
Anti-Angiogenic Treatment in Pseudomyxoma Peritonei—Still a Strong Preclinical Rationale

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
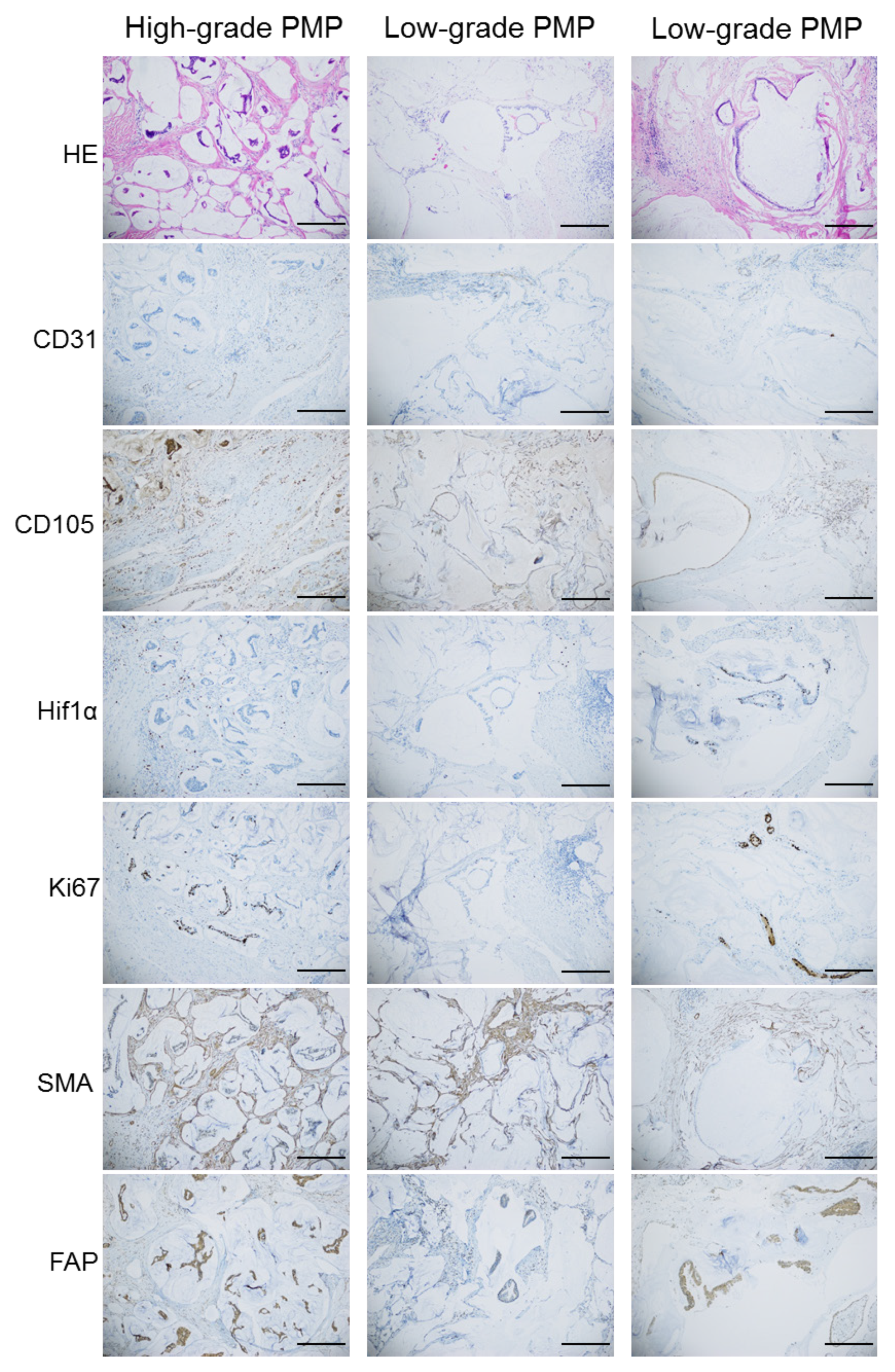
2.1. Immunohistochemistry
2.2. Measurement of Pro-Angiogenic Factors
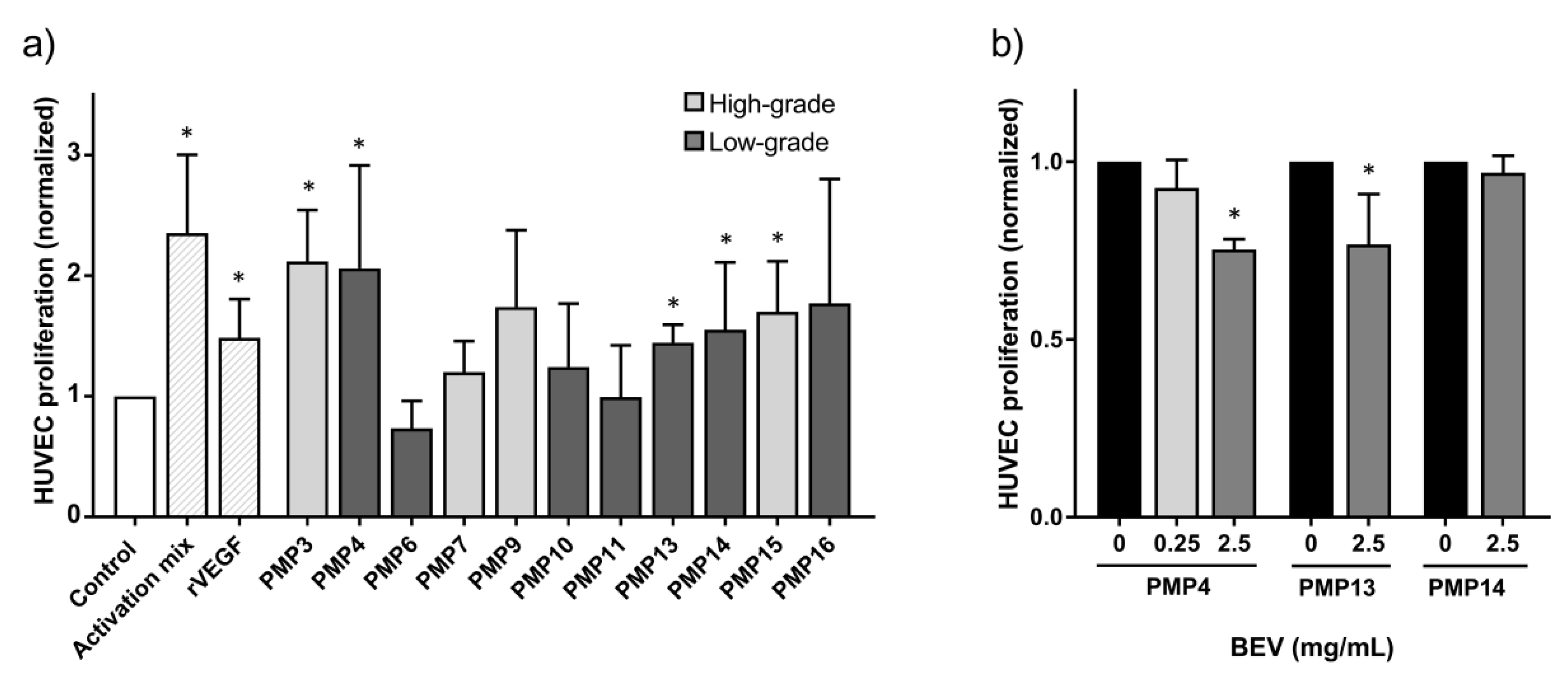
2.3. Incubation with PMP Tumor Samples Increased HUVEC Proliferation Which Could Be Inhibited by Anti-Angiogenic Drugs
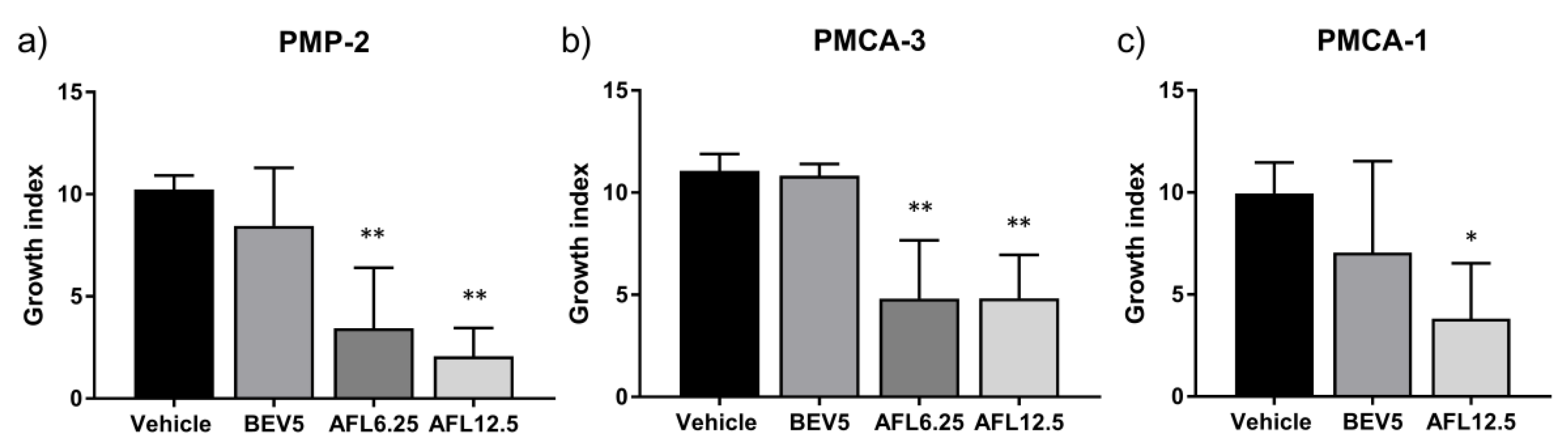
2.4. In Vivo Activity of Anti-Angiogenic Drugs
3. Discussion
4. Materials and Methods
4.1. Patient Samples
4.2. PDX Models
4.3. Storage and Handling of Fresh Patient and Xenograft Samples
4.4. Immunohistochemical Analysis and Quantification of Microvessel Density
4.5. Measurement of Pro-angiogenic Factors in Tumor Samples from Patients and PDX Models
4.6. HUVEC Culture Conditions
4.7. HUVEC Proliferation and Angiogenic Inhibition Assay
4.8. In Vivo Experiments
4.9. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patrick-Brown, T.D.J.H.; Carr, N.J.; Swanson, D.M.; Larsen, S.; Mohamed, F.; Flatmark, K. Estimating the Prevalence of Pseudomyxoma Peritonei in Europe Using a Novel Statistical Method. Ann. Surg. Oncol. 2021, 28, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Chua, T.C.; Moran, B.J.; Sugarbaker, P.H.; Levine, E.A.; Glehen, O.; Gilly, F.N.; Baratti, D.; Deraco, M.; Elias, D.; Sardi, A.; et al. Early- and Long-Term Outcome Data of Patients With Pseudomyxoma Peritonei From Appendiceal Origin Treated by a Strategy of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. J. Clin. Oncol. 2012, 30, 2449–2456. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, O.; Flatmark, K.; Reed, W.; Wiig, J.; Dueland, S.; Giercksky, K.-E.; Larsen, S. Evaluation of complete cytoreductive surgery and two intraperitoneal chemotherapy techniques in pseudomyxoma peritonei. Eur. J. Surg. Oncol. (EJSO) 2012, 38, 969–976. [Google Scholar] [CrossRef]
- Dohan, A.; Lousquy, R.; Eveno, C.; Goere, D.; Broqueres-You, D.; Kaci, R.; Lehmann-Che, J.; Launay, J.-M.; Soyer, P.; Bonnin, P.; et al. Orthotopic Animal Model of Pseudomyxoma Peritonei. Am. J. Pathol. 2014, 184, 1920–1929. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.-L.; Hutarew, G.; Gradl, J.; Gratzl, M.; Denz, H.; Fiegl, M. Successful antiangiogenic combination therapy for pseudomyxoma peritonei with bevacizumab and capecitabine. Cancer Biol. Ther. 2009, 8, 1459–1462. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pietrantonio, F.; Berenato, R.; Maggi, C.; Caporale, M.; Milione, M.; Perrone, F.; Tamborini, E.; Baratti, D.; Kusamura, S.; Mariani, L.; et al. GNAS mutations as prognostic biomarker in patients with relapsed peritoneal pseudomyxoma receiving metronomic capecitabine and bevacizumab: A clinical and translational study. J. Transl. Med. 2016, 14, 125. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Choe, J.H.; Overman, M.J.; Fournier, K.F.; Royal, R.E.; Ohinata, A.; Rafeeq, S.; Beaty, K.; Phillips, J.K.; Wolff, R.A.; Mansfield, P.F.; et al. Improved Survival with Anti-VEGF Therapy in the Treatment of Unresectable Appendiceal Epithelial Neoplasms. Ann. Surg. Oncol. 2015, 22, 2578–2584. [Google Scholar] [CrossRef]
- Akin, S.; Dizdar, Ö; Hayran, M. Anti-VEGF Therapy in the Treatment of Unresectable Appendiceal Epithelial Neoplasms. Ann. Surg. Oncol. 2017, 24, 620. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Flatmark, K.; Reed, W.; Halvorsen, T.; Sørensen, O.; Wiig, J.N.; Larsen, S.G.; Fodstad, Ø.; Giercksky, K.-E. Pseudomyxoma peritonei—Two novel orthotopic mouse models portray the PMCA-I histopathologic subtype. BMC Cancer 2007, 7, 116. [Google Scholar] [CrossRef]
- Gheonea, D.I.; Cartana, E.-T.; Cherciu, I.F.; Streaţa, I.; Uscatu, C.-D.; Nicoli, E.-R.; Ioana, M.; Pirici, D.; Georgescu, C.-V.; Alexandru, D.-O.; et al. Assessing tumor angiogenesis in colorectal cancer by quantitative contrast-enhanced endoscopic ultrasound and molecular and immunohistochemical analysis. Endosc. Ultrasound 2018, 7, 175–183. [Google Scholar] [CrossRef]
- Duff, S.E.; Li, C.; Garland, J.M.; Kumar, S. CD105 is important for angiogenesis: Evidence and potential applications. FASEB J. 2003, 17, 984–992. [Google Scholar] [CrossRef]
- Mohamed, S.Y.; Mohammed, H.L.; Ibrahim, H.M.; Mohamed, E.M.; Salah, M. Role of VEGF, CD105, and CD31 in the Prognosis of Colorectal Cancer Cases. J. Gastrointest. Cancer 2017, 50, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Laddha, A.P.; Kulkarni, Y.A. VEGF and FGF-2: Promising targets for the treatment of respiratory disorders. Respir. Med. 2019, 156, 33–46. [Google Scholar] [CrossRef]
- Zimna, A.; Kurpisz, M. Hypoxia-Inducible Factor-1 in Physiological and Pathophysiological Angiogenesis: Applications and Therapies. BioMed Res. Int. 2015, 2015, 549412. [Google Scholar] [CrossRef] [PubMed]
- Zhan, N.; Dong, W.-G.; Wang, J. The clinical significance of vascular endothelial growth factor in malignant ascites. Tumor Biol. 2015, 37, 3719–3725. [Google Scholar] [CrossRef] [PubMed]
- Fushida, S.; Oyama, K.; Kinoshita, J.; Yagi, Y.; Okamoto, K.; Tajima, H.; Ninomiya, I.; Fujimura, T.; Ohta, T. VEGF is a target molecule for peritoneal metastasis and malignant ascites in gastric cancer: Prognostic significance of VEGF in ascites and efficacy of anti-VEGF monoclonal antibody. OncoTargets Ther. 2013, 6, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Suzumori, N. Women with endometriosis have increased levels of placental growth factor in the peritoneal fluid compared with women with cystadenomas. Hum. Reprod. 2003, 18, 2595–2598. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Akl, M.R.; Nagpal, P.; Ayoub, N.; Tai, B.; Prabhu, S.A.; Capac, C.M.; Gliksman, M.; Goy, A.; Suh, K.S. Molecular and clinical significance of fibroblast growth factor 2 (FGF2/bFGF) in malignancies of solid and hematological cancers for personalized therapies. Oncotarget 2016, 7, 44735–44762. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Adjei, A.A. Targeting Angiogenesis in Cancer Therapy: Moving Beyond Vascular Endothelial Growth Factor. Oncologist 2015, 20, 660–673. [Google Scholar] [CrossRef]
- Fleten, K.G.; Lund-Andersen, C.; Waagene, S.; Abrahamsen, T.W.; Mørch, Y.; Boye, K.; Torgunrud, A.; Flatmark, K. Experimental Treatment of Mucinous Peritoneal Metastases Using Patient-Derived Xenograft Models. Transl. Oncol. 2020, 13, 100793. [Google Scholar] [CrossRef]
- Chiron, M.; Bagley, R.G.; Pollard, J.; Mankoo, P.K.; Henry, C.; Vincent, L.; Geslin, C.; Baltes, N.; Bergstrom, D.A. Differential Antitumor Activity of Aflibercept and Bevacizumab in Patient-Derived Xenograft Models of Colorectal Cancer. Mol. Cancer Ther. 2014, 13, 1636–1644. [Google Scholar] [CrossRef] [PubMed]
- Albonici, L.; Giganti, M.G.; Modesti, A.; Manzari, V.; Bei, R. Multifaceted Role of the Placental Growth Factor (PlGF) in the Antitumor Immune Response and Cancer Progression. Int. J. Mol. Sci. 2019, 20, 2970. [Google Scholar] [CrossRef] [PubMed]
- Carr, N.J.; Cecil, T.D.; Mohamed, F.; Sobin, L.H.; Sugarbaker, P.H.; González-Moreno, S.; Taflampas, P.; Chapman, S.; Moran, B.J. A Consensus for Classification and Pathologic Reporting of Pseudomyxoma Peritonei and Associated Appendiceal Neoplasia. Am. J. Surg. Pathol. 2016, 40, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Flatmark, K.; Davidson, B.; Kristian, A.; Stavnes, H.T.; Førsund, M.; Reed, W. Exploring the peritoneal surface malignancy phenotype—a pilot immunohistochemical study of human pseudomyxoma peritonei and derived animal models. Hum. Pathol. 2010, 41, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- De Jong, D.; Boot, H.; Taal, B. Histological grading with clinical relevance in gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Recent Results Cancer Res. 2000, 156, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Andersson, Y.; Haavardtun, S.I.; Davidson, B.; Dørum, A.; Fleten, K.G.; Fodstad, Ø; Flatmark, K. MOC31PE immunotoxin-targeting peritoneal metastasis from epithelial ovarian cancer. Oncotarget 2017, 8, 61800–61809. [Google Scholar] [CrossRef]
- Flatmark, K.; Guldvik, I.J.; Svensson, H.; Fleten, K.G.; Flørenes, V.A.; Reed, W.; Giercksky, K.-E.; Fodstad, Ø.; Andersson, Y. Immunotoxin targeting EpCAM effectively inhibits peritoneal tumor growth in experimental models of mucinous peritoneal surface malignancies. Int. J. Cancer 2013, 133, 1497–1506. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Markers | High-Grade PMP (n = 10) | Low-Grade PMP (n = 10) | ||
|---|---|---|---|---|
| Median | Min–Max | Median | Min–Max | |
| CD31 | 15.5 | 9–28 | 19.5 | 6–27 |
| CD105 | 12 | 6–21 | 10 | 4–19 |
| Hif1α | 2.5 | 1–4 | 2 | 1–5 |
| Ki67 | 4 † | 3–5 | 2 † | 1–4 |
| (a) | † Patient Tumor Tissue (pg/mL) | # “Normal” Human Serum Values (pg/mL) | ||
| Median | Min–Max | Median | ||
| VEGFA | 1660 | 0–29,225 | 194 | |
| VEGFC | 307 | 0–3107 | 208 | |
| VEGFD | 1618 | 93–2337 | 929 | |
| PlGF | 469 | 124–1898 | 6 | |
| FGF2 | 1558 | 11–27,591 | <2 | |
| Angiopoietin | 5707 | 900–27,591 | 37,122 | |
| sflt1 | 2230 | 544–11,539 | 126 | |
| Tie2 | 1258 | 0–2336 | 6153 | |
| (b) | ‡ PDX Tumor Tissue (pg/mL) | |||
| Median | Min–Max | |||
| hVEGFA | 22,333 | 15,476–34,237 | ||
| mVEGFA | 780 | 700–1240 | ||
| hPlGF | nd | nd | ||
| mPlGF | 2447 | 1133–2848 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andersson, Y.; Fleten, K.G.; Abrahamsen, T.W.; Reed, W.; Davidson, B.; Flatmark, K. Anti-Angiogenic Treatment in Pseudomyxoma Peritonei—Still a Strong Preclinical Rationale. Cancers 2021, 13, 2819. https://doi.org/10.3390/cancers13112819
Andersson Y, Fleten KG, Abrahamsen TW, Reed W, Davidson B, Flatmark K. Anti-Angiogenic Treatment in Pseudomyxoma Peritonei—Still a Strong Preclinical Rationale. Cancers. 2021; 13(11):2819. https://doi.org/10.3390/cancers13112819
Chicago/Turabian StyleAndersson, Yvonne, Karianne G. Fleten, Torveig W. Abrahamsen, Wenche Reed, Ben Davidson, and Kjersti Flatmark. 2021. "Anti-Angiogenic Treatment in Pseudomyxoma Peritonei—Still a Strong Preclinical Rationale" Cancers 13, no. 11: 2819. https://doi.org/10.3390/cancers13112819
APA StyleAndersson, Y., Fleten, K. G., Abrahamsen, T. W., Reed, W., Davidson, B., & Flatmark, K. (2021). Anti-Angiogenic Treatment in Pseudomyxoma Peritonei—Still a Strong Preclinical Rationale. Cancers, 13(11), 2819. https://doi.org/10.3390/cancers13112819