
Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Definitions
2.4. Analyzed Data
2.5. Statistics
3. Results
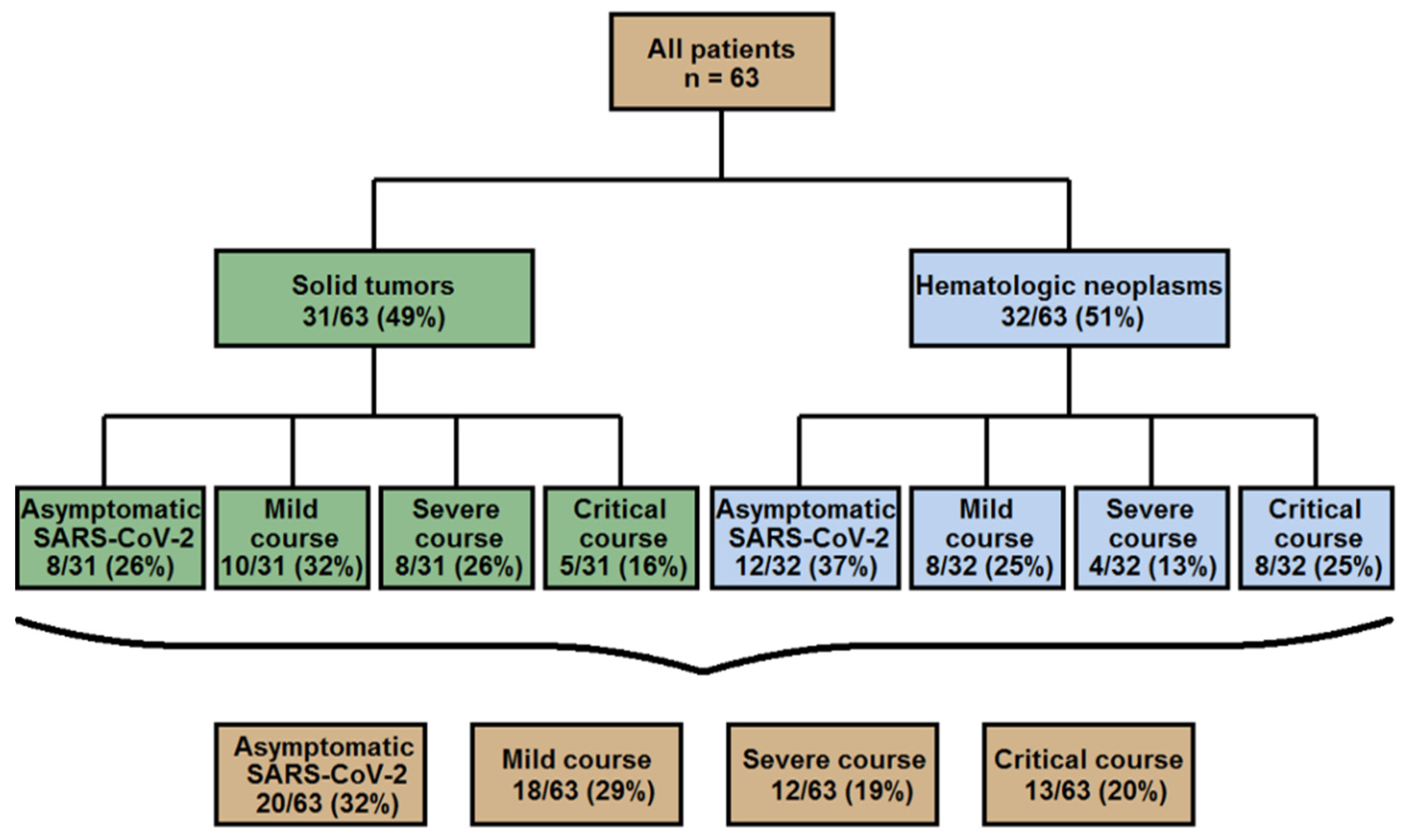
3.1. Characteristics of Cancer Patients Positive for SARS-CoV-2
3.2. Clinical, Laboratory and Imaging Findings in 63 Cancer Patients with SARS-CoV-2
3.3. Course of the SARS-CoV-2 Infection
3.3.1. Asymptomatic SARS-CoV-2 Patients
3.3.2. SARS-CoV-2 Infection with COVID-19 Symptoms
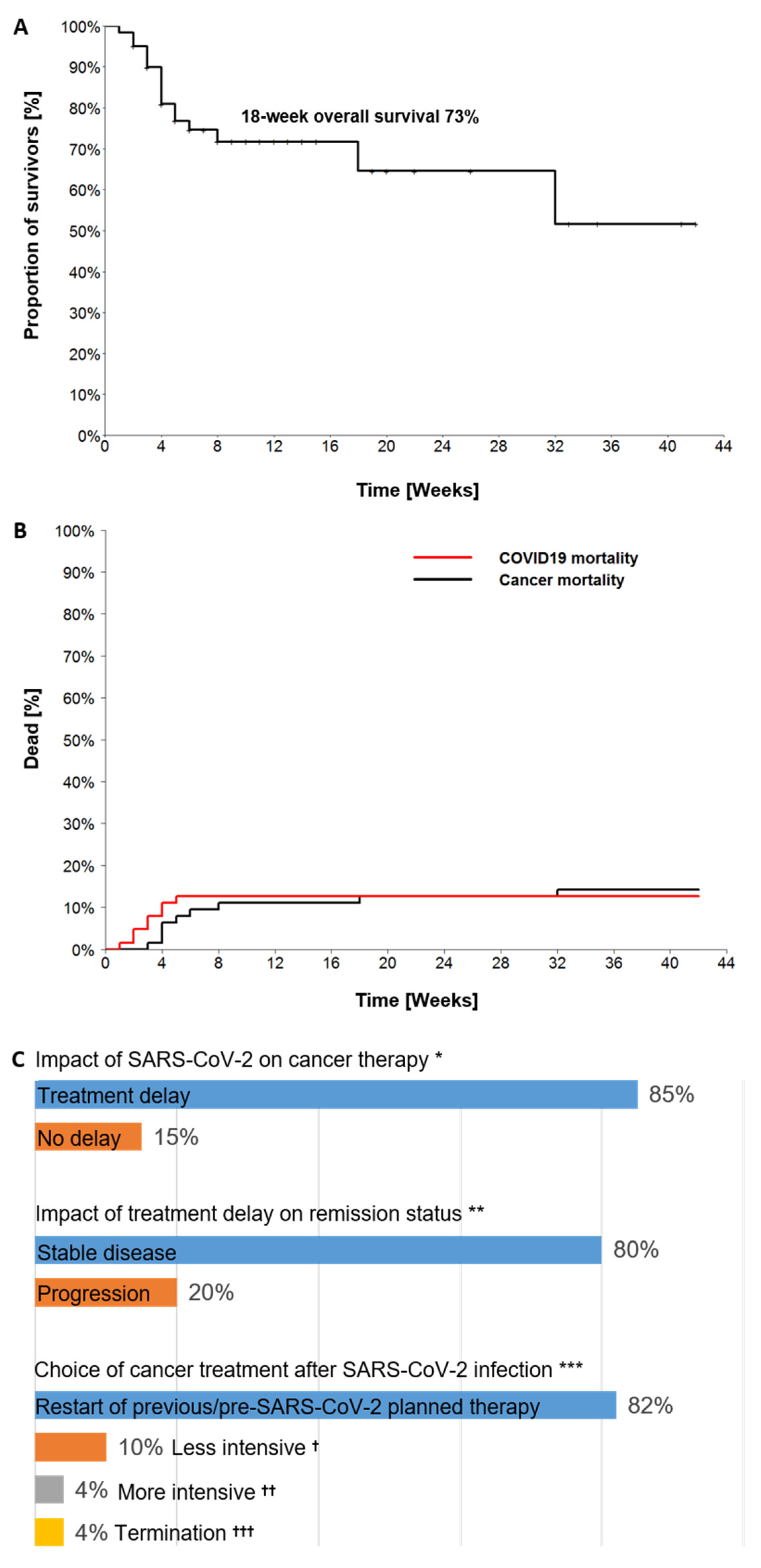
3.3.3. Outcomes of SARS-CoV-2 Infection with Impact on Cancer Course
4. Discussion
5. Conclusions
- At diagnosis of SARS-CoV-2 infection in cancer patients, the likelihood of an asymptomatic or mild course of COVID-19 seems to be greater than that of a severe or critical one.
- Cancer patients diagnosed in an asymptomatic phase of a SARS-CoV-2 infection have around a 30% probability for the subsequent development of COVID-19.
- Diagnostic and clinical pitfalls such as a lack of seroconversion post-SARS-CoV-2 in some of the cancer patients should be considered when planning the management of SARS-CoV-2 infection and subsequent cancer therapy.
- Cancer patients with peri-SARS-CoV-2 lymphocytopenia are especially at risk for the development of a severe or critical COVID-19 course and should be monitored carefully.
- Secondary bacterial infection, presented predominantly by gram-negative bacteria, is common in cancer patients with critical COVID-19 and should be included in a diagnostic and treatment workup for such cases.
- Even though the COVID-19 mortality is higher in cancer patients as compared to non-cancer individuals, the frequency of ICU admission does not necessarily differ significantly compared with non-cancer COVID-19 patients.
- A delay in cancer treatment is extremely likely following SARS-CoV-2 infection and requires thorough clinical and diagnostic surveillance to enable for the earliest possible restart of treatment.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shields, A.M.; Burns, S.O.; Savis, S.; Richter, A.G. COVID-19 in patients with primary and secondary immunodeficiency: The United Kingdom experience. J. Allergy Clin. Immunol. 2021, 147, 870–875.e1. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Worldwide Cancer Incidence Statistics. 2018. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/worldwide-cancer/incidence#heading-Zero (accessed on 14 November 2018).
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Desai, A.; Sachdeva, S.; Parekh, T.; Desai, R. COVID-19 and Cancer: Lessons from a Pooled Meta-Analysis. JCO Glob. Oncol. 2020, 6, 557–559. [Google Scholar] [CrossRef]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; De Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Erdal, G.S.; Polat, O.; Erdem, G.U.; Korkusuz, R.; Hindilerden, F.; Yilmaz, M.; Yasar, K.K.; Isiksacan, N.; Tural, D. The mortality rate of COVID-19 was high in cancer patients: A retrospective single-center study. Int. J. Clin. Oncol. 2021, 26, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case Fatality Rate of Cancer Patients with COVID-19 in a New York Hospital System. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef]
- Bernard, A.; Cottenet, J.; Bonniaud, P.; Piroth, L.; Arveux, P.; Tubert-Bitter, P.; Quantin, C. Comparison of cancer patients to non-cancer patients among COVID-19 inpatients at a national level. Cancers 2021, 13, 1436. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Pinato, D.J.; Zambelli, A.; Aguilar-Company, J.; Bower, M.; Sng, C.C.T.; Salazar, R.; Bertuzzi, A.; Brunet, J.; Mesia, R.; Segui, E.; et al. Clinical Portrait of the SARS-CoV-2 Epidemic in European Patients with Cancer. Cancer Discov. 2020, 10, 1465–1474. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72/314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Bi, J.; Lin, Y.; Zhong, R.; Jiang, G.; Verma, V.; Shi, H.; Li, J.; Tong, X.; Li, Y.; Hu, D.; et al. Prevalence and clinical characterization of cancer patients with asymptomatic SARS-CoV-2 infection history. J. Infect. 2020, 81, e22–e24. [Google Scholar] [CrossRef]
- Hempel, L.; Piehler, A.; Pfaffl, M.W.; Molnar, J.; Kirchner, B.; Robert, S.; Veloso, J.; Gandorfer, B.; Trepotec, Z.; Mederle, S.; et al. SARS-CoV-2 infections in cancer outpatients—Most infected patients are asymptomatic carriers without impact on chemotherapy. Cancer Med. 2020, 9, 8020–8028. [Google Scholar] [CrossRef]
- Rüthrich, M.M.; Giessen-Jung, C.; Borgmann, S.; Classen, A.Y.; Dolff, S.; Grüner, B.; Hanses, F.; Isberner, N.; Köhler, P.; Lanznaster, J.; et al. COVID-19 in cancer patients: Clinical characteristics and outcome-an analysis of the LEOSS registry. Ann. Hematol. 2021, 100, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martin-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuiness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; De Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Shoumariyeh, K.; Biavasco, F.; Ihorst, G.; Rieg, S.; Nieters, A.; Kern, W.V.; Miething, C.; Duyster, J.; Engelhardt, M.; Bertz, H. Covid-19 in patients with hematological and solid cancers at a Comprehensive Cancer Center in Germany. Cancer Med. 2020, 9, 8412–8422. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Windisch, W.; McAuley, D.F.; Welte, T.; Busse, R. Major differences in ICU admissions during the first and second COVID-19 wave in Germany. Lancet Respir. Med. 2021, 9, e47–e48. [Google Scholar] [CrossRef]
- Arcari, G.; Raponi, G.; Sacco, F.; Bibbolini, G.; Di Lella, F.M.; Alessandri, F.; Coletti, M.; Trancassini, M.; Deales, A.; Pugliese, F.; et al. Klebsiella pneumoniae infections in COVID-19 patients: A 2-month retrospective analysis in an Italian hospital. Int. J. Antimicrob. Agents 2021, 57, 106245. [Google Scholar] [CrossRef] [PubMed]
- Belvisi, V.; Del Borge, C.; Vita, S.; Redaelli, P.; Dolce, P.; Pacella, D.; Kertusha, B.; Carraro, A.; Marocco, R.; De Masi, M.; et al. Impact of SARS CoV-2 pandemic on carbapenemase-producing Klebsiella pneumoniae prevention and control programme: Convergent or divergent action? J. Hosp. Infect. 2021, 109, 29–31. [Google Scholar] [CrossRef]
- Luo, J.; Rizvi, H.; Preeshagul, I.R.; Egger, J.V.; Hoyos, D.; Bandlamudi, C.; McCarthy, C.G.; Falcon, C.J.; Schoenfeld, A.J.; Arbour, K.C.; et al. COVID-19 in patients with lung cancer. Ann Oncol. 2020, 31, 1386–1396. [Google Scholar] [CrossRef]
- Nie, L.; Dai, K.; Wu, J.; Zhou, X.; Hu, J.; Zhang, C.; Than, Y.; Song, Y.; Fan, W.; Hu, Z.; et al. Clinical characteristics and risk factors for in-hospital mortality of lung cancer patients with COVID-19: A multicenter, retrospective, cohort study. Thoracic. Cancer 2021, 12, 57–65. [Google Scholar] [CrossRef]
- Wood, W.A.; Neuberg, D.S.; Thompson, J.C.; Tallman, M.S.; Sekeres, M.A.; Sehn, L.H.; Anderson, K.C.; Goldberg, A.D.; Pennell, N.A.; Niemeyer, C.M.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A report from the ASH Research Collaborative Data Hub. Blood Adv. 2020, 4, 5966–5975. [Google Scholar] [CrossRef] [PubMed]
- Rogado, J.; Pangua, C.; Serrano-Montero, G.; Obispo, B.; Marino, A.M.; Pérez-Pérez, M.; López-Alfonso, A.; Gullón, P.; Lara, M.A. Covid-19 and lung cancer: A greater fatality rate? Lung Cancer 2020, 146, 19–22. [Google Scholar] [CrossRef]
- Bird, S.; Panopoulou, A.; Shea, R.L.; Tsui, M.; Saso, R.; Sud, A.; West, S.; Smith, K.; Barwood, J.; Kaczmarek, E.; et al. Response to first vaccination against SARS-CoV-2 in patients with multiple myeloma. Lancet Haematol. 2021, 8, e389–e392. [Google Scholar] [CrossRef]
- SITC Statement on SARS-CoV-2 Vaccination and Cancer Immunotherapy. SIT Cancer. 2020. Available online: https://www.sitcancer.org/aboutsitc/press-releases/2020/sitc-statement-sars-cov-2-vaccination-cancer-immunotherapy (accessed on 23 December 2020).
- National Comprehensive Cancer Network. Preliminary Recommendations of the NCCN COVID-19 Vaccination Advisory Committee Version 1.0 1/22/2021. NCCN, 2021. Available online: https://www.nccn.org/covid-19/pdf/COVID-19_Vaccination_Guidance_V1.0.pdf (accessed on 22 January 2021).
- Garassino, M.C.; Vyas, M.; De Vries, E.G.E.; Kanesvaran, R.; Giuliani, R.; Peters, S. The ESMO Call to Action on COVID-19 vaccinations and patients with cancer: Vaccinate. Monitor. Educate. Ann. Oncol. 2021, 32, 579–581. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients, n = 63 | |
|---|---|---|
| Gender (M/F), n (ratio) | 35/28 | 1.2 |
| Median age, years (range) | 62 | 19–85 |
| Cancer entities, n (%) | n = 63 (100%) | |
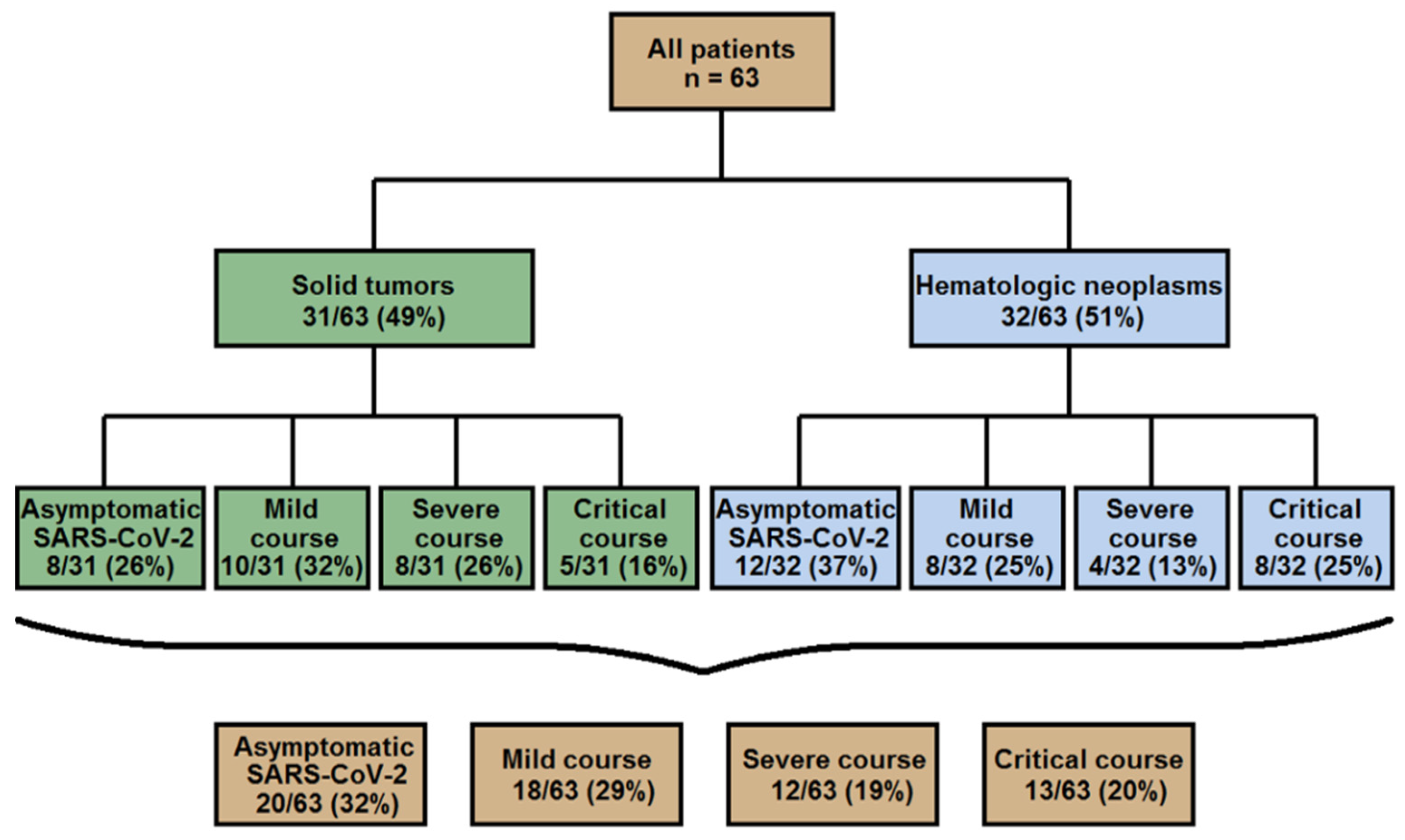
| Solid tumors, n (%) | 31/63 | (49%) |
| Lung cancer | 8 | 12% |
| Breast cancer | 7 | 11% |
| Gastrointestinal cancer | 7 | 11% |
| Sarcoma | 2 | 3% |
| Gynecologic cancer | 2 | 3% |
| Endocrine cancer | 2 | 3% |
| Glioma | 1 | 2% |
| Melanoma | 1 | 2% |
| Urogenital cancer | 1 | 2% |
| Hematologic neoplasms, n (%) | 32/63 | (51%) |
| Lymphoma | 22 | 35% |
| - B-NHL | 20 | 31% |
| - T-NHL | 1 | 2% |
| - Hodgkin lymphoma | 1 | 2% |
| Multiple myeloma | 2 | 3% |
| Acute leukemia | 7 | 11% |
| - ALL | 4 | 6% |
| - AML | 3 | 5% |
| PNH | 1 | 2% |
| Cancer treatment preceding SARS-CoV-2 positivity, n (%) | ||
| Conventional chemotherapy | 37 | 59% |
| - cytostatic agents only | 20 | 32% |
| - combined with immunotherapy | 10 | 16% |
| - combined with targeted therapy | 6 | 9% |
| - combined with radiotherapy | 1 | 2% |
| Immunotherapy | 7 | 11% |
| - immunotherapy monoregimen | 5 | 8% |
| - combined with radiotherapy | 2 | 3% |
| Targeted therapy | 4 | 6% |
| Surgery | 4 | 6% |
| Hormonal therapy | 1 | 2% |
| Radiotherapy | 1 | 2% |
| No therapy yet due to first diagnosis or “watch and wait” strategy | 2 | 3% |
| Aftercare following systemic cancer treatment | 7 | 11% |
| Number of therapy lines at SARS-CoV-2 positivity, n (%) | ||
| No therapy yet | 2 | 3% |
| One therapy line | 30 | 48% |
| Two therapy lines | 20 | 32% |
| Three therapy lines | 3 | 5% |
| ≥Four therapy lines | 8 | 12% |
| Remission status at SARS-CoV-2 positivity, n (%) | ||
| Complete remission | 12 | 19% |
| Partial remission | 12 | 19% |
| Stable disease | 11 | 17% |
| Relapsed/progressive disease | 20 | 32% |
| Not yet assessed | 8 | 13% |
| Comorbidities, n (%) | ||
| Cardiovascular disease | 37 | 59% |
| - arterial hypertension | 33 | 52% |
| - coronary artery disease | 9 | 14% |
| - chronic heart failure | 5 | 8% |
| - atrial fibrillation | 3 | 5% |
| Diabetes mellitus | 9 | 14% |
| Metachronous cancer in the history | 9 | 14% |
| Chronic respiratory disease | 7 | 11% |
| Chronic kidney failure | 7 | 11% |
| Obesity | 5 | 8% |
| Cerebrovascular disease | 4 | 6% |
| Autoimmune disorders | 4 | 6% |
| Chronic liver disease | 2 | 3% |
| No comorbidities | 18 | 29% |
| Coincidence of comorbidities, n (%) | ||
| One comorbidity | 16 | 25% |
| Two comorbidities | 15 | 24% |
| Three comorbidities | 9 | 14% |
| ≥Four comorbidities | 5 | 8% |
| Parameter | All Patients, n = 63 | |
|---|---|---|
| Median time from last cancer treatment to first positive SARS-CoV-2 RT-PCR test, days (range) | 13 | 0–904 |
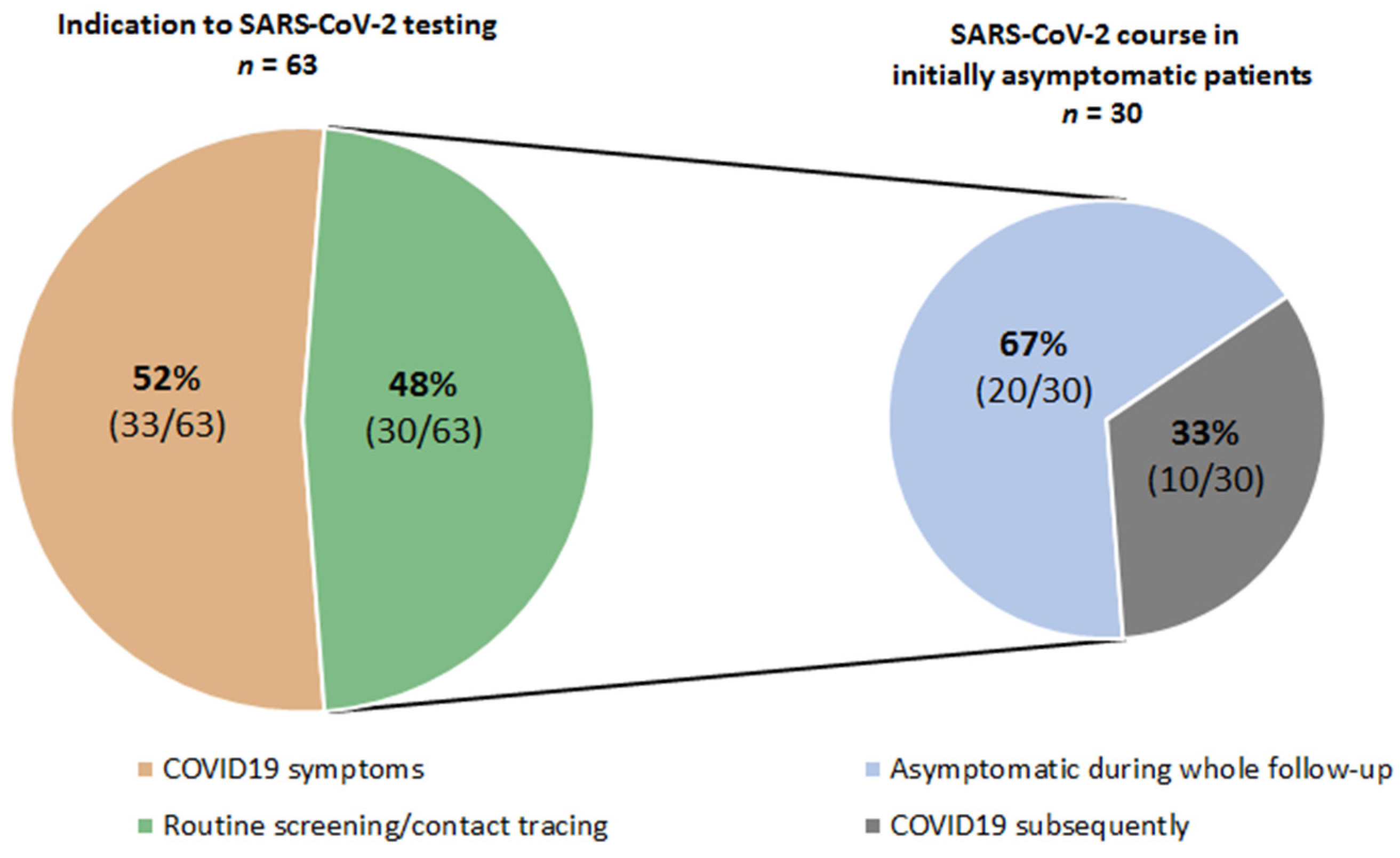
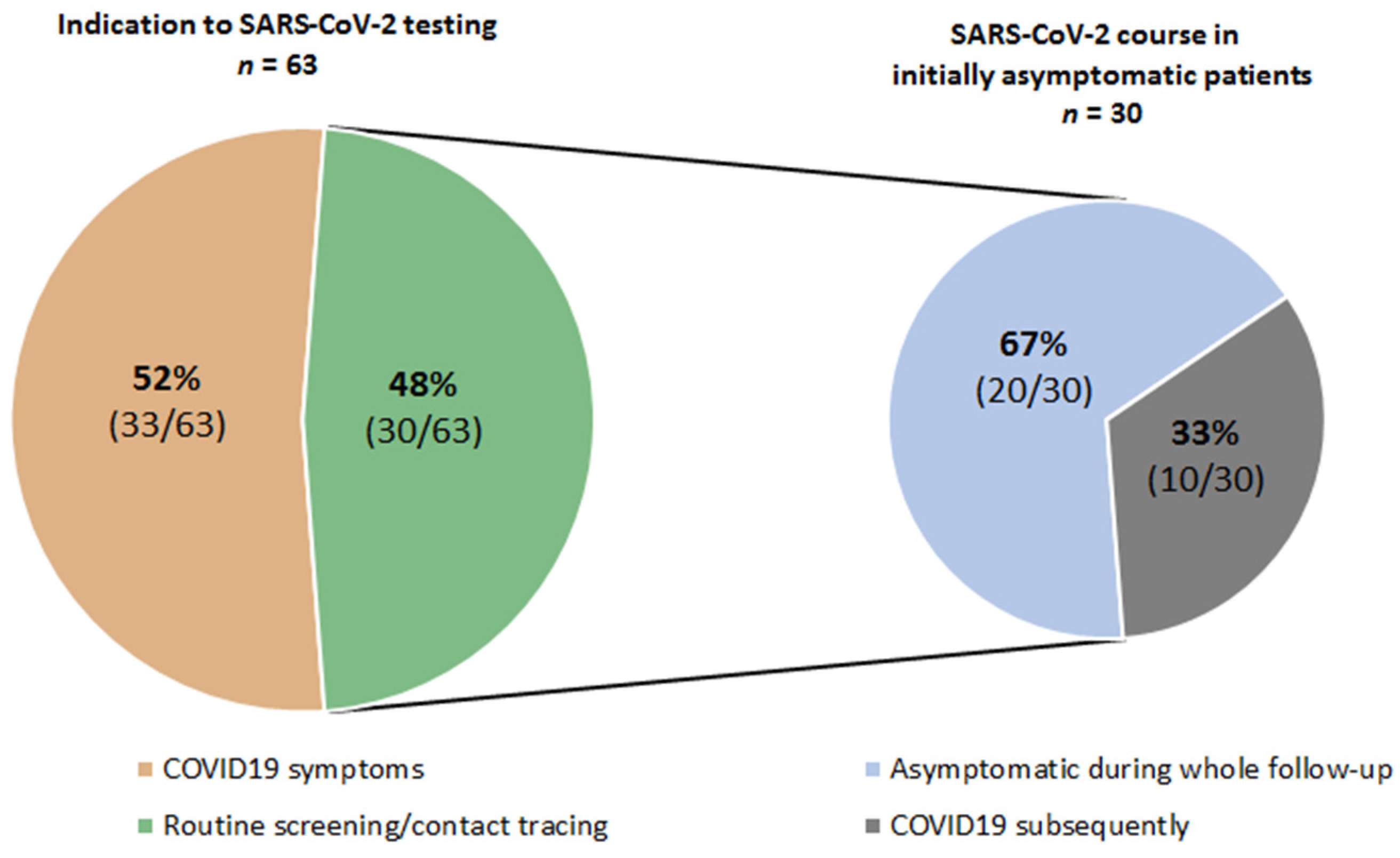
| Indication for SARS-CoV-2 testing, n (%) | ||
| Patients with COVID-19 symptoms | 33 | 52% |
| Routine or contact tracing screening of asymptomatic patients | 30 | 48% |
| - subsequent onset of COVID-19 symptoms | 10/33 | 33% |
| - asymptomatic SARS-CoV-2 during entire follow-up | 20/33 | 67% |
| - median time from positive SARS-CoV-2 test to onset of COVID-19 symptoms days (range) | 13 | (6–24) |
| COVID-19 symptoms (multiple answers possible), n (%) | 43/63 | 68% |
| Fever | 29/43 | 67% |
| Cough | 25/43 | 58% |
| Dyspnea | 24/43 | 56% |
| Gastrointestinal symptoms | 6/43 | 14% |
| Chest pain | 6/43 | 14% |
| Laboratory results at SARS-CoV-2 detection | ||
| WBCs × 109/L, median (range) * | 4.6 | (0.2–12.5) |
| CRP mg/dl, median (range) ** | 18.9 | (1.0–207) |
| PCT ng/mL, median (range) *** | 0.19 | (0.03–2.2) |
| LDH U/L, median (range) **** | 259 | (86–1301) |
| Lymphocytopenia (<1.0 × 109/L) (data available for 37 patients) | 17/37 | 46% |
| Chest imaging for diagnosing COVID-19, n (%) (data available for 39 patients) | ||
| X-ray | 24/39 | 61% |
| CT | 24/39 | 61% |
| Ultrasound | 3/39 | 8% |
| Imaging results, n (%) | ||
| Signs of pneumonia | 23/39 | 59% |
| No indication of pneumonia | 16/39 | 41% |
| SARS-CoV-2 seroconversion †, n (%) (data available for 16 patients) | ||
| - seroconversion achieved | 10/16 | 63% |
| - median time from SARS-CoV-2 diagnosis by RT-PCR to seroconversion or last negative antibody test, days, range | 13 | (3 ††–133) |
| Confirmed secondary bacterial infections in COVID-19 cases, n (%) | 6/43 | 14% |
| Detected microorganisms (multiple answers possible), n (%) | ||
| Gram-negative bacteria | 5/6 | 83% |
| - Klebsiella pneumonia | 4 | 67% |
| - Klebsiella oxytoca | 1 | 17% |
| - Escherichia coli | 2 | 34% |
| - Pseudomonas aeriginosa | 1 | 17% |
| Gram-positive bacteria | 1/6 | 17% |
| - Staphylococcus aureus | 1 | 17% |
| Positive specimen/compartment (multiple answers possible), n (%) | ||
| - trachealbronchial fluid | 4/6 | 67% |
| - blood culture | 3/6 | 50% |
| - urine (including catheter urine) | 2/6 | 33% |
| Parameter | All Patients, n = 63 | |
|---|---|---|
| Severity of SARS-CoV-2 infection, n (%) | ||
| Asymptomatic SARS-CoV-2 course | 20 | 32% |
| COVID-19 | 43 | 68% |
| - mild course | 18 | 29% |
| - severe course | 12 | 19% |
| - critical course | 13 | 20% |
| Patient care, n (%) | ||
| Outpatients | 23 | 37% |
| Inpatients | 40 | 63% |
| - admitted because of COVID-19 symptoms | 26 | 41% |
| - routine admission prior to positive SARS-CoV-2 test, of them: | 12 | 19% |
| a. subsequent COVID-19 | 8 | 13% |
| b. asymptomatic SARS-CoV-2 | 4 | 6% |
| - admission of asymptomatic SARS-CoV-2 cases for observation | 2 | 3% |
| Requiring wards during hospitalization, n (%) | ||
| General ward | 28 | 44% |
| IMC/ICU | 12 | 19% |
| Non- and invasive respiratory support on IMC/ICU, n (%) | 9/12 | 75% |
| Non-invasive respiratory support | 5/12 | 42% |
| - high-flow oxygen | 2/12 | 17% |
| - non-invasive ventilation | 3/12 | 25% |
| Invasive (mechanical) ventilation | 4/12 | 33% |
| Median length of hospital stay of patients admitted because of COVID-19, days, range | 14 | 1–43 |
| Treatment modalities related to SARS-CoV-2 infection, n (%) | ||
| No therapy | 19 | 30% |
| Symptomatic therapy only | 18 | 29% |
| Specific COVID-19 therapy | 11 | 17% |
| - remdesevir | 9 | 14% |
| - convalescent plasma | 7 | 11% |
| - dexamethasone | 2 | 3% |
| - anti-IL-6 receptor/anti-IL-6 antibody | 2 | 3% |
| - serine protease inhibitor | 1 | 2% |
| Antibiotic therapy | 19 | 30% |
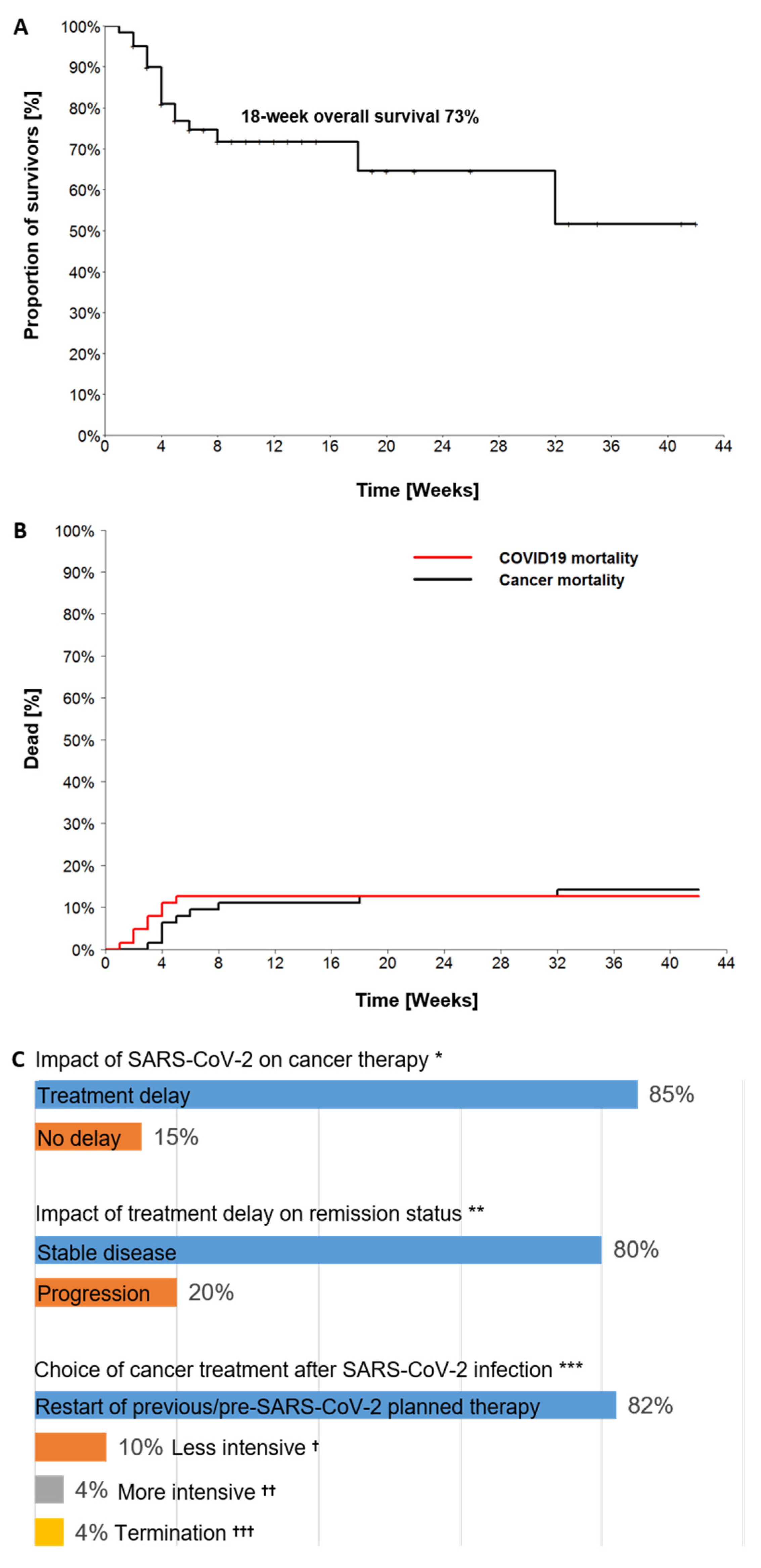
| Treatment delay due to SARS-CoV-2 among 54/63 patients with ongoing or planned cancer therapy before, n (%) | 46/54 | 85% |
| Median time of treatment delay, days, range | 25 | 4–66 |
| Median time from SARS-CoV-2 detection to last follow-up, weeks, range | 6 | 0–42 |
| Remission status at last follow-up, n (%) | ||
| Complete remission | 13 | 20% |
| Partial remission | 10 | 16% |
| Stable disease | 20 | 32% |
| Relapse/progressive disease | 20 | 32% |
| Survival status at last follow-up, n (%) | ||
| Alive | 46 | 73% |
| Dead | 17 | 27% |
| Causes of death (n = 17) | ||
| COVID-19 | 8 | 47% |
| Relapsed/refractory malignancy | 9 | 53% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shumilov, E.; Hoffknecht, P.; Koch, R.; Peceny, R.; Voigt, S.; Schmidt, N.; Peeck, M.; Bacher, U.; Scheithauer, S.; Trümper, L.; et al. Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers. Cancers 2021, 13, 2917. https://doi.org/10.3390/cancers13122917
Shumilov E, Hoffknecht P, Koch R, Peceny R, Voigt S, Schmidt N, Peeck M, Bacher U, Scheithauer S, Trümper L, et al. Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers. Cancers. 2021; 13(12):2917. https://doi.org/10.3390/cancers13122917
Chicago/Turabian StyleShumilov, Evgenii, Petra Hoffknecht, Raphael Koch, Rudolf Peceny, Steffen Voigt, Nicole Schmidt, Micha Peeck, Ulrike Bacher, Simone Scheithauer, Lorenz Trümper, and et al. 2021. "Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers" Cancers 13, no. 12: 2917. https://doi.org/10.3390/cancers13122917
APA StyleShumilov, E., Hoffknecht, P., Koch, R., Peceny, R., Voigt, S., Schmidt, N., Peeck, M., Bacher, U., Scheithauer, S., Trümper, L., Lenz, G., Kerkhoff, A., & Bleckmann, A. (2021). Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers. Cancers, 13(12), 2917. https://doi.org/10.3390/cancers13122917