
Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Study Setting
2.2. Surgical Technique and Follow-Up Routine
2.3. Variables
2.4. Statistics
3. Results
3.1. Baseline and Treatment Data
3.2. Outcome Data
3.3. Functional Outcome
3.4. Elderly vs. Non-Elderly Patients
3.5. Predictors of Improved Functional Outcome
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| mMCs | modified McCormick scale |
| MRI | magnetic resonance imaging |
| OR | odds ratio |
| WHO | World Health Organization |
References
- Kshettry, V.R.; Hsieh, J.K.; Ostrom, Q.T.; Kruchko, C.; Benzel, E.C.; Barnholtz-Sloan, J.S. Descriptive epidemiology of spinal meningiomas in the United States. Spine 2015, 40, E886–E889. [Google Scholar] [CrossRef] [PubMed]
- Maiti, T.K.; Bir, S.C.; Patra, D.P.; Kalakoti, P.; Guthikonda, B.; Nanda, A. Spinal meningiomas: Clinicoradiological factors predicting recurrence and functional outcome. Neurosurg. Focus 2016, 41, E6. [Google Scholar] [CrossRef]
- Ravindra, V.M.; Schmidt, M.H. Management of spinal meningiomas. Neurosurg. Clin. N. Am. 2016, 27, 195–205. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Menezes, A.H.; Shimizu, K.; Woodroffe, R.W.; Helland, L.C.; Hitchon, P.W.; Howard, M.A. Differences and characteristics of symptoms by tumor location, size, and degree of spinal cord compression: A retrospective study on 53 surgically treated, symptomatic spinal meningiomas. J. Neurosurg. Spine 2020, 32, 931–940. [Google Scholar] [CrossRef]
- Koeller, K.K.; Shih, R.Y. Intradural extramedullary spinal neoplasms: Radiologic-pathologic correlation. Radiographics 2019, 39, 468–490. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Tsuji, O.; Fujiyoshi, K.; Hosogane, N.; Watanabe, K.; Tsuji, T.; Ishii, K.; Toyama, Y.; Chiba, K.; Matsumoto, M. Long-term surgical outcomes of spinal meningiomas. Spine 2012, 37, E617–E623. [Google Scholar] [CrossRef]
- Westwick, H.J.; Yuh, S.-J.; Shamji, M.F. Complication avoidance in the resection of spinal meningiomas. World Neurosurg. 2015, 83, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Voldřich, R.; Netuka, D.; Beneš, V. Spinal meningiomas: Is Simpson grade II resection radical enough? Acta Neurochir. 2020, 162, 1401–1408. [Google Scholar] [CrossRef]
- Kim, C.H.; Chung, C.K.; Lee, S.-H.; Jahng, T.-A.; Hyun, S.-J.; Kim, K.-J.; Yoon, S.H.; Kim, E.-S.; Eoh, W.; Kim, H.-J.; et al. Long-term recurrence rates after the removal of spinal meningiomas in relation to Simpson grades. Eur. Spine J. 2016, 41, 4025–4032. [Google Scholar] [CrossRef] [PubMed]
- Frati, A.; Pesce, A.; Toccaceli, G.; Fraschetti, F.; Caruso, R.; Raco, A. Spinal Meningiomas Prognostic Evaluation Score (SPES): Predicting the neurological outcomes in spinal meningioma surgery. Neurosurg. Rev. 2019, 42, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Raco, A.; Pesce, A.; Toccaceli, G.; Domenicucci, M.; Miscusi, M.; Delfini, R. Factors leading to a poor functional outcome in spinal meningioma surgery: Remarks on 173 cases. Neurosurgery 2017, 80, 602–609. [Google Scholar] [CrossRef]
- Hua, L.; Zhu, H.; Deng, J.; Tian, M.; Jiang, X.; Tang, H.; Luan, S.; Wakimoto, H.; Xie, Q.; Gong, Y. Clinical and prognostic features of spinal meningioma: A thorough analysis from a single neurosurgical center. J. Neurooncol. 2018, 140, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Gilard, V.; Goia, A.; Ferracci, F.X.; Marguet, F.; Magne, N.; Langlois, O.; Perez, A.; Derrey, S. Spinal meningioma and factors predictive of post-operative deterioration. J. Neurooncol. 2018, 140, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Setzer, M.; Vatter, H.; Marquardt, G.; Seifert, V.; Vrionis, F.D. Management of spinal meningiomas: Surgical results and a review of the literature. Neurosurg. Focus 2007, 23, E14. [Google Scholar] [CrossRef]
- Bayoumi, A.B.; Laviv, Y.; Karaali, C.N.; Ertilav, K.; Kepoglu, U.; Toktas, Z.O.; Konya, D.; Kasper, E.M. Spinal meningiomas: 61 cases with predictors of early postoperative surgical outcomes. J. Neurosurg. Sci. 2017, 64, 446–451. [Google Scholar] [PubMed]
- Schaller, B. Spinal meningioma: Relationship between histological subtypes and surgical outcome? J. Neurooncol. 2005, 75, 157–161. [Google Scholar] [CrossRef]
- Gezen, F.; Kahraman, S.; Çanakci, Z.; Bedük, A. Review of 36 cases of spinal cord meningioma. Spine 2000, 25, 727–731. [Google Scholar] [CrossRef]
- Haegelen, C.; Morandi, X.; Riffaud, L.; Amlashi, S.F.A.; Leray, E.; Brassier, G. Results of spinal meningioma surgery in patients with severe preoperative neurological deficits. Eur. Spine J. 2005, 14, 440–444. [Google Scholar] [CrossRef] [Green Version]
- Arima, H.; Takami, T.; Yamagata, T.; Naito, K.; Abe, J.; Shimokawa, N.; Ohata, K. Surgical management of spinal meningiomas: A retrospective case analysis based on preoperative surgical grade. Surg. Neurol. Int. 2014, 5, S333–S338. [Google Scholar]
- Klekamp, J.; Samii, M. Surgical results for spinal meningiomas. Surg. Neurol. 1999, 52, 552–562. [Google Scholar] [CrossRef]
- Sacko, O.; Haegelen, C.; Mendes, V.; Brenner, A.; Sesay, M.; Brauge, D.; Lagarrigue, J.; Loiseau, H.; Roux, F.E. Spinal meningioma surgery in elderly patients with paraplegia or severe paraparesis: A multicenter study. Neurosurgery 2009, 64, 503–509. [Google Scholar] [CrossRef]
- Morandi, X.; Haegelen, C.; Riffaud, L.; Amlashi, S.; Adn, M.; Brassier, G. Results in the operative treatment of elderly patients with spinal meningiomas. Spine 2004, 29, 2191–2194. [Google Scholar] [CrossRef]
- Helseth, A.; Mork, S.J. Primary intraspinal neoplasms in Norway, 1955 to 1986: A population-based survey of 467 patients. J. Neurosurg. 1989, 71, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Iacoangeli, M.; Gladi, M.; Di Rienzo, A.; Dobran, M.; Alvaro, L.; Nocchi, N.; Maria, L.G.; Somma, D.; Colasanti, R.; Scerrati, M. Minimally invasive surgery for benign intradural extramedullary spinal meningiomas: Experience of a single institution in a cohort of elderly patients and review of the literature. Clin. Interv. Aging 2012, 7, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dripps, R.D.; Lamont, A.; Eckenhoff, J.E. The role of anesthesia in surgical mortality. J. Am. Med. Assoc. 1961, 178, 261–266. [Google Scholar] [CrossRef]
- Bartek, J.; Sjåvik, K.; Förander, P.; Solheim, O.; Gulati, S.; Weber, C.; Ingebrigtsen, T.; Jakola, A.S. Predictors of severe complications in intracranial meningioma surgery: A population-based multicenter study. World Neurosurg. 2015, 83, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Rautalin, I.; Niemelä, M.; Korja, M. Is surgery justified for 80-year-old or older intracranial meningioma patients? A systematic review. Neurosurg. Rev. 2020, 44, 1061–1069. [Google Scholar] [CrossRef] [Green Version]
- Turrentine, F.E.; Wang, H.; Simpson, V.B.; Jones, R.S. Surgical risk factors, morbidity, and mortality in elderly patients. J. Am. Coll. Surg. 2006, 203, 865–877. [Google Scholar] [CrossRef]
- Engel, D.C.; Gawellek, L.; Peraio, S.; Stanojevic, M.; Tatagiba, M.; Ebner, F.H. Spinal meningioma surgery in the elderly: Who benefits? J. Neurosurg. Sci. 2018. [Google Scholar] [CrossRef]
- McCormick, P.C.; Post, K.D.; Stein, B.M. Intradural extramedullary tumors in adults. Neurosurg. Clin. N. Am. 1990, 1, 591–608. [Google Scholar] [CrossRef]
- Cohen-Gadol, A.A.; Zikel, O.M.; Koch, C.A.; Scheithauer, B.W.; Krauss, W.E. Spinal meningiomas in patients younger than 50 years of age: A 21-year experience. J. Neurosurg. 2003, 98, 258–263. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: http://www.r-project.org/ (accessed on 1 February 2021).
- King, A.T.; Sharr, M.M.; Gullan, R.W.; Bartlett, J.R. Spinal meningiomas: A 20-year review. Br. J. Neurosurg. 1998, 12, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Saraceni, C.; Harrop, J.S. Spinal meningioma: Chronicles of contemporary neurosurgical diagnosis and management. Clin. Neurol. Neurosurg. 2009, 111, 221–226. [Google Scholar] [CrossRef]
- Hohenberger, C.; Gugg, C.; Schmidt, N.O.; Zeman, F.; Schebesch, K.M. Functional outcome after surgical treatment of spinal meningioma. J. Clin. Neurosci. 2020, 77, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Sandalcioglu, I.E.; Hunold, A.; Müller, O.; Bassiouni, H.; Stolke, D.; Asgari, S. Spinal meningiomas: Critical review of 131 surgically treated patients. Eur. Spine J. 2008, 17, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Mirian, C.; Skyrman, S.; Bartek, J.; Jensen, L.R.; Kihlström, L.; Förander, P.; Orrego, A.; Mathiesen, T. The Ki-67 proliferation index as a marker of time to recurrence in intracranial meningioma. Neurosurgery 2020, 87, 1289–1298. [Google Scholar] [CrossRef]
- Gallagher, M.J.; Jenkinson, M.D.; Brodbelt, A.R.; Mills, S.J.; Chavredakis, E. WHO grade 1 meningioma recurrence: Are location and Simpson grade still relevant? Clin. Neurol. Neurosurg. 2016, 141, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Boström, A.; Bürgel, U.; Reinacher, P.; Krings, T.; Rohde, V.; Gilsbach, J.M.; Hans, F.J. A less invasive surgical concept for the resection of spinal meningiomas. Acta Neurochir. 2008, 150, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Pettersson-Segerlind, J.; Orrego, A.; Lönn, S.; Mathiesen, T. Long-term 25-year follow-up of surgically treated parasagittal meningiomas. World Neurosurg. 2011, 76, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Epstein, N. Nursing review of spinal meningiomas. Surg. Neurol. Int. 2018, 9, 41. [Google Scholar] [CrossRef]
- Persson, O.; Fletcher-Sandersjöö, A.; Burström, G.; Edström, E.; Elmi-Terander, A. Surgical treatment of intra- and juxtamedullary spinal cord tumors: A population based observational cohort study. Front. Neurol. 2019, 10, 814. [Google Scholar] [CrossRef] [Green Version]
- Zuo, M.R.; Liang, R.F.; Li, M.; Xiang, Y.F.; Zhang, S.X.; Yang, Y.; Wang, X.; Mao, Q.; Liu, Y.H. A comprehensive study of risk factors for post-operative pneumonia following resection of meningioma. BMC Cancer 2019, 19, 100. [Google Scholar] [CrossRef]
- Nunno, A.; Li, Y.; Pieters, T.A.; Towner, J.E.; Schmidt, T.; Shi, M.; Walter, K.; Li, Y.M. Risk factors and associated complications of symptomatic venous thromboembolism in patients with craniotomy for meningioma. World Neurosurg. 2019, 122, e1505–e1510. [Google Scholar] [CrossRef] [PubMed]
- Lemée, J.M.; Corniola, M.V.; Da Broi, M.; Schaller, K.; Meling, T.R. Early postoperative complications in meningioma: Predictive factors and impact on outcome. World Neurosurg. 2019, 128, e851–e858. [Google Scholar] [CrossRef]
- Carrabba, G.; Riva, M.; Conte, V.; Di Cristofori, A.; Caroli, M.; Locatelli, M.; Castellani, M.; Bucciarelli, P.; Artoni, A.; Stocchetti, N.; et al. Risk of post-operative venous thromboembolism in patients with meningioma. J. Neurooncol. 2018, 138, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Brokinkel, B.; Holling, M.; Spille, D.C.; Heß, K.; Sauerland, C.; Bleimüller, C.; Paulus, W.; Wölfer, J.; Stummer, W. Surgery for meningioma in the elderly and long-term survival: Comparison with an age- and sex-matched general population and with younger patients. J. Neurosurg. 2017, 126, 1201–1211. [Google Scholar] [CrossRef] [Green Version]
- Maiuri, F.; Del Basso De Caro, M.L.; De Divitiis, O.; Vergara, P.; Mariniello, G. Spinal meningiomas: Age-related features. Clin. Neurol. Neurosurg. 2011, 113, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Ekşi, M.Ş.; Canbolat, Ç.; Akbaş, A.; Özmen, B.B.; Akpınar, E.; Usseli, M.İ.; Güngör, A.; Güdük, M.; Hacıhanefioğlu, M.; Erşen Danyeli, A.; et al. Elderly patients with intracranial meningioma: Surgical considerations in 228 patients with a comprehensive analysis of the literature. World Neurosurg. 2019, 132, e350–e365. [Google Scholar] [CrossRef] [PubMed]
- Soriano Sánchez, J.A.; Soto García, M.E.; Soriano Solís, S.; Rodríguez García, M.; Trejo Huerta, P.; Sánchez Escandón, O.; Flores Soria, E.R.; Romero-Rangel, J.A.I. Microsurgical resection of intraspinal benign tumors using non-expansile tubular access. World Neurosurg. 2020, 133, e97–e104. [Google Scholar] [CrossRef] [PubMed]
- Thavara, B.; Kidangan, G.; Rajagopalawarrier, B. Analysis of the surgical technique and outcome of the thoracic and lumbar intradural spinal tumor excision using minimally invasive tubular retractor system. Asian J. Neurosurg. 2019, 14, 453. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yu, B.F.; Liu, C.H.; Zheng, W.; Xiao, Y.H.; Lin, Y. Microscopic keyhole technique for surgical removal of thoracic spinal meningiomas. World Neurosurg. 2019, 124, e373–e379. [Google Scholar] [CrossRef]
- Raygor, K.P.; Than, K.D.; Chou, D.; Mummaneni, P.V. Comparison of minimally invasive transspinous and open approaches for thoracolumbar intradural-extramedullary spinal tumors. Neurosurg. Focus 2015, 39, E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatter, C.; Fletcher-Sandersjöö, A.; Persson, O.; Burström, G.; Grane, P.; Edström, E.; Elmi-Terander, A. Incidence and predictors of kyphotic deformity following resection of cervical intradural tumors in adults: A population-based cohort study. Acta Neurochir. 2020, 162, 2905–2913. [Google Scholar] [CrossRef]
- Mathiesen, T.; Lindquist, C.; Kihlström, L.; Karlsson, B. Recurrence of cranial base meningiomas. Neurosurgery 1996, 39, 2–9. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Explanation |
|---|---|
| 1 | Intact neurologically, normal ambulation, minimal dysesthesia |
| 2 | Mild motor or sensory deficit, functional independence |
| 3 | Moderate deficit, limitation of function, independent w/external aid |
| 4 | Severe motor or sensory deficit, limited function, dependent |
| 5 | Paraplegia or quadriplegia, even w/flickering movement |
| Variables | All Patients (n = 129) | Elderly (n = 46) | Non-Elderly (n = 83) | p-Value |
|---|---|---|---|---|
| Age (years) | 65 (23–94) | 76 (70–94) | 58 (23–69) | - |
| Male sex | 23 (18%) | 10 (22%) | 13 (16%) | 0.388 |
| ASA class | 2 (1–3) | 3 (2–3) | 2 (1–3) | 0.023 |
| Prior radiotherapy | 2 (1.6%) | 0 (0%) | 2 (2.4%) | - |
| Prior spinal surgery | 1 (0.8%) | 1 (2.2%) | 0 (0%) | - |
| Concurrent cranial meningioma | 8 (6%) | 2 (4%) | 6 (7%) | - |
| Neurofibromatosis type 2 | 1 (0.8%) | 0 (0%) | 1 (1.2%) | - |
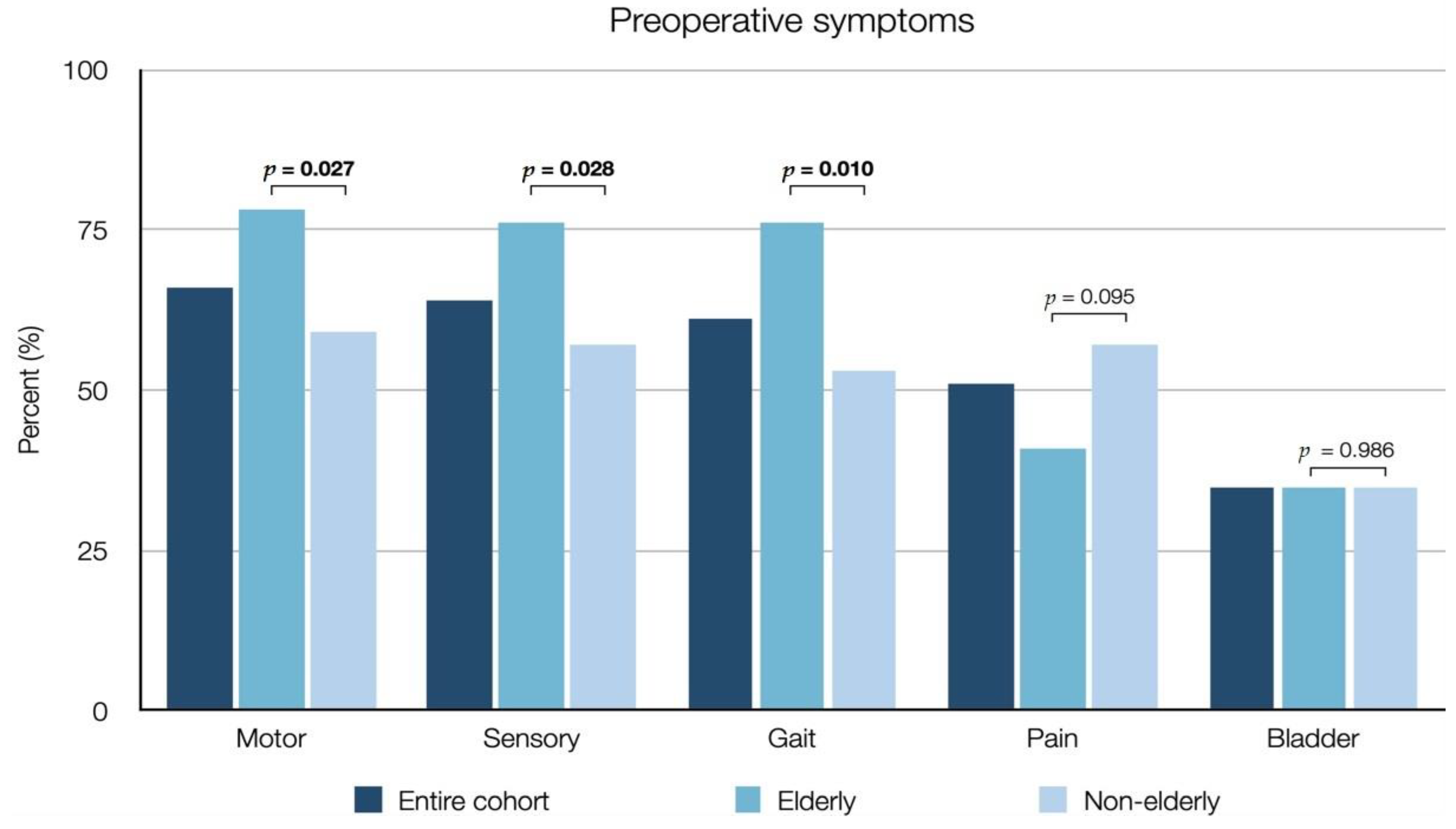
| Neurological deficits | ||||
| Motor deficit | 85 (66%) | 36 (78%) | 49 (59%) | 0.027 |
| Sensory deficit | 82 (64%) | 35 (76%) | 47 (57%) | 0.028 |
| Gait disturbance | 79 (61%) | 35 (76%) | 44 (53%) | 0.010 |
| Bladder dysfunction | 45 (35%) | 16 (35%) | 29 (35%) | 0.986 |
| Pain | 66 (51%) | 19 (41%) | 47 (57%) | 0.095 |
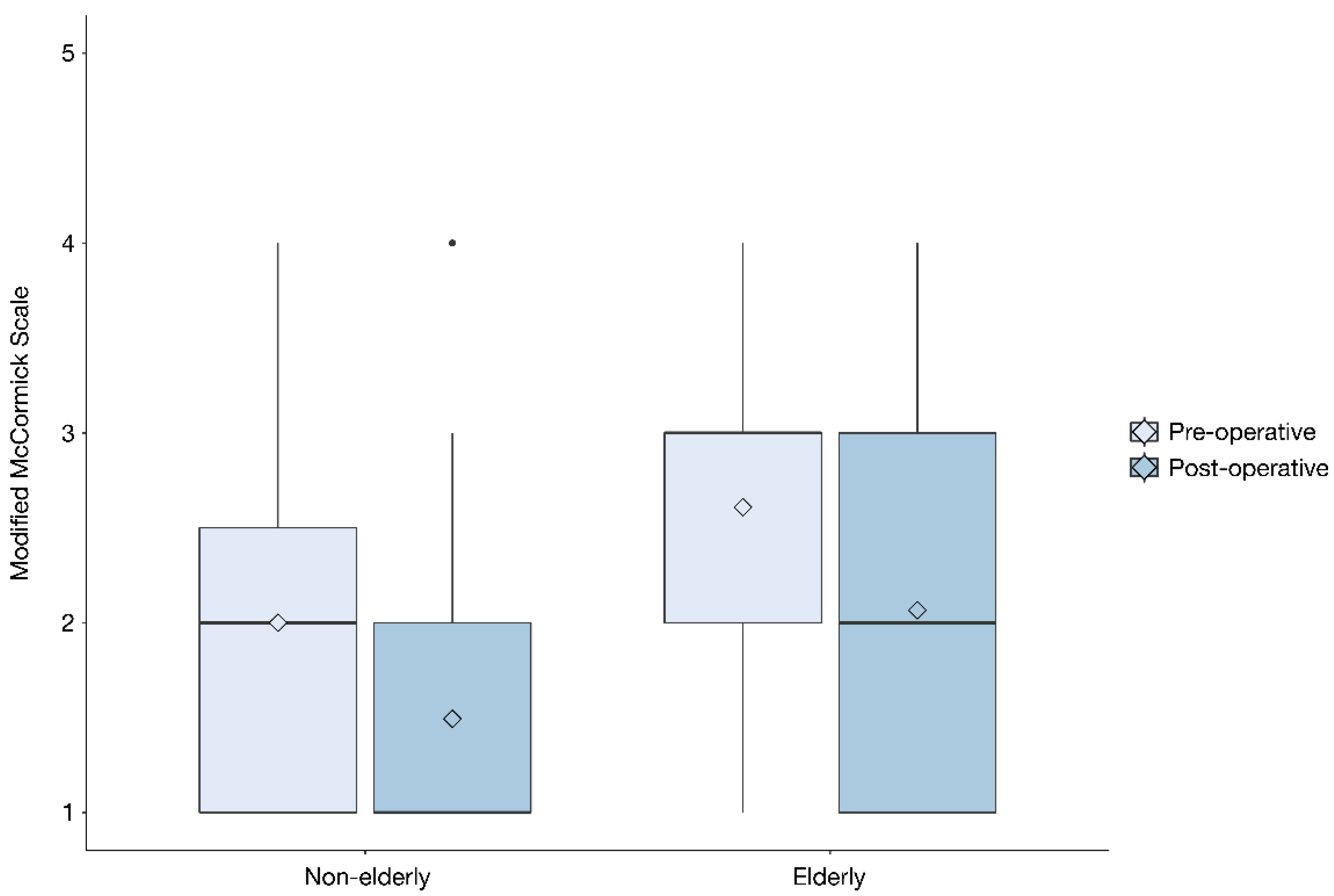
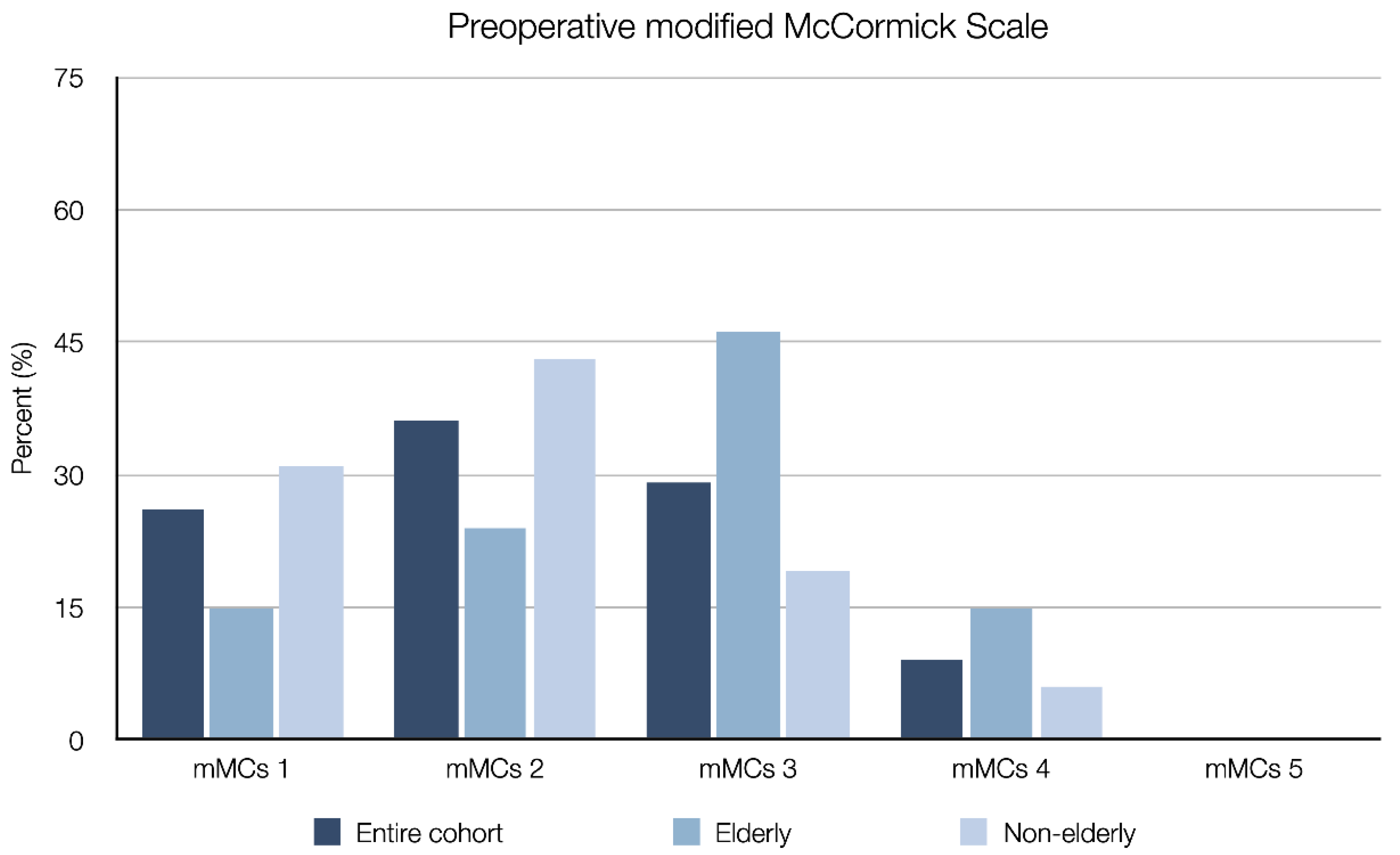
| Modified McCormick scale (mMCs) | 2 (1–4) | 3 (1–4) | 2 (1–4) | <0.001 |
| mMCs 1 | 33 (26%) | 7 (15%) | 26 (31%) | - |
| mMCs 2 | 47 (36%) | 11 (24%) | 36 (43%) | - |
| mMCs 3 | 37 (29%) | 21 (46%) | 16 (19%) | - |
| mMCs 4 | 12 (9.3%) | 7 (15%) | 5 (6.0%) | - |
| mMCs 5 | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Tumor level | ||||
| Cervical | 39 (30%) | 12 (26%) | 27 (33%) | 0.445 |
| Thoracic | 89 (69%) | 34 (74%) | 55 (66%) | - |
| Lumbar | 1 (0.8%) | 0 (0%) | 1 (1.2%) | - |
| Anterior tumor component | 30 (23%) | 14 (30%) | 16 (19%) | 0.151 |
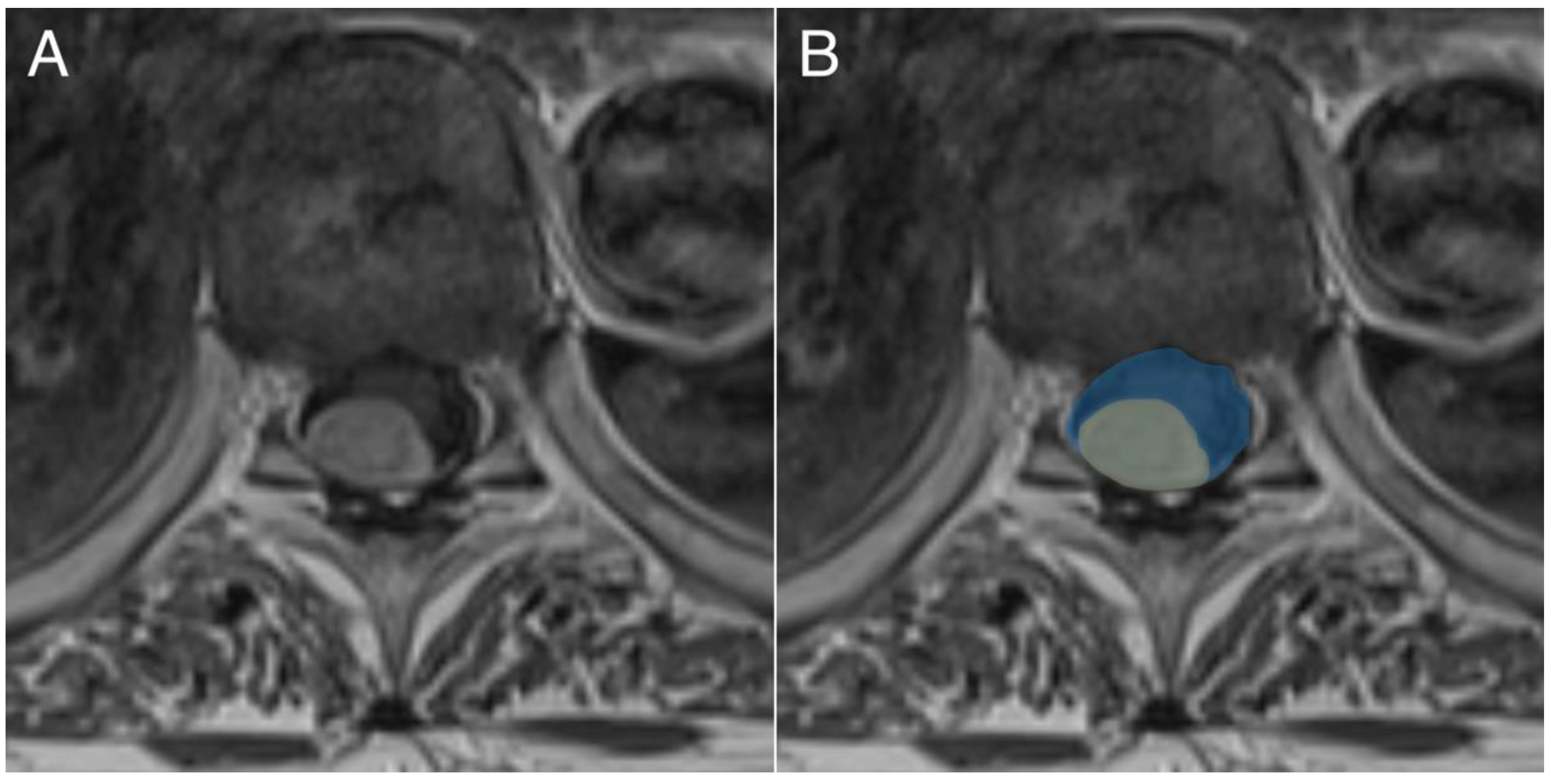
| Tumor area (cm2) | 1.4 (0.2–4.5) | 1.4 (0.4–3.1) | 1.4 (0.2–4.5) | 0.689 |
| Spinal cord compression (%) | 69 (12–89) | 69 (20–89) | 69 (12–89) | 0.303 |
| Variable | All Patients (n = 129) | Elderly (n = 46) | Non-Elderly (n = 83) | p-Value |
|---|---|---|---|---|
| Time from diagnosis to surgery (months) | 1.3 (0.03–36) | 0.5 (0.03–36) | 1.8 (0.03–30) | 0.005 |
| Laminectomy range (levels) | 3 (1–6) | 3 (1–6) | 2 (1–5) | 0.803 |
| Laminoplasty | 35 (27%) | 9 (20%) | 26 (31%) | 0.150 |
| Simpson grade | ||||
| Simpson grade 1 | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Simpson grade 2 | 92 (71%) | 32 (70%) | 60 (72%) | 0.743 |
| Simpson grade 3 | 17 (13%) | 6 (13%) | 11 (13%) | 0.973 |
| Simpson grade 4 | 20 (16%) | 8 (17%) | 12 (14%) | 0.194 |
| Simpson grade 5 | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Histopathological data | ||||
| Meningioma WHO grade 1 | 127 (98%) | 45 (98%) | 82 (99%) | 0.670 |
| Meningioma WHO grade 2 | 2 (1.5%) | 1 (2.2%) | 1 (1.2%) | - |
| Meningioma WHO grade 3 | 0 (0%) | 0 (0%) | 0 (0%) | - |
| MIB1-index (%) | 4.5 (0–20) | 4.8 (1.0–20) | 4.0 (0–15) | 0.944 |
| Postoperative radiotherapy | 1 (0.8%) | 1 (2.2%) | 0 (0%) | - |
| Postoperative chemotherapy | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Variable | All Patients (n = 129) | Elderly (n = 46) | Non-Elderly (n = 83) | p-Value |
|---|---|---|---|---|
| Time to initial follow-up (months) | 4.6 (2.7–10) | 4.7 (3.2–9.2) | 4.4 (2.7–9.8) | 0.516 |
| Long-term follow-up time (years) | 8.2 (0.3–16) | 6.8 (0.3–16) | 8.6 (3.1–16) | 0.117 |
| Postoperative complication | 10 (7.8%) | 1 (0.8%) | 9 (11%) | 0.077 |
| Tethered spinal cord | 1 | 1 | 0 | - |
| Wound infection | 3 | 0 | 3 | - |
| Pneumonia | 1 | 0 | 1 | - |
| Cerebrospinal fluid leak | 2 | 0 | 2 | - |
| Kyphosis | 2 | 0 | 2 | - |
| Myocardial infarction | 1 | 0 | 1 | - |
| Reoperation | 4 (3.1%) | 2 (4.3%) | 2 (2.4%) | 0.543 |
| Tethered spinal cord | 1 | 1 | 0 | - |
| Tumor resection (local tumor recurrence) | 2 | 1 | 1 | - |
| Wound revision (infection) | 1 | 0 | 1 | - |
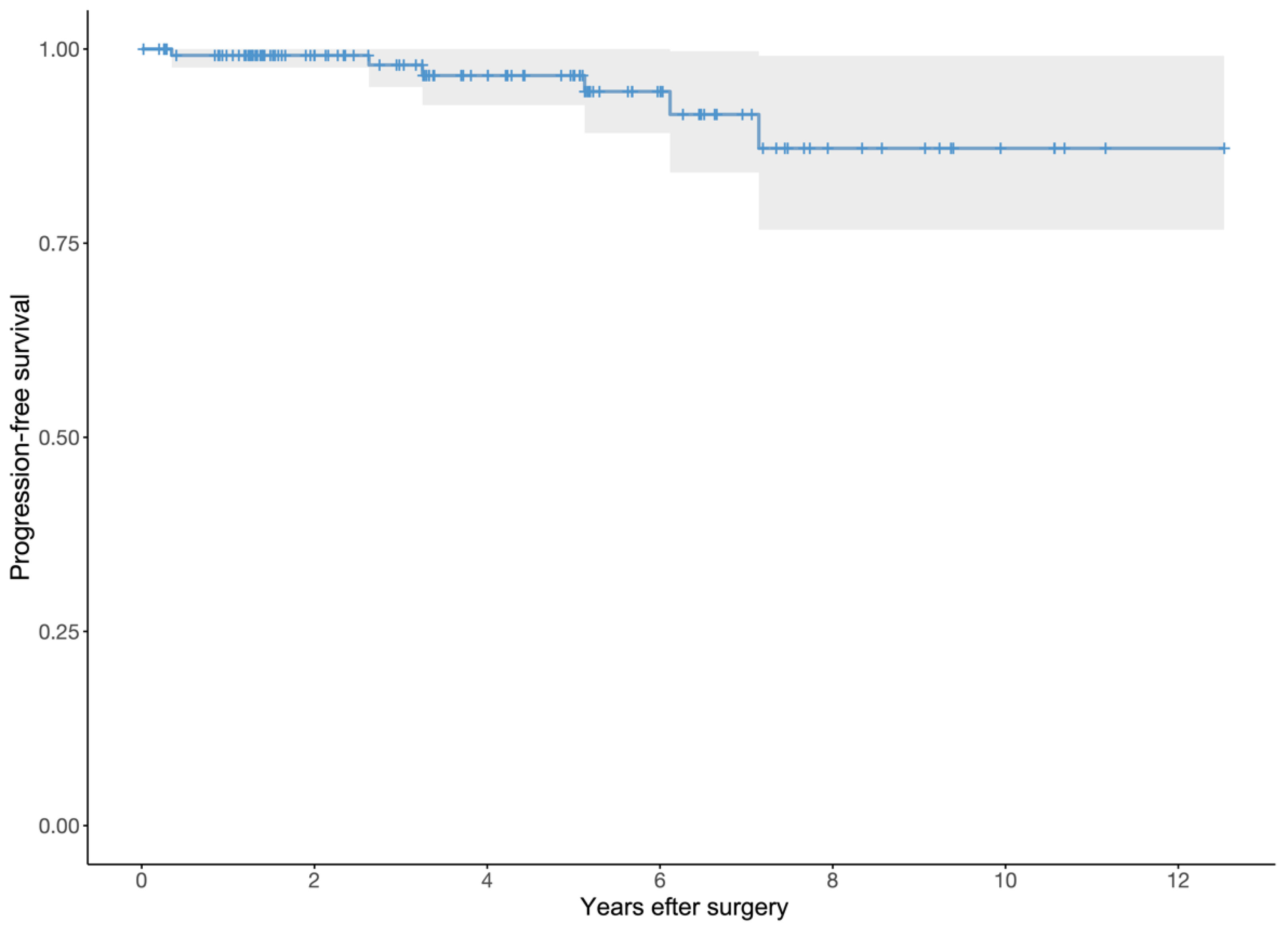
| Tumor growth/recurrence | 6 (4.7%) | 1 (2.2%) | 5 (6.0%) | 0.320 |
| Local recurrence | 2 | 1 | 1 | - |
| Local progression | 4 | 0 | 4 | - |
| Change in mMCs | 0 (−1–3) | 0.5 (0–2) | 0 (−1–3) | 0.629 |
| Improved | 61 (47%) | 23 (50%) | 38 (46%) | 0.646 |
| Unchanged | 66 (51%) | 23 (50%) | 43 (52%) | 0.844 |
| Worse | 2 (1.6%) | 0 (0%) | 2 (2.4%) | - |
| Mortality | ||||
| 3-month mortality | 0 (0%) | 0 (0%) | 0 (0%) | - |
| Long-term mortality | 27 (21%) | 22 (48%) | 5 (6.0%) | <0.001 |
| Tumor-related death | 1 (1%) | 1 (2%) | 0 (0%) | - |
| Years from surgery to death | 6.6 (0.3–15) | 5.9 (0.3–15) | 8.5 (3.1–12) | - |
| Postoperative Change | Motor | Sensory | Gait | Bladder | Pain |
|---|---|---|---|---|---|
| Patients with preoperative deficit (n) | 85 | 82 | 79 | 45 | 66 |
| Completely resolved | 39 (46%) | 38 (46%) | 40 (51%) | 34 (76%) | 35 (53%) |
| Unchanged/partial improvement | 46 (54%) | 44 (54%) | 39 (49%) | 11 (24%) | 31 (47%) |
| Worse (increased deficit) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Worse (new deficit) | 2 | 4 | 2 | 2 | 9 |
| p-value (paired testing) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Variable | p-Value | OR (95% CI) | Nagelkerke’s R2 |
|---|---|---|---|
| Elderly | 0.646 | - | |
| Male sex | 0.330 | - | |
| ASA class ≥ 3 | 0.589 | - | |
| Months to surgery | 0.005 | 0.86 (0.76–0.94) | 0.141 |
| Cervical tumor | 0.830 | - | |
| Anterior tumor | 0.734 | - | |
| Tumor area (cm2) | 0.030 | 1.73 (1.00–3.17) | 0.053 |
| Spinal cord compression (%) | <0.001 | 1.03 (1.01–1.06) | 0.137 |
| MIB1-index | 0.053 | - | |
| Simpson grade ≥ 3 | 0.690 | - |
| Variable | p-Value |
|---|---|
| Included in final step-down model | |
| Spinal cord compression | 0.002 |
| Not included in final step-down model | |
| Months to surgery | >0.05 |
| Tumor area | >0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; Tatter, C.; Burström, G.; Persson, O.; Förander, P.; Mathiesen, T.; Bartek, J., Jr.; Edström, E.; Elmi-Terander, A. Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study. Cancers 2021, 13, 3244. https://doi.org/10.3390/cancers13133244
Pettersson-Segerlind J, Fletcher-Sandersjöö A, Tatter C, Burström G, Persson O, Förander P, Mathiesen T, Bartek J Jr., Edström E, Elmi-Terander A. Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study. Cancers. 2021; 13(13):3244. https://doi.org/10.3390/cancers13133244
Chicago/Turabian StylePettersson-Segerlind, Jenny, Alexander Fletcher-Sandersjöö, Charles Tatter, Gustav Burström, Oscar Persson, Petter Förander, Tiit Mathiesen, Jiri Bartek, Jr., Erik Edström, and Adrian Elmi-Terander. 2021. "Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study" Cancers 13, no. 13: 3244. https://doi.org/10.3390/cancers13133244
APA StylePettersson-Segerlind, J., Fletcher-Sandersjöö, A., Tatter, C., Burström, G., Persson, O., Förander, P., Mathiesen, T., Bartek, J., Jr., Edström, E., & Elmi-Terander, A. (2021). Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study. Cancers, 13(13), 3244. https://doi.org/10.3390/cancers13133244