Preoperative Serum Thyroglobulin and Its Correlation with the Burden and Extent of Differentiated Thyroid Cancer


Abstract
1. Introduction
2. Results
2.1. Baseline Patient Population Characteristics
2.2. Tumor Burden and Recurrence According to Preoperative Thyroglobulin Levels
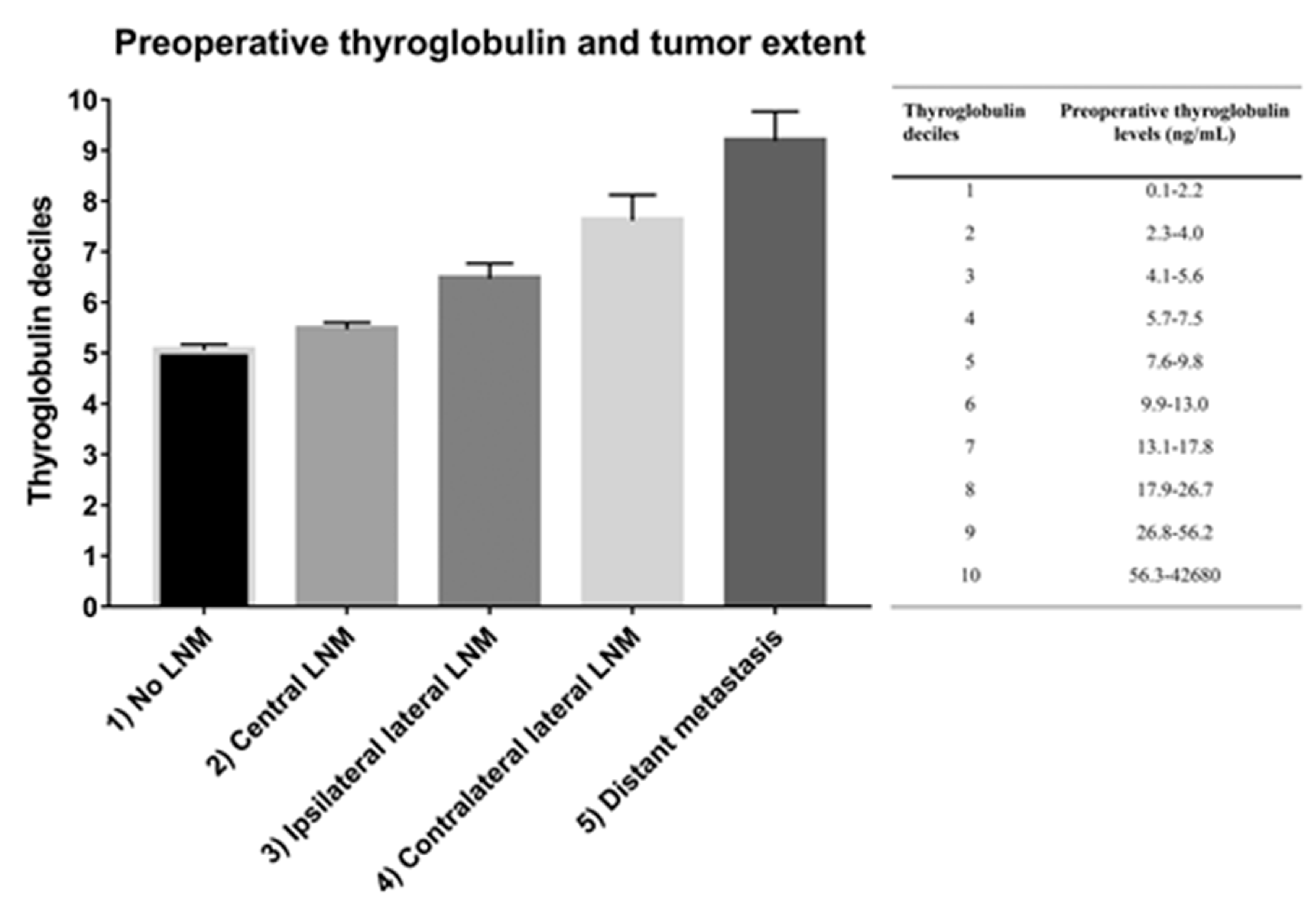
2.3. Tumor Extent According to Preoperative Thyroglobulin Levels
3. Discussion
4. Materials and Methods
Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jung, K.W.; Won, Y.J.; Oh, C.M.; Kong, H.J.; Lee, D.H.; Lee, K.H. Community of population-based regional cancer registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2014. Cancer Res. Treat. 2017, 49, 292–305. [Google Scholar] [CrossRef]
- Sherman, S.I. Thyroid carcinoma. Lancet 2003, 361, 501–511. [Google Scholar] [CrossRef]
- Smith, V.A.; Sessions, R.B.; Lentsch, E.J. Cervical lymph node metastasis and papillary thyroid carcinoma: Does the compartment involved affect survival? Experience from the SEER database. J. Surg. Oncol. 2012, 106, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: What is new and what has changed? Cancer 2017, 123, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Podnos, Y.D.; Smith, D.; Wagman, L.D.; Ellenhorn, J.D. The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am. Surg. 2005, 71, 731–734. [Google Scholar] [PubMed]
- Zaydfudim, V.; Feurer, I.D.; Griffin, M.R.; Phay, J.E. The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma. Surgery 2008, 144, 1070–1077; discussion 1077–1078. [Google Scholar] [CrossRef]
- Kim, E.; Park, J.S.; Son, K.R.; Kim, J.H.; Jeon, S.J.; Na, D.G. Preoperative diagnosis of cervical metastatic lymph nodes in papillary thyroid carcinoma: Comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography. Thyroid 2008, 18, 411–418. [Google Scholar] [CrossRef]
- Oltmann, S.C.; Schneider, D.F.; Chen, H.; Sippel, R.S. All thyroid ultrasound evaluations are not equal: Sonographers specialized in thyroid cancer correctly label clinical N0 disease in well differentiated thyroid cancer. Ann. Surg. Oncol. 2015, 22, 422–428. [Google Scholar] [CrossRef]
- Machens, A.; Dralle, H. Biomarker-based risk stratification for previously untreated medullary thyroid cancer. J. Clin. Endocrinol. Metab. 2010, 95, 2655–2663. [Google Scholar] [CrossRef]
- Kim, H.; Kim, Y.N.; Kim, H.I.; Park, S.Y.; Choe, J.H.; Kim, J.H.; Kim, J.S.; Chung, J.H.; Kim, T.H.; Kim, S.W. Preoperative serum thyroglobulin predicts initial distant metastasis in patients with differentiated thyroid cancer. Sci. Rep. 2017, 7, 16955. [Google Scholar] [CrossRef]
- Durante, C.; Montesano, T.; Torlontano, M.; Attard, M.; Monzani, F.; Tumino, S.; Costante, G.; Meringolo, D.; Bruno, R.; Trulli, F.; et al. Papillary thyroid cancer: Time course of recurrences during postsurgery surveillance. J. Clin. Endocrinol. Metab. 2013, 98, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Olaleye, O.; Ekrikpo, U.; Moorthy, R.; Lyne, O.; Wiseberg, J.; Black, M.; Mitchell, D. Increasing incidence of differentiated thyroid cancer in South East England: 1987–2006. Eur. Arch. Otorhinolaryngol. 2011, 268, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Oh, C.M.; Cho, H.; Lee, J.Y.; Jung, K.W.; Jun, J.K.; Won, Y.J.; Kong, H.J.; Choi, K.S.; Lee, Y.J.; et al. Association between screening and the thyroid cancer “epidemic” in South Korea: Evidence from a nationwide study. BMJ 2016, 355, i5745. [Google Scholar] [CrossRef] [PubMed]
- Jeon, M.J.; Kim, H.K.; Kim, E.H.; Kim, E.S.; Yi, H.S.; Kim, T.Y.; Kang, H.C.; Shong, Y.K.; Kim, W.B.; Kim, B.H.; et al. Decreasing disease-specific mortality of differentiated thyroid cancer in Korea: A multicenter cohort study. Thyroid 2018, 28, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Bowles, E.J.A.; Williams, S.B.; Morrison, C.C. Screening for thyroid cancer: updated evidence report and systematic review for the US preventive services task force. JAMA 2017, 317, 1888–1903. [Google Scholar] [CrossRef]
- James, B.C.; Timsina, L.; Graham, R.; Angelos, P.; Haggstrom, D.A. Changes in total thyroidectomy versus thyroid lobectomy for papillary thyroid cancer during the past 15 years. Surgery 2019, 166, 41–47. [Google Scholar] [CrossRef]
- Kim, H.; Kim, T.H.; Choe, J.H.; Kim, J.H.; Kim, J.S.; Oh, Y.L.; Hahn, S.Y.; Shin, J.H.; Chi, S.A.; Jung, S.H.; et al. Patterns of initial recurrence in completely resected papillary thyroid carcinoma. Thyroid 2017, 27, 908–914. [Google Scholar] [CrossRef]
- Wada, N.; Duh, Q.Y.; Sugino, K.; Iwasaki, H.; Kameyama, K.; Mimura, T.; Ito, K.; Takami, H.; Takanashi, Y. Lymph node metastasis from 259 papillary thyroid microcarcinomas: Frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann. Surg. 2003, 237, 399–407. [Google Scholar] [CrossRef]
- Milhaud, G.; Tubiana, M.; Parmentier, C.; Coutris, G. Epithelioma of the thyroid secreting thyrocalcitonin. C. R. Acad. Hebd. Seances Acad. Sci. 1968, 266, 608–610. [Google Scholar]
- Patell, R.; Mikhael, A.; Tabet, M.; Bena, J.; Berber, E.; Nasr, C. Assessing the utility of preoperative serum thyroglobulin in differentiated thyroid cancer: A retrospective cohort study. Endocrine 2018, 61, 506–510. [Google Scholar] [CrossRef]
- Kim, M.; Jeon, M.J.; Kim, W.G.; Lee, J.J.; Ryu, J.S.; Cho, E.J.; Ko, D.H.; Lee, W.; Chun, S.; Min, W.K.; et al. Comparison of thyroglobulin measurements using three different immunoassay kits: A BRAMHS Tg-Plus RIA Kit, a BRAMHS hTg sensitive kryptor Kit, and a beckman coulter ACCESS immunoassay Kit. Endocrinol. Metab. (Seoul) 2016, 31, 462–468. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Data |
|---|---|
| Age at diagnosis (Years) | 46.43 ± 11.34 |
| Sex | |
| Female | 3135 (77.8%) |
| Male | 894 (22.2%) |
| Tumor histology | |
| Papillary thyroid carcinoma | 3979 (98.8%) |
| Follicular thyroid carcinoma | 50 (1.2%) |
| Tumor size (diameter; cm) | 1.06 ± 0.84 |
| Extrathyroidal extension | |
| None | 1685 (41.8%) |
| Microscopic | 1773 (44.0%) |
| Gross | 571 (14.2%) |
| Positive resection margin | |
| No | 3850 (95.6%) |
| Yes | 179 (4.4%) |
| Positive lymphatic invasion | |
| No | 3973 (98.6%) |
| Yes | 56 (1.4%) |
| Positive vascular invasion | |
| No | 3972 (98.6%) |
| Yes | 57 (1.4%) |
| Extent of LNM | |
| Central LNM | 1884 (46.8%) |
| Ipsilateral lateral LNM | 348 (8.6%) |
| Contralateral lateral LNM | 112 (2.8%) |
| Distant metastasis | |
| No | 3985 (98.9%) |
| Yes | 44 (1.1%) |
| Overall deaths | 15 (0.4%) |
| Disease-specific deaths | 8 (0.2%) |
| Characteristics | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| β ± SE | p-Value | β ± SE | p-Value | |
| Age at diagnosis (years) | −0.002 ± 0.004 | 0.628 | 0.010 ± 0.004 | 0.0009 |
| Sex (female) | 0.291 ±0.108 | 0.007 | 0.532 ± 0.101 | <0.001 |
| Tumor histology (FTC) | 2.021 ± 0.406 | <0.001 | 0.828 ± 0.400 | 0.039 |
| Tumor size | 0.830 ± 0.041 | <0.001 | 1.078 ± 0.056 | <0.001 |
| Positive lymphatic invasion | 1.678 ± 0.384 | <0.001 | 0.315 ± 0.360 | 0.382 |
| Positive blood vessel invasion | 1.800 ± 0.381 | <0.001 | −0.156 ± 0.372 | 0.674 |
| Number of LNM | 0.160 ± 0.010 | <0.001 | 0.091 ± 0.011 | <0.001 |
| Positive ETE | 0.595 ± 0.064 | <0.001 | −0.009 ± 0.065 | 0.889 |
| Positive resection margin | 1.534 ± 0.217 | <0.001 | 0.662 ± 0.206 | 0.001 |
| Presence of distant metastasis | 4.066 ± 0.439 | <0.001 | 0.577 ± 0.424 | 0.174 |
| Thyroglobulin Deciles | Preoperative Thyroglobulin Levels (ng/mL) | n | Primary Tumor Diameter (cm) | Number of LNM | Recurrence | DSD | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | n | % | n | % | |||
| 1 | 0.1–2.2 | 387 | 0.81 | 0.76; 0.86 | 1.42 | 1.13; 1.72 | 5 | 1.3 | 0 | 0 |
| 2 | 2.3–4.0 | 399 | 0.76 | 0.71; 0.80 | 1.16 | 0.93; 1.39 | 6 | 1.5 | 1 | 0.3 |
| 3 | 4.1–5.6 | 407 | 0.77 | 0.73; 0.81 | 1.33 | 1.03; 1.62 | 6 | 1.5 | 0 | 0 |
| 4 | 5.7–7.5 | 406 | 0.82 | 0.77; 0.87 | 1.34 | 1.08; 1.60 | 7 | 1.7 | 0 | 0 |
| 5 | 7.6–9.8 | 404 | 0.86 | 0.80; 0.92 | 1.67 | 1.37; 1.97 | 8 | 2 | 0 | 0 |
| 6 | 9.9–13.0 | 408 | 0.98 | 0.92; 1.04 | 2.02 | 1.66; 2.38 | 12 | 2.9 | 0 | 0 |
| 7 | 13.1–17.8 | 405 | 1 | 0.94; 1.06 | 2.06 | 1.72; 2.39 | 13 | 3.2 | 0 | 0 |
| 8 | 17.9–26.7 | 404 | 1.16 | 1.08; 1.24 | 2.25 | 1.88; 2.62 | 16 | 4 | 0 | 0 |
| 9 | 26.8–56.2 | 404 | 1.31 | 1.22; 1.40 | 3.32 | 2.83; 3.81 | 21 | 5.2 | 1 | 0.2 |
| 10 | 56.3–42680 | 405 | 2.07 | 1.93; 2.21 | 5.48 | 4.71; 6.25 | 44 | 10.9 | 6 | 1.5 |
| Total | 4029 | 1.06 | 1.03; 1.08 | 2.21 | 2.01; 2.34 | 138 | 3.4 | 8 | 0.2 | |
| Thyroglobulin Deciles | Preoperative Thyroglobulin Levels (ng/mL) | n | Central LNM | Ipsilateral Lateral LNM | Contralateral Lateral LNM | Distant Metastasis | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |||
| 1 | 0.1–2.2 | 387 | 135 | 34.9 | 21 | 5.4 | 5 | 1.3 | 0 | 0.0 |
| 2 | 2.3–4.0 | 399 | 145 | 36.3 | 22 | 5.5 | 1 | 0.3 | 1 | 0.3 |
| 3 | 4.1–5.6 | 407 | 149 | 36.6 | 22 | 5.4 | 5 | 1.2 | 0 | 0.0 |
| 4 | 5.7–7.5 | 406 | 156 | 38.4 | 16 | 3.9 | 4 | 1.0 | 1 | 0.2 |
| 5 | 7.6–9.8 | 404 | 160 | 39.6 | 33 | 8.2 | 4 | 1.0 | 2 | 0.5 |
| 6 | 9.9–13.0 | 408 | 165 | 40.4 | 31 | 7.6 | 5 | 1.2 | 0 | 0.0 |
| 7 | 13.1–17.8 | 405 | 144 | 35.6 | 36 | 8.9 | 13 | 3.2 | 1 | 0.2 |
| 8 | 17.9–26.7 | 404 | 157 | 38.9 | 41 | 10.1 | 11 | 2.7 | 1 | 0.2 |
| 9 | 26.8–56.2 | 404 | 158 | 39.1 | 53 | 13.1 | 20 | 5.0 | 3 | 0.7 |
| 10 | 56.3–42680 | 405 | 143 | 35.3 | 59 | 14.6 | 35 | 8.6 | 35 | 8.6 |
| Total | 4029 | 1512 | 37.5 | 334 | 8.3 | 103 | 2.6 | 44 | 1.1 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Park, S.Y.; Choe, J.-H.; Kim, J.S.; Hahn, S.Y.; Kim, S.W.; Chung, J.H.; Jung, J.; Kim, T.H. Preoperative Serum Thyroglobulin and Its Correlation with the Burden and Extent of Differentiated Thyroid Cancer. Cancers 2020, 12, 625. https://doi.org/10.3390/cancers12030625
Kim H, Park SY, Choe J-H, Kim JS, Hahn SY, Kim SW, Chung JH, Jung J, Kim TH. Preoperative Serum Thyroglobulin and Its Correlation with the Burden and Extent of Differentiated Thyroid Cancer. Cancers. 2020; 12(3):625. https://doi.org/10.3390/cancers12030625
Chicago/Turabian StyleKim, Hosu, So Young Park, Jun-Ho Choe, Jee Soo Kim, Soo Yeon Hahn, Sun Wook Kim, Jae Hoon Chung, Jaehoon Jung, and Tae Hyuk Kim. 2020. "Preoperative Serum Thyroglobulin and Its Correlation with the Burden and Extent of Differentiated Thyroid Cancer" Cancers 12, no. 3: 625. https://doi.org/10.3390/cancers12030625
APA StyleKim, H., Park, S. Y., Choe, J.-H., Kim, J. S., Hahn, S. Y., Kim, S. W., Chung, J. H., Jung, J., & Kim, T. H. (2020). Preoperative Serum Thyroglobulin and Its Correlation with the Burden and Extent of Differentiated Thyroid Cancer. Cancers, 12(3), 625. https://doi.org/10.3390/cancers12030625