
Cultural and Ethical Barriers to Cancer Treatment in Nursing Homes and Educational Strategies: A Scoping Review

 ,
, {kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Definitions
3. Results
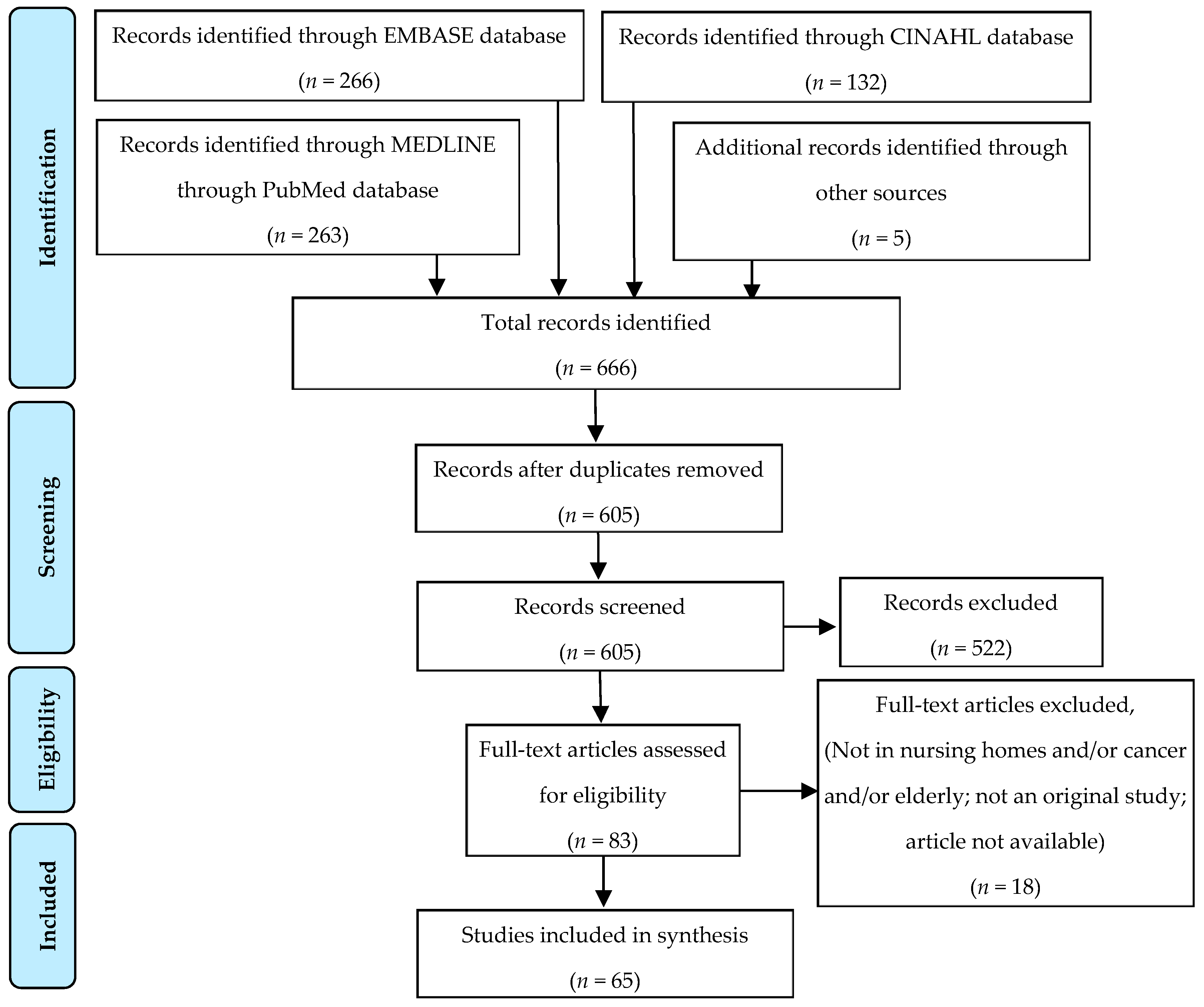
3.1. Database Search
3.2. Testing
3.2.1. Screening
Screening Habits in Nursing Homes
Cancer Screening
Role of the Nurse
3.2.2. Diagnosis
Unstaged or Late Disease
Physicians’ Motivation for Non-Referral
3.3. Treatment
3.3.1. Patient Profiles
Prevalence and Particularities of Nursing Home Residents with Cancer
Risk Factors for Long-Term Care Use
3.3.2. Cancer Management in Nursing Homes
3.3.3. Treatment Outcomes
Breast Cancer Treatment
Colorectal Cancer Treatment
3.3.4. Shared Medical Decision
3.4. Symptoms
3.4.1. Physical Symptoms
3.4.2. Impacts of Cognitive Impairment
3.4.3. Pain Management
3.4.4. Severity of Pain
3.4.5. Neuropsychiatric Symptoms
3.4.6. Role of the Nurse in Psychological Symptoms
3.5. Advanced Care Planning (ACP)
3.5.1. Do-Not-Resuscitate Wishes
3.5.2. Trajectory of Disease as Guide for ACP
3.5.3. Implication of Nurses
3.6. End of Life
3.6.1. Places for Death
3.6.2. Caring
3.7. Nursing Home Care
3.7.1. Deprescription
3.7.2. Transitions between Acute and Long-Term Care
3.7.3. Quality Indicators
3.8. Education
3.8.1. Facilitators of Continuing Education
3.8.2. Educational Strategies: Training Programs and Problem-Based Learning
Training Programs
Problem-Based Learning
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yancik, R. Cancer in Older Persons: An International Issue in an Aging World. Semin. Oncol. 2004, 31, 128–136. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Hurria, A.; Hortobagyi, G.N.; Buchholz, T.A. Future of Cancer Incidence in the United States: Burdens Upon an Aging, Changing Nation. J. Clin. Oncol. 2009, 27, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, S.M. Therapy Insight: Therapeutic Challenges in the Treatment of Elderly Cancer Patients. Nat. Rev. Clin. Oncol. 2006, 3, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Yellen, S.B.; Cella, D.F.; Leslie, W.T. Age and Clinical Decision Making in Oncology Patients. JNCI J. Natl. Cancer Inst. 1994, 86, 1766–1770. [Google Scholar] [CrossRef] [PubMed]
- Cook, P.S.; McCarthy, A.L. Cancer Treatment Decision-Making with/for Older Adults with Dementia: The Intersections of Autonomy, Capital, and Power. Health Sociol. Rev. 2018, 27, 184–198. [Google Scholar] [CrossRef]
- Martin, C.; Shrestha, A.; Burton, M.; Collins, K.; Wyld, L. How Are Caregivers Involved in Treatment Decision Making for Older People with Dementia and a New Diagnosis of Cancer? Psycho-oncology 2019, 28, 1197–1206. [Google Scholar] [CrossRef]
- McWilliams, L.; Farrell, C.; Keady, J.; Swarbrick, C.; Burgess, L.; Grande, G.; Bellhouse, S.; Yorke, J. Cancer-Related Information Needs and Treatment Decision-Making Experiences of People with Dementia in England: A Multiple Perspective Qualitative Study. BMJ Open 2018, 8, e020250. [Google Scholar] [CrossRef]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Trico, A.; Khalil, H. Chapter 11: Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- PROSPERO: International Prospective Register of Systematic Reviews. Scoping Reviews. Available online: https://www.crd.york.ac.uk/prospero/#aboutregpage (accessed on 14 October 2020).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- NIH National Institute on Aging : What Is Long-Term Care? Available online: http://www.nia.nih.gov/health/what-long-term-care (accessed on 8 October 2020).
- NIH National Institute on Aging : What Are Palliative Care and Hospice Care? Available online: https://www.nia.nih.gov/health/what-are-palliative-care-and-hospice-care (accessed on 10 October 2020).
- Rudel, R.J. On Breast Cancer Detection, Directors of Nursing and Female Residents: A Study in Rural Long-Term Care. Online J. Rural. Nurs. Health Care 2007, 7, 21–35. [Google Scholar] [CrossRef]
- Yadav, N.R.; Jain, M.; Sharma, A.; Yadav, R.; Pahuja, M.; Jain, V. Distribution and Prevalence of Oral Mucosal Lesions in Residents of Old Age Homes in Delhi, India. Nepal J. Epidemiol. 2018, 8, 727–734. [Google Scholar] [CrossRef]
- Christos, P.J.; Oliveria, S.A.; Mâsse, L.C.; McCormick, L.K.; Halpern, A.C. Skin Cancer Prevention and Detection by Nurses: Attitudes, Perceptions, and Barriers. J. Cancer Educ. 2004, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Darjani, A.; Alizadeh, N.; Rafiei, E.; Moulaei, M.; Alavi, S.H.N.; Eftekhari, H.; Rafiei, R.; Gharaei-Nejad, K.; Mohtasham-Amiri, Z. Skin Diseases among the Old Age Residents in a Nursing Home: A Neglected Problem. Dermatol. Res. Pract. 2020, 8849355. [Google Scholar] [CrossRef]
- Bradley, C.J.; Clement, J.P.; Lin, C. Absence of Cancer Diagnosis and Treatment in Elderly Medicaid-Insured Nursing Home Residents. J. Natl. Cancer Inst. 2008, 100, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Clement, J.P.; Bradley, C.J.; Lin, C. Organizational Characteristics and Cancer Care for Nursing Home Residents. Health Serv. Res. 2009, 44, 1983–2003. [Google Scholar] [CrossRef] [Green Version]
- Koroukian, S.M.; Xu, F.; Beaird, H.; Diaz, M.; Murray, P.; Rose, J.H. Complexity of Care Needs and Unstaged Cancer in Elders: A Population-Based Study. Cancer Detect. Prev. 2007, 31, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Hamaker, M.E.; Hamelinck, V.C.; van Munster, B.C.; Bastiaannet, E.; Smorenburg, C.H.; Achterberg, W.P.; Liefers, G.-J.; de Rooij, S.E. Nonreferral of Nursing Home Patients with Suspected Breast Cancer. J. Am. Med. Dir. Assoc. 2012, 13, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Wildiers, H.; Mauer, M.; Elseviers, M.; De Wolf, J.; Hatse, S.; Hamaker, M.; Buntinx, F.; De Lepeleire, J.; Uytterschaut, G.; Falandry, C.; et al. Cancer Events in Belgian Nursing Home Residents: An EORTC Prospective Cohort Study. J. Geriatr. Oncol. 2019, 10, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Blytt, K.M.; Selbæk, G.; Drageset, J.; Natvig, G.K.; Husebo, B.S. Comorbid Dementia and Cancer in Residents of Nursing Homes: Secondary Analyses of a Cross-Sectional Study. Cancer Nurs. 2018, 41, E13–E20. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, R.J.; Barkley, J.; Wang, S.; Kim, M. Analyses of Nursing Home Residents with Cancer at Admission. Cancer Nurs. 2005, 28, 406–414. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Ranhoff, A.H. Cancer in Nursing Homes: Characteristics and Health-Related Quality of Life among Cognitively Intact Residents with and without Cancer. Cancer Nurs. 2012, 35, 295–301. [Google Scholar] [CrossRef]
- Liuu, E.; Guyot, N.; Valero, S.; Jamet, A.; Ouazzani, H.E.; Bouchaert, P.; Tourani, J.; Migeot, V.; Paccalin, M. Prevalence of Cancer and Management in Elderly Nursing Home Residents. A Descriptive Study in 45 French Nursing Homes. Eur. J. Cancer Care 2019, 28, e12957. [Google Scholar] [CrossRef]
- Williams, G.R.; Dunham, L.; Chang, Y.; Deal, A.M.; Pergolotti, M.; Lund, J.L.; Guerard, E.J.; Kenzik, K.; Muss, H.B.; Sanoff, H.K. Geriatric Assessment to Predict Hospitalization Frequency and Long-Term Care Utilization in Older Adult Cancer Survivors. J. Clin. Oncol. 2018, 36, 10036. [Google Scholar] [CrossRef]
- Muss, H.B. Adjuvant Chemotherapy in Older and Younger Women With Lymph Node–Positive Breast Cancer. JAMA 2005, 293, 1073–1081. [Google Scholar] [CrossRef]
- Tang, V.; Zhao, S.; Boscardin, J.; Sudore, R.; Covinsky, K.; Walter, L.C.; Esserman, L.; Mukhtar, R.; Finlayson, E. Functional Status and Survival After Breast Cancer Surgery in Nursing Home Residents. JAMA Surg. 2018, 153, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, E.; Zhao, S.; Boscardin, W.J.; Fries, B.E.; Landefeld, C.S.; Dudley, R.A. Functional Status after Colon Cancer Surgery in Elderly Nursing Home Residents. J. Am. Geriatr. Soc. 2012, 60, 967–973. [Google Scholar] [CrossRef]
- Chan, T.Y.; Foo, C.C.; Law, W.L.; Lo, O. Outcomes of Colorectal Cancer Surgery in the Nonagenarians: 20-Year Result from a Tertiary Center. BMC Surg. 2019, 19, 155. [Google Scholar] [CrossRef] [PubMed]
- Finlayson, E.; Zhao, S.; Varma, M.G. Outcomes after Rectal Cancer Surgery in Elderly Nursing Home Residents. Dis. Colon. Rectum. 2012, 55, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Bern-Klug, M.; Singh, J.; Liu, J.; Shinkunas, L. Prospect Theory Concepts Applied to Family Members of Nursing Home Residents with Cancer: A Good Ending Is a Gain. J. Soc. Work. End Life Palliat. Care 2019, 15, 34–54. [Google Scholar] [CrossRef]
- Duncan, J.G.; Bott, M.J.; Thompson, S.A.; Gajewski, B.J. Symptom Occurrence and Associated Clinical Factors in Nursing Home Residents with Cancer. Res. Nurs. Health 2009, 32, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Monroe, T.; Carter, M.; Feldt, K.; Tolley, B.; Cowan, R.L. Assessing Advanced Cancer Pain in Older Adults with Dementia at the End-of-Life. J. Adv. Nurs. 2012, 68, 2070–2078. [Google Scholar] [CrossRef] [Green Version]
- Lukas, A.; Mayer, B.; Fialová, D.; Topinkova, E.; Gindin, J.; Onder, G.; Bernabei, R.; Nikolaus, T.; Denkinger, M.D. Pain Characteristics and Pain Control in European Nursing Homes: Cross-Sectional and Longitudinal Results from the Services and Health for Elderly in Long TERm Care (SHELTER) Study. J. Am. Med. Dir. Assoc. 2013, 14, 421–428. [Google Scholar] [CrossRef]
- Dubé, C.E.; Mack, D.S.; Hunnicutt, J.N.; Lapane, K.L. Cognitive Impairment and Pain Among Nursing Home Residents With Cancer. J. Pain Symptom Manag. 2018, 55, 1509–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monroe, T.B.; Carter, M.A.; Feldt, K.S.; Dietrich, M.S.; Cowan, R.L. Pain and Hospice Care in Nursing Home Residents with Dementia and Terminal Cancer. Geriatr. Gerontol. Int. 2013, 13, 1018–1025. [Google Scholar] [CrossRef] [Green Version]
- Sørbye, L.W.; Steindal, S.A.; Kalfoss, M.H.; Vibe, O.E. Opioids, Pain Management, and Palliative Care in a Norwegian Nursing Home From 2013 to 2018. Health Serv. Insights 2019, 12, 1178632919834318. [Google Scholar] [CrossRef] [Green Version]
- Hunnicutt, J.N.; Tjia, J.; Lapane, K.L. Hospice Use and Pain Management in Elderly Nursing Home Residents With Cancer. J. Pain Symptom Manag. 2017, 53, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.-H.; Hunnicutt, J.N.; Ulbricht, C.M.; Dubé, C.E.; Hume, A.L.; Lapane, K.L. Adjuvant Use and the Intensification of Pharmacologic Management for Pain in Nursing Home Residents with Cancer: Data from a US National Database. Drugs Aging 2019, 36, 549–557. [Google Scholar] [CrossRef]
- Teno, J.M.; Kabumoto, G.; Wetle, T.; Roy, J.; Mor, V. Daily Pain That Was Excruciating at Some Time in the Previous Week: Prevalence, Characteristics, and Outcomes in Nursing Home Residents. J. Am. Geriatr. Soc. 2004, 52, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, C.B.; Briesacher, B.A.; Gurwitz, J.H.; Rosen, A.B.; Pimentel, M.T.; Lapane, K.L. Pain Management in Nursing Home Residents with Cancer. J. Am. Geriatr. Soc. 2015, 63, 633–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, P.H. The Pain of Residents with Terminal Cancer in USA Nursing Homes: Family Members’ Perspectives. Int. J. Palliat. Nurs. 2007, 13, 20–27. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Dysvik, E.; Furnes, B.; Hauge, S. Loneliness, Loss, and Social Support among Cognitively Intact Older People with Cancer, Living in Nursing Homes—A Mixed-Methods Study. Clin. Interv. Aging 2015, 10, 1529–1536. [Google Scholar] [CrossRef] [Green Version]
- Drageset, J.; Eide, G.E.; Kirkevold, M.; Ranhoff, A.H. Emotional Loneliness Is Associated with Mortality among Mentally Intact Nursing Home Residents with and without Cancer: A Five-Year Follow-up Study. J. Clin. Nurs. 2013, 22, 106–114. [Google Scholar] [CrossRef]
- Drageset, J.; Eide, G.E.; Ranhoff, A.H. Anxiety and Depression and Mortality among Cognitively Intact Nursing Home Residents with and without a Cancer Diagnosis: A 5-Year Follow-up Study. Cancer Nurs. 2013, 36, E68–E74. [Google Scholar] [CrossRef]
- Reblin, M.; Clayton, M.F.; Xu, J.; Hulett, J.M.; Latimer, S.; Donaldson, G.W.; Ellington, L. Caregiver, Patient, and Nurse Visit Communication Patterns in Cancer Home Hospice. Psycho-oncology 2017, 26, 2285–2293. [Google Scholar] [CrossRef] [PubMed]
- Godino, C.; Jodar, L.; Durán, Á.; Martínez, I.; Schiaffino, A. Nursing Education as an Intervention to Decrease Fatigue Perception in Oncology Patients. Eur. J. Oncol. Nurs. 2006, 10, 150–155. [Google Scholar] [CrossRef]
- Tseng, Y.-P.; Huang, L.-H.; Huang, T.-H.; Hsu, L.-L.; Hsieh, S.-I. Factors Associated With the Do-Not-Resuscitate Decision Among Surrogates of Elderly Residents at a Nursing Home in Taiwan. Int. J. Gerontol. 2017, 11, 95–99. [Google Scholar] [CrossRef]
- Dobalian, A.; Tsao, J.C.I.; Radcliff, T.A. Diagnosed Mental and Physical Health Conditions in the United States Nursing Home Population: Differences between Urban and Rural Facilities. J. Rural. Health 2003, 19, 477–483. [Google Scholar] [CrossRef]
- Brink, P. Examining Do-Not-Resuscitate Orders Among Newly Admitted Residents of Long-Term Care Facilities. Palliat. Care 2014, 8, PCRT-S13042. [Google Scholar] [CrossRef] [Green Version]
- Bai, Q.; Zhang, Z.; Lu, X.; Shi, Y.; Liu, X.; Chan, H. Attitudes towards Palliative Care among Patients and Health Professionals in Henan, China. Prog. Palliat. Care 2010, 18, 341–345. [Google Scholar] [CrossRef]
- Lawrence, S.; Robinson, A.; Eagar, K. Identification of the Trajectory of Functional Decline for Advance Care Planning in a Nursing Home Population. Australas. J. Ageing 2017, 36, E14–E20. [Google Scholar] [CrossRef] [PubMed]
- Epstein, A.S.; Desai, A.V.; Bernal, C.; Romano, D.; Wan, P.J.; Okpako, M.; Anderson, K.; Chow, K.; Kramer, D.; Calderon, C.; et al. Giving Voice to Patient Values Throughout Cancer: A Novel Nurse-Led Intervention. J. Pain Symptom Manag. 2019, 58, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Walling, A.M.; D’Ambruoso, S.F.; Malin, J.L.; Hurvitz, S.; Zisser, A.; Coscarelli, A.; Clarke, R.; Hackbarth, A.; Pietras, C.; Watts, F.; et al. Effect and Efficiency of an Embedded Palliative Care Nurse Practitioner in an Oncology Clinic. J. Oncol. Pract. 2017, 13, e792–e799. [Google Scholar] [CrossRef]
- Dyason, C.; Simon, J.; Wityk Martin, T.L. Advance Care Planning Discussions among Residents of Long Term Care and Designated Assisted Living: Experience from Calgary, Alberta. BMJ Support. Palliat. Care 2015, 5, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Dobalian, A. Advance Care Planning Documents in Nursing Facilities: Results from a Nationally Representative Survey. Arch. Gerontol. Geriatr. 2006, 43, 193–212. [Google Scholar] [CrossRef]
- Johnston, G.M.; Urquhart, R.; Lethbridge, L.; MacIntyre, M. Increasing Our Understanding of Dying of Breast Cancer: Comorbidities and Care. Prog. Palliat. Care 2016, 24, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Bainbridge, D.; Seow, H.; Sussman, J.; Pond, G. Factors Associated with Acute Care Use among Nursing Home Residents Dying of Cancer: A Population-Based Study. Int. J. Palliat. Nurs. 2015, 21, 349–356. [Google Scholar] [CrossRef]
- Cagle, J.G.; Lee, J.; Ornstein, K.A.; Guralnik, J.M. Hospice Utilization in the United States: A Prospective Cohort Study Comparing Cancer and Noncancer Deaths. J. Am. Geriatr. Soc. 2020, 68, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Boyd, M.; Frey, R.; Balmer, D.; Robinson, J.; McLeod, H.; Foster, S.; Slark, J.; Gott, M. End of Life Care for Long-Term Care Residents with Dementia, Chronic Illness and Cancer: Prospective Staff Survey. BMC Geriatr. 2019, 19, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drageset, J.; Eide, G.E.; Ranhoff, A.H. Mortality in Nursing Home Residents without Cognitive Impairment and Its Relation to Self-Reported Health-Related Quality of Life, Sociodemographic Factors, Illness Variables and Cancer Diagnosis: A 5-Year Follow-up Study. Qual. Life Res. 2013, 22, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Kiely, D.K.; Flacker, J.M. Common and Gender Specific Factors Associated with One-Year Mortality in Nursing Home Residents. J. Am. Med. Dir. Assoc. 2002, 3, 302–309. [Google Scholar] [CrossRef]
- Irvin, S. The Experiences of the Registered Nurse Caring for the Person Dying of Cancer in a Nursing Home. Collegian 2000, 7, 30–34. [Google Scholar] [CrossRef]
- Sommerbakk, R.; Haugen, D.F.; Tjora, A.; Kaasa, S.; Hjermstad, M.J. Barriers to and Facilitators for Implementing Quality Improvements in Palliative Care—Results from a Qualitative Interview Study in Norway. BMC Palliat. Care 2016, 15, 61. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.; Maio, L.; van Riet Paap, J.; Mariani, E.; Jaspers, B.; Sommerbakk, R.; Grammatico, D.; Manthorpe, J.; Ahmedzai, S.; Vernooij-Dassen, M.; et al. Quality Palliative Care for Cancer and Dementia in Five European Countries: Some Common Challenges. Aging Ment. Health 2014, 18, 400–410. [Google Scholar] [CrossRef] [Green Version]
- Zueger, P.M.; Holmes, H.M.; Calip, G.S.; Qato, D.M.; Pickard, A.S.; Lee, T.A. Older Medicare Beneficiaries Frequently Continue Medications with Limited Benefit Following Hospice Admission. J. Gen. Intern. Med. 2019, 34, 2029–2037. [Google Scholar] [CrossRef]
- Onder, G.; Vetrano, D.L.; Villani, E.R.; Carfì, A.; Monaco, M.R.L.; Cipriani, M.C.; Gravina, E.M.; Denkinger, M.; Pagano, F.; van der Roest, H.G.; et al. Deprescribing in Nursing Home Residents on Polypharmacy: Incidence and Associated Factors. J. Am. Med. Dir. Assoc. 2019, 20, 1116–1120. [Google Scholar] [CrossRef] [PubMed]
- Drageset, J.; Eide, G.E.; Harrington, C.; Ranhoff, A.H. Acute Hospital Admission for Nursing Home Residents without Cognitive Impairment with a Diagnosis of Cancer. Eur. J. Cancer Care 2015, 24, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Lage, D.E.; DuMontier, C.; Lee, Y.; Nipp, R.D.; Mitchell, S.L.; Temel, J.S.; El-Jawahri, A.; Berry, S.D. Potentially Burdensome End-of-Life Transitions among Nursing Home Residents with Poor-Prognosis Cancer. Cancer 2020, 126, 1322–1329. [Google Scholar] [CrossRef]
- Aamodt, I.M.T.; Lie, I.; Hellesø, R. Nurses’ Perspectives on the Discharge of Cancer Patients with Palliative Care Needs from a Gastroenterology Ward. Int. J. Palliat. Nurs. 2013, 19, 396–402. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, M.A.; Buck, H.G.; Meghani, S.H.; Riegel, B. Unique Correlates of Heart Failure and Cancer Caregiver Satisfaction With Hospice Care. J. Pain Symptom Manag. 2016, 51, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijers, J.M.M.; Schols, J.M.G.A.; van Bokhorst-de van der Schueren, M.A.E.; Dassen, T.; Janssen, M.A.P.; Halfens, R.J.G. Malnutrition Prevalence in The Netherlands: Results of the Annual Dutch National Prevalence Measurement of Care Problems. Br. J. Nutr. 2009, 101, 417–423. [Google Scholar] [CrossRef]
- Bakker, D.; Butler, L.; Fitch, M.; Green, E.; Olson, K.; Cummings, G. Canadian Cancer Nurses’ Views on Recruitment and Retention. J. Nurs. Manag. 2010, 18, 205–214. [Google Scholar] [CrossRef]
- Nagamatsu, Y.; Natori, Y.; Yanai, H.; Horiuchi, S. Impact of a Nursing Education Program about Caring for Patients in Japan with Malignant Pleural Mesothelioma on Nurses’ Knowledge, Difficulties and Attitude: A Randomized Control Trial. Nurse Educ. Today 2014, 34, 1087–1093. [Google Scholar] [CrossRef] [Green Version]
- Gerhart, J.I.; Varela, V.S.; Burns, J.W. Brief Training on Patient Anger Increases Oncology Providers’ Self-Efficacy in Communicating With Angry Patients. J. Pain Symptom Manag. 2017, 54, 355–360. [Google Scholar] [CrossRef] [Green Version]
- Passik, S.D.; Donaghy, K.B.; Theobald, D.E.; Lundberg, J.C.; Holtsclaw, E.; Dugan, W.M., Jr.; Passik, S.D.; Donaghy, K.B.; Theobald, D.E.; Lundberg, J.C.; et al. Oncology Staff Recognition of Depressive Symptoms on Videotaped Interviews of Depressed Cancer Patients: Implications for Designing a Training Program. J. Pain Symptom Manag. 2000, 19, 329–338. [Google Scholar] [CrossRef]
- Fukui, S.; Ogawa, K.; Yamagishi, A. Effectiveness of Communication Skills Training of Nurses on the Quality of Life and Satisfaction with Healthcare Professionals among Newly Diagnosed Cancer Patients: A Preliminary Study. Psycho-oncology 2011, 20, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Hwang, S.Y.; Oh, E.G.; Lee, J.E. Development and Evaluation of a PBL-based Continuing Education for Clinical Nurses: A Pilot Study. J. Korean Acad. Nurs. 2006, 36, 1308. [Google Scholar] [CrossRef] [Green Version]
- Baile, W.F.; Kudelka, A.P.; Beale, E.A.; Glober, G.A.; Myers, E.G.; Greisinger, A.J.; Bast, R.C.; Goldstein, M.G.; Novack, D.; Lenzi, R. Communication Skills Training in Oncology. Description and Preliminary Outcomes of Workshops on Breaking Bad News and Managing Patient Reactions to Illness. Cancer 1999, 86, 887–897. [Google Scholar] [CrossRef]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef] [Green Version]
- Fujimori, M.; Oba, A.; Koike, M.; Okamura, M.; Akizuki, N.; Kamiya, M.; Akechi, T.; Sakano, Y.; Uchitomi, Y. Communication Skills Training for Japanese Oncologists on How to Break Bad News. J. Cancer Educ. 2003, 18, 194–201. [Google Scholar] [CrossRef]
- Yancik, R.; Ries, L.A. Cancer in Older Persons. Magnitude of the Problem-how Do We Apply What We Know? Cancer 1994, 74, 1995–2003. [Google Scholar] [CrossRef]
- Brody, B.A.; Halevy, A. Is Futility a Futile Concept? J. Med. Philos. 1995, 20, 123–144. [Google Scholar] [CrossRef]
- Bosslet, G.T.; Pope, T.M.; Rubenfeld, G.D.; Lo, B.; Truog, R.D.; Rushton, C.H.; Curtis, J.R.; Ford, D.W.; Osborne, M.; Misak, C.; et al. An Official ATS/AACN/ACCP/ESICM/SCCM Policy Statement: Responding to Requests for Potentially Inappropriate Treatments in Intensive Care Units. Am. J. Respir. Crit. Care Med. 2015, 191, 1318–1330. [Google Scholar] [CrossRef] [PubMed]
- Ramjaun, A.; Nassif, M.O.; Krotneva, S.; Huang, A.R.; Meguerditchian, A.N. Improved Targeting of Cancer Care for Older Patients: A Systematic Review of the Utility of Comprehensive Geriatric Assessment. J. Geriatr. Oncol. 2013, 4, 271–281. [Google Scholar] [CrossRef]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H.; Brown, R.H.; DeFelice, J.; Levine, R.M.; Lubiner, E.T.; Reyes, P.; Schreiber, F.J.; et al. Predicting the Risk of Chemotherapy Toxicity in Older Patients: The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) Score. Cancer 2012, 118, 3377–3386. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Tonorezos, E.; Zorowitz, R.; Novotny, J.; Dubin, S.; Maurer, M.S. Inpatient Care for Nursing Home Patients: An Opportunity to Improve Transitional Care. J. Am. Med. Dir. Assoc. 2006, 7, 383–387. [Google Scholar] [CrossRef] [PubMed]
- De Gagne, J.C.; Park, H.K.; Hall, K.; Woodward, A.; Yamane, S.; Kim, S.S. Microlearning in Health Professions Education: Scoping Review. JMIR Med. Educ. 2019, 5, e13997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, S.; Jolliffe, S.; Stanmore, E.; Renwick, L.; Booth, R. Social Media in Nursing and Midwifery Education: A Mixed Study Systematic Review. J. Adv. Nurs. 2018, 74, 2273–2289. [Google Scholar] [CrossRef]
- Qalehsari, M.Q.; Khaghanizadeh, M.; Ebadi, A. Lifelong Learning Strategies in Nursing: A Systematic Review. Electron. Physician 2017, 9, 5541–5550. [Google Scholar] [CrossRef] [Green Version]
- Bourbonniere, M.; Van Cleave, J.H. Cancer Care in Nursing Homes. Semin. Oncol. Nurs. 2006, 22, 51–57. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filteau, C.; Simeone, A.; Ravot, C.; Dayde, D.; Falandry, C. Cultural and Ethical Barriers to Cancer Treatment in Nursing Homes and Educational Strategies: A Scoping Review. Cancers 2021, 13, 3514. https://doi.org/10.3390/cancers13143514
Filteau C, Simeone A, Ravot C, Dayde D, Falandry C. Cultural and Ethical Barriers to Cancer Treatment in Nursing Homes and Educational Strategies: A Scoping Review. Cancers. 2021; 13(14):3514. https://doi.org/10.3390/cancers13143514
Chicago/Turabian StyleFilteau, Cynthia, Arnaud Simeone, Christine Ravot, David Dayde, and Claire Falandry. 2021. "Cultural and Ethical Barriers to Cancer Treatment in Nursing Homes and Educational Strategies: A Scoping Review" Cancers 13, no. 14: 3514. https://doi.org/10.3390/cancers13143514
APA StyleFilteau, C., Simeone, A., Ravot, C., Dayde, D., & Falandry, C. (2021). Cultural and Ethical Barriers to Cancer Treatment in Nursing Homes and Educational Strategies: A Scoping Review. Cancers, 13(14), 3514. https://doi.org/10.3390/cancers13143514