seven-eleven criteria. Liver Cancer 2021, 1–12. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Hwang, J.P.; Somerfield, M.R.; Alston-Johnson, D.E.; Cryer, D.R.; Feld, J.J.; Kramer, B.S.; Sabichi, A.L.; Wong, S.L.; Artz, A.S. Hepatitis B virus screening for patients with cancer before therapy: American Society of Clinical Oncology provisional clinical opinion update. J. Clin. Oncol. 2015, 33, 2212. [Google Scholar] [CrossRef]
- Lee, P.-C.; Chao, Y.; Chen, M.-H.; Lan, K.-H.; Lee, I.-C.; Hou, M.-C.; Huang, Y.-H. Risk of HBV reactivation in patients with immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. J. Immunother. Cancer 2020, 8, e001072. [Google Scholar] [CrossRef] [PubMed]
- Torres, H.A.; Hosry, J.; Mahale, P.; Economides, M.P.; Jiang, Y.; Lok, A.S. Hepatitis C virus reactivation in patients receiving cancer treatment: A prospective observational study. Hepatology 2017, 67, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 2019, 69, 1492–1501. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.-R.; Chen, Z.-H.; Liu, M.-M.; Lin, J.-X.; Zhang, X.-P.; Chen, J.; Lin, Q.; Ma, X.-K.; Wen, J.-Y.; Xie, S.-D.; et al. Modified CLIP score with the albumin-bilirubin grade retains prognostic value in HBV-related hepatocellular carcinoma patients treated with trans-catheter arterial chemoembolization therapy. J. Cancer 2018, 9, 2380–2388. [Google Scholar] [CrossRef]
- Kim, J.H.; Sinn, D.H.; Lee, J.H.; Hyun, D.; Cho, S.K.; Shin, S.W.; Chang, Y.; Kim, Y.J.; Yoon, J.H.; Kang, W.; et al. Novel albumin–bilirubin grade-based risk prediction model for patients with hepatocellular carcinoma undergoing chemoembolization. Dig. Dis. Sci. 2018, 63, 1062–1071. [Google Scholar] [CrossRef] [PubMed]
- Siriwardana, R.C.; Niriella, M.A.; Dassanayake, A.S.; Liyanage, C.A.H.; Upasena, A.; Sirigampala, C.; de Silva, H.J. Factors affecting post-embolization fever and liver failure after trans-arterial chemo-embolization in a cohort without background infective hepatitis-a prospective analysis. BMC Gastroenterol. 2015, 15, 96. [Google Scholar] [CrossRef]
- Boulin, M.; Adam, H.; Guiu, B.; Aho, L.S.; Cercueil, J.P.; Di Martino, C.; Fagnoni, P.; Minello, A.; Jouve, J.L.; Hillon, P.; et al. Predictive factors of transarterial chemoembolisation toxicity in unresectable hepatocellular carcinoma. Dig. Liver Dis. 2014, 46, 358–362. [Google Scholar] [CrossRef]
- Hsin, I.F.; Hsu, C.Y.; Huang, H.C.; Huang, Y.H.; Lin, H.C.; Lee, R.C.; Chiang, J.H.; Lee, F.Y.; Huo, T.I.; Lee, S.D. Liver failure after transarterial chemoembolization for patients with hepatocellular carcinoma and ascites: Incidence, risk factors, and prognostic prediction. J. Clin. Gastroenterol. 2011, 45, 556–562. [Google Scholar] [CrossRef]
- Jang, J.W.; Kwon, J.H.; You, C.R.; Kim, J.D.; Woo, H.Y.; Bae, S.H.; Choi, J.Y.; Yoon, S.K.; Chung, K.W. Risk of HBV reactivation according to viral status and treatment intensity in patients with hepatocellular carcinoma. Antivir. Ther. 2011, 16, 969–977. [Google Scholar] [CrossRef]
- Dan, J.-Q.; Zhang, Y.; Huang, J.; Chen, M.-S.; Gao, H.-J.; Peng, Z.-W.; Xu, L.; Lau, W. Hepatitis B virus reactivation after radiofrequency ablation or hepatic resection for HBV-related small hepatocellular carcinoma: A retrospective study. Eur. J. Surg. Oncol. (EJSO) 2013, 39, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.W.; Choi, J.Y.; Bae, S.H.; Kim, C.W.; Yoon, S.K.; Cho, S.H.; Yang, J.M.; Ahn, B.M.; Lee, C.D.; Lee, Y.S.; et al. Transarterial chemo-lipiodolization can reactivate hepatitis B virus replication in patients with hepatocellular carcinoma. J. Hepatol. 2004, 41, 427–435. [Google Scholar] [CrossRef]
- Jang, J.W.; Choi, J.Y.; Bae, S.H.; Yoon, S.K.; Chang, U.I.; Kim, C.W.; Cho, S.H.; Han, J.Y.; Lee, Y.S. A randomized controlled study of preemptive lamivudine in patients receiving transarterial chemo-lipiodolization. Hepatology 2006, 43, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Lao, X.-M.; Luo, G.; Ye, L.-T.; Luo, C.; Shi, M.; Wang, D.; Guo, R.; Chen, M.; Li, S.; Lin, X.; et al. Effects of antiviral therapy on hepatitis B virus reactivation and liver function after resection or chemoembolization for hepatocellular carcinoma. Liver Int. 2013, 33, 595–604. [Google Scholar] [CrossRef]
- Park, J.-W.; Park, K.W.; Cho, S.H.; Park, H.S.; Lee, W.J.; Lee, D.H.; Kim, C.-M. Risk of Hepatitis B exacerbation is low after transcatheter arterial chemoembolization therapy for patients with HBV-related hepatocellular carcinoma: Report of a prospective study. Am. J. Gastroenterol. 2005, 100, 2194–2200. [Google Scholar] [CrossRef]
- Hucke, F.; Pinter, M.; Graziadei, I.; Bota, S.; Vogel, W.; Müller, C.; Heinzl, H.; Waneck, F.; Trauner, M.; Peck-Radosavljevic, M.; et al. How to STATE suitability and START transarterial chemoembolization in patients with intermediate stage hepatocellular carcinoma. J. Hepatol. 2014, 61, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Chan, S.; Minami, T.; Chishina, H.; Aoki, T.; Takita, M.; Hagiwara, S.; Minami, Y.; Ida, H.; et al. Lenvatinib as an initial treatment in patients with intermediate-stage hepatocellular carcinoma beyond up-to-seven criteria and child-pugh a liver function: A proof-of-concept study. Cancers 2019, 11, 1084. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Tovoli, F.; Foerster, F.; Wörns, M.A.; Cucchetti, A.; Bolondi, L. The treatment of intermediate stage tumours beyond TACE: From surgery to systemic therapy. J. Hepatol. 2017, 67, 173–183. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Basic Characteristics | BCLC-B HCC |
|---|---|
| n = 531 | |
| Age (years), mean ± S.D. | 69.0 ± 12.3 |
| Gender, Male, n (%) | 412 (77.6) |
| HBsAg, Positive, n (%) | 244 (46.0) |
| Anti-HCV, Positive, n (%) | 180 (33.9) |
| Alcoholic, n (%) | 66 (12.4) |
| Cirrhosis, n (%) | 379 (71.4) |
| Platelet count (×104/μL), median (range) | 141 (22–601) |
| ALT (IU/L), median (range) | 46 (7–355) |
| AST (IU/L) †, median (range) | 54 (6–806) |
| INR, median (range) | 1.07 (0.85–14.50) |
| Albumin (g/dL), median (range) | 3.6 (2.1–4.9) |
| Total bilirubin (mg/dL), median (range) | 0.77 (0.19–3.79) |
| Child-Pugh class, A/B, n (%) | 459 (86.4)/72 (13.6) |
| ALBI grade, 1/2/3, n (%) | 167/327/37 (31.5/61.6/7.0) |
| Tumor size (cm), mean ± SD | 6.58 ± 3.72 |
| HBV-HCC (n = 220) | 7.05 ± 3.92 |
| HCV-HCC (n = 156) | 5.47 ± 2.93 |
| HBV-HCV-HCC (n = 24) | 6.21 ± 3.21 |
| Tumor location, Unilobar/Bilobar, n (%) | 273 (51.4)/258 (48.6) |
| Tumor number, ≥3/<3, n (%) | 269 (50.7)/262 (49.3) |
| Tumor size plus tumor number models | |
| Up-to-6, In/Out, n (%) | 83/448 (15.6/84.4) |
| Up-to-7, In/Out, n (%) | 165/366 (31.1/68.9) |
| Up-to-11, In/Out, n (%) | 390/141 (73.4/26.6) |
| Up-to-12, In/Out, n (%) | 424/107 (79.8/20.2) |
| AFP (ng/mL), median (range) | 50.33 (1.00–1,050,960.00) |
| Post-TACE ALBI Grade | Pre-TACE ALBI Grade | |||
|---|---|---|---|---|
| ALBI Grade 1 | ALBI Grade 2 | ALBI Grade 3 | ||
| Acute phase | ALBI Grade 1 | 78 (14.7%) | 0 | 0 |
| ALBI Grade 2 | 86 (16.2%) | 287 (54.0%) | 0 | |
| ALBI Grade 3 | 3 (0.6%) | 40 (7.5%) | 37 (7.0%) | |
| Chronic phase | ALBI Grade 1 | 103 (19.4%) | 0 | 0 |
| ALBI Grade 2 | 64 (12.1%) | 306 (57.6%) | 0 | |
| ALBI Grade 3 | 0 | 21 (3.9%) | 37 (7.0%) | |
| Factors | No. | Univariate | Multivariate | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| Age (years), >70/≤70 | 265/266 | 1.209 (0.812–1.798) | 0.350 | - | |||||||
| Gender, Male/Female | 412/119 | 1.446 (0.872–2.398) | 0.153 | - | |||||||
| HBV vs. HCV † | 220/156 | 2.092 (1.263–3.465) | 0.004 | 2.046 (1.232–3.399) | 0.006 | 1.968 (1.178–3.288) | 0.010 | 1.882 (1.125–3.146) | 0.016 | 2.061 (1.243–3.416) | 0.005 |
| Alcoholic, Yes/No | 66/465 | 1.196 (0.668–2.141) | 0.547 | - | |||||||
| Cirrhosis, Yes/No | 379/152 | 0.710 (0.464–1.086) | 0.114 | - | |||||||
| PLT (K), ≤120/>120 | 196/335 | 0.557 (0.360–0.862) | 0.009 | 0.830 (0.491–1.403) | 0.487 | 0.911 (0.533–1.557) | 0.733 | 0.883 (0.516–1.511) | 0.650 | 0.848 (0.498–1.446) | 0.545 |
| ALT (IU/L), >40/≤40 | 306/225 | 1.218 (0.812–1.827) | 0.340 | - | |||||||
| AST (IU/L) ‡, >45/≤45 | 325/205 | 1.462 (0.960–2.228) | 0.077 | 1.302 (0.774–2.190) | 0.320 | 1.230 (0.728–2.077) | 0.439 | 1.209 (0.710–2.056) | 0.485 | 1.271 (0.751–2.151) | 0.372 |
| INR, >1.0/≤1.0 | 427/104 | 1.440 (0.844–2.456) | 0.181 | - | |||||||
| Tumor location Bilobar/Unilobar | 258/273 | 0.860 (0.578–1.280) | 0.457 | - | |||||||
| Tumor size, per cm | 531 | 1.133 (1.075–1.193) | <0.001 | - | |||||||
| Tumor number, ≥3/<3 | 269/262 | 0.739 (0.497–1.101) | 0.138 | - | |||||||
| Up-to-6, Out/In | 448/83 | 1.881 (1.003–3.527) | 0.049 | 2.031 (0.952–4.330) | 0.067 | - | - | - | - | - | - |
| Up-to-7, Out/In | 366/165 | 2.517 (1.534–4.129) | <0.001 | - | - | 2.838 (1.567–5.141) | 0.001 | - | - | - | - |
| Up-to-11, Out/In | 141/390 | 2.267 (1.484–3.463) | <0.001 | - | - | - | - | 1.836 (1.095–3.080) | 0.021 | - | - |
| Up-to-12, Out/In | 107/424 | 1.907 (1.204–3.023) | 0.006 | - | - | - | - | - | - | 1.625 (0.919–2.875) | 0.095 |
| AFP (ng/mL), >400/≤400 | 149/382 | 1.686 (1.104–2.574) | 0.016 | 1.260 (0.756–2.100) | 0.376 | 1.181 (0.705–1.979) | 0.528 | 1.266 (0.759–2.111) | 0.367 | 1.316 (0.792–2.185) | 0.289 |
| Factors | No. | Univariate | |
|---|---|---|---|
| OR (95% CI) | p | ||
| Age (years), >70/≤70 | 69/60 | 0.816 (0.392–1.697) | 0.586 |
| Gender, Male/Female | 106/23 | 1.037 (0.402–2.675) | 0.940 |
| HBV vs. HCV † | 67/27 | 0.754 (0.287–1.981) | 0.567 |
| Alcoholic, Yes/No | 18/111 | 1.041 (0.362–2.991) | 0.940 |
| Cirrhosis, Yes/No | 85/44 | 0.621 (0.280–1.376) | 0.241 |
| PLT (K), ≤120/>120 | 35/94 | 1.180 (0.515–2.706) | 0.695 |
| ALT (IU/L), >40/≤40 | 79/50 | 0.635 (0.295–1.367) | 0.246 |
| AST (IU/L) ‡, >45/≤45 | 87/41 | 1.216 (0.558–2.648) | 0.623 |
| INR, >1.0/≤1.0 | 109/20 | 0.801 (0.285–2.253) | 0.674 |
| Tumor location, Bilobar/Unilobar | 59/70 | 2.411 (1.123–5.176) | 0.024 |
| Tumor size | |||
| >5 cm/≤5 cm | 98/31 | 1.083 (0.465–2.526) | 0.853 |
| >6 cm/≤6 cm | 85/44 | 0.999 (0.463–2.153) | 0.998 |
| >7 cm/≤7 cm | 65/64 | 1.024 (0.494–2.120) | 0.949 |
| >8 cm/≤8 cm | 51/78 | 1.225 (0.578–2.596) | 0.596 |
| >9 cm/≤9 cm | 46/83 | 1.513 (0.693–3.304) | 0.298 |
| >10 cm/≤10 cm | 34/95 | 1.338 (0.573–3.125) | 0.502 |
| >11 cm/≤11 cm | 26/103 | 1.949 (0.720–5.277) | 0.189 |
| Tumor number | |||
| >2 vs. ≤2 | 58/71 | 1.284 (0.615–2.682) | 0.506 |
| >3 vs. ≤3 | 45/84 | 0.906 (0.424–1.939) | 0.800 |
| AFP (ng/mL) | |||
| >20/≤20 | 84/45 | 0.948 (0.441–2.039) | 0.892 |
| >200/≤200 | 57/72 | 0.609 (0.292–1.268) | 0.185 |
| >400/≤400 | 47/82 | 0.646 (0.306–1.366) | 0.253 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chi, C.-T.; Lee, I.-C.; Lee, R.-C.; Hung, Y.-W.; Su, C.-W.; Hou, M.-C.; Chao, Y.; Huang, Y.-H. Effect of Transarterial Chemoembolization on ALBI Grade in Intermediate-Stage Hepatocellular Carcinoma: Criteria for Unsuitable Cases Selection. Cancers 2021, 13, 4325. https://doi.org/10.3390/cancers13174325
Chi C-T, Lee I-C, Lee R-C, Hung Y-W, Su C-W, Hou M-C, Chao Y, Huang Y-H. Effect of Transarterial Chemoembolization on ALBI Grade in Intermediate-Stage Hepatocellular Carcinoma: Criteria for Unsuitable Cases Selection. Cancers. 2021; 13(17):4325. https://doi.org/10.3390/cancers13174325
Chicago/Turabian StyleChi, Chen-Ta, I-Cheng Lee, Rheun-Chuan Lee, Ya-Wen Hung, Chien-Wei Su, Ming-Chih Hou, Yee Chao, and Yi-Hsiang Huang. 2021. "Effect of Transarterial Chemoembolization on ALBI Grade in Intermediate-Stage Hepatocellular Carcinoma: Criteria for Unsuitable Cases Selection" Cancers 13, no. 17: 4325. https://doi.org/10.3390/cancers13174325
APA StyleChi, C.-T., Lee, I.-C., Lee, R.-C., Hung, Y.-W., Su, C.-W., Hou, M.-C., Chao, Y., & Huang, Y.-H. (2021). Effect of Transarterial Chemoembolization on ALBI Grade in Intermediate-Stage Hepatocellular Carcinoma: Criteria for Unsuitable Cases Selection. Cancers, 13(17), 4325. https://doi.org/10.3390/cancers13174325