
Intra- and Extrathoracic Malignant Tracheoesophageal Fistula—A Differentiated Reconstructive Algorithm


 , , ,
, , ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Preoperative Evaluation
2.3. Intra- and Postoperative Airway Management
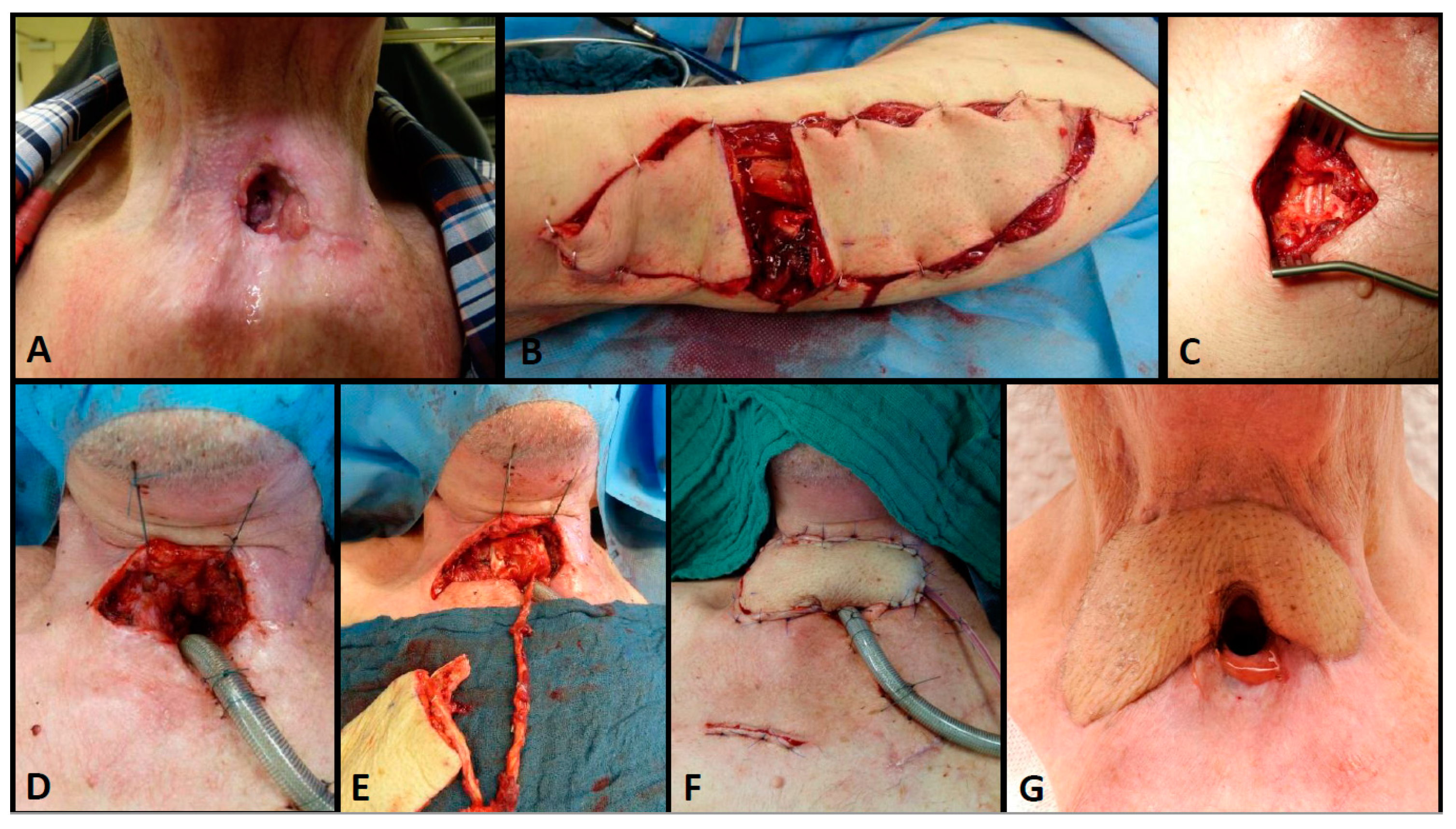
2.4. Operative Approach
2.5. Recipient Vessels in Free Flap Reconstructions
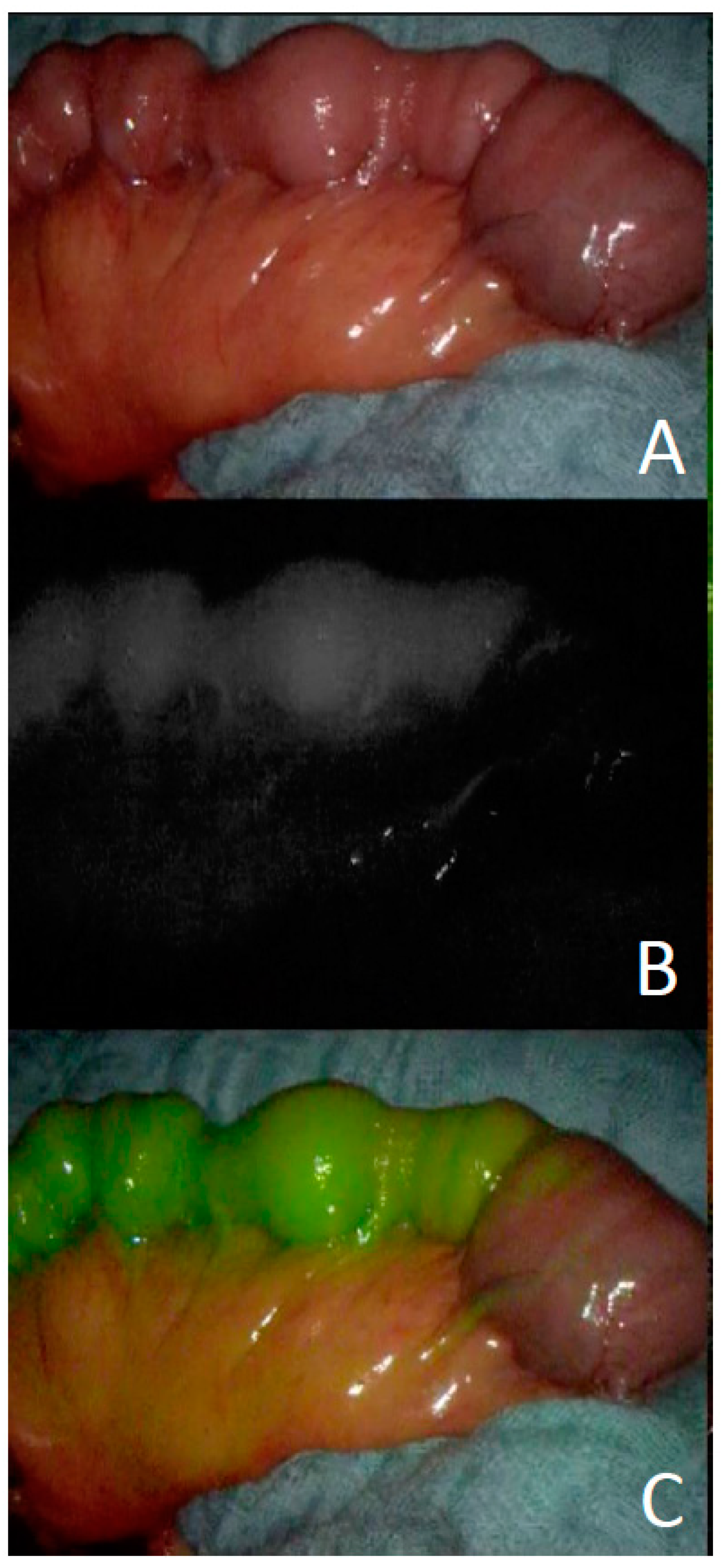
2.6. Intraoperative Perfusion Control of Flaps
2.7. Outcome Measurements
3. Results
Therapeutic Algorithm Derived from the Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strojan, P.; Hutcheson, K.; Eisbruch, A.; Beitler, J.J.; Langendijk, J.A.; Lee, A.W.; Corry, J.; Mendenhall, W.M.; Smee, R.; Rinaldo, A.; et al. Treatment of late sequelae after radiotherapy for head and neck cancer. Cancer Treat. Rev. 2017, 59, 79–92. [Google Scholar] [CrossRef] [Green Version]
- Al-Mamgani, A.; Van Rooij, P.H.; Mehilal, R.; Verduijn, G.M.; Tans, L.; Kwa, S.L.S. Radiotherapy for T1a glottic cancer: The influence of smoking cessation and fractionation schedule of radiotherapy. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Kikidis, D.; Vlastarakos, P.V.; Manolopoulos, L.; Yiotakis, I. Continuation of smoking after treatment of laryngeal cancer: An inde-pendent prognostic factor? ORL J. Otorhinolaryngol. Relat. Spec. 2012, 74, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.T.; Cartmel, B.; Kirsh, V.; Goodwin, W.J. Alcohol and Tobacco Use Prediagnosis and Postdiagnosis, and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity, Pharynx, and Larynx. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3368–3374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Imhoff, L.C.; Kranenburg, G.G.; Macco, S.; Nijman, N.L.; van Overbeeke, E.J.; Wegner, I.; Grolman, W.; Pothen, A.J. Prognostic value of continued smoking on survival and recurrence rates in patients with head and neck cancer: A systematic review. Head Neck 2016, 38 (Suppl. 1), E2214–E2220. [Google Scholar] [CrossRef] [PubMed]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge, H.M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [Green Version]
- Borras, J.M.; Barton, M.; Grau, C.; Corral, J.; Verhoeven, R.; Lemmens, V.; van Eycken, L.; Henau, K.; Primic-Zakelj, M.; Strojan, P.; et al. The impact of cancer incidence and stage on optimal utilization of radiotherapy: Methodology of a population based analysis by the ESTRO-HERO project. Radiother. Oncol. 2015, 116, 45–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirghani, H.; Leymarie, N.; Amen, F.; Qassemyar, Q.; Leclère, F.M.; Kolb, F. Pharyngotracheal fistula closure using the internal mammary artery perforator island flap. Laryngoscope 2013, 124, 1106–1111. [Google Scholar] [CrossRef]
- Shamji, F.M.; Inculet, R. Management of Malignant Tracheoesophageal Fistula. Thorac. Surg. Clin. 2018, 28, 393–402. [Google Scholar] [CrossRef]
- Serra, A.; Spinato, G.; Spinato, R.; Conti, A.; Licciardello, L.; Di Luca, M.; Campione, G.; Tonoli, G.; Politi, D.; Castro, V.; et al. Multicenter prospective crossover study on new prosthetic opportunities in post-laryngectomy voice rehabilitation. J. Boil. Regul. Homeost. Agents 2017, 31, 803–809. [Google Scholar]
- Stamatis, G.; Freitag, L. Tracheoesophageal fistula. Chirurg 2011, 82, 148–153. [Google Scholar] [CrossRef]
- Sevilla, G.M.A.; Suárez, F.V.; Rodrigo, T.J.P.; Llorente, P.J.L. El tubo de derivación salival de montgomery: Una solución sencilla para las fístulas faringocutáneas Montgomery salivary bypass tube: A simple solution for pharyngocutaneous fistulas. Acta Otorrinolaringol. Esp. 2006, 57, 467–470. [Google Scholar] [CrossRef]
- Chao, J.W.; Spector, J.A.; Taylor, E.M.; Otterburn, D.M.; Kutler, D.I.; Caruana, S.M.; Rohde, C.H. Pectoralis Major Myocutaneous Flap versus Free Fasciocutaneous Flap for Reconstruction of Partial Hypopharyngeal Defects: What Should We Be Doing? J. Reconstr. Microsurg. 2014, 31, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Xue, A.; Liu, J.; Hanasono, M.M.; Skoracki, R.J.; Chang, E.I.; Yu, P.; Selber, J.C. Pharyngoesophageal Reconstruction Outcomes Following 349 Cases. J. Reconstr. Microsurg. 2014, 30, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Hammoudeh, Z.S.; Gursel, E.; Baciewicz, F.A. Split Latissimus Dorsi Muscle Flap Repair of Acquired, Nonmalignant, Intrathoracic Tracheoesophageal and Bronchoesophageal Fistulas. Hear. Lung Circ. 2015, 24, e75–e78. [Google Scholar] [CrossRef] [PubMed]
- Blatter, J.; Krueger, T.; Ris, H.B.; Baeriswyl, M.; Lovis, A.; Zellweger, M.; Gonzalez, M.; Perentes, J.Y. Complex Tracheocarinal Recon-structions Using Extrathoracic Muscle Flaps as Airway Substitutes. Ann. Thorac. Surg. 2018, 105, 1492–1498. [Google Scholar] [CrossRef] [Green Version]
- Bertheuil, N.; Cusumano, C.; Meal, C.; Harnoy, Y.; Watier, E.; Meunier, B. Skin Perforator Flap Pedicled by Intercostal Muscle for Repair of a Tracheobronchoesophageal Fistula. Ann. Thorac. Surg. 2017, 103, e571–e573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marulli, G.; Loizzi, M.; Cardillo, G.; Battistella, L.; DE Palma, A.; Ialongo, P.; Zampieri, D.; Rea, F. Early and late outcome after surgical treatment of acquired non-malignant tracheo-oesophageal fistulae. Eur. J. Cardio-Thorac. Surg. 2013, 43, e155–e161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuda, T.; Makino, T.; Shiraishi, O.; Sogabe, S. Pedicled posterior pericardial repair of tracheoesophageal fistula after chemoradiotherapy for esophageal cancer. J. Thorac. Cardiovasc. Surg. 2016, 151, e95–e97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, E.H.; Castro, J.R.; Mojica, J.; Lazarus, C.L.; Su, H.K.; Alpert, E.H.; Dos Reis, L.L.; Urken, M.L. Reconstruction of expanding tra-cheoesophageal fistulae in post-radiation therapy patients who undergo total laryngectomy with a bipaddled radial forearm free flap: Report of 8 cases. Head Neck 2016, 38 (Suppl. 1), E172–E178. [Google Scholar] [CrossRef] [PubMed]
- Moradi, P.; Glass, G.E.; Atherton, D.D.; Eccles, S.; Coffey, M.; Majithia, A.; Speirs, A.J.; Clarke, P.M.; Wood, S.H. Reconstruction of phar-yngolaryngectomy defects using the jejunal free flap: A 10-year experience from a single reconstructive center. Plast. Reconstr. Surg. 2010, 126, 1960–1966. [Google Scholar] [CrossRef]
- Perez-Smith, D.; Wagels, M.; Theile, D.R. Jejunal free flap reconstruction of the pharyngolaryngectomy defect: 368 Consecutive cases. J. Plast. Reconstr. Aesthetic Surg. 2013, 66, 9–15. [Google Scholar] [CrossRef]
- Wreesmann, V.B.; Smeele, L.E.; Hilgers, F.J.M.; Lohuis, P.J.F.M. Closure of tracheoesophageal fistula with prefabricated revascularized bilaminar radial forearm free flap. Head Neck 2009, 31, 838–842. [Google Scholar] [CrossRef]
- Kremer, T.; Cordts, T.; Hirche, C.; Hernekamp, F.; Radu, C.; Kneser, U. Reconstruction of Defects after Oncologic Resection and Radiation—Indications for Microsurgical Reconstruction. Handchir. Mikrochir. Plast. Chir. 2015, 47, 353–358. [Google Scholar]
- Grebenik, C. ANAESTHETIC MANAGEMENT OF MALIGNANT TRACHEO—OESOPHAGEAL FISTULA. Br. J. Anaesth. 1989, 63, 492–496. [Google Scholar] [CrossRef] [Green Version]
- Dartevelle, P.; Macchiarini, P. Management of acquired tracheoesophageal fistula. Chest Surg. Clin. N. Am. 1996, 6, 819–836. [Google Scholar]
- Ichinose, M.; Sakai, H.; Miyazaki, I.; Muraoka, A.; Aizawa, M.; Igarashi, K.; Okazaki, A. Independent lung ventilation combined with HFOV for a patient suffering from tra-cheo-gastric roll fistula. J. Anesth. 2008, 22, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Karampinis, I.; Ronellenfitsch, U.; Mertens, C.; Gerken, A.; Hetjens, S.; Post, S.; Kienle, P.; Nowak, K. Indocyanine green tissue angiography affects anastomotic leakage after esophagectomy. A retrospective, case-control study. Int. J. Surg. 2017, 48, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Nowak, K.; Karampinis, I.; Gerken, A.L.H. Application of Fluorescent Dyes in Visceral Surgery: State of the Art and Future Per-spectives. Visc. Med. 2020, 36, 80–87. [Google Scholar] [CrossRef]
- Bigdeli, A.K.; Thomas, B.; Falkner, F.; Gazyakan, E.; Hirche, C.; Kneser, U. The Impact of Indocyanine-Green Fluorescence Angi-ography on Intraoperative Decision-Making and Postoperative Outcome in Free Flap Surgery. J. Reconstr. Microsurg. 2020, 36, 556–566. [Google Scholar] [PubMed]
- McCombe, A.W.; Jones, A.S. Radiotherapy and complications of laryngectomy. J. Laryngol. Otol. 1993, 107, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.J.; Lee, P.; Foo, A.Z.X.; Tan, E.H.; Ong, H.S.; Hsu, A.A.L. Characteristics and Outcomes of Airway Involvement in Esophageal Cancer. Ann. Thorac. Surg. 2021, 112, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Geyer, M.; Tan, N.; Ismail-Koch, H.; Puxeddu, R. A simple closure technique for reversal of tracheoesophageal puncture. Am. J. Otolaryngol. 2011, 32. [Google Scholar] [CrossRef] [PubMed]
- Ariyan, S. Further experiences with the pectoralis major myocutaneous flap for the immediate repair of defects from excisions of head and neck cancers. Plast. Reconstr. Surg. 1979, 64, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Anehosur, V.; Dikhit, P.S.; Nagraj, N.; Jayade, B.; Kumar, N. PMMC Flap Revisited and its Clinical Outcome in 150 Patients. J. Maxillofac. Oral Surg. 2020, 19, 26–31. [Google Scholar] [CrossRef]
- Sharaf, B.; Xue, A.; Solari, M.G.; Boa, O.; Liu, J.; Hanasono, M.M.; Skoracki, R.; Yu, P.; Selber, J.C. Optimizing Outcomes in Pharyn-goesophageal Reconstruction and Neck Resurfacing: 10-Year Experience of 294 Cases. Plast. Reconstr. Surg. 2017, 139, 105e–119e. [Google Scholar] [CrossRef]
- Ciudad, P.; Agko, M.; Date, S.; Chang, W.-L.; Manrique, O.J.; Huang, T.C.T.; Torto, F.L.; Trignano, E.; Chen, H.-C. The radial forearm free flap as a “vascular bridge” for secondary microsurgical head and neck reconstruction in a vessel-depleted neck. Microsurgery 2018, 38, 651–658. [Google Scholar] [CrossRef]
- Henn, D.; AbouArab, M.H.; Hirche, C.; Hernekamp, J.F.; Schmidt, V.J.; Kneser, U.; Kremer, T. Sequential chimeric medial femoral condyle and anterolateral thigh flow-through flaps for one-stage reconstructions of composite bone and soft tissue defects: Report of three cases. Microsurgery 2017, 37, 824–830. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Percent | ||
|---|---|---|---|
| Age (Years) | 67.1 ± 7.0 | ||
| Sex | Female | 3 | 17% |
| Male | 15 | 83% | |
| Tumor location | Esophagus | 11 | 61% |
| Larynx | 3 | 17% | |
| Pharynx | 1 | 5% | |
| Hypopharynx | 3 | 17% | |
| Fistula classification | Cervical | 9 | 50% |
| Cervico-thoracic | 4 | 22% | |
| Intrathoracic | 5 | 28% | |
| Radiation | Yes | 17 | 95% |
| No | 1 | 5% | |
| Patient-No. | Localization of TEF | Malignancy | 1st Recon. | 2nd Recon. | 3rd Recon. | Success of Recon. | 30-Day Survival |
|---|---|---|---|---|---|---|---|
| 1 | Cervical | Esophageal | Jejunum | - | - | Yes | Yes |
| 2 | Laryngeal | Jejunum | - | - | Yes | Yes | |
| 3 | Esophageal | None | - | - | No | No | |
| 4 | Laryngeal | PM | Jejunum | - | Yes | Yes | |
| 5 | Hypopharyngeal | Split-ALT | - | - | Yes | Yes | |
| 6 | Laryngeal | Split-ALT | - | - | Yes | Yes | |
| 7 | Hypopharyngeal | PM | ALT | ALT/AMT | Yes | Yes | |
| 8 | Pharyngeal | ALT/Jejunum | - | - | Yes | Yes | |
| 9 | Hypopharyngeal | ALT/Jejunum | - | - | Yes | Yes | |
| 10 | Cervico-thoracic | Esophageal | Discont. Resection Sterno-cleido. | - | - | Yes | Yes |
| 11 | Esophageal | ICM | ALT | - | No | Yes | |
| 12 | Esophageal | Discont. Resection ICM | Sterno-cleido. | Gastric pull-up | Yes | Yes | |
| 13 | Esophageal | None | - | - | No | Yes | |
| 14 | Intrathoracic | Esophageal | Discont. Resection ICM | Gastric pull-up | Yes | Yes | |
| 15 | Esophageal | ICM | LD | - | Yes | No | |
| 16 | Esophageal | ICM | - | - | Yes | Yes | |
| 17 | Esophageal | ICM | - | - | Yes | Yes | |
| 18 | Esophageal | ICM | - | - | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kremer, T.; Gazyakan, E.; Maurer, J.T.; Ott, K.; Gerken, A.; Schmittner, M.; Ronellenfitsch, U.; Kneser, U.; Nowak, K. Intra- and Extrathoracic Malignant Tracheoesophageal Fistula—A Differentiated Reconstructive Algorithm. Cancers 2021, 13, 4329. https://doi.org/10.3390/cancers13174329
Kremer T, Gazyakan E, Maurer JT, Ott K, Gerken A, Schmittner M, Ronellenfitsch U, Kneser U, Nowak K. Intra- and Extrathoracic Malignant Tracheoesophageal Fistula—A Differentiated Reconstructive Algorithm. Cancers. 2021; 13(17):4329. https://doi.org/10.3390/cancers13174329
Chicago/Turabian StyleKremer, Thomas, Emre Gazyakan, Joachim T. Maurer, Katja Ott, Andreas Gerken, Marc Schmittner, Ulrich Ronellenfitsch, Ulrich Kneser, and Kai Nowak. 2021. "Intra- and Extrathoracic Malignant Tracheoesophageal Fistula—A Differentiated Reconstructive Algorithm" Cancers 13, no. 17: 4329. https://doi.org/10.3390/cancers13174329
APA StyleKremer, T., Gazyakan, E., Maurer, J. T., Ott, K., Gerken, A., Schmittner, M., Ronellenfitsch, U., Kneser, U., & Nowak, K. (2021). Intra- and Extrathoracic Malignant Tracheoesophageal Fistula—A Differentiated Reconstructive Algorithm. Cancers, 13(17), 4329. https://doi.org/10.3390/cancers13174329