Worldwide Review and Meta-Analysis of Cohort Studies Measuring the Effect of Mammography Screening Programmes on Incidence-Based Breast Cancer Mortality


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection of Sources of Evidence
2.3. Statistical Methods
Adjustment for Self-Selection Bias
3. Results
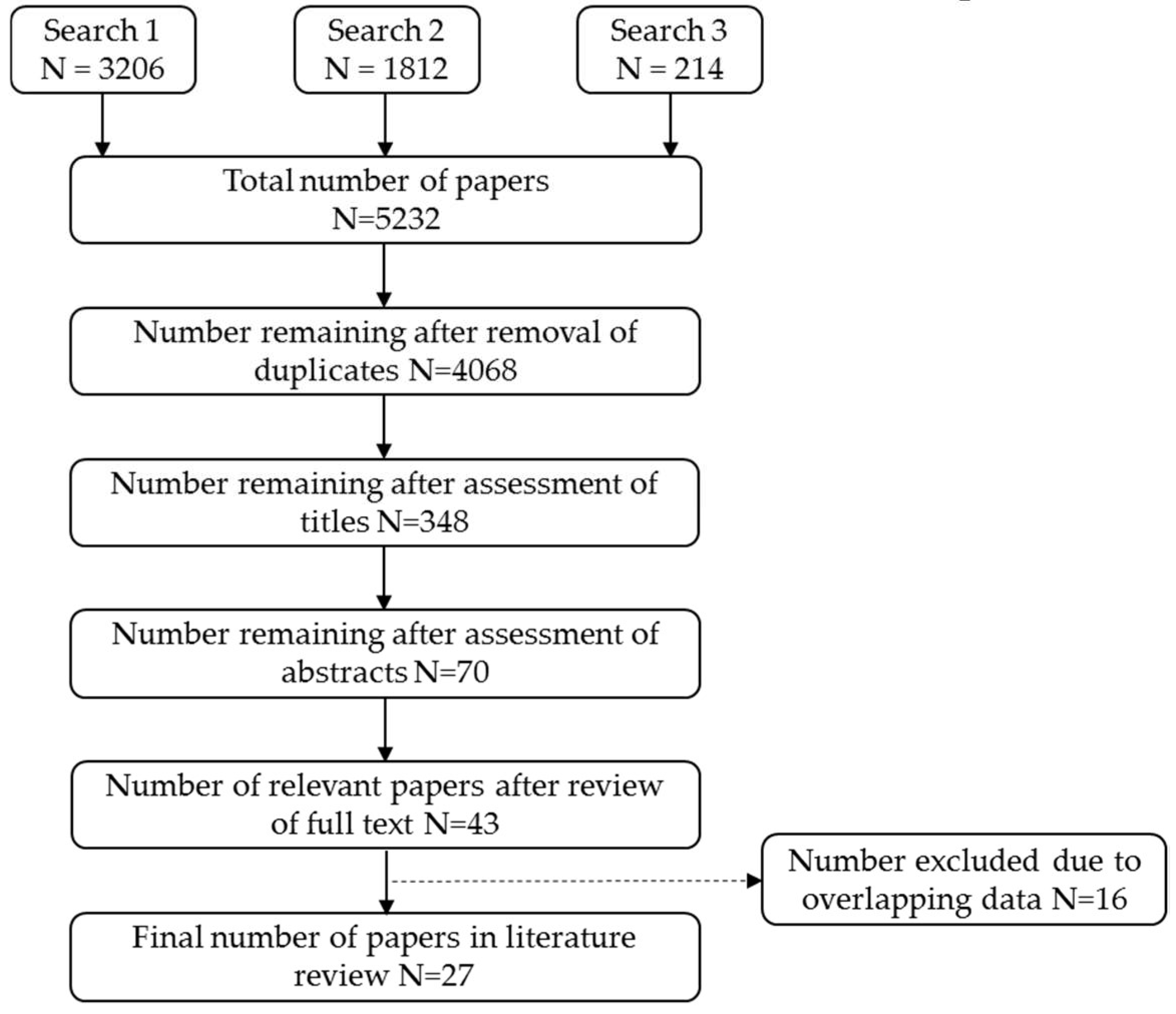
3.1. Literature Selection
3.2. Study Findings
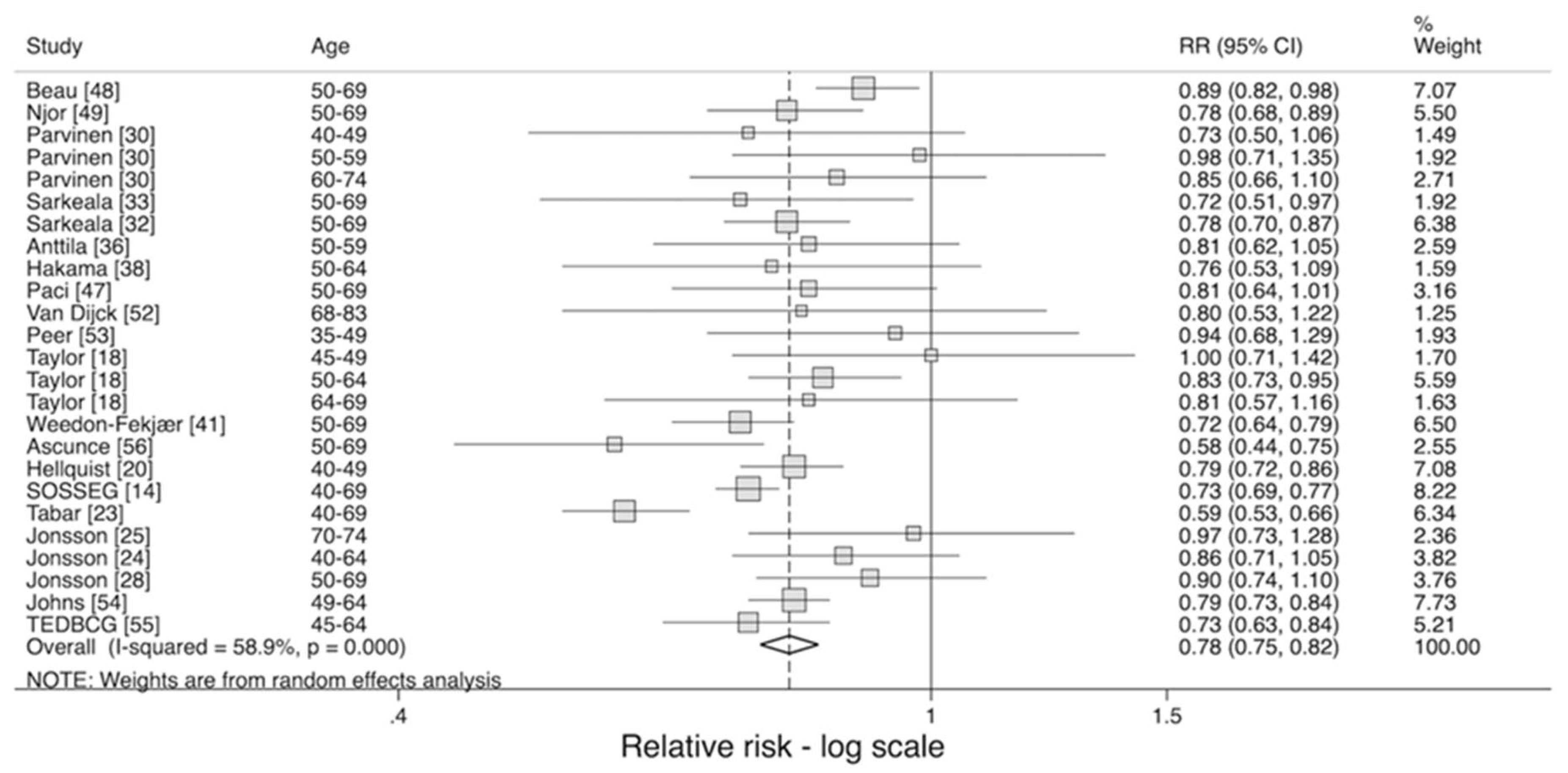
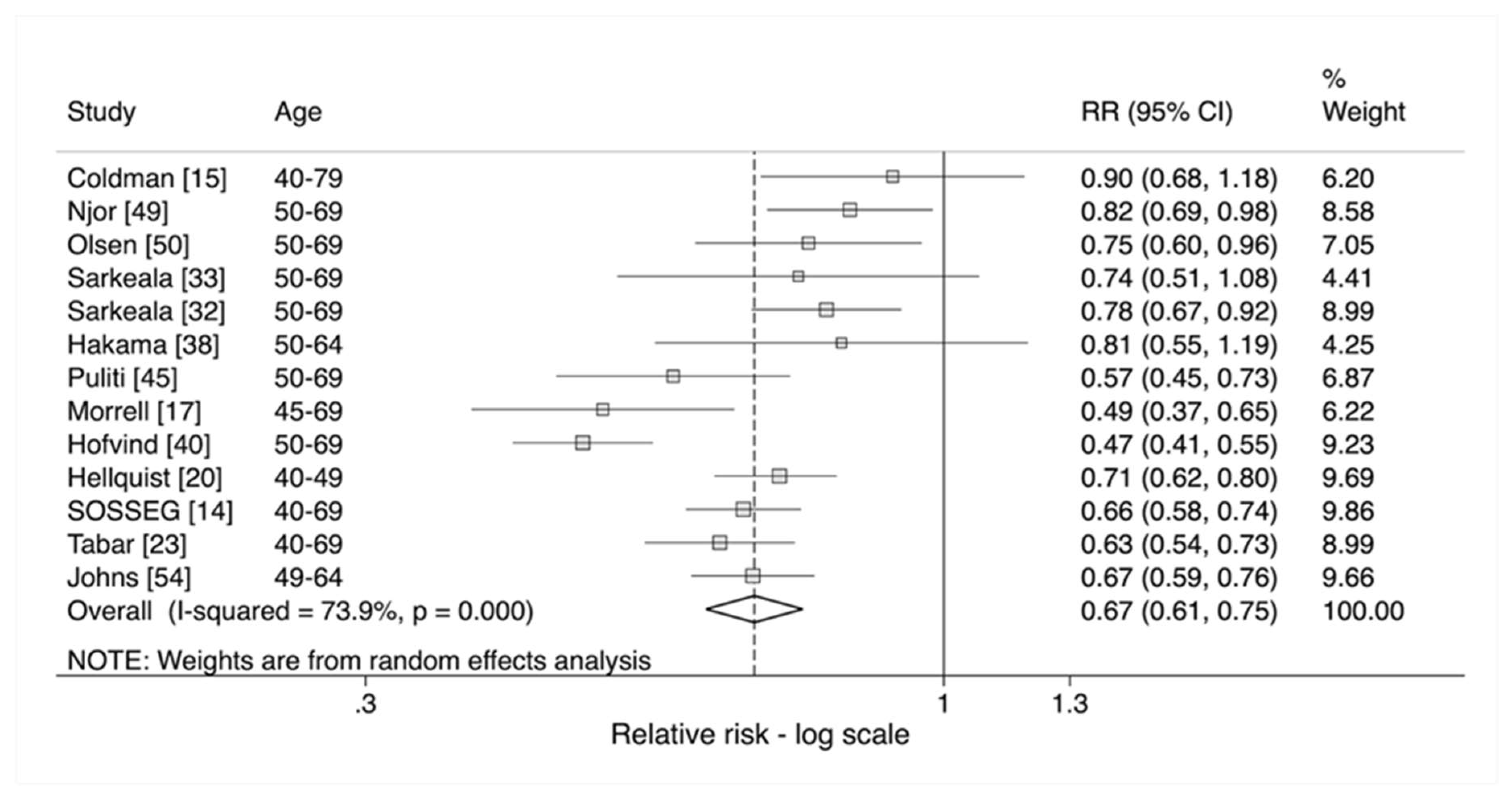
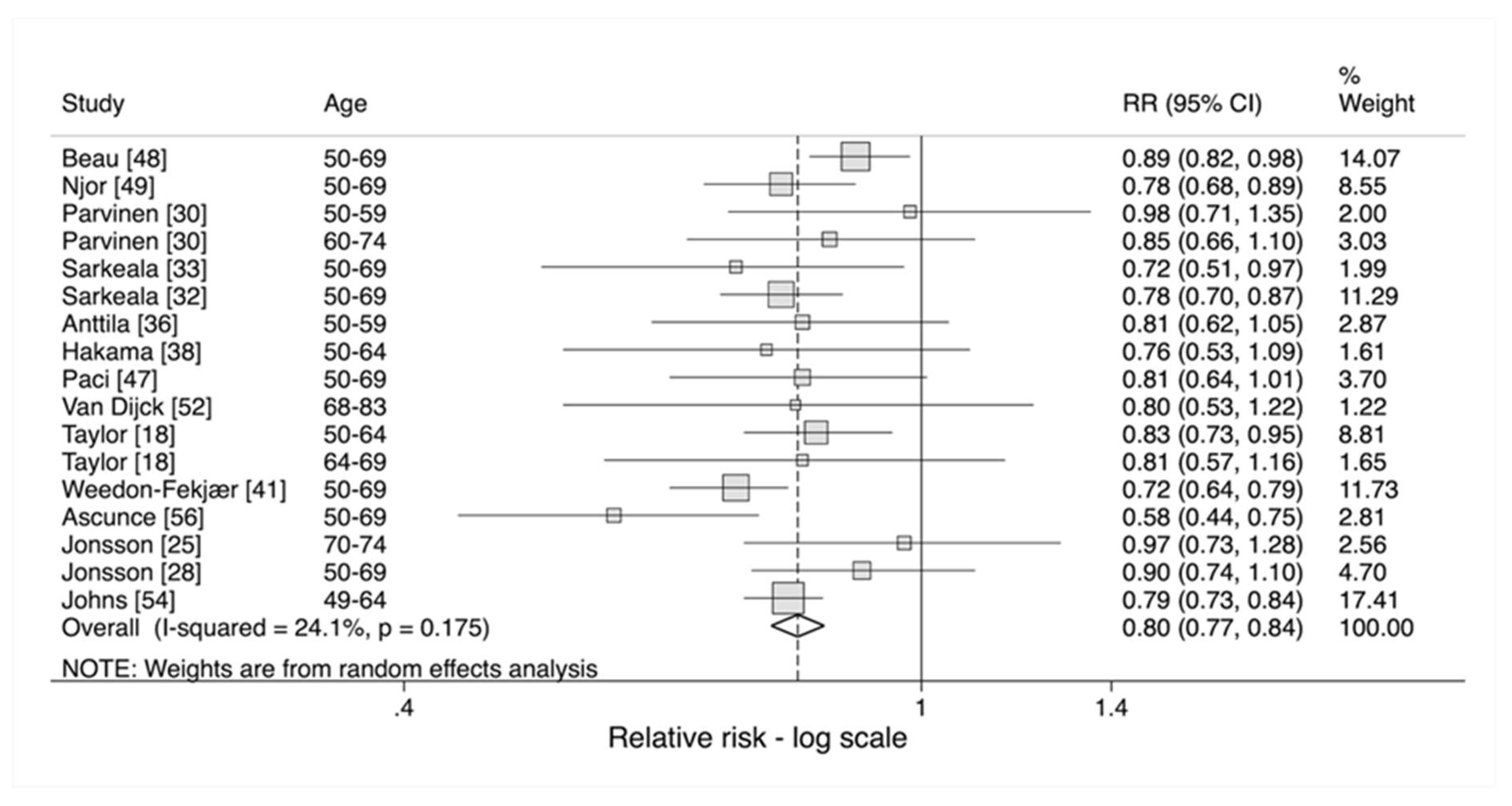
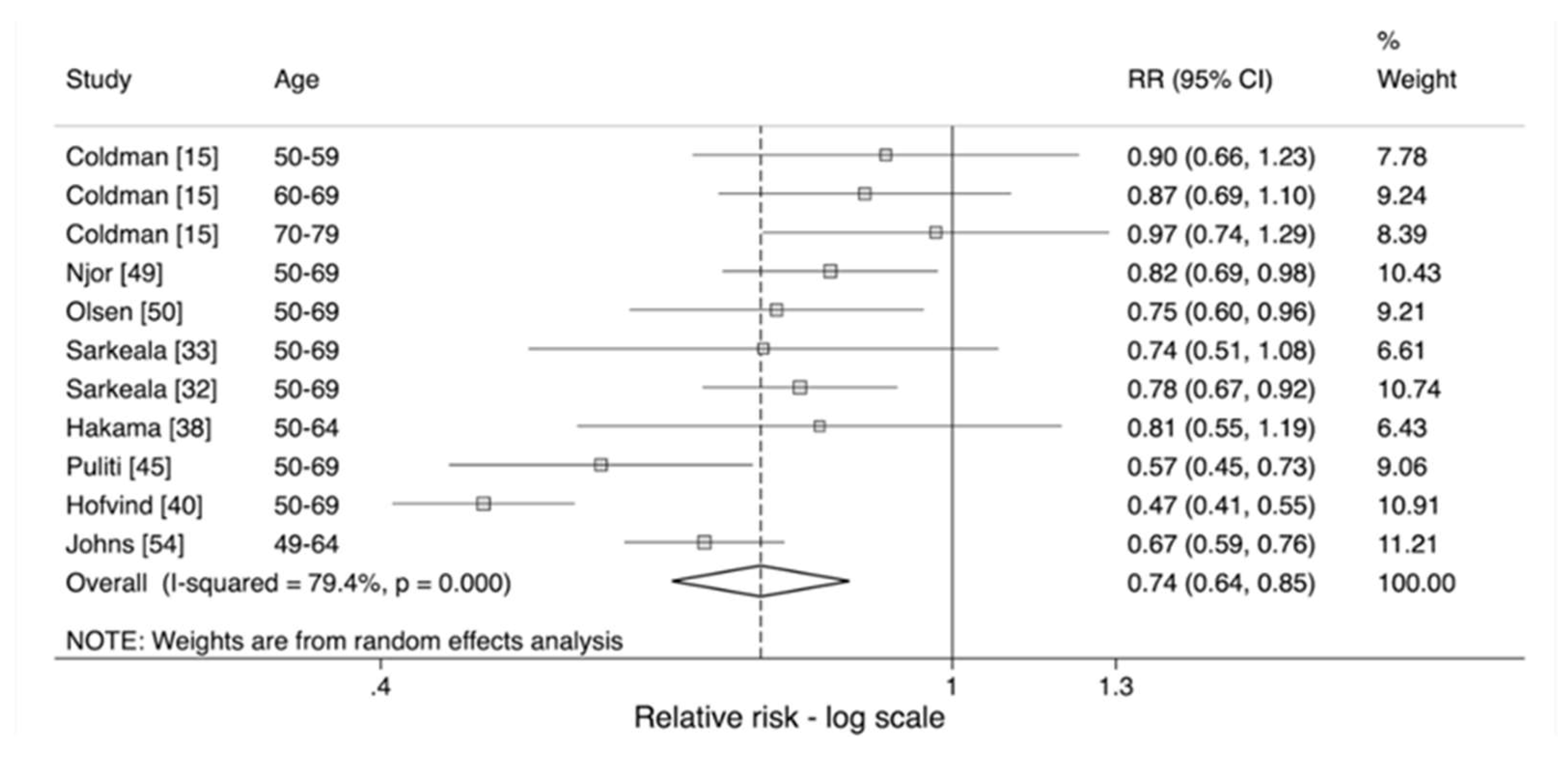
3.3. Meta-Analysis by Age-Group of Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
Search Strategy
- (1)
- (“breast neoplasms/mortality*” [MeSH Terms] OR breast cancer mortality OR “mortality” [MeSH Terms]) AND ((“mass screening” [MeSH Terms] OR screening) AND (“mammography” [MeSH Terms] OR mammography) AND English [lang] [8]
- (2)
- (effect* OR evaluation OR impact OR trend) AND (service screening OR programme screening OR mass screening) AND breast cancer AND (mortality OR survival) AND English [lang]
- (3)
- “Breast neoplasm/mortality*” [MeSH Terms] AND “mass screening” [MeSH Terms] AND (“mortality/trends” [MeSH Terms] OR “survival analysis” [MeSH Terms] OR “survival rate/trends” [MeSH Terms]) AND English [lang]
References
- Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: An independent review. Lancet (Lond. Engl.) 2012, 380, 1778–1786. [Google Scholar] [CrossRef]
- Gotzsche, P.C.; Jorgensen, K.J. Screening for breast cancer with mammography. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Cancer Research UK. Breast Cancer Incidence Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/incidence-invasive#heading-Two (accessed on 24 April 2019).
- Cancer Research UK. Breast Cancer Mortality Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/mortality#heading-Two (accessed on 24 April 2019).
- Broeders, M.; Moss, S.; Nystrom, L.; Njor, S.; Jonsson, H.; Paap, E.; Massat, N.; Duffy, S.; Lynge, E.; Paci, E. The impact of mammographic screening on breast cancer mortality in Europe: A review of observational studies. J. Med. Screen. 2012, 19, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Gabe, R.; Duffy, S.W. Evaluation of service screening mammography in practice: The impact on breast cancer mortality. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2005, 16, ii153–ii162. [Google Scholar] [CrossRef]
- Chu, K.C.; Miller, B.A.; Feuer, E.J.; Hankey, B.F. A method for partitioning cancer mortality trends by factors associated with diagnosis: An application to female breast cancer. J. Clin. Epidemiol. 1994, 47, 1451–1461. [Google Scholar] [CrossRef]
- Njor, S.; Nystrom, L.; Moss, S.; Paci, E.; Broeders, M.; Segnan, N.; Lynge, E. Breast cancer mortality in mammographic screening in Europe: A review of incidence-based mortality studies. J. Med. Screen. 2012, 19, 33–41. [Google Scholar] [CrossRef]
- Duffy, S.W.; Chen, T.H.H.; Yen, A.M.F.; Tabar, L.; Gabe, R.; Smith, R.A. Methodologic Issues in the Evaluation of Service Screening. Semin. Breast Dis. 2007, 10, 68–71. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M. Systematic Reviews in Health Care: Meta-Analysis in Context, 2nd ed.; BMJ Publishing Group: London, UK, 2008; Volume 2, pp. 211–227. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Duffy, S.W. Case-Control Studies to Evaluate the Effect of Mammographic Service Screening on Mortality from Breast Cancer. Semin. Breast Dis. 2007, 10, 61–63. [Google Scholar] [CrossRef]
- Duffy, S.W.; Cuzick, J.; Tabar, L.; Vitak, B.; Hsiu-Hsi Chen, T.; Yen, M.-F.; Smith, R.A. Correcting for non-compliance bias in case–control studies to evaluate cancer screening programmes. J. R. Stat. Soc. Ser. C (Appl. Stat.) 2002, 51, 235–243. [Google Scholar] [CrossRef]
- Swedish Organised Service Screening Evaluation Group. Reduction in breast cancer mortality from organized service screening with mammography: 1. Further confirmation with extended data. Cancer Epidemiol. Biomark. Prev. 2006, 15, 45–51. [Google Scholar] [CrossRef]
- Coldman, A.; Phillips, N.; Wilson, C.; Decker, K.; Chiarelli, A.M.; Brisson, J.; Zhang, B.; Payne, J.; Doyle, G.; Ahmad, R. Pan-Canadian study of mammography screening and mortality from breast cancer. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.S.; Barlow, W.E.; Taplin, S.H.; Grothaus, L.; Immanuel, V.; Salazar, A.; Wagner, E.H. A population-based case-cohort evaluation of the efficacy of mammographic screening for breast cancer. Am. J. Epidemiol. 1994, 140, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Morrell, S.; Taylor, R.; Roder, D.; Robson, B.; Gregory, M.; Craig, K. Mammography service screening and breast cancer mortality in New Zealand: A National Cohort Study 1999–2011. Br. J. Cancer 2017, 116, 828–839. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Gregory, M.; Sexton, K.; Wharton, J.; Sharma, N.; Amoyal, G.; Morrell, S. Breast cancer mortality and screening mammography in New Zealand: Incidence-based and aggregate analyses. J. Med. Screen. 2019, 26, 35–43. [Google Scholar] [CrossRef]
- Hellquist, B.N.; Czene, K.; Hjalm, A.; Nystrom, L.; Jonsson, H. Effectiveness of population-based service screening with mammography for women ages 40 to 49 years with a high or low risk of breast cancer: Socioeconomic status, parity, and age at birth of first child. Cancer 2015, 121, 251–258. [Google Scholar] [CrossRef]
- Hellquist, B.N.; Duffy, S.W.; Abdsaleh, S.; Bjorneld, L.; Bordas, P.; Tabar, L.; Vitak, B.; Zackrisson, S.; Nystrom, L.; Jonsson, H. Effectiveness of population-based service screening with mammography for women ages 40 to 49 years: Evaluation of the Swedish Mammography Screening in Young Women (SCRY) cohort. Cancer 2011, 117, 714–722. [Google Scholar] [CrossRef]
- Jonsson, H.; Bordas, P.; Wallin, H.; Nystrom, L.; Lenner, P. Service screening with mammography in Northern Sweden: Effects on breast cancer mortality—An update. J. Med. Screen. 2007, 14, 87–93. [Google Scholar] [CrossRef]
- Baker, S.G.; Kramer, B.S.; Prorok, P.C. Comparing breast cancer mortality rates before-and-after a change in availability of screening in different regions: Extension of the paired availability design. BMC Med. Res. Methodol. 2004, 4, 12. [Google Scholar] [CrossRef]
- Tabar, L.; Yen, M.F.; Vitak, B.; Chen, H.H.; Smith, R.A.; Duffy, S.W. Mammography service screening and mortality in breast cancer patients: 20-year follow-up before and after introduction of screening. Lancet (Lond. Engl.) 2003, 361, 1405–1410. [Google Scholar] [CrossRef]
- Jonsson, H.; Nystrom, L.; Tornberg, S.; Lundgren, B.; Lenner, P. Service screening with mammography. Long-term effects on breast cancer mortality in the county of Gavleborg, Sweden. Breast (Edinb. Scotl.) 2003, 12, 183–193. [Google Scholar] [CrossRef]
- Jonsson, H.; Tornberg, S.; Nystrom, L.; Lenner, P. Service screening with mammography of women aged 70-74 years in Sweden. Effects on breast cancer mortality. Cancer Detect. Prev. 2003, 27, 360–369. [Google Scholar] [CrossRef]
- Duffy, S.W.; Tabar, L.; Chen, H.H.; Holmqvist, M.; Yen, M.F.; Abdsalah, S.; Epstein, B.; Frodis, E.; Ljungberg, E.; Hedborg-Melander, C.; et al. The impact of organized mammography service screening on breast carcinoma mortality in seven Swedish counties. Cancer 2002, 95, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Tabar, L.; Vitak, B.; Chen, H.H.; Yen, M.F.; Duffy, S.W.; Smith, R.A. Beyond randomized controlled trials: Organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001, 91, 1724–1731. [Google Scholar] [CrossRef]
- Jonsson, H.; Nystrom, L.; Tornberg, S.; Lenner, P. Service screening with mammography of women aged 50-69 years in Sweden: Effects on mortality from breast cancer. J. Med. Screen. 2001, 8, 152–160. [Google Scholar] [CrossRef]
- Jonsson, H.; Tornberg, S.; Nystrom, L.; Lenner, P. Service screening with mammography in Sweden--evaluation of effects of screening on breast cancer mortality in age group 40–49 years. Acta Oncol. (Stockh. Swed.) 2000, 39, 617–623. [Google Scholar]
- Parvinen, I.; Heinavaara, S.; Anttila, A.; Helenius, H.; Klemi, P.; Pylkkanen, L. Mammography screening in three Finnish residential areas: Comprehensive population-based study of breast cancer incidence and incidence-based mortality 1976–2009. Br. J. Cancer 2015, 112, 918–924. [Google Scholar] [CrossRef]
- Wu, J.C.-Y.; Anttila, A.; Yen, A.M.-F.; Hakama, M.; Saarenmaa, I.; Sarkeala, T.; Malila, N.; Auvinen, A.; Chiu, S.Y.-H.; Chen, T.H.-H. Evaluation of breast cancer service screening programme with a Bayesian approach: Mortality analysis in a Finnish region. Breast Cancer Res. Treat. 2010, 121, 671–678. [Google Scholar] [CrossRef]
- Sarkeala, T.; Heinavaara, S.; Anttila, A. Organised mammography screening reduces breast cancer mortality: A cohort study from Finland. Int. J. Cancer 2008, 122, 614–619. [Google Scholar] [CrossRef]
- Sarkeala, T.; Heinavaara, S.; Anttila, A. Breast cancer mortality with varying invitational policies in organised mammography. Br. J. Cancer 2008, 98, 641–645. [Google Scholar] [CrossRef]
- Anttila, A.; Sarkeala, T.; Hakulinen, T.; Heinavaara, S. Impacts of the Finnish service screening programme on breast cancer rates. BMC Public Health 2008, 8, 38. [Google Scholar] [CrossRef]
- Parvinen, I.; Helenius, H.; Pylkkanen, L.; Anttila, A.; Immonen-Raiha, P.; Kauhava, L.; Rasanen, O.; Klemi, P.J. Service screening mammography reduces breast cancer mortality among elderly women in Turku. J. Med. Screen. 2006, 13, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Anttila, A.; Koskela, J.; Hakama, M. Programme sensitivity and effectiveness of mammography service screening in Helsinki, Finland. J. Med. Screen. 2002, 9, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Hakama, M.; Pukkala, E.; Soderman, B.; Day, N. Implementation of screening as a public health policy: Issues in design and evaluation. J. Med. Screen. 1999, 6, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Hakama, M.; Pukkala, E.; Heikkila, M.; Kallio, M. Effectiveness of the public health policy for breast cancer screening in Finland: Population based cohort study. BMJ (Clin. Res. Ed.) 1997, 314, 864–867. [Google Scholar] [CrossRef]
- Moller, M.H.; Lousdal, M.L.; Kristiansen, I.S.; Stovring, H. Effect of organized mammography screening on breast cancer mortality: A population-based cohort study in Norway. Int. J. Cancer 2019, 144, 697–706. [Google Scholar] [CrossRef]
- Hofvind, S.; Ursin, G.; Tretli, S.; Sebuodegard, S.; Moller, B. Breast cancer mortality in participants of the Norwegian Breast Cancer Screening Program. Cancer 2013, 119, 3106–3112. [Google Scholar] [CrossRef]
- Weedon-Fekjaer, H.; Romundstad, P.R.; Vatten, L.J. Modern mammography screening and breast cancer mortality: Population study. BMJ (Clin. Res. Ed.) 2014, 348, g3701. [Google Scholar] [CrossRef]
- Olsen, A.H.; Lynge, E.; Njor, S.H.; Kumle, M.; Waaseth, M.; Braaten, T.; Lund, E. Breast cancer mortality in Norway after the introduction of mammography screening. Int. J. Cancer 2013, 132, 208–214. [Google Scholar] [CrossRef]
- Kalager, M.; Zelen, M.; Langmark, F.; Adami, H.O. Effect of screening mammography on breast-cancer mortality in Norway. N. Engl. J. Med. 2010, 363, 1203–1210. [Google Scholar] [CrossRef]
- Capodaglio, G.; Zorzi, M.; Tognazzo, S.; Greco, A.; Michieletto, F.; Fedato, C.; Montaguti, A.; Turrin, A.; Ferro, A.; Cinquetti, S.; et al. Impact of breast cancer screening in a population with high spontaneous coverage with mammography. Tumori 2018, 104, 258–265. [Google Scholar] [CrossRef]
- Puliti, D.; Miccinesi, G.; Zappa, M.; Manneschi, G.; Crocetti, E.; Paci, E. Balancing harms and benefits of service mammography screening programs: A cohort study. Breast Cancer Res. BCR 2012, 14, R9. [Google Scholar] [CrossRef] [PubMed]
- Paci, E.; Duffy, S.W.; Giorgi, D.; Zappa, M.; Crocetti, E.; Vezzosi, V.; Bianchi, S.; del Turco, M.R. Quantification of the effect of mammographic screening on fatal breast cancers: The Florence Programme 1990–1996. Br. J. Cancer 2002, 87, 65–69. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Paci, E.; Giorgi, D.; Bianchi, S.; Vezzosi, V.; Zappa, M.; Crocetti, E.; Rosselli del Turco, M. Assessment of the early impact of the population-based breast cancer screening programme in Florence (Italy) using mortality and surrogate measures. Eur. J. Cancer (Oxf. Engl. 1990) 2002, 38, 568–573. [Google Scholar] [CrossRef]
- Beau, A.B.; Andersen, P.K.; Vejborg, I.; Lynge, E. Limitations in the Effect of Screening on Breast Cancer Mortality. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2988–2994. [Google Scholar] [CrossRef] [PubMed]
- Njor, S.H.; Schwartz, W.; Blichert-Toft, M.; Lynge, E. Decline in breast cancer mortality: How much is attributable to screening? J. Med. Screen. 2015, 22, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Olsen, A.H.; Njor, S.H.; Vejborg, I.; Schwartz, W.; Dalgaard, P.; Jensen, M.B.; Tange, U.B.; Blichert-Toft, M.; Rank, F.; Mouridsen, H.; et al. Breast cancer mortality in Copenhagen after introduction of mammography screening: Cohort study. BMJ (Clin. Res. Ed.) 2005, 330, 220. [Google Scholar] [CrossRef]
- Olsen, A.H.; Njor, S.H.; Lynge, E. Estimating the benefits of mammography screening: The impact of study design. Epidemiology (Camb. Mass.) 2007, 18, 487–492. [Google Scholar] [CrossRef]
- Van Dijck, J.A.; Verbeek, A.L.; Beex, L.V.; Hendriks, J.H.; Holland, R.; Mravunac, M.; Straatman, H.; Werre, J.M. Breast-cancer mortality in a non-randomized trial on mammographic screening in women over age 65. Int. J. Cancer 1997, 70, 164–168. [Google Scholar] [CrossRef]
- Peer, P.G.; Werre, J.M.; Mravunac, M.; Hendriks, J.H.; Holland, R.; Verbeek, A.L. Effect on breast cancer mortality of biennial mammographic screening of women under age 50. Int. J. Cancer 1995, 60, 808–811. [Google Scholar] [CrossRef][Green Version]
- Johns, L.E.; Coleman, D.A.; Swerdlow, A.J.; Moss, S.M. Effect of population breast screening on breast cancer mortality up to 2005 in England and Wales: An individual-level cohort study. Br. J. Cancer 2017, 116, 246–252. [Google Scholar] [CrossRef]
- UK Trial of Early Detection of Breast Cancer Group. 16-year mortality from breast cancer in the UK Trial of Early Detection of Breast Cancer. Lancet (Lond. Engl.) 1999, 353, 1909–1914. [Google Scholar] [CrossRef]
- Ascunce, E.N.; Moreno-Iribas, C.; Barcos Urtiaga, A.; Ardanaz, E.; Ederra Sanz, M.; Castilla, J.; Egues, N. Changes in breast cancer mortality in Navarre (Spain) after introduction of a screening programme. J. Med. Screen. 2007, 14, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Giordano, L.; von Karsa, L.; Tomatis, M.; Majek, O.; de Wolf, C.; Lancucki, L.; Hofvind, S.; Nyström, L.; Segnan, N.; Ponti, A. Mammographic screening programmes in Europe: Organization, coverage and participation. J. Med. Screen. 2012, 19, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Swedish Organised Service Screening Evaluation Group. Reduction in breast cancer mortality from the organised service screening with mammography: 2. Validation with alternative analytic methods. Cancer Epidemiol. Biomark. Prev. 2006, 15, 52–56. [Google Scholar] [CrossRef]
- Doyle, G.P.; Major, D.; Chu, C.; Stankiewicz, A.; Harrison, M.L.; Pogany, L.; Mai, V.M.; Onysko, J. A review of screening mammography participation and utilization in Canada. Chronic Dis. Inj. Can. 2011, 31, 152–156. [Google Scholar]
- Breslow, N.E.; Day, N.E. Statistical Methods in Cancer Research. Vol II. The Deisgn and Analysis of Cohort Studies; International Agency for Cancer Research: Lyon, France, 1987. [Google Scholar]
- Tabár, L.; Vitak, B.; Chen, T.H.-H.; Yen, A.M.-F.; Cohen, A.; Tot, T.; Chiu, S.Y.-H.; Chen, S.L.-S.; Fann, J.C.-Y.; Rosell, J.; et al. Swedish Two-County Trial: Impact of Mammographic Screening on Breast Cancer Mortality during 3 Decades. Radiology 2011, 260, 658–663. [Google Scholar] [CrossRef]
- Moss, S.M.; Nystrom, L.; Jonsson, H.; Paci, E.; Lynge, E.; Njor, S.; Broeders, M. The impact of mammographic screening on breast cancer mortality in Europe: A review of trend studies. J. Med. Screen. 2012, 19, 26–32. [Google Scholar] [CrossRef]
- Tabar, L.; Dean, P.B.; Chen, T.H.; Yen, A.M.; Chen, S.L.; Fann, J.C.; Chiu, S.Y.; Ku, M.M.; Wu, W.Y.; Hsu, C.Y.; et al. The incidence of fatal breast cancer measures the increased effectiveness of therapy in women participating in mammography screening. Cancer 2019, 125, 515–523. [Google Scholar] [CrossRef]
- Sasieni, P. On the expected number of cancer deaths during follow-up of an initially cancer-free cohort. Epidemiology (Camb. Mass.) 2003, 14, 108–110. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effect of Invitation to Screening | Effect of Attendance Adjusted for Self-Selection |
|---|---|
| Reference (by Country and Date) | Region | Age Range of Screening | Screening Interval | Comparison Group(s) | Accrual/follow up Period in Screening Group | Accrual/follow up Period in Comparison Group | Person-Years Study/Comparison Groups(Average Population) |
|---|---|---|---|---|---|---|---|
| Coldman, 2014 [15] | 7 provinces, Canada | 40–79 depending on province | 2 years 1 | Contemporaneous | 1990–2009 | Same | 20,155,000 |
| Beau, 2018 [48] | Copenhagen, Denmark | 50–69 | 2 years | Regional and historical | 1991–2007 | 1977–1991 (pre-screening) 1991–2007 (screening) | 976,743/17,804,549 |
| Njor, 2015 [49] | Funen, Denmark | 50–69 | 2 years | Regional and historical | 1993–2007/09 | 1979–1993/95 (pre-screening) 1993–2007/09 (screening) | 870,465/ 7,096,056; 828,508; 6,151,011 |
| Olsen, 2005 [50] | Copenhagen, Denmark | 50–69 | 2 years | Regional and historical | 1991–2001 | 1981–1991 (pre-screening) 1991–2001 (screening) | 430,823/ 634,224; 4,396,417; 4,055,004 |
| Parvinen, 2015 [30] | Turku, Finland | 40–74 | 2 years 2 | Regional and historical | 1987–2009 | 1976–1986 (pre-screening) 1987–2009 (screening) | 853,297/ Helsinki: 2,700,574; Rest of Finland: 21,761,900 |
| Sarkeala, 2008 [33] | 8 municipalities, Finland | 50–69 | 2 years | Historical | 1992–2003 | 1974–1985 (pre-screening) 1992–2003 (screening) | 228,527 |
| Sarkeala, 2008 [32] | 260 municipalities, Finland | 50–69 | 2 years | Historical | 1992–2003 | 1974–1985 (pre-screening) 1992–2003 (screening) | 2,731,268 |
| Anttila, 2002 [36] | Helsinki, Finland | 50–59 | 2 years | Contemporaneous 3 | 1986–1997 | Same | 161,400/155,400 |
| Hakama, 1997 [38] | Finland | 50–64 | 2 years | Contemporaneous | 1987–1989/1992 | Same | 400,804/299,228 |
| Puliti, 2012 [45] | Florence, Italy | 50–69 | 2 years | Contemporaneous | 1991–2007/08 | Same | 50–59: 270,399/113,409 60–69: 233,543/151,615 |
| Paci, 2002 [47] | Florence, Italy | 50–69 | 2 years | Contemporaneous | 1990–1996/99 | Same | 254,890 |
| Van Dijck, 1997 [52] | Nijmegen, Netherlands | 68–83 | 2 years | Regional | 1977–1990 | 1978–1990 | 60,313/ 61,832 |
| Peer, 1995 [53] | Nijmegen, Netherlands | 35–49 | 2 years | Regional | 1975–1990 | 1976–1990 | 166,307/ 154,103 |
| Taylor, 2019 [18] | New Zealand | 50–64 45–49/ 65–69 | 2 years | Historical | 2001–03/ 2009–11 2006–08/ 2009–11 | 1996–98/ 2004–06 2001–03/ 2004–06 | 930,000/766,000 480,000/409,000 249,000/205,000 4 |
| Morrell, 2017 [17] | New Zealand | 45–69 | 2 years | Contemporaneous | 1999–2011/ 2000–2011 | Same | 3,707,483/ 5,405,518 |
| Weedon-Fekjær, 2014 [41] | Norway | 50–69 | 2 years | Contemporaneous | 1986–2009 | Same | 2,407,709/ 12,785,325 |
| Hofvind, 2013 [40] | Norway | 50–69 | 2 years | Contemporaneous 5 | 1996–2009/10 | Same | 4,814,060/ 988,641 |
| Ascunce, 2007 [56] | Navarre, Spain | 50–69 | 2 years | Historical | 1991–2001/ 1997–2001 | 1980–1990/ 1986–1990 | 293,000/ 289,000 6 |
| Hellquist, 2011 [20] | Sweden | 40–49 | 1.5–2 years | Regional | 1986–2005 | Same | 7,261,415/ 8,843,852 |
| SOSSEG, 2006 [14] | 13 counties, Sweden | 40–69 depending on county | 2 years | Historical | 1980–2001 depending on county | 1958–1989 depending on county | 7,542,833/ 7,265,841 |
| Tabar, 2003 [23] | Östergötland and Dalarna, Sweden | 40–69 | 1.5–2 years | Historical | 1978–1997 | 1958–1977 | 2,399,000/ 2,416,000 |
| Jonsson, 2003 [25] | 10 counties, Sweden | 70–74 | 2 years | Regional and historical | 1986–1998 | 1976–1988 (pre-screening) 1986–1998 (screening) | 1,251,300/ 580,100; 533,400; 1,162,800 |
| Jonsson, 2003 [24] | Gӓvleborg, Sweden | 40–64 | 2 years 7 | Regional and historical | 1974–1986/1998 | 1964–1973/1985 (pre-screening) 1974–1986/1998 (screening) | 855,000/ 2,581,000; 12,619,000 |
| Jonsson, 2001 [28] | 7 counties, Sweden | 50–69 | 2 years | Regional and historical | 1986–1994/97 | 1979–1987/1990 (pre-screening) 1987–1993/97 (screening) | 2,0360,00/ 1,265,000; 2,046,000; 1,296,000 |
| Johns, 2017 [54] | England and Wales, UK | 49–64 | 3 years | Contemporaneous | 1991–2005 8 | Same | 1,675,356/ 4,719,228 |
| UK Trial of Early Detection of Breast Cancer Group, 1999 [55] | Guildford and Edinburgh, UK | 45–64 | 2 years | Regional | 1979–1995 | Same | (45,607/ 127,123) |
| Thompson [16] | Washington, USA | 40+ if high risk/50+ if low risk | 3 years | Contemporaneous | 1982–1988 | Same | (94,656) |
| Reference (by Country and Date) | Country | Age at Screening | Attendance | RR: Unadjusted Effect on Incidence-Based Breast Cancer Mortality | RR Calculated from Effect of Attendance | RR Adjusted for Self-Selection | |
|---|---|---|---|---|---|---|---|
| Invited Versus not Invited 1 | Screened Versus not Screened 1 | ||||||
| Coldman, 2014 [15] | 7 provinces, Canada | 40–79 40–49 50–59 60–69 70–79 | 0.437 | NR | 0.60 (0.52–0.67) 0.56 (0.45–0.67) 2 0.60 (0.49–0.70) 0.58 (0.50–0.67) 0.65 (0.56–0.74) 3 | 0.97 (0.88–1.06) 0.95 (0.85–1.05) 0.97 (0.87–1.07) 0.96 (0.87–1.05) 0.99 (0.90–1.09) | 0.90 (0.68–1.18) 0.84 (0.61–1.16) 0.90 (0.66–1.23) 0.87 (0.69–1.10) 0.97 (0.74–1.29) |
| Beau, 2018 [48] | Copenhagen, Denmark | 50–69 | 0.71 4 | 0.89 (0.82–0.98) | NR | NA | NA |
| Njor,2015 [49] | Funen, Denmark | 50–69 | 0.84 | 0.78 (0.68–0.89) | 0.68 (0.59–0.79) | 0.86 (0.75–0.98) | 0.82 (0.69–0.98) |
| Olsen, 2005 [50] | Copenhagen, Denmark | 50–69 | 0.71 | 0.75 (0.63–0.89) 5 | 0.60 (0.49–0.74) | 0.84 (0.72–0.97) | 0.75 (0.60–0.96) |
| Parvinen, 2015 [30] | Turku, Finland | 40–49 50–59 60–74 | 0.867 | 0.73 (0.50–1.06) 0.98 (0.71–1.35) 0.85 (0.66–1.10) | NR | NA | NA |
| Sarkeala, 2008 [33] | 8 municipalities, Finland | 50–69 | 0.905 | 0.72 (0.51–0.97) | 0.62 (0.43–0.85) | 0.77 (0.56–1.06) | 0.74 (0.51–1.08) |
| Sarkeala, 2008 [32] | 260 municipalities, Finland | 50–69 | 0.924 | 0.78 (0.70–0.87) | 0.66 (0.58–0.75) | 0.80 (0.70–0.92) | 0.78 (0.67–0.92) |
| Anttila, 2002 [36] | Helsinki, Finland | 50–59 | 0.82 | 0.81 (0.62–1.05) | NR | NA | NA |
| Hakama, 1997 [38] | Finland | 50–64 | 0.85 | 0.76 (0.53–1.09) | 0.67 (0.46–0.97) 6 | 0.84 (0.62–1.15) | 0.81 (0.55–1.19) |
| Puliti, 2012 [45] | Florence, Italy | 50–69 50–59 60–69 | 0.64 | NR | 0.44 (0.36–0.54) 7 0.55 (0.41–0.75) 0.49 (0.38–0.64) | 0.75 (0.67–0.85) 0.83 (0.71–0.98) 0.79 (0.68–0.91) | 0.57 (0.45–0.73) 0.71 (0.51–0.98) 0.63 (0.47–0.85) |
| Paci, 2002 [47] | Florence, Italy | 50–69 | 0.60 | 0.81 (0.64–1.01) | NR | 0.75 (0.67–0.85) | 0.57 (0.45–0.73) |
| Van Dijck, 1997 [52] | Nijmegen, Netherlands | 68–83 | 0.46 | 0.80 (0.53–1.22) | NR | NA | NA |
| Peer,1995 [53] | Nijmegen, Netherlands | 35–49 | 0.65 | 0.94 (0.68–1.29) | NR | NA | NA |
| Taylor, 2019 [18] | New Zealand | 45–49 50–64 65–69 | 0.72 | 1.00 (0.71–1.42) 8 0.83 (0.73–0.95) 0.81 (0.57–1.16) | NR | NA | NA |
| Morrell, 2017 [17] | New Zealand | 45–69 | 0.64 | NR | 0.38 (0.30–0.49) | 0.71 (0.62–0.80) | 0.49 (0.37–0.65) |
| Weedon-Fekjær, 2014 [41] | Norway | 50–69 | 0.76 | 0.72 (0.64–0.79) | NR | NA | NA |
| Hofvind, 2013 [40] | Norway | 50–69 | 0.84 | NR | 0.39 (0.35–0.44) | 0.57 (0.51–0.64) | 0.47 (0.41–0.55) |
| Ascunce, 2007 [56] | Navarre, Spain | 50–69 | 0.85 | 0.58 (0.44–0.75) 9 | NR | NA | NA |
| Hellquist, 2011 [20] | Sweden | 40–49 | 0.80 | 0.79 (0.72–0.86) | NR | 0.74 (0.66–0.83) 10 | 0.71 (0.62–0.80) |
| SOSSEG, 2006 [14] | 13 counties, Sweden | 40–69 | 0.80 11 | 0.73 (0.69–0.77) | 0.55 (0.51–0.59) | 0.75 (0.68–0.82) | 0.66 (0.58–0.74) |
| Tabar, 2003 [23] | Östergötland and Dalarna, Sweden | 40–69 | 0.85 | 0.59 (0.53–0.66) | 0.52 (0.46–0.59) | 0.69 (0.61–0.78) | 0.63 (0.54–0.73) |
| Jonsson, 2003 [25] | 10 counties, Sweden | 70–74 | 0.84 12 | 0.97 (0.73–1.28) | NR | NA | NA |
| Jonsson, 2003 [24] | Gӓvleborg, Sweden | 40–64 | 0.84 | 0.86 (0.71–1.05) | NR | NA | NA |
| Jonsson, 2001 [28] | 7 counties, Sweden | 50–69 | 0.80 11 | 0.90 (0.74–1.10) | NR | NA | NA |
| Johns, 2017 [54] | England and Wales, UK | 49–64 | 0.74 | 0.79 (0.73–0.84) | 0.54 (0.51–0.57) | 0.77 (0.71–0.84) | 0.67 (0.59–0.76) |
| UK Trial of Early Detection of Breast Cancer Group, 1999 [55] | Guildford and Edinburgh, UK | 45–64 | 0.654 | 0.73 (0.63–0.84) | NR | NA | NA |
| Thompson, 1994 [16] | Washington, USA | ≥50 | NR | NR | 0.61 (0.23–1.62) | NA | NA |
| Pooled RR from all studies | Random effects Heterogeneity p-value | 0.78 (0.75–0.82) <0.001 | 0.54 (0.49–0.59) <0.001 | 0.76 (0.71–0.83) <0.001 | 0.67 (0.61–0.75) <0.001 | ||
| Pooled RR from studies inviting women aged 50 and over | Random effects Heterogeneity p-value | 0.80 (0.77–0.84) 0.175 | 0.57 (0.51–0.64) <0.001 | 0.82 (0.74–0.92) <0.001 | 0.74 (0.64–0.85) <0.001 | ||
| Pooled RR from studies inviting women under 50 years | Random effects Heterogeneity p-value | 0.81 (0.74–0.87) 0.418 | 0.56 (0.45–0.67) 13– | 0.84 (0.66–1.06) 0.002 | 0.73 (0.65–0.82) 0.343 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dibden, A.; Offman, J.; Duffy, S.W.; Gabe, R. Worldwide Review and Meta-Analysis of Cohort Studies Measuring the Effect of Mammography Screening Programmes on Incidence-Based Breast Cancer Mortality. Cancers 2020, 12, 976. https://doi.org/10.3390/cancers12040976
Dibden A, Offman J, Duffy SW, Gabe R. Worldwide Review and Meta-Analysis of Cohort Studies Measuring the Effect of Mammography Screening Programmes on Incidence-Based Breast Cancer Mortality. Cancers. 2020; 12(4):976. https://doi.org/10.3390/cancers12040976
Chicago/Turabian StyleDibden, Amanda, Judith Offman, Stephen W. Duffy, and Rhian Gabe. 2020. "Worldwide Review and Meta-Analysis of Cohort Studies Measuring the Effect of Mammography Screening Programmes on Incidence-Based Breast Cancer Mortality" Cancers 12, no. 4: 976. https://doi.org/10.3390/cancers12040976
APA StyleDibden, A., Offman, J., Duffy, S. W., & Gabe, R. (2020). Worldwide Review and Meta-Analysis of Cohort Studies Measuring the Effect of Mammography Screening Programmes on Incidence-Based Breast Cancer Mortality. Cancers, 12(4), 976. https://doi.org/10.3390/cancers12040976