
Undifferentiated Embryonal Sarcoma of the Liver in Children Versus Adults: A National Cancer Database Analysis †

 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
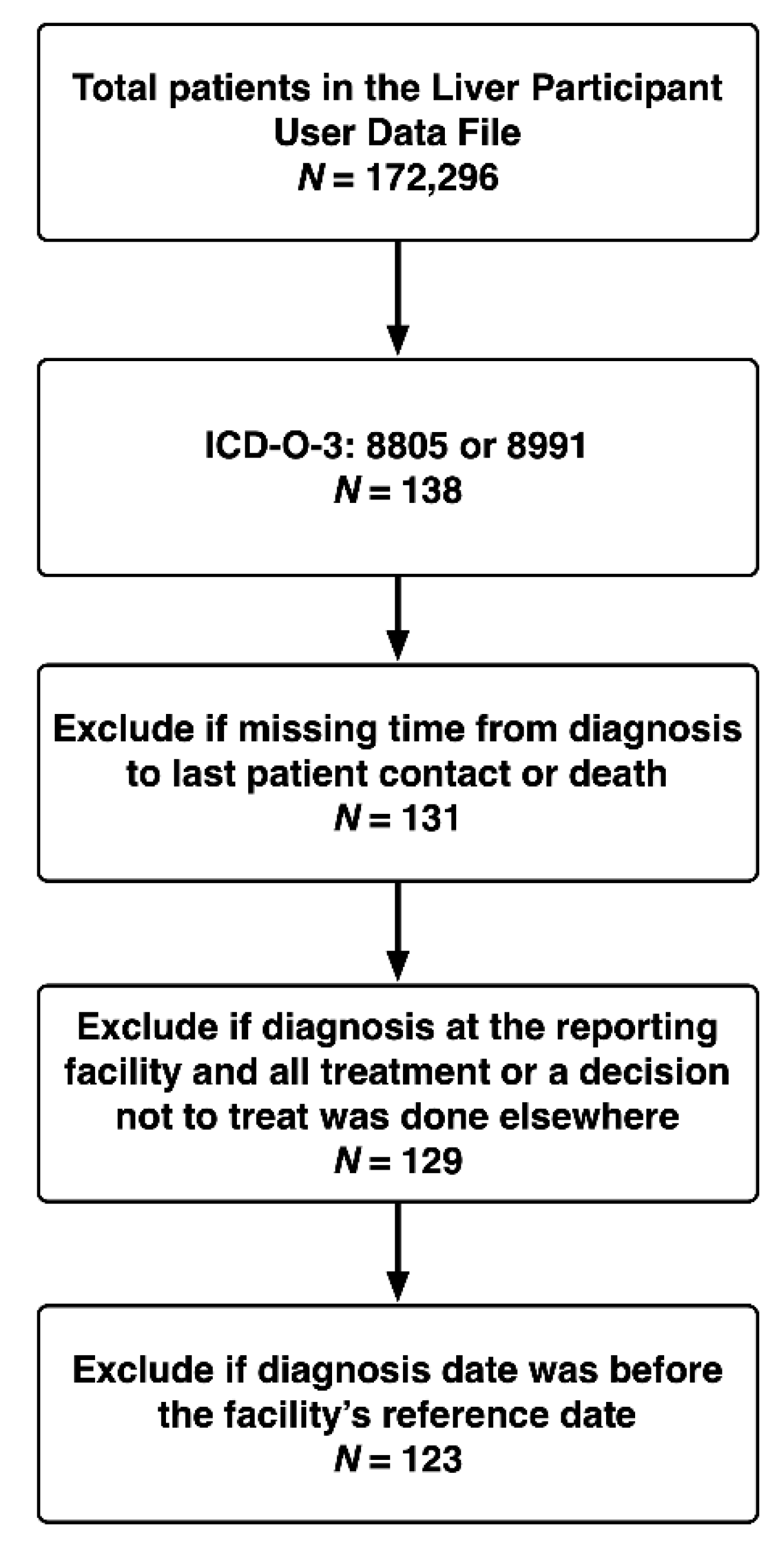
2.1. Data Source and Patient Population
2.2. Covariates and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics and Treatment Modalities
3.2. Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stocker, J.T.; Ishak, K.G. Undifferentiated (embryonal) sarcoma of the liver: Report of 31 cases. Cancer 1978, 42, 336–348. [Google Scholar] [CrossRef]
- Shi, Y.; Rojas, Y.; Zhang, W.; Beierle, E.A.; Doski, J.J.; Goldfarb, M.; Goldin, A.B.; Gow, K.W.; Langer, M.; Meyers, R.L.; et al. Characteristics and outcomes in children with undifferentiated embryonal sarcoma of the liver: A report from the National Cancer Database. Pediatr. Blood Cancer 2017, 64, 1–8. [Google Scholar] [CrossRef]
- Pinamonti, M.; Vittone, F.; Ghiglione, F.; Borasi, A.; Silvestri, S.; Coverlizza, S. Unexpected Liver Embryonal Sarcoma in the Adult: Diagnosis and Treatment. Case Rep. Surg. 2018, 2018, 8362012. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.G.; Tang, L.F.; Chen, Z.M.; Tang, H.F.; Li, M.J. Childhood undifferentiated embryonal liver sarcoma: Clinical features and immunohistochemistry analysis. J. Pediatr. Surg. 2008, 43, 1912–1919. [Google Scholar] [CrossRef]
- Massani, M.; Caratozzolo, E.; Baldessin, M.; Bonariol, L.; Bassi, N. Hepatic cystic lesion in adult: A challenging diagnosis of undifferentiated primary embryonal sarcoma. Il Giornale di Chirurgia 2010, 31, 225–228. [Google Scholar]
- Wu, Z.; Wei, Y.; Cai, Z.; Zhou, Y. Long-term survival outcomes of undifferentiated embryonal sarcoma of the liver: A pooled analysis of 308 patients. ANZ J. Surg. 2020, 90, 1615–1620. [Google Scholar] [CrossRef]
- Buetow, P.C.; Buck, J.L.; Pantongrag-Brown, L.; Marshall, W.H.; Ros, P.R.; Levine, M.S.; Goodman, Z.D. Undifferentiated (embryonal) sarcoma of the liver: Pathologic basis of imaging findings in 28 cases. Radiology 1997, 203, 779–783. [Google Scholar] [CrossRef]
- Joshi, S.W.; Merchant, N.H.; Jambhekar, N.A. Primary multilocular cystic undifferentiated (embryonal) sarcoma of the liver in childhood resembling hydatid cyst of the liver. Br. J. Radiol. 1997, 70, 314–316. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.M.; Lattin, G.E.J.; Cube, R.; Lewis, R.B.; Marichal-Hernández, C.; Shawhan, R.; Conran, R.M. From the archives of the AFIP: Pediatric liver masses: Radiologic-pathologic correlation. Part 2. Malignant tumors. Radiographics 2011, 31, 483–507. [Google Scholar] [CrossRef]
- Bisogno, G.; Pilz, T.; Perilongo, G.; Ferrari, A.; Harms, D.; Ninfo, V.; Treuner, J.; Carli, M. Undifferentiated sarcoma of the liver in childhood: A curable disease. Cancer 2002, 94, 252–257. [Google Scholar] [CrossRef]
- Kim, D.-Y.; Kim, K.-H.; Jung, S.-E.; Lee, S.-C.; Park, K.-W.; Kim, W.-K. Undifferentiated (embryonal) sarcoma of the liver: Combination treatment by surgery and chemotherapy. J. Pediatr. Surg. 2002, 37, 1419–1423. [Google Scholar] [CrossRef]
- Plant, A.S.; Busuttil, R.W.; Rana, A.; Nelson, S.D.; Auerbach, M.; Federman, N.C. A single-institution retrospective cases series of childhood undifferentiated embryonal liver sarcoma (UELS): Success of combined therapy and the use of orthotopic liver transplant. J. Pediatr. Hematol. Oncol. 2013, 35, 451–455. [Google Scholar] [CrossRef]
- Ismail, H.; Dembowska–Bagińska, B.; Broniszczak, D.; Kaliciński, P.; Maruszewski, P.; Kluge, P.; Święszkowska, E.; Kościesza, A.; Lembas, A.; Perek, D. Treatment of undifferentiated embryonal sarcoma of the liver in children—single center experience. J. Pediatr. Surg. 2013, 48, 2202–2206. [Google Scholar] [CrossRef]
- Merli, L.; Mussini, C.; Gabor, F.; Branchereau, S.; Martelli, H.; Pariente, D.; Guérin, F. Pitfalls in the surgical management of undifferentiated sarcoma of the liver and benefits of preoperative chemotherapy. Eur. J. Pediatr. Surg. 2015, 25, 132–137. [Google Scholar] [CrossRef]
- Cao, Q.; Ye, Z.; Chen, S.; Liu, N.; Li, S.; Liu, F. Undifferentiated embryonal sarcoma of liver: A multi-institutional experience with 9 cases. Int. J. Clin. Exp. Pathol. 2014, 7, 8647. [Google Scholar] [PubMed]
- Lenze, F.; Birkfellner, T.; Lenz, P.; Hussein, K.; Länger, F.; Kreipe, H.; Domschke, W. Undifferentiated embryonal sarcoma of the liver in adults. Cancer 2008, 112, 2274–2282. [Google Scholar] [CrossRef] [PubMed]
- Boffa, D.J.; Rosen, J.E.; Mallin, K.; Loomis, A.; Gay, G.; Palis, B.; Thoburn, K.; Gress, D.; McKellar, D.P.; Shulman, L.N.; et al. Using the National Cancer Database for Outcomes Research: A Review. JAMA Oncol. 2017, 3, 1722–1728. [Google Scholar] [CrossRef]
- National Cancer Data Base Participant User File (PUF) Data Dictionary. Available online: https://www.facs.org/-/media/files/quality-programs/cancer/ncdb/puf_data_dictionary.ashx (accessed on 1 February 2020).
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection–a review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef]
- Pachera, S.; Nishio, H.; Takahashi, Y.; Yokoyama, Y.; Oda, K.; Ebata, T.; Igami, T.; Nagino, M. Undifferentiated embryonal sarcoma of the liver: Case report and literature survey. J. Hepatobiliary Pancreat. Surg. 2008, 15, 536–544. [Google Scholar] [CrossRef]
- Webber, E.M.; Morrison, K.B.; Pritchard, S.L.; Sorensen, P.H.B. Undifferentiated embryonal sarcoma of the liver: Results of clinical management in one center. J. Pediatr. Surg. 1999, 34, 1641–1644. [Google Scholar] [CrossRef]
- Lack, E.E.; Schloo, B.L.; Azumi, N.; Travis, W.D.; Grier, H.E.; Kozakewich, H.P. Undifferentiated (embryonal) sarcoma of the liver. Clinical and pathologic study of 16 cases with emphasis on immunohistochemical features. Am. J. Surg. Pathol. 1991, 15, 1–16. [Google Scholar] [CrossRef]
- Walker, N.I.; Horn, M.J.; Strong, R.W.; Lynch, S.V.; Cohen, J.; Ong, T.H.; Harris, O.D. Undifferentiated (embryonal) sarcoma of the liver: Pathologic findings and long-term survival after complete surgical resection. Cancer 1992, 69, 52–59. [Google Scholar] [CrossRef]
- Chen, L.E.; Shepherd, R.W.; Nadler, M.L.; Chapman, W.C.; Kotru, A.; Lowell, J.A. Liver transplantation and chemotherapy in children with unresectable primary hepatic malignancies: Development of a management algorithm. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 487–493. [Google Scholar] [CrossRef]
- Upadhyaya, M.; McKiernan, P.; Hobin, D.; Kelly, D.A.; Brown, R.; Lloyd, C.; Buckels, J.; Millar, A.J.W.; Degoyet, J.D.; Mirza, D.F. Primary hepatic sarcomas in children—a single-center experience over 19 years. J. Pediatr. Surg. 2010, 45, 2124–2128. [Google Scholar] [CrossRef] [PubMed]
- Walther, A.; Geller, J.; Coots, A.; Towbin, A.; Nathan, J.; Alonso, M.; Sheridan, R.; Tiao, G. Multimodal therapy including liver transplantation for hepatic undifferentiated embryonal sarcoma. Liver Transpl. 2014, 20, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Techavichit, P.; Masand, P.M.; Himes, R.W.; Abbas, R.; Goss, J.A.; Vasudevan, S.A.; Finegold, M.J.; Heczey, A. Undifferentiated embryonal sarcoma of the liver (UESL): A single-center experience and review of the literature. J. Pediatr. Hematol. Oncol. 2016, 38, 261–268. [Google Scholar] [CrossRef]
- Murawski, M.; Scheer, M.; Leuschner, I.; Stefanowicz, J.; Bonar, J.; Dembowska-Bagińska, B.; Kaliciński, P.; Koscielniak, E.; Czauderna, P.; Fuchs, J. Undifferentiated sarcoma of the liver: Multicenter international experience of the Cooperative Soft-Tissue Sarcoma Group and Polish Paediatric Solid Tumor Group. Pediatr. Blood Cancer 2020, 67, e28598. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.-H.; Huang, J.; Ge, N.-J.; Yang, Y.-F.; Zhao, J.-Y. Recurrent undifferentiated embryonal sarcoma of the liver in adult patient treated by pembrolizumab: A case report. World J. Clin. Cases 2021, 9, 2281–2288. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Morales, E.G.; Clemente-Gutiérrez, E.U.; Alvarez-Bautista, E.F.; Santes-Jasso, O.; Carpinteyro-Espin, P.; Mercado Miguel, A. Undifferentiated embryonal sarcoma of the liver in adult patient: A report of two cases. Ann. Hepatobiliary Pancreat. Surg. 2018, 22, 269–273. [Google Scholar] [CrossRef]
- Almogy, G.; Lieberman, S.; Gips, M.; Pappo, O.; Edden, Y.; Jurim, O.; Simon Slasky, B.; Uzieli, B.; Eid, A. Clinical outcomes of surgical resections for primary liver sarcoma in adults: Results from a single centre. Eur. J. Surg. Oncol. 2004, 30, 421–427. [Google Scholar] [CrossRef]
- Dhanasekaran, R.; Hemming, A.; Salazar, E.; Cabrera, R. Rare case of adult undifferentiated (embryonal) sarcoma of the liver treated with liver transplantation: Excellent long-term survival. Case Rep. Hepatol. 2012, 2012, 519741. [Google Scholar] [CrossRef]
- Leuschner, I.; Schmidt, D.; Harms, D. Undifferentiated sarcoma of the liver in childhood: Morphology, flow cytometry, and literature review. Hum. Pathol. 1990, 21, 68–76. [Google Scholar] [CrossRef]
- Kiani, B.; Ferrell, L.D.; Qualman, S.; Frankel, W.L. Immunohistochemical analysis of embryonal sarcoma of the liver. Appl Immunohistochem. Mol. Morphol. 2006, 14, 193–197. [Google Scholar] [CrossRef]
- Lee, K.H.; Maratovich, M.N.; Lee, K.-B. Undifferentiated embryonal sarcoma of the liver in an adult patient. Clin. Mol. Hepatol. 2016, 22, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-W.; Gong, S.-J.; Song, W.-H.; Zhu, J.-J.; Pan, C.-H.; Wu, M.-C.; Xu, A.-M. Undifferentiated liver embryonal sarcoma in adults: A report of four cases and literature review. World J. Gastroenterol. 2010, 16, 4725–4732. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.J.; Martin, L.; Alonso, M.; Altura, R.A. Liver transplant for relapsed undifferentiated embryonal sarcoma in a young child. J. Pediatr. Surg. 2009, 44, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Babu, B.I.; Bigam, D.L.; Gilmour, S.M.; Dajani, K.Z.; Shapiro, A.M.J.; Kneteman, N.M. Liver Transplantation in Locally Unresectable, Undifferentiated Embryonal Cell Sarcoma. Transpl. Direct 2021, 7, e654. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 123) | Children (n = 82) | Adults (n = 41) | p Value |
|---|---|---|---|---|
| Age (years) | 11.0 (6.0–23.0) | 7.5 (5.0–11.0) | 36.0 (23.0–62.0) | <0.001 |
| Sex | 0.01 | |||
| Female | 71 (57.7%) | 41 (50.0%) | 30 (73.2%) | |
| Male | 52 (42.3%) | 41 (50.0%) | 11 (26.8%) | |
| Race | 0.22 | |||
| African American | 24 (19.5%) | 13 (15.9%) | 11 (26.8%) | |
| Caucasian | 86 (69.9%) | 60 (73.2%) | 26 (63.4%) | |
| Other | 9 (7.3%) | 5 (6.1%) | 4 (9.8%) | |
| Unknown | 4 (3.3%) | 4 (4.9%) | 0 (0.0%) | |
| Insurance status | 0.97 | |||
| Not insured | 3 (2.4%) | 2 (2.4%) | 1 (2.4%) | |
| Private | 63 (51.2%) | 41 (50.0%) | 22 (53.7%) | |
| Public | 53 (43.1%) | 36 (43.9%) | 17 (41.5%) | |
| Unknown | 4 (3.3%) | 3 (3.7%) | 1 (2.4%) | |
| Tumor size (cm) (n = 108) | 14.0 (10.0–16.0) | 14.0 (11.0–15.9) | 14.8 (7.6–19.5) | 0.90 |
| Regional lymph node status | 0.44 | |||
| Negative | 30 (24.4%) | 18 (22.0%) | 12 (29.3%) | |
| Positive | 4 (3.3%) | 3 (3.7%) | 1 (2.4%) | |
| No nodes were examined | 86 (69.9%) | 60 (73.2%) | 26 (63.4%) | |
| Unknown | 3 (2.4%) | 1 (1.2%) | 2 (4.9%) | |
| Metastasis at diagnosis | 0.33 | |||
| No | 101 (82.1%) | 65 (79.3%) | 36 (87.8%) | |
| Yes | 17 (13.8%) | 14 (17.1%) | 3 (7.3%) | |
| Unknown | 5 (4.1%) | 3 (3.7%) | 2 (4.9%) | |
| Chemotherapy | <0.001 | |||
| No | 18 (14.6%) | 4 (4.9%) | 14 (34.2%) | |
| Yes | 103 (83.7%) | 76 (92.7%) | 27 (65.9%) | |
| Unknown | 2 (1.6%) | 2 (2.4%) | 0 (0.0%) | |
| Radiation | 0.20 | |||
| No | 101 (82.1%) | 64 (78.1%) | 37 (90.2%) | |
| Yes | 21 (17.1%) | 17 (20.7%) | 4 (9.8%) | |
| Unknown | 1 (0.8%) | 1 (1.2%) | 0 (0.0%) | |
| Surgical treatment | 0.31 | |||
| No | 21 (17.1%) | 12 (14.6%) | 9 (22.0%) | |
| Yes | 102 (82.9%) | 70 (85.4%) | 32 (78.0%) | |
| Type of surgical treatment (n = 102) | 0.29 | |||
| Wedge/segmental resection | 30 (29.4%) | 22 (31.4%) | 8 (25.0%) | |
| Lobectomy | 43 (42.2%) | 28 (40.0%) | 15 (46.9%) | |
| Extended lobectomy | 14 (13.7%) | 7 (10.0%) | 7 (21.9%) | |
| Resection, not otherwise specified | 11 (10.8%) | 9 (12.9%) | 2 (6.3%) | |
| Liver transplantation | 4 (3.9%) | 4 (5.7%) | 0 (0.0%) | |
| Margin status (n = 102) | 1.00 | |||
| No residual tumor | 71 (69.6%) | 48 (68.6%) | 23 (71.9%) | |
| Residual tumor | 17 (16.7%) | 12 (17.1%) | 5 (15.6%) | |
| Not evaluable/unknown | 14 (13.7%) | 10 (14.3%) | 4 (12.5%) | |
| Chemotherapy/surgery sequence (n = 102) | <0.001 | |||
| None | 13 (12.8%) | 4 (5.7%) | 9 (28.1%) | |
| Neoadjuvant | 15 (14.7%) | 14 (20.0%) | 1 (3.1%) | |
| Adjuvant | 59 (57.8%) | 37 (52.9%) | 22 (68.8%) | |
| Neoadjuvant and adjuvant | 13 (12.8%) | 13 (18.6%) | 0 (0.0%) | |
| Unknown | 2 (2.0%) | 2 (2.9%) | 0 (0.0%) | |
| Follow-up time after diagnosis (months) | 48.1 (20.2–92.6) | 61.2 (22.9–102.9) | 29.6 (12.0–71.4) | 0.007 |
| Characteristics | n | Univariable | n | Multivariable (n = 115) | ||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |||
| Age group | ||||||
| Children | 82 | Reference | - | 76 | Reference | - |
| Adults | 41 | 4.36 (2.08–9.11) | <0.001 | 39 | 5.35 (2.24–12.77) | <0.001 |
| Surgical treatment | ||||||
| No | 21 | Reference | - | 18 | Reference | - |
| Yes | 102 | 0.16 (0.08–0.34) | <0.001 | 97 | 0.21 (0.09–0.52) | 0.001 |
| Chemotherapy | ||||||
| No | 18 | Reference | - | 16 | Reference | - |
| Yes | 103 | 0.36 (0.16–0.81) | 0.01 | 99 | 0.59 (0.22–1.60) | 0.30 |
| Radiation | ||||||
| No | 101 | Reference | - | 94 | Reference | - |
| Yes | 21 | 0.72 (0.25–2.07) | 0.55 | 21 | 1.18 (0.39–3.56) | 0.77 |
| Metastasis at diagnosis | ||||||
| No | 101 | Reference | - | 98 | Reference | - |
| Yes | 17 | 2.82 (1.19–6.66) | 0.02 | 17 | 3.34 (1.20–9.29) | 0.02 |
| Characteristics | n | Univariable | n | Multivariable (n = 79) | ||
|---|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |||
| Age group | ||||||
| Children | 70 | Reference | - | 53 | Reference | - |
| Adults | 32 | 4.95 (1.85–13.23) | 0.001 | 26 | 10.68 (2.10–54.33) | 0.004 |
| Surgical margins | ||||||
| No residual tumor | 72 | Reference | - | 64 | Reference | - |
| Residual tumor | 17 | 2.08 (0.71–6.08) | 0.18 | 15 | 5.41 (1.18–24.75) | 0.03 |
| Tumor size (cm) | 92 | 1.02 (0.99–1.04) | 0.09 | 79 | 1.00 (0.97–1.04) | 0.89 |
| Chemotherapy | ||||||
| Neoadjuvant and adjuvant | 13 | Reference | - | 12 | Reference | - |
| None | 13 | 1.13 (0.23–5.62) | 0.88 | 9 | 0.43 (0.04–5.26) | 0.51 |
| Neoadjuvant | 15 | 0.55 (0.09–3.28) | 0.51 | 9 | 1.24 (0.11–14.50) | 0.86 |
| Adjuvant | 59 | 0.73 (0.20–2.65) | 0.63 | 49 | 0.25 (0.03–1.84) | 0.18 |
| Radiation | ||||||
| No | 82 | Reference | - | 63 | Reference | - |
| Yes | 19 | 0.92 (0.27–3.18) | 0.90 | 16 | 0.51 (0.07–3.52) | 0.49 |
| Metastasis at diagnosis | ||||||
| No | 90 | Reference | - | 72 | Reference | - |
| Yes | 10 | 1.45 (0.33–6.31) | 0.62 | 7 | 4.29 (0.59–30.89) | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziogas, I.A.; Zamora, I.J.; Lovvorn III, H.N.; Bailey, C.E.; Alexopoulos, S.P. Undifferentiated Embryonal Sarcoma of the Liver in Children Versus Adults: A National Cancer Database Analysis. Cancers 2021, 13, 2918. https://doi.org/10.3390/cancers13122918
Ziogas IA, Zamora IJ, Lovvorn III HN, Bailey CE, Alexopoulos SP. Undifferentiated Embryonal Sarcoma of the Liver in Children Versus Adults: A National Cancer Database Analysis. Cancers. 2021; 13(12):2918. https://doi.org/10.3390/cancers13122918
Chicago/Turabian StyleZiogas, Ioannis A., Irving J. Zamora, Harold N. Lovvorn III, Christina E. Bailey, and Sophoclis P. Alexopoulos. 2021. "Undifferentiated Embryonal Sarcoma of the Liver in Children Versus Adults: A National Cancer Database Analysis" Cancers 13, no. 12: 2918. https://doi.org/10.3390/cancers13122918
APA StyleZiogas, I. A., Zamora, I. J., Lovvorn III, H. N., Bailey, C. E., & Alexopoulos, S. P. (2021). Undifferentiated Embryonal Sarcoma of the Liver in Children Versus Adults: A National Cancer Database Analysis. Cancers, 13(12), 2918. https://doi.org/10.3390/cancers13122918