Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients

 ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Preoperative Evaluation
2.2. Surgical Treatment and Pathologic Examination
2.3. Postoperative Management and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Preoperative Data
3.2. Surgical Procedure
3.3. Pathological Examination
3.4. Follow-Up
3.5. Statistical Analysis
3.5.1. Univariate Analysis
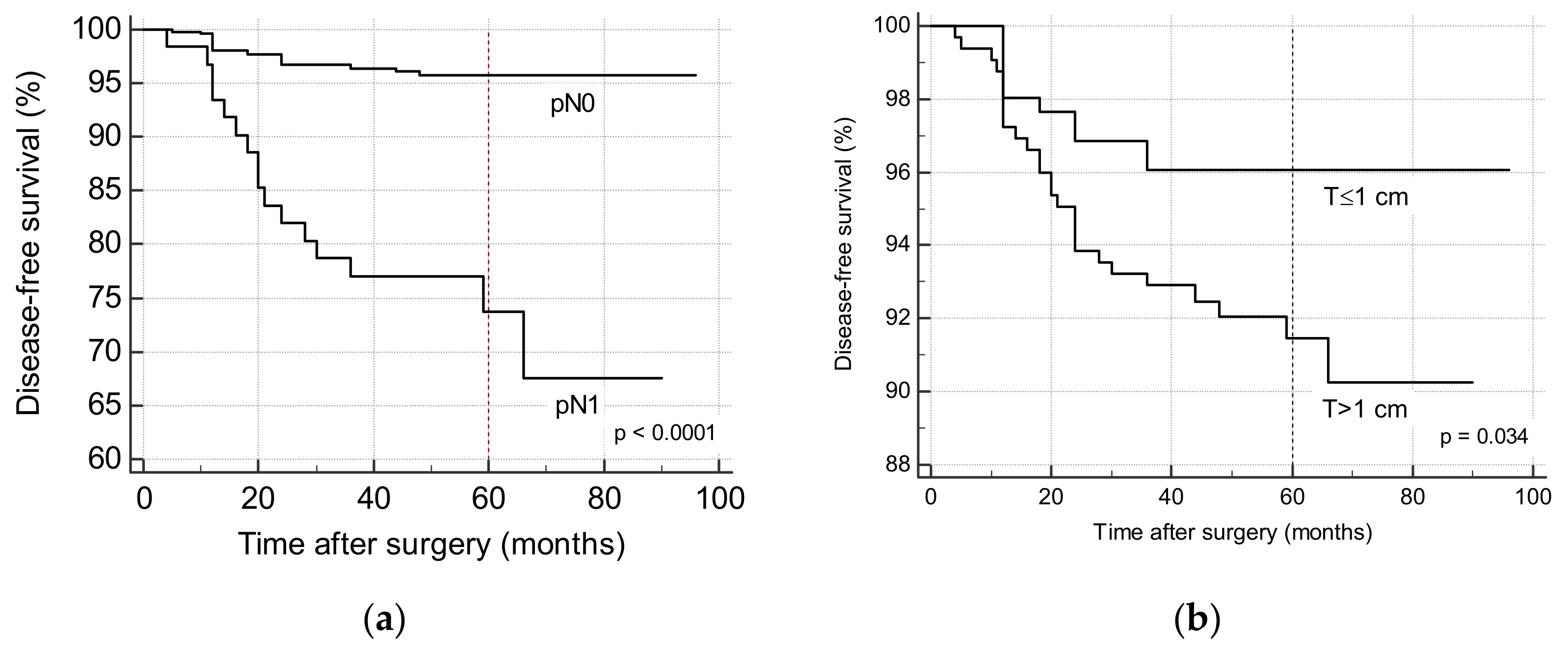
3.5.2. Multivariate and Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA. Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Plzák, J.; Astl, J.; Psychogios, G.; Zenk, J.; Laštůvka, P.; Betka, J. Current treatment strategies for papillary thyroid microcarcinoma. HNO 2013, 61, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Schilling, T.; Büchler, M.W. Thyroid carcinoma. Curr. Opin. Oncol. 2006, 18, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Markovina, S.; Grigsby, P.W.; Schwarz, J.K.; DeWees, T.; Moley, J.F.; Siegel, B.A.; Perkins, S.M. Treatment Approach, Surveillance, and Outcome of Well-Differentiated Thyroid Cancer in Childhood and Adolescence. Thyroid 2014, 24, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Barczyński, M.; Konturek, A.; Stopa, M.; Nowak, W. Prophylactic central neck dissection for papillary thyroid cancer. BJS 2013, 100, 410–418. [Google Scholar] [CrossRef]
- Calò, P.G.; Conzo, G.; Raffaelli, M.; Medas, F.; Gambardella, C.; De Crea, C.; Gordini, L.; Patrone, R.; Sessa, L.; Erdas, E.; et al. Total thyroidectomy alone versus ipsilateral versus bilateral prophylactic central neck dissection in clinically node-negative differentiated thyroid carcinoma. A retrospective multicenter study. Eur. J. Surg. Oncol. 2017, 43, 126–132. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef]
- Edge, S.B. AJCC Cancer Staging Manual, 7th ed.; American Joint Committee on Cancer, Ed.; Springer: New York, NY, USA, 2010; ISBN 978-0-387-88440-0. [Google Scholar]
- Hay, I.D.; Grant, C.S.; Taylor, W.F.; McConahey, W.M. Ipsilateral lobectomy versus bilateral lobar resection in papillary thyroid carcinoma: A retrospective analysis of surgical outcome using a novel prognostic scoring system. Surgery 1987, 102, 1088–1095. [Google Scholar] [PubMed]
- Cady, B.; Rossi, R. An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery 1988, 104, 947–953. [Google Scholar] [PubMed]
- Hay, I.D.; Bergstralh, E.J.; Goellner, J.R.; Ebersold, J.R.; Grant, C.S. Predicting outcome in papillary thyroid carcinoma: Development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1993, 114, 1050–1057. [Google Scholar] [PubMed]
- Shaha, A.R.; Loree, T.R.; Shah, J.P. Prognostic factors and risk group analysis in follicular carcinoma of the thyroid. Surgery 1995, 118, 1131–1138. [Google Scholar] [CrossRef]
- Sherman, S.I.; Brierley, J.D.; Sperling, M.; Ain, K.B.; Bigos, S.T.; Cooper, D.S.; Haugen, B.R.; Ho, M.; Klein, I.; Ladenson, P.W.; et al. Prospective multicenter study of thyroiscarcinoma treatment: Initial analysis of staging and outcome. National Thyroid Cancer Treatment Cooperative Study Registry Group. Cancer 1998, 83, 1012–1021. [Google Scholar] [PubMed]
- Tuttle, R.M.; Tala, H.; Shah, J.; Leboeuf, R.; Ghossein, R.; Gonen, M.; Brokhin, M.; Omry, G.; Fagin, J.A.; Shaha, A. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: Using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid 2010, 20, 1341–1349. [Google Scholar]
- Bates, M.F.; Lamas, M.R.; Randle, R.W.; Long, K.L.; Pitt, S.C.; Schneider, D.F.; Sippel, R.S. Back so soon? Is early recurrence of papillary thyroid cancer really just persistent disease? Surgery 2018, 163, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Kudo, T.; Kobayashi, K.; Miya, A.; Ichihara, K.; Miyauchi, A. Prognostic factors for recurrence of papillary thyroid carcinoma in the lymph nodes, lung, and bone: Analysis of 5768 patients with average 10-year follow-up. World J. Surg. 2012, 36, 1274–1278. [Google Scholar] [CrossRef]
- Randolph, G.W.; Duh, Q.-Y.; Heller, K.S.; LiVolsi, V.A.; Mandel, S.J.; Steward, D.L.; Tufano, R.P.; Tuttle, R.M. American Thyroid Association Surgical Affairs Committee’s Taskforce on Thyroid Cancer Nodal Surgery The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid 2012, 22, 1144–1152. [Google Scholar]
- Kim, Y.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Risk Factors for Lateral Neck Recurrence of N0/N1a Papillary Thyroid Cancer. Ann. Surg. Oncol. 2017, 24, 3609–3616. [Google Scholar] [CrossRef]
- Lee, Y.C.; Na, S.Y.; Park, G.C.; Han, J.H.; Kim, S.W.; Eun, Y.G. Occult lymph node metastasis and risk of regional recurrence in papillary thyroid cancer after bilateral prophylactic central neck dissection: A multi-institutional study. Surgery 2017, 161, 465–471. [Google Scholar] [CrossRef]
- Raffaelli, M.; De Crea, C.; Sessa, L.; Tempera, S.E.; Belluzzi, A.; Lombardi, C.P.; Bellantone, R. Risk factors for local recurrence following lateral neck dissection for papillary thyroid carcinoma. Endocrine 2019, 63, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Conzo, G.; Calò, P.G.; Sinisi, A.A.; De Bellis, A.; Pasquali, D.; Iorio, S.; Tartaglia, E.; Mauriello, C.; Gambardella, C.; Cavallo, F.; et al. Impact of prophylactic central compartment neck dissection on locoregional recurrence of differentiated thyroid cancer in clinically node-negative patients: A retrospective study of a large clinical series. Surgery 2014, 155, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Barczyński, M.; Konturek, A.; Stopa, M.; Nowak, W. Nodal recurrence in the lateral neck after total thyroidectomy with prophylactic central neck dissection for papillary thyroid cancer. Langenbeck’s Arch. Surg. 2014, 399, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Uruno, T.; Nakano, K.; Takamura, Y.; Miya, A.; Kobayashi, K.; Yokozawa, T.; Matsuzuka, F.; Kuma, S.; Kuma, K.; et al. An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid 2003, 13, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Miyauchi, A.; Kudo, T.; Ito, Y.; Oda, H.; Sasai, H.; Higashiyama, T.; Fukushima, M.; Masuoka, H.; Kihara, M.; Miya, A. Estimation of the lifetime probability of disease progression of papillary microcarcinoma of the thyroid during active surveillance. Surgery 2018, 163, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, T.A.; Hrafnkelsson, J.; Olafsdottir, E.J.; Jonasson, J.G. Tall cell variant of papillary thyroid carcinoma: A population-based study in Iceland. Thyroid 2015, 25, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Ganly, I.; Ibrahimpasic, T.; Rivera, M.; Nixon, I.; Palmer, F.; Patel, S.G.; Tuttle, R.M.; Shah, J.P.; Ghossein, R. Prognostic implications of papillary thyroid carcinoma with tall-cell features. Thyroid 2014, 24, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.; Virk, R.K.; Hui, P.; Prasad, A.; Westra, W.H.; Tallini, G.; Adeniran, A.J.; Udelsman, R.; Sasaki, C.T.; Roman, S.A.; et al. Tall cell variant of papillary thyroid microcarcinoma: Clinicopathologic features with BRAF (V600E) mutational analysis. Thyroid 2013, 23, 1525–1531. [Google Scholar] [CrossRef]
- Michels, J.J.; Jacques, M.; Henry-Amar, M.; Bardet, S. Prevalence and prognostic significance of tall cell variant of papillary thyroid carcinoma. Hum. Pathol. 2007, 38, 212–219. [Google Scholar] [CrossRef]
- Ghossein, R.A.; Leboeuf, R.; Patel, K.N.; Rivera, M.; Katabi, N.; Carlson, D.L.; Tallini, G.; Shaha, A.; Singh, B.; Tuttle, R.M. Tall cell variant of papillary thyroid carcinoma without extrathyroid extension: Biologic behavior and clinical implications. Thyroid 2007, 17, 655–661. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, W.; Liu, C.; Li, J. Tall cell variant of papillary thyroid carcinoma: Current evidence on clinicopathologic features and molecular biology. Oncotarget 2016, 7, 40792–40799. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.; Ghossein, R.A.; Schoder, H.; Gomez, D.; Larson, S.M.; Tuttle, R.M. Histopathologic characterization of radioactive iodine-refractory fluorodeoxyglucose-positron emission tomography-positive thyroid carcinoma. Cancer 2008, 113, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Singh, B.; Tallini, G.; Carlson, D.L.; Katabi, N.; Shaha, A.; Tuttle, R.M.; Ghossein, R.A. Follicular variant of papillary thyroid carcinoma: A clinicopathologic study of a problematic entity. Cancer 2006, 107, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Vivero, M.; Kraft, S.; Barletta, J.A. Risk stratification of follicular variant of papillary thyroid carcinoma. Thyroid 2013, 23, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Baloch, Z.W.; Shafique, K.; Flannagan, M.; Livolsi, V.A. Encapsulated classic and follicular variants of papillary thyroid carcinoma: Comparative clinicopathologic study. Endocr. Pract. 2010, 16, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E.; Seethala, R.R.; Tallini, G.; Baloch, Z.W.; Basolo, F.; Thompson, L.D.R.; Barletta, J.A.; Wenig, B.M.; Ghuzlan, A.A.; Kakudo, K.; et al. Nomenclature Revision for Encapsulated Follicular Variant of Papillary Thyroid Carcinoma. JAMA Oncol. 2016, 2, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs; IARC Publications: Lyon, France, 2017; ISBN 978-92-832-4493-6. [Google Scholar]
- Haigh, P.I.; Urbach, D.R. The treatment and prognosis of Hürthle cell follicular thyroid carcinoma compared with its non-Hürthle cell counterpart. Surgery 2005, 138, 1152–1158. [Google Scholar] [CrossRef]
- Sugino, K.; Kameyama, K.; Ito, K.; Nagahama, M.; Kitagawa, W.; Shibuya, H.; Ohkuwa, K.; Uruno, T.; Akaishi, J.; Suzuki, A.; et al. Does Hürthle cell carcinoma of the thyroid have a poorer prognosis than ordinary follicular thyroid carcinoma? Ann. Surg. Oncol. 2013, 20, 2944–2950. [Google Scholar] [CrossRef]
- Kim, H.J.; Sohn, S.Y.; Jang, H.W.; Kim, S.W.; Chung, J.H. Multifocality, but not bilaterality, is a predictor of disease recurrence/persistence of papillary thyroid carcinoma. World J. Surg. 2013, 37, 376–384. [Google Scholar] [CrossRef]
- Lin, J.-D.; Chao, T.-C.; Hsueh, C.; Kuo, S.-F. High recurrent rate of multicentric papillary thyroid carcinoma. Ann. Surg. Oncol. 2009, 16, 2609–2616. [Google Scholar] [CrossRef]
- Wang, W.; Su, X.; He, K.; Wang, Y.; Wang, H.; Wang, H.; Zhao, Y.; Zhao, W.; Zarnegar, R.; Fahey, T.J.; et al. Comparison of the clinicopathologic features and prognosis of bilateral versus unilateral multifocal papillary thyroid cancer: An updated study with more than 2000 consecutive patients. Cancer 2016, 122, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yu, X.; Shen, X.; Zhu, G.; Huang, Y.; Liu, R.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; et al. The Prognostic Value of Tumor Multifocality in Clinical Outcomes of Papillary Thyroid Cancer. J. Clin. Endocrinol. Metab. 2017, 102, 3241–3250. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.R.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Multifocality of papillary thyroid carcinoma as a risk factor for disease recurrence. Oral Oncol. 2019, 94, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Rosai, J.; DeLellis, R.A.; Carcangiu, M.L.; Frable, W.J.; Tallini, G. Tumors of the Thyroid Glands (Atlas of Tumor Pathology); Amer Registry of Pathology: Silver Spring, MD, USA, 2016; ISBN 978-1-933477-32-9. [Google Scholar]
- D’Avanzo, A.; Treseler, P.; Ituarte, P.H.G.; Wong, M.; Streja, L.; Greenspan, F.S.; Siperstein, A.E.; Duh, Q.-Y.; Clark, O.H. Follicular thyroid carcinoma: Histology and prognosis. Cancer 2004, 100, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, C.J.; Vaughan, L.; Learoyd, D.L.; Sidhu, S.B.; Delbridge, L.W.; Sywak, M.S. Management of follicular thyroid carcinoma should be individualised based on degree of capsular and vascular invasion. Eur. J. Surg. Oncol. 2011, 37, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, D.; Levy, S.; Tsvetov, G.; Gorshtein, A.; Slutzky-Shraga, I.; Akirov, A.; Robenshtok, E.; Shimon, I.; Benbassat, C.A. Long-Term Outcomes and Prognostic Factors in Patients with Differentiated Thyroid Cancer and Distant Metastases. Endocr. Pract. 2017, 23, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Bradley, N.L.; Wiseman, S.M. Papillary thyroid microcarcinoma: The significance of high risk features. BMC Cancer 2017, 17, 142. [Google Scholar] [CrossRef]
- Fraser, S.; Go, C.; Aniss, A.; Sidhu, S.; Delbridge, L.; Learoyd, D.; Clifton-Bligh, R.; Tacon, L.; Tsang, V.; Robinson, B.; et al. BRAFV600E Mutation is Associated with Decreased Disease-Free Survival in Papillary Thyroid Cancer. World J. Surg. 2016, 40, 1618–1624. [Google Scholar] [CrossRef]
- Liu, X.; Yan, K.; Lin, X.; Zhao, L.; An, W.; Wang, C.; Liu, X. The association between BRAF (V600E) mutation and pathological features in PTC. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 3041–3052. [Google Scholar] [CrossRef]
- Schob, S.; Voigt, P.; Bure, L.; Meyer, H.J.; Wickenhauser, C.; Behrmann, C.; Höhn, A.; Kachel, P.; Dralle, H.; Hoffmann, K.T.; et al. Diffusion-Weighted Imaging Using a Readout-Segmented, Multishot EPI Sequence at 3 T Distinguishes between Morphologically Differentiated and Undifferentiated Subtypes of Thyroid Carcinoma—A Preliminary Study. Transl. Oncol. 2016, 9, 403–410. [Google Scholar] [CrossRef]
- Schob, S.; Meyer, H.J.; Dieckow, J.; Pervinder, B.; Pazaitis, N.; Höhn, A.K.; Garnov, N.; Horvath-Rizea, D.; Hoffmann, K.T.; Surov, A. Histogram Analysis of Diffusion Weighted Imaging at 3T is Useful for Prediction of Lymphatic Metastatic Spread, Proliferative Activity, and Cellularity in Thyroid Cancer. Int. J. Mol. Sci. 2017, 18, 821. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Guo, Y.; Zhang, J.; Shi, L.; Ning, H.; Zhang, X.; Lu, Y. Utility of high b-value (2000 sec/mm2) DWI with RESOLVE in differentiating papillary thyroid carcinomas and papillary thyroid microcarcinomas from benign thyroid nodules. PLoS ONE 2018, 13, e0200270. [Google Scholar] [CrossRef] [PubMed]
- Schob, S.; Meyer, H.J.; Pazaitis, N.; Schramm, D.; Bremicker, K.; Exner, M.; Höhn, A.K.; Garnov, N.; Surov, A. ADC Histogram Analysis of Cervical Cancer Aids Detecting Lymphatic Metastases-a Preliminary Study. Mol. Imaging Biol. 2017, 19, 953–962. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Patients (n = 579) |
|---|---|
| Sex | |
| - Male | 139 (24%) |
| - Female | 440 (76%) |
| Age (years) | 50.7 ± 14.1 |
| Familiarity for thyroid carcinoma | 103 (17.8%) |
| Hyperthyroidism | 53 (9.2%) |
| Autoimmune thyroiditis | 215 (21.6%) |
| Surgical procedure | |
| - TT | 444 (76.7%) |
| - TT + CLND | 110 (19%) |
| - TT + CLND + LND | 25 (4.3%) |
| Nodule size (mm) | 13.7 ± 11.6 |
| Microcarcinoma | 255 (44.1%) |
| Lymph node metastases | 62 (10.7%) |
| Follow up (months) | 55 ± 15.7 |
| NED | 543 (93.8%) |
| Persistent/recurrent disease | 36 (6.2%) |
| Variable | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| NED (n = 543) | Persistent/Recurrent Disease (n = 36) | p-Value | Regression Coefficient | Odds Ratio | 95% CI | p-Value | |
| Male sex | 126 (23.2%) | 13 (36.1%) | 0.072 | 0.4867 | 1.626 | 0.734–3.605 | 0.231 |
| Age (years) | 50.8 ± 14.1 | 49.8 ± 13.3 | 0.68 | ||||
| Age > 40 years | 402 (74%) | 26 (72%) | 0.81 | ||||
| Familiarity for thyroid carcinoma | 13 (2.4%) | 1 (2.8%) | 0.88 | ||||
| Hyperthyroidism | 55 (10.1%) | 1 (2.8%) | 0.14 | ||||
| Autoimmune thyroiditis | 214 (39.4%) | 13 (36.1%) | 0.69 | ||||
| Surgical procedure | p < 0.001 | ||||||
| - TT | 431 (79.4%) | 13 (36.1%) | 1.000 | 1.000 | Reference | ||
| - TT + CLND | 96 (17.7%) | 14 (38.9%) | −0.602 | 0.548 | 0.159–1.878 | 0.339 | |
| - TT + CLND + LND | 16 (2.9%) | 9 (25%) | 0.592 | 1.807 | 0.297–10.998 | 0.521 | |
| Variable | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| NED (n = 543) | Persistent/Recurrent Disease (n = 36) | p-Value | Regression Coefficient | Odds Ratio | 95% CI | p-Value | |
| Nodule size | 13.5 ± 11.5 | 16.1 ± 12.1 | 0.21 | ||||
| Microcarcinoma | 249 (45.8%) | 6 (16.6%) | p < 0.001 | −1.114 | 0.328 | 0.117–0.920 | 0.034 |
| Thyroid weight | 28.2 ± 19 | 29.7 ± 24.6 | 0.72 | ||||
| Histotype | p < 0.01 | ||||||
| - PTC | 267 (49.2%) | 21 (58.3%) | 1.000 | 1.000 | Reference | ||
| - FV−PTC | 163 (30%) | 5 (13.9%) | −0.721 | 0.486 | 0.166–1.425 | 0.189 | |
| - Tall cell carcinoma | 37 (6.8%) | 6 (16.7%) | 0.209 | 1.233 | 0.397–3.826 | 0.716 | |
| - Diffuse sclerosing variant of PTC | 1 (0.2%) | 1 (2.8%) | 1.476 | 4.374 | 0.202–94.541 | 0.347 | |
| - FTC | 54 (9.9%) | 3 (8.3%) | −0.474 | 0.622 | 0.154–2.514 | 0.505 | |
| - Hürtle cell carcinoma | 21 (3.9%) | 0 | −19.818 | <0.001 | 0.998 | ||
| Lymph node yield | 5.8 ± 7.7 | 14 ± 10.7 | p < 0.01 | −0.012 | 0.988 | 0.929–1.049 | 0.697 |
| Lymph node metastasis | 45 (8.3%) | 16 (44.4%) | p < 0.01 | 1.453 | 4.274 | 1.367–13.359 | 0.012 |
| Lymph node ratio | 0.44 ± 0.29 | 0.5 ± 0.28 | 0.53 | ||||
| Extrathyroidal invasion | 36 (6.6%) | 7 (19.4%) | p < 0.01 | 0.258 | 1.295 | 0.444–3.775 | 0.636 |
| Multicentric carcinoma | 177 (32.6%) | 20 (55.6%) | p < 0.01 | −1.114 | 1.423 | 0.632–3.201 | 0.394 |
| Angioinvasive carcinoma | 16 (2.9%) | 3 (8.3%) | 0.08 | 0.959 | 2.611 | 0.567–12.050 | 0.219 |
| Variable | Persistent Disease (n = 10) | Recurrent Disease (n = 26) | ||||||
|---|---|---|---|---|---|---|---|---|
| Regression Coefficient | Odds Ratio | 95% CI | p-Value | Regression Coefficient | Odds Ratio | 95% CI | p-Value | |
| Microcarcinoma | −0.37710 | 0.6859 | 0.1041–4.5179 | 0.6950 | −1.51926 | 0.2189 | 0.0488–0.9812 | 0.0472 |
| Lymph node metastasis | 2.16126 | 8.6821 | 1.5796 to 47.7213 | 0.0129 | 1.34217 | 3.8273 | 1.2665–11.5661 | 0.0174 |
| Angioinvasive carcinoma | −18.64235 | <0.001 | - | 0.9986 | 1.82154 | 6.1813 | 1.1587–32.9760 | 0.0330 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medas, F.; Canu, G.L.; Boi, F.; Lai, M.L.; Erdas, E.; Calò, P.G. Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients. Cancers 2019, 11, 1230. https://doi.org/10.3390/cancers11091230
Medas F, Canu GL, Boi F, Lai ML, Erdas E, Calò PG. Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients. Cancers. 2019; 11(9):1230. https://doi.org/10.3390/cancers11091230
Chicago/Turabian StyleMedas, Fabio, Gian Luigi Canu, Francesco Boi, Maria Letizia Lai, Enrico Erdas, and Pietro Giorgio Calò. 2019. "Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients" Cancers 11, no. 9: 1230. https://doi.org/10.3390/cancers11091230
APA StyleMedas, F., Canu, G. L., Boi, F., Lai, M. L., Erdas, E., & Calò, P. G. (2019). Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients. Cancers, 11(9), 1230. https://doi.org/10.3390/cancers11091230