Vincristine-Induced Peripheral Neuropathy in Pediatric Oncology: A Randomized Controlled Trial Comparing Push Injections with One-Hour Infusions (The VINCA Trial)

 ,
,  , , ,
, , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
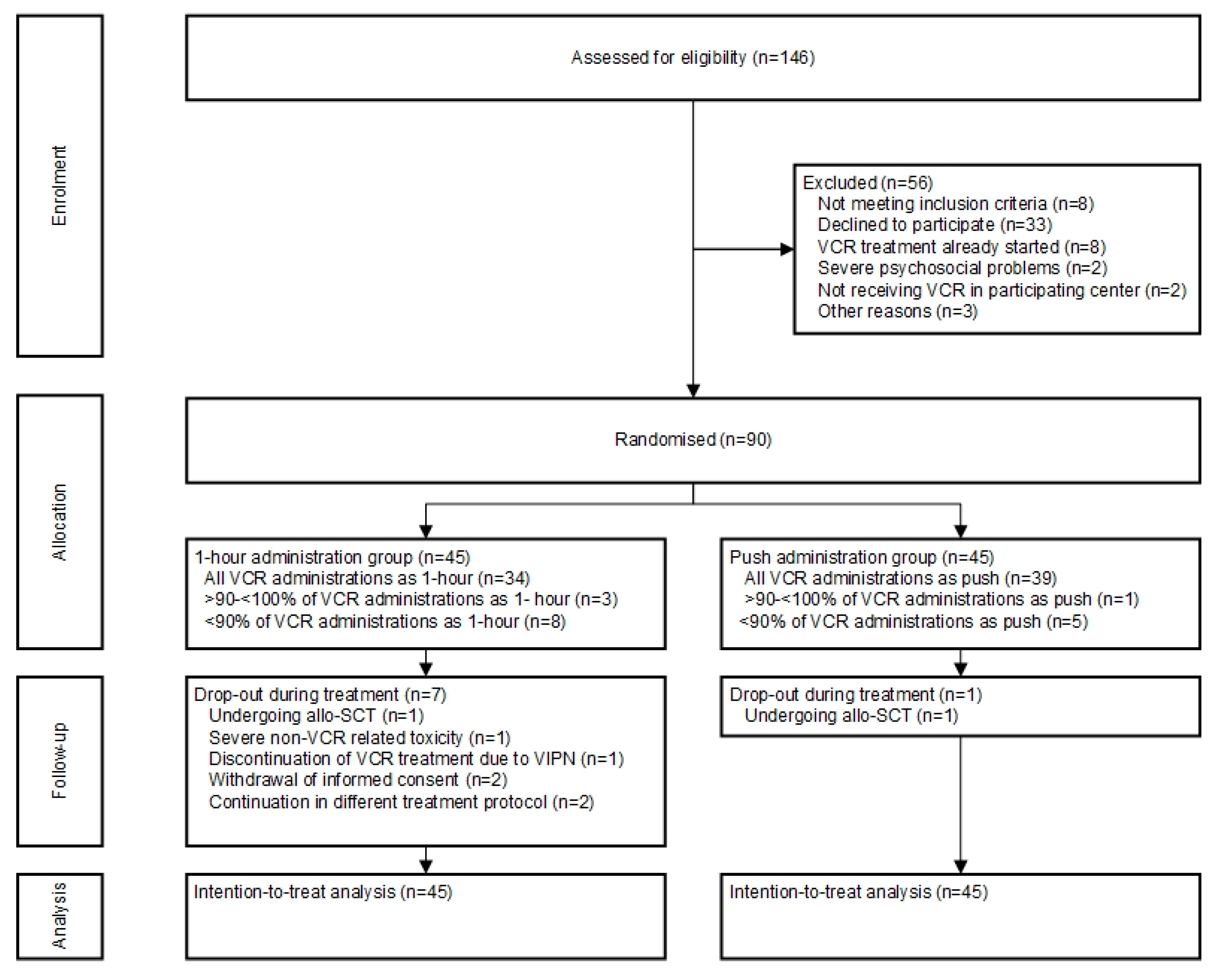
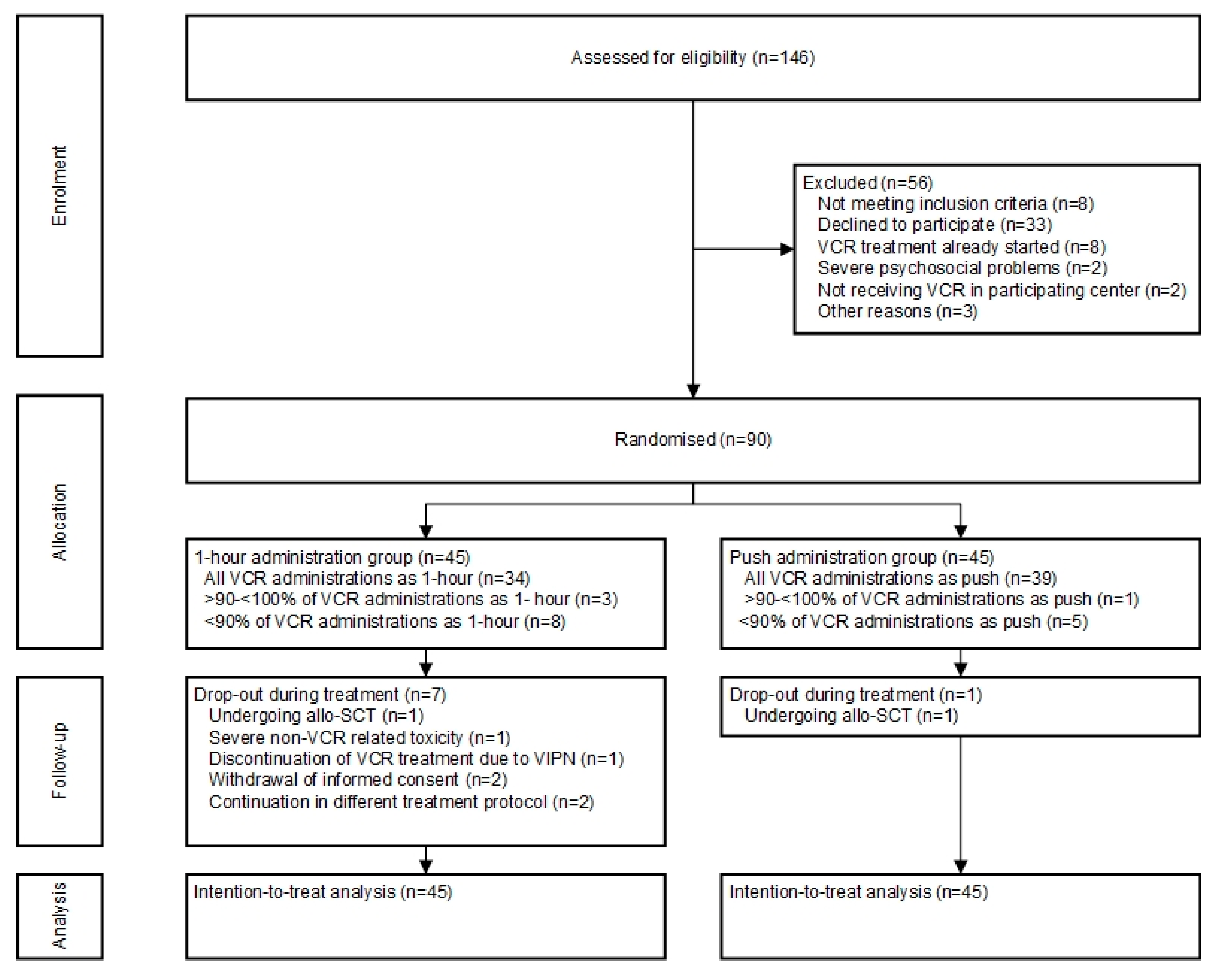
2.1. Participants
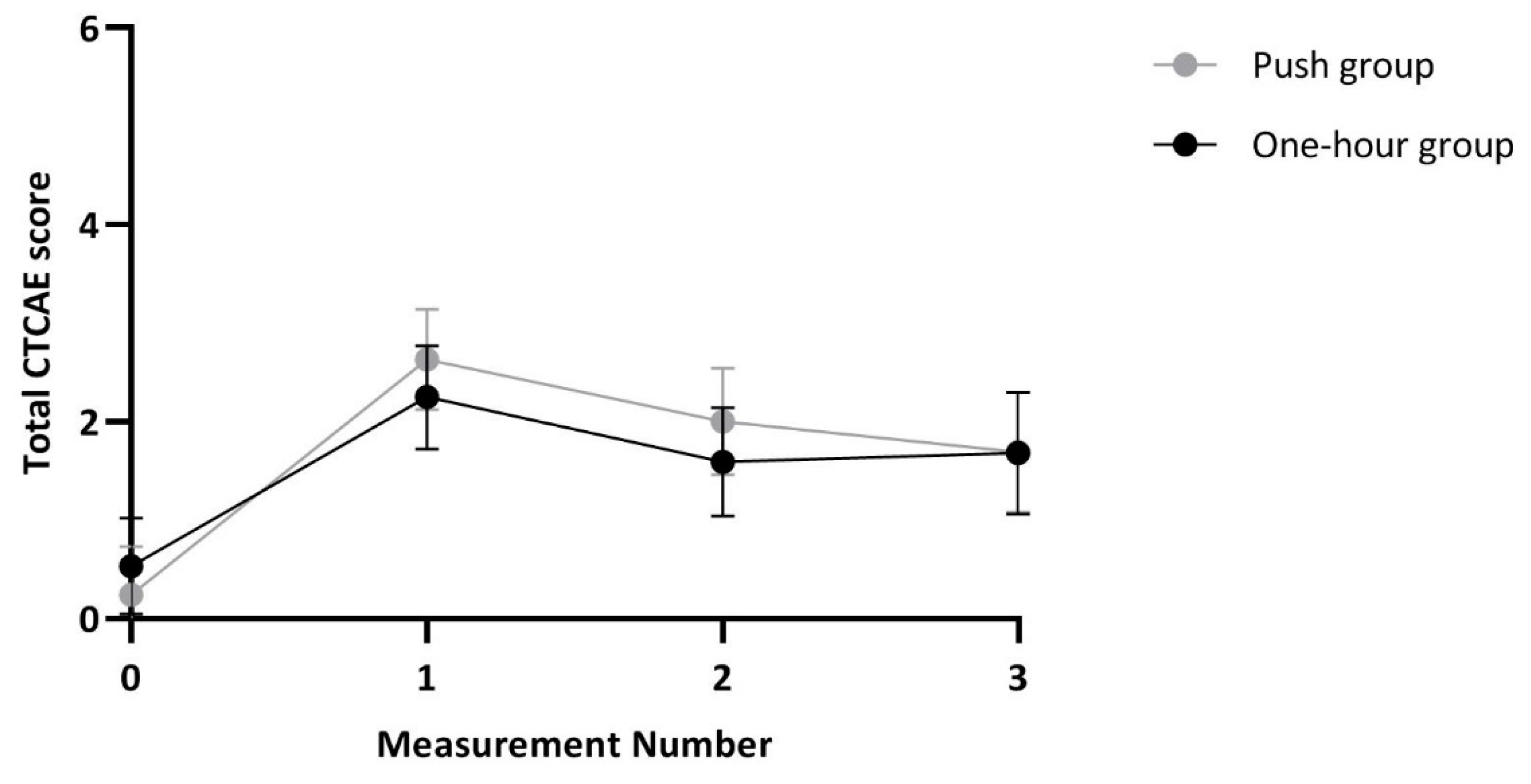
2.2. Primary Endpoints
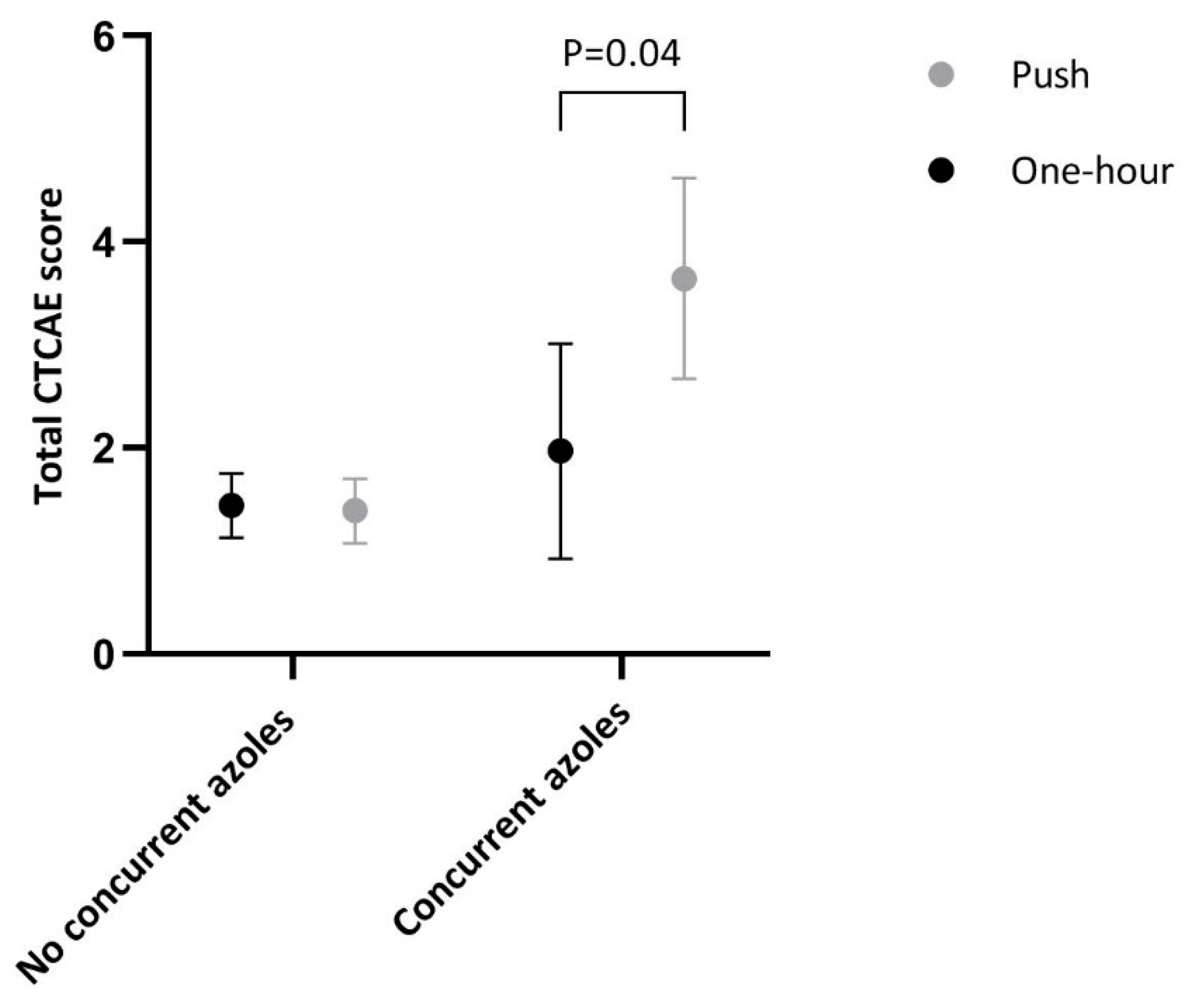
2.3. Secondary Endpoints
3. Discussion
4. Materials and Methods
4.1. Trial Design
4.2. Study Participants
4.3. Trial Regimen
4.4. Assessments of VIPN and Other Study Outcomes
4.5. Sample Size Calculation
4.6. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- van de Velde, M.E.; Kaspers, G.L.; Abbink, F.C.H.; Wilhelm, A.J.; Ket, J.C.F.; van den Berg, M.H. Vincristine-induced peripheral neuropathy in children with cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2017, 114, 114–130. [Google Scholar] [CrossRef] [PubMed]
- Gidding, C.E.; Kellie, S.J.; Kamps, W.A.; De Graaf, S.S. Vincristine revisited. Crit. Rev. Oncol. Hematol. 1999, 29, 267–287. [Google Scholar] [CrossRef]
- Coccia, P.F.; Altman, J.; Bhatia, S.; Borinstein, S.C.; Flynn, J.; George, S.; Goldsby, R.; Hayashi, R.; Huang, M.S.; Johnson, R.H.; et al. Adolescent and young adult oncology clinical practice guidelines in oncology. JNCCN J. Natl. Compr. Cancer Netw. 2012, 10, 1112–1150. [Google Scholar] [CrossRef] [PubMed]
- Stryckmans, P.A.; Lurie, P.M.; Manaster, J.; Vamecq, G. Mode of action of chemotherapy in vivo on human acute leukemia--II. Vincristine. Eur. J. Cancer 1973, 9, 613–620. [Google Scholar] [CrossRef]
- Dennison, J.B.; Jones, D.R.; Renbarger, J.L.; Hall, S.D. Effect of CYP3A5 expression on vincristine metabolism with human liver microsomes. J. Pharmacol. Exp. Ther. 2007, 321, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Anghelescu, D.L.; Faughnan, L.G.; Jeha, S.; Relling, M.V.; Hinds, P.S.; Sandlund, J.T.; Cheng, C.; Pei, D.; Hankins, G.; Pauley, J.L.; et al. Neuropathic pain during treatment for childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 2011, 57, 1147–1153. [Google Scholar] [CrossRef]
- Gutierrez-Camino, A.; Martin-Guerrero, I.; Lopez-Lopez, E.; Echebarria-Barona, A.; Zabalza, I.; Ruiz, I.; Guerra-Merino, I.; Garcia-Orad, A. Lack of association of the CEP72 rs924607 TT genotype with vincristine-related peripheral neuropathy during the early phase of pediatric acute lymphoblastic leukemia treatment in a Spanish population. Pharmacogenet. Genom. 2016, 26, 100–102. [Google Scholar] [CrossRef]
- Gilchrist, L.S.; Marais, L.; Tanner, L. Comparison of two chemotherapy-induced peripheral neuropathy measurement approaches in children. Supportive Care Cancer 2014, 22, 359–366. [Google Scholar] [CrossRef]
- Gutierrez-Gutierrez, G.; Sereno, M.; Miralles, A.; Casado-Saenz, E.; Gutierrez-Rivas, E. Chemotherapy-induced peripheral neuropathy: Clinical features, diagnosis, prevention and treatment strategies. Clin. Transl. Oncol 2010, 12, 81–91. [Google Scholar] [CrossRef]
- Gomber, S.; Dewan, P.; Chhonker, D. Vincristine induced neurotoxicity in cancer patients. Indian J. Pediatrics 2010, 77, 97–100. [Google Scholar] [CrossRef]
- Windebank, A.J.; Grisold, W. Chemotherapy-induced neuropathy. J. Peripher. Nerv. Syst 2008, 13, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Beijers, A.J.; Jongen, J.L.; Vreugdenhil, G. Chemotherapy-induced neurotoxicity: the value of neuroprotective strategies. Neth. J. Med. 2012, 70, 18–25. [Google Scholar] [PubMed]
- Rosca, L.; Robert-Boire, V.; Delisle, J.F.; Samson, Y.; Perreault, S. Carboplatin and vincristine neurotoxicity in the treatment of pediatric low-grade gliomas. Pediatr. Blood Cancer 2018, 65, e27351. [Google Scholar] [CrossRef] [PubMed]
- Diouf, B.; Crews, K.R.; Lew, G.; Pei, D.; Cheng, C.; Bao, J.; Zheng, J.J.; Yang, W.; Fan, Y.; Wheeler, H.E.; et al. Association of an inherited genetic variant with vincristine-related peripheral neuropathy in children with acute lymphoblastic leukemia. JAMA J. Am. Med Assoc. 2015, 313, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Egbelakin, A.; Ferguson, M.J.; MacGill, E.A.; Lehmann, A.S.; Topletz, A.R.; Quinney, S.K.; Li, L.; McCammack, K.C.; Hall, S.D.; Renbarger, J.L. Increased risk of vincristine neurotoxicity associated with low CYP3A5 expression genotype in children with acute lymphoblastic leukemia. Pediatric Blood Cancer 2011, 56, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Kishi, S.; Cheng, C.; French, D.; Pei, D.; Das, S.; Cook, E.H.; Hijiya, N.; Rizzari, C.; Rosner, G.L.; Frudakis, T.; et al. Ancestry and pharmacogenetics of antileukemic drug toxicity. Blood 2007, 109, 4151–4157. [Google Scholar] [CrossRef]
- Ceppi, F.; Langlois-Pelletier, C.; Gagné, V.; Rousseau, J.; Iolino, C.; Orenzo, S.D.; Evin, K.M.; Ijov, D.; Allan, S.E.; Ilverman, L.B.; et al. Polymorphisms of the vincristine pathway and response to treatment in children with childhood acute lymphoblastic leukemia. Pharmacogenomics 2014, 15, 1105–1116. [Google Scholar] [CrossRef]
- Abaji, R.; Ceppi, F.; Patel, S.; Gagne, V.; Xu, C.J.; Spinella, J.F.; Colombini, A.; Parasole, R.; Buldini, B.; Basso, G.; et al. Genetic risk factors for VIPN in childhood acute lymphoblastic leukemia patients identified using whole-exome sequencing. Pharmacogenomics 2018, 19, 1181–1193. [Google Scholar] [CrossRef]
- Lopez-Lopez, E.; Gutierrez-Camino, A.; Astigarraga, I.; Navajas, A.; Echebarria-Barona, A.; Garcia-Miguel, P.; Garcia de Andoin, N.; Lobo, C.; Guerra-Merino, I.; Martin-Guerrero, I.; et al. Vincristine pharmacokinetics pathway and neurotoxicity during early phases of treatment in pediatric acute lymphoblastic leukemia. Pharmacogenomics 2016, 17, 10. [Google Scholar] [CrossRef]
- Aplenc, R.; Glatfelter, W.; Han, P.; Rappaport, E.; La, M.; Cnaan, A.; Blackwood, M.A.; Lange, B.; Rebbeck, T. CYP3A genotypes and treatment response in paediatric acute lymphoblastic leukaemia. Br. J. Haematol. 2003, 122, 240–244. [Google Scholar] [CrossRef]
- Renbarger, J.L.; McCammack, K.C.; Rouse, C.E.; Hall, S.D. Effect of race on vincristine-associated neurotoxicity in pediatric acute lymphoblastic leukemia patients. Pediatr. Blood Cancer 2008, 50, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Van Schie, R.M.; Bruggemann, R.J.; Hoogerbrugge, P.M.; Te Loo, D.M. Effect of azole antifungal therapy on vincristine toxicity in childhood acute lymphoblastic leukaemia. J. Antimicrob. Chemother. 2011, 66, 1853–1856. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, B.; Henning, S.A.; Leung, J.; Falade-Nwulia, O.; Jarosinski, P.; Penzak, S.R.; Walsh, T.J. Adverse interactions between antifungal azoles and vincristine: review and analysis of cases. Mycoses 2012, 55, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Baxter, C.G.; Marshall, A.; Roberts, M.; Felton, T.W.; Denning, D.W. Peripheral neuropathy in patients on long-term triazole antifungal therapy. J. Antimicrob. Chemother. 2011, 66, 2136–2139. [Google Scholar] [CrossRef]
- Science, M.; Robinson, P.D.; MacDonald, T.; Rassekh, S.R.; Dupuis, L.L.; Sung, L. Guideline for primary antifungal prophylaxis for pediatric patients with cancer or hematopoietic stem cell transplant recipients. Pediatr. Blood Cancer 2014, 61, 393–400. [Google Scholar] [CrossRef]
- Kellie, S.J.; Koopmans, P.; Earl, J.; Nath, C.; Roebuck, D.; Uges, D.R.A.; De Graaf, S.S.N. Increasing the dosage of vincristine: A clinical and pharmacokinetic study of continuous-infusion vincristine in children with central nervous system tumors. Cancer 2004, 100, 2637–2643. [Google Scholar] [CrossRef]
- Pinkerton, C.R.; McDermott, B.; Philip, T.; Biron, P.; Ardiet, C.; Vandenberg, H.; Brunat-Mentigny, M. Continuous vincristine infusion as part of a high dose chemoradiotherapy regimen: Drug kinetics and toxicity. Cancer Chemother. Pharmacol. 1988, 22, 271–274. [Google Scholar] [CrossRef]
- Gidding, C.E.; Fock, J.M.; Begeer, J.H.; Koopmans, P.; Meeuwsen-de Boer, G.J.; Kamps, W.A.; Uges, D.R.A.; De Graaf, S.S.N. Vincristine disposition and neurotoxicity in children. In Proceedings of the Annual Meeting-American Society of Clinical Oncology, Los Angeles, CA, USA, 16–19 May 1998. Abstract N22-2068-ASCO 1998. 16-5-1998. [Google Scholar]
- DCOG Protocol ALL-11 (2013): Treatment Study Protocol of the Dutch Childhood Oncology Group for Children and Adolescents (1–19 year) with Newly Diagnosed Acute Lymphoblastic Leukemia. Version 4.0. Available online: https://www.skion.nl/workspace/uploads/Onderzoeksprotocol-ALL11-version-4-3-september-2014.pdf (accessed on 5 October 2020).
- Varedi, M.; Lu, L.; Howell, C.R.; Partin, R.E.; Hudson, M.M.; Pui, C.H.; Krull, K.R.; Robison, L.L.; Ness, K.K.; McKenna, R.F. Peripheral Neuropathy, Sensory Processing, and Balance in Survivors of Acute Lymphoblastic Leukemia. J. Clin. Oncol. 2018, 36, 2315–2322. [Google Scholar] [CrossRef]
- Gilchrist, L.S.; Tanner, L. The pediatric-modified total neuropathy score: A reliable and valid measure of chemotherapy-induced peripheral neuropathy in children with non-CNS cancers. Supportive Care Cancer 2013, 21, 847–856. [Google Scholar] [CrossRef]
- Smolik, S.; Arland, L.; Hensley, M.A.; Schissel, D.; Shepperd, B.; Thomas, K.; Rodgers, C. Assessment Tools for Peripheral Neuropathy in Pediatric Oncology: A Systematic Review From the Children’s Oncology Group. J. Pediatr. Oncol. Nurs. 2018, 35, 267–275. [Google Scholar] [CrossRef]
- Leverger, G.; Timsit, J.F.; Milpied, N.; Gachot, B. Use of Micafungin for the Prevention and Treatment of Invasive Fungal Infections in Everyday Pediatric Care in France: Results of the MYRIADE Study. Pediatr. Infect Dis. J. 2019, 38, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Bochennek, K.; Balan, A.; Muller-Scholden, L.; Becker, M.; Farowski, F.; Muller, C.; Groll, A.H.; Lehrnbecher, T. Micafungin twice weekly as antifungal prophylaxis in paediatric patients at high risk for invasive fungal disease. J. Antimicrob Chemother. 2015, 70, 1527–1530. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Lin, J.C.; Ho, C.L.; Sun, M.; Yen, W.T.; Lin, C. Efficacy and safety of micafungin versus extensive azoles in the prevention and treatment of invasive fungal infections for neutropenia patients with hematological malignancies: A meta-analysis of randomized controlled trials. PLoS ONE 2017, 12, e0180050. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.T.; Zaoutis, T.; Dvorak, C.C.; Nieder, M.; Zerr, D.; Wingard, J.R.; Callahan, C.; Villaluna, D.; Chen, L.; Dang, H.; et al. Effect of Caspofungin vs Fluconazole Prophylaxis on Invasive Fungal Disease among Children and Young Adults with Acute Myeloid Leukemia: A Randomized Clinical Trial. JAMA 2019, 322, 1673–1681. [Google Scholar] [CrossRef]
- Papachristou, S.; Iosifidis, E.; Roilides, E. Invasive Aspergillosis in Pediatric Leukemia Patients: Prevention and Treatment. J. Fungi. 2019, 5, 14. [Google Scholar] [CrossRef]
- Saad, A.H.; DePestel, D.D.; Carver, P.L. Factors influencing the magnitude and clinical significance of drug interactions between azole antifungals and select immunosuppressants. Pharmacotherapy 2006, 26, 1730–1744. [Google Scholar] [CrossRef]
- Pana, Z.D.; Roilides, E. Risk of azole-enhanced vincristine neurotoxicity in pediatric patients with hematological malignancies: old problem—New dilemma. Pediatr. Blood Cancer 2011, 57, 30–35. [Google Scholar] [CrossRef]
- The EuroNet-PHL-C2 Protocol (2016) Second International Inter-Group Study for Classical Hodgkin’s Lymphoma in Children and Adolescents. Version 3.0. Available online: https://clinicaltrials.gov/ct2/show/NCT02684708 (accessed on 5 October 2020).
- Lavoie Smith, E.M.; Li, L.; Hutchinson, R.J.; Ho, R.; Burnette, W.B.; Wells, E.; Bridges, C.; Renbarger, J. Measuring vincristine-induced peripheral neuropathy in children with acute lymphoblastic leukemia. Cancer Nurs. 2013, 36, E49–E60. [Google Scholar] [CrossRef]
- Van de Velde, M.E.; Panetta, J.C.; Wilhelm, A.J.; van den Berg, M.H.; van der Sluis, I.M.; van den Bos, C.; Abbink, F.C.H.; van den Heuvel-Eibrink, M.M.; Segers, H.; Chantrain, C.; et al. Population Pharmacokinetics of Vincristine Related to Infusion Duration and Peripheral Neuropathy in Pediatric Oncology Patients. Cancers 2020, 12, 1789. [Google Scholar] [CrossRef]
- EsPhALL (2015): An Open-Label Study to Evaluate the Safety and Efficacy of IMATINIB with Chemotherapy in Pediatric Patients with Ph+/BCR-ABL+ Acute Lymphoblastic Leukemia (Ph+ALL). Available online: https://www.skion.nl/workspace/uploads/EsPhALL_Amendment-2_01102015_final_1.pdf (accessed on 5 October 2020).
- EORTC-58081-CLG Translational Research-Observational Study for Identification of New Possible Prognostic Factors and Future Therapeutic Targets in Children with Acute Lymphoblastic Leukaemia (ALL). Available online: https://www.eortc.org/research_field/clinical-detail/58081/ (accessed on 5 October 2020).
- The EuroNet-PHL-C1 Protocol (2012) First International Inter-Group Study for Classical Hodgkin’s Lymphoma in Children and Adolescents. Available online: https://www.skion.nl/workspace/uploads/euronet-phl-c1_workingcopy_inkl_amendm06_mw_2012-11-14_0.pdf (accessed on 5 October 2020).
- SIOP Wilms (2001): Chemotherapy Before and After Surgery in Treating Children With Wilm’s tumor. Available online: https://clinicaltrials.gov/ct2/show/NCT00047138 (accessed on 5 October 2020).
- The EpSSG Protocol (2012) A Protocol for Non Metastatic Rhabdomyosarcoma. Version 1.3. Available online: https://www.skion.nl/workspace/uploads/Protocol-EpSSG-RMS-2005-1-3-May-2012_1.pdf (accessed on 5 October 2020).
- SIOP LGG 2004: Cooperative Multicenter Study for Children and Adolescents with Low Grade Glioma. Available online: https://www.kinderkrebsinfo.de/sites/kinderkrebsinfo/content/e1676/e9032/e68518/e5400/download7688/Master-ProtokollGPOHVersionI,April2004_Druck_KLEIN_ger.pdf (accessed on 5 October 2020).
- ACNS0331 (2004): A Study Evaluating Limited Target Volume Boost Irradiation and Reduced Dose Craniospinal Radiotherapy (18.00 Gy) and Chemotherapy in Children with Newly Diagnosed Standard Risk Medulloblastoma: A Phase III Double Randomized Trial. Available online: https://www.childrensoncologygroup.org/acns0331 (accessed on 5 October 2020).
- ACNS0332 (2007): Efficacy of Carboplatin Administered Concomitantly with Radiation and Isotretinoin as a Pro-Apoptotic Agent in Other than Average Risk Medulloblastoma/PNET Patients. Available online: https://clinicaltrials.gov/ProvidedDocs/27/NCT00392327/Prot_SAP_000.pdf (accessed on 5 October 2020).
- National Institutes of Health, N.C.I. (2010) Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03. Available online: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf (accessed on 5 October 2020).
- Schouten, S.M.; van de Velde, M.E.; Kaspers, G.J.L.; Mokkink, L.B.; van der Sluis, I.M.; van den Bos, C.; Hartman, A.; Abbink, F.C.H.; van den Berg, M.H. Measuring vincristine-induced peripheral neuropathy in children with cancer: validation of the Dutch pediatric-modified Total Neuropathy Score. Support Care Cancer 2019. [Google Scholar] [CrossRef]
- Purser, M.J.; Johnston, D.L.; McMillan, H.J. Chemotherapy-induced peripheral neuropathy among paediatric oncology patients. Can. J. Neurol. Sci. 2014, 41, 442–447. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| One-Hour Administration Group (n = 45) | Push Administration Group (n = 45) | |
|---|---|---|
| Sex | ||
| Male | 26 (58) | 24 (53) |
| Female | 19 (42) | 21 (47) |
| Age, years (mean(SD)) | 9.06 (5.11) | 9.29 (5.25) |
| Age ≥ 5 years and included for ped-mTNS assessment | 32 (71) | 34 (76) |
| Disease | ||
| Acute lymphoblastic leukemia | 29 (64) | 29 (64) |
| Hodgkin lymphoma | 7 (16) | 11 (24) |
| Nephroblastoma | 6 (13) | 2 (4) |
| Medulloblastoma | 1 (2) | 1 (2) |
| Rhabdomyosarcoma | 2 (4) | 0 (0) |
| Low-grade glioma | 0 (0) | 2 (4) |
| Ancestry a | ||
| Europe | 36 (80) | 37 (82) |
| Eastern Asia | 1 (2) | 0 (0) |
| Latin-America (including Caribbean) | 1 (2) | 2 (4) |
| Middle-East (including Northern Africa) | 3 (7) | 3 (7) |
| Sub-Saharan Africa | 1 (2) | 0 (0) |
| Combination | 2 (4) | 3 (7) |
| Missing | 1 (2) | 0 (0) |
| No. (%) of patients needing VCR dose reductions or omissions | 1 (3) | 0 (0) |
| No. (%) of patients using analgesics for neuropathic pain | 9 (20) | 11 (24) |
| Relapse (No. (%)) | 2 (4) | 1 (2) |
| Death (No. (%)) | 3 (7) | 1 (2) |
| One-Hour (n = 45) n (%) * | Push (n = 45) n (%) * | p Value | |
|---|---|---|---|
| VIPN based on CTCAE | 21 (46.7) | 23 (51.1) | 0.67 |
| Severe VIPN based on CTCAE | 3 (6.7) | 6 (13.3) | 0.49 |
| VIPN based on ped-mTNS | 27 (84.4) ** | 28 (82.4) ** | 0.83 |
| VIPN pain medication | 9 (20.0) | 11 (24.4) | 0.61 |
| VIPN based on CTCAE item constipation | 3 (6.7) | 8 (17.8) | 0.20 |
| VIPN based on CTCAE item peripheral sensory neuropathy | 5 (11.1) | 6 (13.3) | 0.75 |
| VIPN based on CTCAE item peripheral motor neuropathy | 17 (37.8) | 15 (33.3) | 0.66 |
| VIPN based on CTCAE item neuralgia | 6 (13.3) | 12 (26.7) | 0.11 |
| CTCAE score (median [IQR]) | 2.00 [1.00–3.00] | 1.50 [0.00–3.00] | 0.43 |
| ped-mTNS score (median [IQR]) | 6.00 [3.75–10.00] ** | 5.50 [2.00–9.00] ** | 0.19 |
| VIPN outcomes without concurrent azole antifungals | One-hour (n = 35) | Push (n = 36) | |
| CTCAE score without concurrent azole treatment (median [IQR]) | 2.00 [1.00–2.75] | 1.00 [0.00–3.00] | 0.20 |
| ped-mTNS score without concurrent azole treatment (median [IQR]) | 5.50 [3.25–9.00] *** | 5.00 [2.00–8.00] *** | 0.09 |
| VIPN outcomes with concurrent azole antifungals | One-hour (n = 10) | Push (n = 9) | |
| CTCAE score with concurrent azole treatment (median [IQR]) | 2.00 [1.00–3.00] | 3.00 [1.00–6.00] | 0.21 |
| ped-mTNS score with concurrent azole treatment (median [IQR]) | 8.50 [3.75–11.50] **** | 10.00 [7.00–13.00] **** | 0.39 |
| Total Group (n = 90) | Subgroup of Participants without Concurrent Azole Treatment (n = 71) | Subgroup of Participants with Concurrent Azole Treatment (n = 19) | ||||
|---|---|---|---|---|---|---|
| β/OR (95% CI) | p-Value | β/OR (95% CI) | p-Value | β/OR (95% CI) | p-Value | |
| CTCAE a Total score during treatment | −0.29 (−0.89 to 0.31) | 0.34 | −0.12 (−0.73 to 0.49) | 0.69 | −1.58 (−3.11 to −0.05) | 0.04 |
| Ped-mTNS a Total score during treatment | −0.25 (−1.95 to 1.45) | 0.77 | 0.03 (−1.78 to 1.84) | 0.97 | −1.80 (−5.33 to 1.72) | 0.31 |
| Participants with VIPN a,b Based on CTCAE Based on ped-mTNS Based on analgesics use | 1.21 (0.43 to 1.46) 1.12 (0.58 to 2.16) 0.76 (0.30 to 1.94) | 0.45 0.74 0.57 | 0.93 (0.49 to 1.79) 1.33 (0.63 to 2.80) 0.67 (0.21 to 2.18) | 0.84 0.46 0.51 | 0.26 (0.04 to 1.67) 0.22 (0.02 to 2.76) 0.86 (0.17 to 4.43) | 0.16 0.24 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van de Velde, M.E.; Kaspers, G.J.L.; Abbink, F.C.H.; Twisk, J.W.R.; van der Sluis, I.M.; van den Bos, C.; van den Heuvel-Eibrink, M.M.; Segers, H.; Chantrain, C.; van der Werff ten Bosch, J.; et al. Vincristine-Induced Peripheral Neuropathy in Pediatric Oncology: A Randomized Controlled Trial Comparing Push Injections with One-Hour Infusions (The VINCA Trial). Cancers 2020, 12, 3745. https://doi.org/10.3390/cancers12123745
van de Velde ME, Kaspers GJL, Abbink FCH, Twisk JWR, van der Sluis IM, van den Bos C, van den Heuvel-Eibrink MM, Segers H, Chantrain C, van der Werff ten Bosch J, et al. Vincristine-Induced Peripheral Neuropathy in Pediatric Oncology: A Randomized Controlled Trial Comparing Push Injections with One-Hour Infusions (The VINCA Trial). Cancers. 2020; 12(12):3745. https://doi.org/10.3390/cancers12123745
Chicago/Turabian Stylevan de Velde, Mirjam Esther, Gertjan J. L. Kaspers, Floor C. H. Abbink, Jos W. R. Twisk, Inge M. van der Sluis, Cor van den Bos, Marry M. van den Heuvel-Eibrink, Heidi Segers, Christophe Chantrain, Jutte van der Werff ten Bosch, and et al. 2020. "Vincristine-Induced Peripheral Neuropathy in Pediatric Oncology: A Randomized Controlled Trial Comparing Push Injections with One-Hour Infusions (The VINCA Trial)" Cancers 12, no. 12: 3745. https://doi.org/10.3390/cancers12123745
APA Stylevan de Velde, M. E., Kaspers, G. J. L., Abbink, F. C. H., Twisk, J. W. R., van der Sluis, I. M., van den Bos, C., van den Heuvel-Eibrink, M. M., Segers, H., Chantrain, C., van der Werff ten Bosch, J., Willems, L., & van den Berg, M. H. (2020). Vincristine-Induced Peripheral Neuropathy in Pediatric Oncology: A Randomized Controlled Trial Comparing Push Injections with One-Hour Infusions (The VINCA Trial). Cancers, 12(12), 3745. https://doi.org/10.3390/cancers12123745