
Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
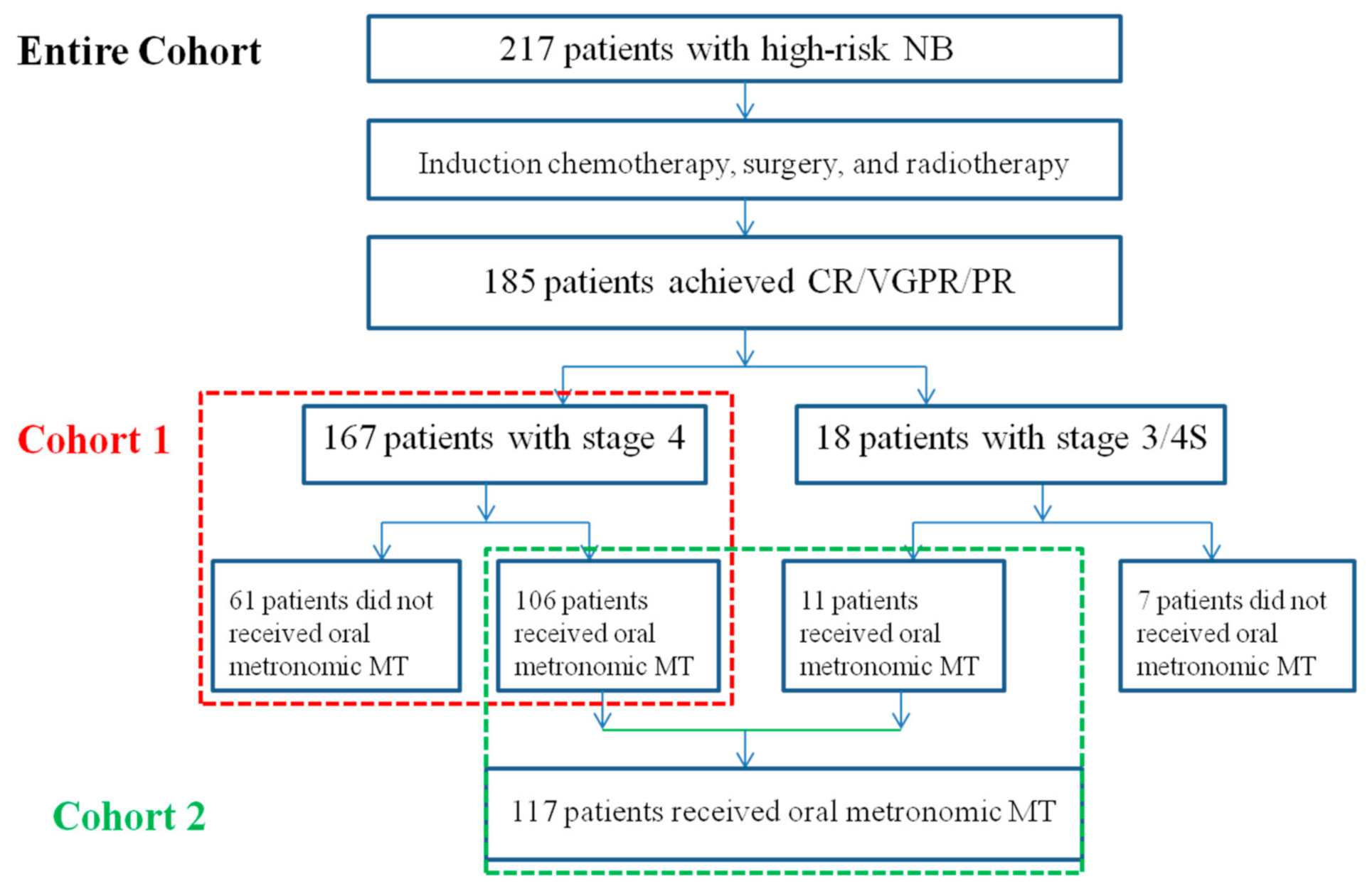
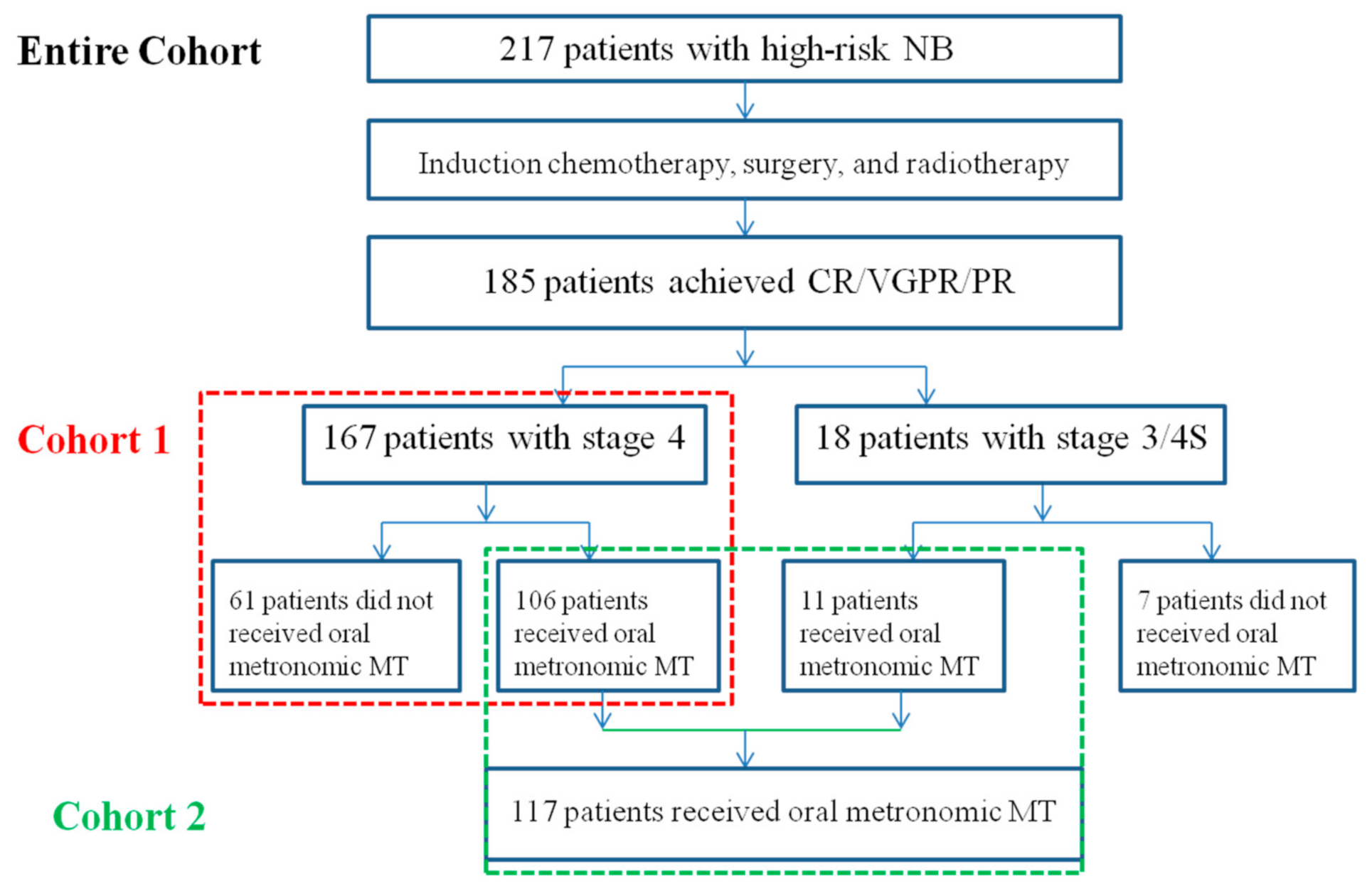
2.1. Patients
2.2. Treatment Protocol
2.3. Evaluation of Response and Toxicity
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Outcome
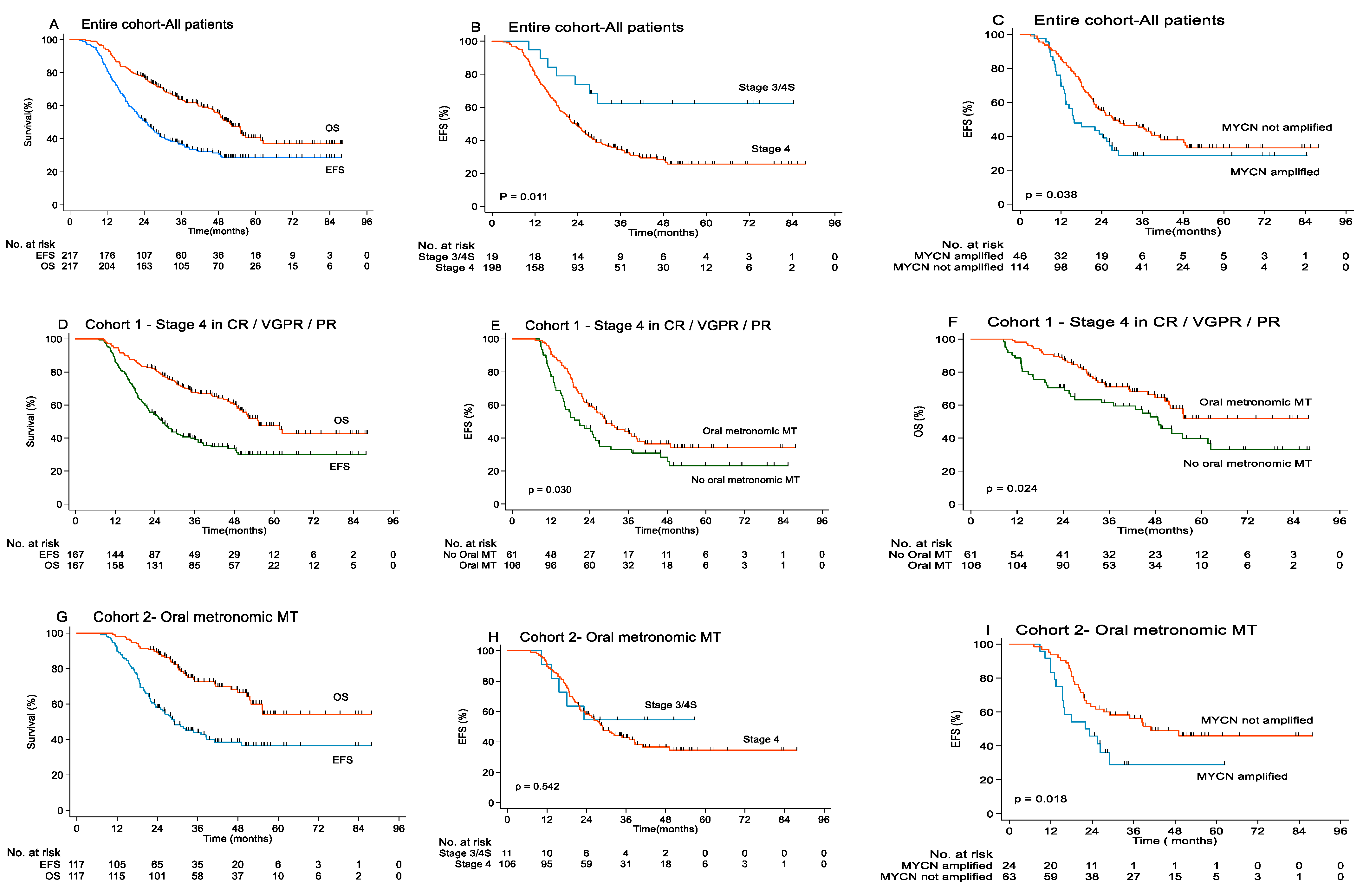
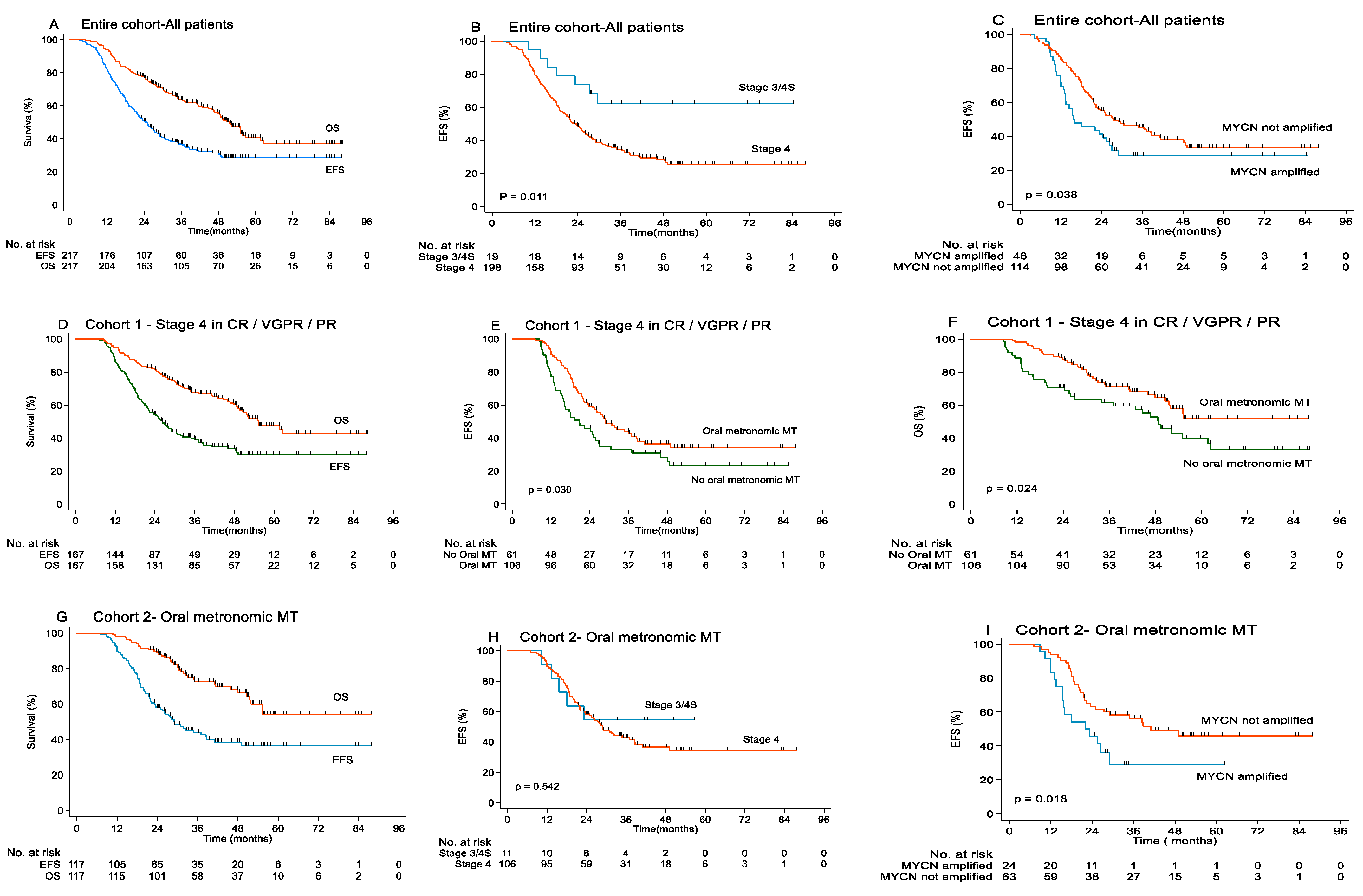
3.3. Survival
3.4. The Toxicity of Oral Metronomic MT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matthay, K.K.; Villablanca, J.G.; Seeger, R.C.; Stram, D.O.; Harris, R.E.; Ramsay, N.K.; Swift, P.; Shimada, H.; Black, C.T.; Brodeur, G.M.; et al. Treatment of High-Risk Neuroblastoma With Intensive Chemotherapy, Radiotherapy, Autologous Bone Marrow Transplantation, and 13-Cis-Retinoic Acid. N. Engl. J. Med. 1999, 341, 1165–1173. [Google Scholar] [CrossRef]
- Berthold, F.; Boos, J.; Burdach, S.; Erttmann, R.; Henze, G.; Hermann, J.; Klingebiel, T.; Kremens, B.; Schilling, F.H.; Schrappe, M.; et al. Myeloablative megatherapy with autologous stem-Cell rescue versus oral maintenance chemotherapy as consolidation treatment in patients with high-risk neuroblastoma: A randomized controlled trial. Lancet Oncol. 2005, 6, 649–658. [Google Scholar] [CrossRef]
- Pritchard, J.; Cotterill, S.J.; Germond, S.M.; Imeson, J.; De Kraker, J.; Jones, D.R. High dose melphalan in the treatment of advanced neuroblastoma: Results of a randomized trial (ENSG-1) by the European Neuroblastoma Study Group. Pediatr. Blood Cancer 2005, 44, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Matthay, K.K.; Reynolds, C.P.; Seeger, R.C.; Shimada, H.; Adkins, E.S.; Haas-Kogan, D.; Gerbing, R.B.; London, W.B.; Villablanca, J.G. Long-term results for children with high-risk neuroblastoma treated on a randomized trial of myeloablative therapy followed by 13-cis-retinoic acid: A children’s oncology group study. J. Clin. Oncol. 2009, 27, 1007–1013. [Google Scholar] [CrossRef] [Green Version]
- Berthold, F.; Ernst, A.; Hero, B.; Klingebiel, T.; Kremens, B.; Schilling, F.H.; Simon, T. Long-term outcomes of the GPOH NB97 trial for children with high-risk neuroblastoma comparing high-dose chemotherapy with autologous stem cell transplantation and oral chemotherapy as consolidation. Br. J. Cancer 2018, 119, 282–290. [Google Scholar] [CrossRef]
- Yalçin, B.; Kremer, L.C.; van Dalen, E.C. High-dose chemotherapy and autologous haematopoietic stem cell rescue for children with high-risk neuroblastoma. Cochrane Database Syst. Rev. 2015, 10, CD006301. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.L.; Gilman, A.L.; Ozkaynak, M.F.; London, W.B.; Kreissman, S.G.; Chen, H.X.; Smith, M.; Anderson, B.; Villablanca, J.G.; Matthay, K.K.; et al. Anti-GD2 antibody with GM-CSF, interleukin-2, and isotretinoin for neuroblastoma. N. Engl. J. Med. 2010, 363, 1324–1334. [Google Scholar] [CrossRef] [Green Version]
- Cheung, N.K.; Cheung, I.Y.; Kushner, B.H.; Ostrovnaya, I.; Chamberlain, E.; Kramer, K.; Modak, S. Murine anti-GD2 monoclonal antibody 3F8 combined with granulocyte-macrophage colony-stimulating factor and 13-cis-retinoic acid in high-risk patients with stage 4 neuroblastoma in first remission. J. Clin. Oncol. 2012, 30, 3264–3270. [Google Scholar] [CrossRef] [Green Version]
- Ladenstein, R.; Pötschger, U.; Valteau-Couanet, D.; Luksch, R.; Castel, V.; Yaniv, I.; Laureys, G.; Brock, P.; Michon, J.M.; Owens, C.; et al. Interleukin 2 with anti-GD2 antibody ch14.18/CHO (dinutuximab beta) in patients with high-risk neuroblastoma (HR-NBL1/SIOPEN): A multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1617–1629. [Google Scholar] [CrossRef]
- Yu, A.L.; Gilman, A.L.; Ozkaynak, M.F.; Naranjo, A.; Diccianni, M.B.; Gan, J.; Hank, J.A.; Batova, A.; London, W.B.; Tenney, S.C.; et al. Long-Term Follow-up of a Phase III Study of ch14.18 (Dinutuximab) + Cytokine Immunotherapy in Children with High-Risk Neuroblastoma: COG Study ANBL0032. Clin. Cancer Res. 2021, 27, 2179–2189. [Google Scholar] [CrossRef]
- Zapletalova, D.; André, N.; Deak, L.; Kyr, M.; Bajciova, V.; Mudry, P.; Dubska, L.; Demlova, R.; Pavelka, Z.; Zitterbart, K.; et al. Metronomic chemotherapy with the COMBAT regimen in advanced pediatric malignancies: A multicenter experience. Oncology 2012, 82, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Stempak, D.; Gammon, J.; Halton, J.; Moghrabi, A.; Koren, G.; Baruchel, S. A Pilot Pharmacokinetic and antiangiogenic Biomarker Study of Celecoxib and Low-dose Metronomic Vinblastine or Cyclophosphamide in Pediatric Recurrent Solid Tumors. J. Pediatr. Hematol. Oncol. 2006, 28, 720–728. [Google Scholar] [CrossRef] [PubMed]
- André, N.; Rome, A.; Coze, C.; Padovani, L.; Pasquier, E.; Camoin, L.; Gentet, J.C. Metronomic etoposide/cyclophosphamide/celecoxib regimen given to children and adolescents with refractory cancer: A preliminary monocentric study. Clin. Ther. 2008, 30, 1336–1340. [Google Scholar] [CrossRef]
- Bouche, G.; André, N.; Banavali, S.; Berthold, F.; Berruti, A.; Bocci, G.; Brandi, G.; Cavallaro, U.; Cinieri, S.; Colleoni, M.; et al. Lessons from the Fourth Metronomic and Anti-angiogenic Therapy Meeting, 24–25 June 2014, Milan. Ecancermedicalscience 2014, 8, 463. [Google Scholar]
- Schmiegelow, K.; Nielsen, S.N.; Frandsen, T.L.; Nersting, J. Mercaptopurine/Methotrexate maintenance therapy of childhood acute lymphoblastic leukemia: Clinical facts and fiction. J. Pediatr. Hematol. Oncol. 2014, 36, 503–517. [Google Scholar] [CrossRef] [Green Version]
- Klingebiel, T.; Boos, J.; Beske, F.; Hallmen, E.; Int-Veen, C.; Dantonello, T.; Treuner, J.; Gadner, H.; Marky, I.; Kazanowska, B.; et al. Treatment of children with metastatic soft tissue sarcoma with oral maintenance compared to high dose chemotherapy: Report of the HD CWS-96. Trial. Pediatr. Blood Cancer 2008, 50, 739–745. [Google Scholar] [CrossRef]
- Bisogno, G.; De Salvo, G.L.; Bergeron, C.; Gallego Melcón, S.; Merks, J.H.; Kelsey, A.; Martelli, H.; Minard-Colin, V.; Orbach, D.; Glosli, H.; et al. Vinorelbine and continuous low-dose cyclophosphamide as maintenance chemotherapy in patients with high-risk rhabdomyosarcoma (RMS 2005): A multicenter, open-label, randomized, phase 3 trial. Lancet Oncol. 2019, 20, 1566–1575. [Google Scholar] [CrossRef]
- Shimada, H.; Ambros, I.M.; Dehner, L.P.; Hata, J.; Joshi, V.V.; Roald, B.; Stram, D.O.; Gerbing, R.B.; Lukens, J.N.; Matthay, K.K.; et al. The International Neuroblastoma Pathology Classification (the Shimada System). Cancer 1999, 86, 364–372. [Google Scholar] [CrossRef]
- Brodeur, G.M.; Pritchard, J.; Berthold, F.; Carlsen, N.L.; Castel, V.; Castelberry, R.P.; De Bernardi, B.; Evans, A.E.; Favrot, M.; Hedborg, F.; et al. Revisions of the International Criteria for Neuroblastoma Diagnosis, Staging, and Response to Treatment. J. Clin. Oncol. 1993, 11, 1466–1477. [Google Scholar] [CrossRef]
- Su, Y.; Ma, X.L.; Wang, H.M.; Qin, H.; Qin, M.Q.; Zhang, F.Q.; Jin, M.; Zhang, D.W.; Chen, C.H.; Zeng, Q.; et al. Clinical characteristics and prognostic analysis of 458 children with high-risk neuroblastoma in a single center. Chin. J. Pediatr. 2020, 58, 796–801. [Google Scholar]
- Simon, T.; Hero, B.; Faldum, A.; Handgretinger, R.; Schrappe, M.; Klingebiel, T.; Berthold, F. Long term outcome of high-risk neuroblastoma patients after immunotherapy with antibody ch14.18 or oral metronomic chemotherapy. BMC Cancer 2011, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Kushner, B.H.; Ostrovnaya, I.; Cheung, I.; Kuk, D.; Modak, S.; Kramer, K.; Roberts, S.S.; Basu, E.M.; Yataghene, K.; Cheung, N.K. Lack of survival advantage with autologous stem-cell transplantation in high-risk neuroblastoma consolidated by anti-GD2 immunotherapy and isotretinoin. Oncotarget 2016, 7, 4155–4166. [Google Scholar] [CrossRef] [Green Version]
- Robison, N.J.; Campigotto, F.; Chi, S.N.; Manley, P.E.; Turner, C.D.; Zimmerman, M.A.; Chordas, C.A.; Werger, A.M.; Allen, J.C.; Goldman, S.; et al. A phase II trial of a multi-agent oral antiangiogenic (metronomic) regimen in children with recurrent or progressive cancer. Pediatr. Blood Cancer 2014, 61, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Son, M.H.; Cho, H.W.; Ma, Y.E.; Yoo, K.H.; Sung, K.W.; Koo, H.H. Clinical significance of MYCN amplification in patients with high-risk neuroblastoma. Pediatr. Blood Cancer 2018, 65, e27257. [Google Scholar] [CrossRef]
- Campbell, K.; Gastier-Foster, J.M.; Mann, M.; Naranjo, A.H.; Van Ryn, C.; Bagatell, R.; Matthay, K.K.; London, W.B.; Irwin, M.S.; Shimada, H.; et al. Association of MYCN Copy Number with Clinical Features, Tumor Biology, and Outcomes in Neuroblastoma: A Report from the Children’s Oncology Group. Cancer 2017, 123, 4224–4235. [Google Scholar] [CrossRef] [Green Version]
- Aygun, N. Biological and Genetic Features of Neuroblastoma and Their Clinical Importance. Curr. Pediatric Rev. 2018, 14, 73–90. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.; Shyr, D.; Bagatell, R.; Fischer, M.; Nakagawara, A.; Nieto, A.C.; Brodeur, G.M.; Matthay, K.K.; London, W.B.; DuBois, S.G. Comprehensive evaluation of context dependence of the prognostic impact of MYCN amplification in neuroblastoma: A report from the International Neuroblastoma Risk Group (INRG) project. Pediatr. Blood Cancer 2019, 66, e27819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canete, A.; Gerrard, M.; Rubie, H.; Castel, V.; Di Cataldo, A.; Munzer, C.; Ladenstein, R.; Brichard, B.; Bermúdez, J.D.; Couturier, J.; et al. Poor survival for infants with MYCN-amplified metastatic neuroblastoma despite intensified treatment: The International Society of Paediatric Oncology European Neuroblastoma Experience. J. Clin. Oncol. 2009, 27, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, F.; Yamasaki, K.; Kiyotani, C.; Hashii, Y.; Shioda, Y.; Hara, J.; Matsumoto, K. Thiotepa–melphalan myeloablative therapy for high-risk neuroblastoma. Pediatr. Blood Cancer 2021, 68, e28896. [Google Scholar] [CrossRef]
- Pinto, N.R.; Applebaum, M.A.; Volchenboum, S.L.; Matthay, K.K.; London, W.B.; Ambros, P.F.; Nakagawara, A.; Berthold, F.; Schleiermacher, G.; Park, J.R.; et al. Advances in Risk Classification and Treatment Strategies for Neuroblastoma. J. Clin. Oncol. 2015, 33, 3008–3017. [Google Scholar] [CrossRef]
- London, W.B.; Castel, V.; Monclair, T.; Ambros, P.F.; Pearson, A.D.; Cohn, S.L.; Berthold, F.; Nakagawara, A.; Ladenstein, R.L.; Iehara, T.; et al. Clinical and biologic features predictive of survival after relapse of neuroblastoma: A report from the International Neuroblastoma Risk Group project. J. Clin. Oncol. 2011, 29, 3286–3292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, W.B.; Bagatell, R.; Weigel, B.J.; Fox, E.; Guo, D.; Van Ryn, C.; Naranjo, A.; Park, J.R. Historical time to disease progression and progression—free survival in patients with recurrent/refractory neuroblastoma treated in the modern era on Children’s Oncology Group early-phase trials. Cancer 2017, 123, 4914–4923. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.; Rubie, H.; Varo, A.; Le Deley, M.C.; Amoroso, L.; Chevance, A.; Garaventa, A.; Gambart, M.; Bautista, F.; Valteau-Couanet, D.; et al. Outcome of children with relapsed or refractory neuroblastoma: A meta-analysis of ITCC/SIOPEN European phase II clinical trials. Pediatr. Blood Cancer 2017, 64, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Chemotherapy Regimens | Drugs Dosage and Administration |
|---|---|
| Induction Chemotherapy: | |
| CAV (Cycle 1, 3, 5, and 7) | Cyclophosphamide (CTX) 1 g/m2, iv drip for 0.5 h, d1–2 Mesna 330 mg/m2 0, 4, and 8 h after CTX, iv, d1–2 Vincristine 1.5 mg/m2, iv, d1 Pirarubicin 50 mg/m2, iv, d1 |
| VIP (Cycle 2, 4, 6, and 8) | Cisplatin 25 mg/m2, iv drip for 3 h, d1–4 Etoposide 100 mg/m2, iv drip for 3 h, d1–4 Ifosfamide (IFO) 1.5 g/m2, iv drip for 3 h, d1–4 Mesna 300 mg/m2, iv 0, 4, 8 h after IFO, d1–4 |
| Second-line chemotherapy: | |
| VIT | Vincristine 1.5 mg/m2, iv, d1 Irinotecan 50 mg/m2, iv drip for 1.5 h, d1–5 Temozolomide 100 mg/m2, po, d1–5 |
| Maintenance therapy: | |
| Oral metronomic anti-angiogenic agents | At months 1, 3, 5, 7, 9, and 11: Cyclophosphamide 25–50 mg/m2, po, d1–30 Vinorelbine 40 mg/m2, po, qw × 3 Etoposide 25 mg/m2, po, d1–21 Celecoxib 200 mg/m2, po, bid d1–30 At months 2, 4, 6, 8, 10, and 12: Cyclophosphamide 25-50 mg/m2, po, d1–30 Vinorelbine 40 mg/m2, po, qw × 3 Topotecan a 1.4 mg/m2, po, d1–5 Celecoxib 200 mg/m2, po, bid d1–30 |
| Feature | Entire Cohort (n = 217) | Cohort 1 (n = 167) | Cohort 2 (n = 117) |
|---|---|---|---|
| Sex | |||
| Male | 145 (66.8%) | 122 (65.9%) | 76 (65%) |
| Female | 72 (33.2%) | 63 (34.1%) | 41 (35%) |
| Age | |||
| Age ≥ 18 months at diagnosis | 200 (92.2%) | 171 (92.4%) | 107 (91.5%) |
| Age < 18 months at diagnosis | 17 (7.8%) | 14 (7.6%) | 10 (8.5%) |
| Stage | |||
| INSS Stage 4 | 198 (91.2%) | 167 (90.3%) | 106 (90.6%) |
| INSS Stage 3 | 18 (8.3%) | 10 (8.5%) | |
| INSS Stage 4S | 1 (0.5%) | 1 (0.9%) | |
| Primary tumor site | |||
| Adrenal gland primary | 121 (55.8%) | 106 (57.3%) | 72 (61.5%) |
| Retroperitoneal primary | 71 (32.7%) | 59 (31.9%) | 36 (30.8%) |
| Mediastinum primary | 17 (7.8%) | 12 (6.5%) | 5 (4.3%) |
| Other primary sites | 8 (3.7%) | 8 (4.3%) | 4 (3.4%) |
| Metastatic sites | |||
| Bone marrow/bone metastasis | 172 (79.3%) | 146 (78.9%) | 94 (80.3%) |
| Other metastasis sites | 45 (20.7%) | 39 (21.1%) | 23 (19.7%) |
| MYCN status | |||
| MYCN amplified | 46 (28.8%) | 39 (28.3%) | 24 (27.6%) |
| MYCN not amplified | 114 (71.3%) | 99 (53.5%) | 63 (72.4%) |
| MYCN unknown | 57 (26.3%) | 47 (25.4%) | 30 (25.6%) |
| N | 3-Year EFS (%) | p-Value | 3-Year OS (%) | p-Value | |
|---|---|---|---|---|---|
| Entire Cohort | 217 | 36.3 ± 3.4 | 63.1 ± 3.4 | ||
| Age | |||||
| Age ≥ 18 months | 200 | 35.5 ± 3.5 | 0.63 | 63.6 ± 3.5 | 0.575 |
| Age < 18 months | 17 | 45.3 ± 12.4 | 57.4 ± 12.3 | ||
| Sex | |||||
| Male | 145 | 36.4 ± 4.1% | 0.752 | 64.1 ± 4.1 | 0.965 |
| Female | 72 | 36.0 ± 6.0% | 61.1 ± 6.1 | ||
| Stage | |||||
| INSS Stage 4 | 198 | 33.8 ± 3.5 | 0.011 | 60.3 ± 3.6 | 0.008 |
| INSS Stage 3/4S | 19 | 62.2 ± 11.4 | 83.3 ± 11.2 | ||
| MYCN status | |||||
| MYCN amplified | 46 | 28.6 ± 7.0 | 0.038 | 48.6 ± 8.0 | 0.008 |
| MYCN no amplified | 114 | 44.3 ± 4.8 | 74.0 ± 4.3 | ||
| Metastatic sites | |||||
| BM/bone metastasis | 172 | 32.6 ± 3.7 | 0.102 | 60.4 ± 3.9 | 0.097 |
| Other metastasis sites | 45 | 47.0 ± 7.7 | 70.5 ± 7.3 | ||
| Cohort 1 a | 167 | 37.8 ± 3.9 | 66.9 ± 3.8 | ||
| Age | |||||
| Age ≥ 18 months | 154 | 36.0 ± 0.4 | 0.212 | 67.5 ± 3.9 | 0.910 |
| Age < 18 months | 13 | 59.8 ± 14 | 59.2 ± 14.1 | ||
| Sex | |||||
| Male | 110 | 37.2 ± 4.8 | 0.953 | 68.2 ± 4.6 | 0.652 |
| Female | 57 | 38.8 ± 6.9 | 64.2 ± 4.7 | ||
| MYCN status | |||||
| MYCN amplified | 27 | 12.3 ± 9.9 | 0.019 | 37.8 ± 10.9 | 0.000 |
| MYCN not amplified | 93 | 46.1 ± 5.3 | 76.7 ± 4.6 | ||
| Oral MT | |||||
| Oral metronomic MT | 106 | 42.5 ± 5.1 | 0.017 | 71.1 ± 6.7 | 0.022 |
| No oral metronomic MT | 61 | 29.6 ± 6 | 59.4 ± 6.4 | ||
| Cohort 2 b | 117 | 42.7 ± 4.8 | 72.1 ± 4.5 | ||
| Age | |||||
| Age ≥ 18 months | 107 | 41.4 ± 5.0 | 0.261 | 72.2 ± 4.6 | 0.563 |
| Age < 18 months | 10 | 68.6 ± 15.1 | 77.8 ± 13.9 | ||
| Sex | |||||
| Male | 76 | 46.8 ± 5.9 | 0.513 | 70.5 ± 5.5 | 0.600 |
| Female | 41 | 36.2 ± 8.3 | 76.6 ± 7.4 | ||
| MYCN status | |||||
| MYCN amplified | 24 | 16.8 ± 13 | 0.026 | 56.3 ± 13.4 | 0.042 |
| MYCN not amplified | 63 | 53.9 ± 6.5 | 78.1 ± 5.7 | ||
| Stage | |||||
| Stage 4 | 106 | 42.5 ± 5.1 | 0.556 | 71.1 ± 4.7 | 0.167 |
| Stage 3/4S | 11 | 54.5 ± 15 | 88.9 ± 10.5 |
| Category | No | 3-Year Event-Free Survival | 3-Year Overall Survival | ||||
|---|---|---|---|---|---|---|---|
| Univariate | Multivariate b | Univariate | Multivariate b | ||||
| p-Value | HR (95% CI) | p-Value | p-Value | HR (95% CI) | p-Value | ||
| Age | |||||||
| ≥18 months | 200 | 0.631 | 0.680 | 0.285 | 0.576 | 1.075 | 0.859 |
| <18 months | 17 | (0.335, 1.379) | (0.481, 2.402) | ||||
| Sex | |||||||
| Male | 145 | 0.752 | 1. 218 | 0.362 | 0.965 | 1.125 | 0.649 |
| Female | 72 | (0.798, 1.858) | (0.677, 1.869) | ||||
| Stage | |||||||
| Stage 4 | 198 | 0.014 | 0.246 | 0.002 | 0.014 | 0.147 | 0.003 |
| Stage 3/4S | 19 | (0.102, 0.594) | (0.041, 0.525) | ||||
| MYCN amplified | |||||||
| Yes | 46 | 0.040 | 0.462 | 0.001 | 0.009 | 0.351 | 0.000 |
| No | 114 | (0.292, 0.732) | (0.209, 0.590) | ||||
| Metastasis sites | |||||||
| BM/Bone | 172 | 0.104 | 1.151 | 0.608 | 0.100 | 1.026 | 0.937 |
| Other | 45 | (0.672, 1.972) | (0.550, 1.914) | ||||
| Stage 4 in CR/VGPR/PR | |||||||
| Oral MT c | 106 | 0.030 | 0.559 | 0.014 | 0.024 | 0.366 | 0.001 |
| No oral MT | 61 | (0.351, 0.891) | (0.197, 0.680) | ||||
| Toxicity Grading [n (%)] | |||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Hemoglobin | 27 (23.1) | 43 (36.8) | 45 (38.5) | 2 (1.7) | 0 (0) |
| White blood cell | 13 (11.1) | 46 (39.3) | 49 (41.9) | 9 (7.7) | 0 (0) |
| Platelets | 116 (99.1) | 1 (0.9) | 0 (0) | 0 (0) | 0 (0) |
| Transaminase | 104 (88.9) | 10 (8.5) | 2 (1.7) | 1 (0.9) | 0 (0) |
| Nausea | 114 (97.4) | 1 (0.9) | 2 (1.7) | 0 (0) | 0 (0) |
| Creatinine | 113 (96.6) | 4 (3.4) | 0 (0) | 0 (0) | 0 (0) |
| Gastritis | 114 (97.4) | 1 (0.9) | 2 (1.7) | 0 (0) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, X.; Zhen, Z.; Guo, Y.; Gao, Y.; Wang, J.; Zhang, Y.; Zhu, J.; Lu, S.; Sun, F.; Huang, J.; et al. Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies. Cancers 2021, 13, 3494. https://doi.org/10.3390/cancers13143494
Sun X, Zhen Z, Guo Y, Gao Y, Wang J, Zhang Y, Zhu J, Lu S, Sun F, Huang J, et al. Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies. Cancers. 2021; 13(14):3494. https://doi.org/10.3390/cancers13143494
Chicago/Turabian StyleSun, Xiaofei, Zijun Zhen, Ying Guo, Yuanhong Gao, Juan Wang, Yu Zhang, Jia Zhu, Suying Lu, Feifei Sun, Junting Huang, and et al. 2021. "Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies" Cancers 13, no. 14: 3494. https://doi.org/10.3390/cancers13143494
APA StyleSun, X., Zhen, Z., Guo, Y., Gao, Y., Wang, J., Zhang, Y., Zhu, J., Lu, S., Sun, F., Huang, J., Cai, R., Zhang, Y., Liu, J., Xiao, Z., Zeng, S., & Liu, Z. (2021). Oral Metronomic Maintenance Therapy Can Improve Survival in High-Risk Neuroblastoma Patients Not Treated with ASCT or Anti-GD2 Antibodies. Cancers, 13(14), 3494. https://doi.org/10.3390/cancers13143494