Respiratory-Gated Proton Beam Therapy for Hepatocellular Carcinoma Adjacent to the Gastrointestinal Tract without Fiducial Markers

 , ,
, ,
Abstract
:1. Introduction
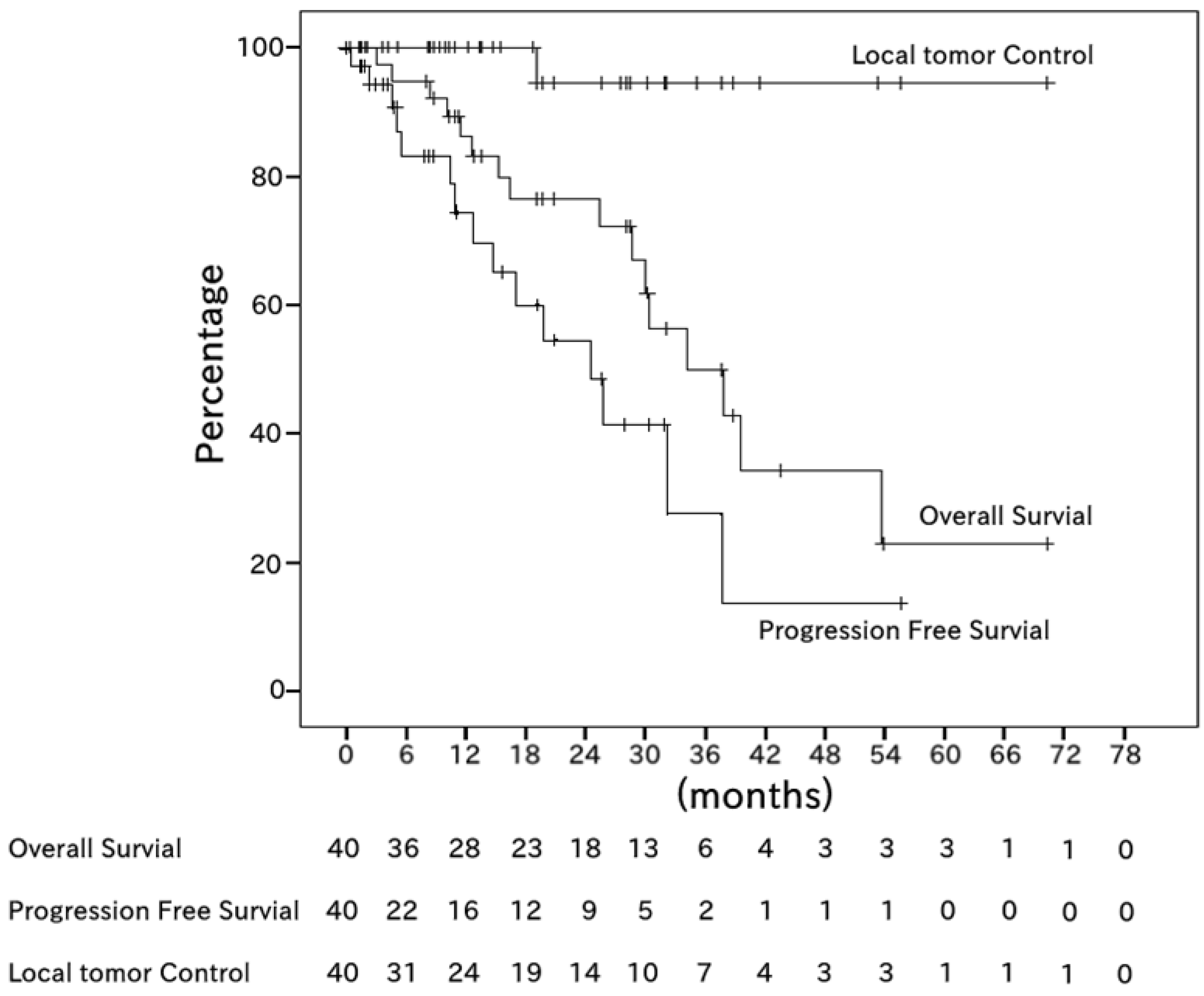
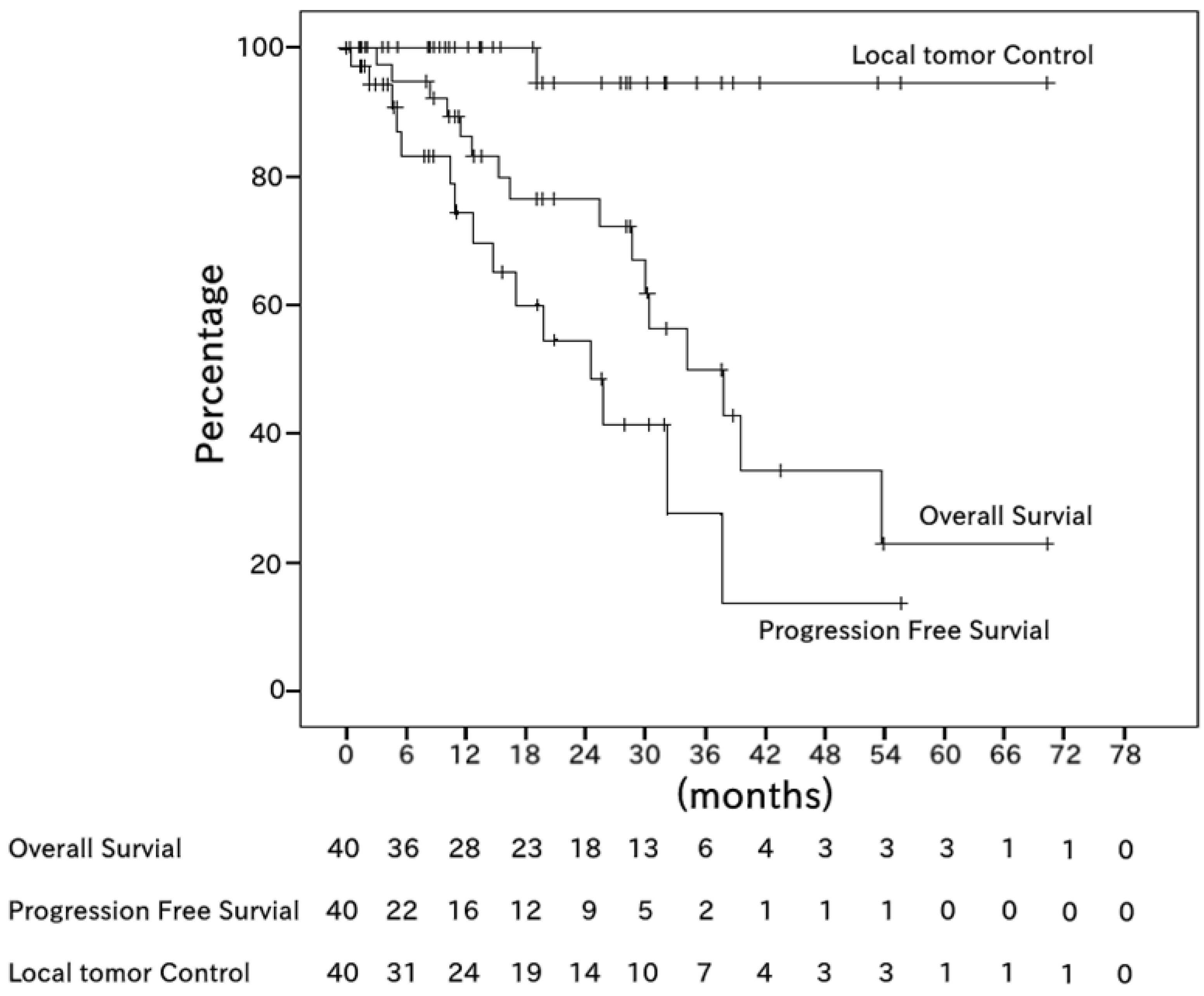
2. Results
3. Discussion
3.1. Treatment Effect
3.2. Adverse Effects
3.3. Fiducial Markers
4. Patients and Methods
4.1. Patients and Clinical Examination
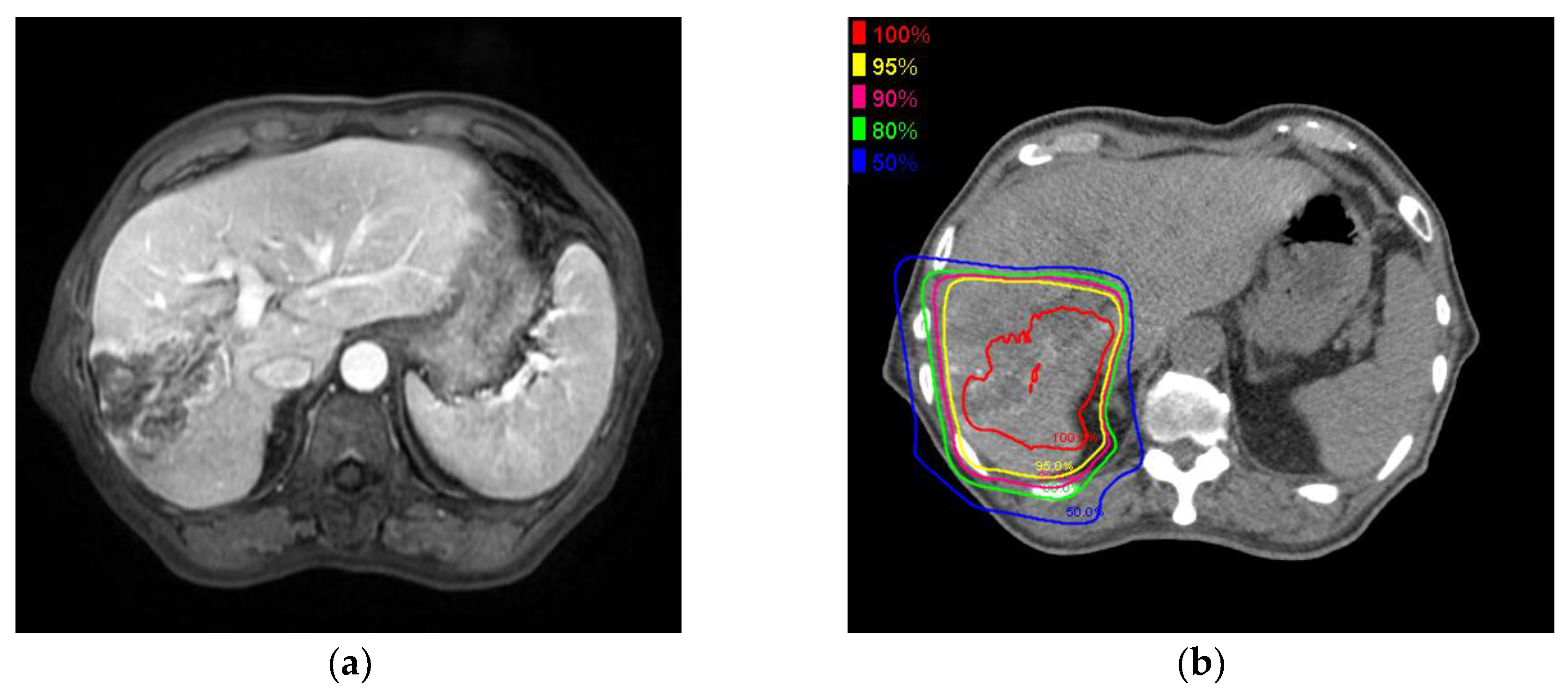
4.2. PBT Planning
4.3. PBT
4.4. Follow-Up and Toxicity Evaluation
4.5. Statistical Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Liver Cancer. Estimated Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/old/FactSheets/cancers/liver-new.asp (accessed on 15 January 2018).
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- Forner, A.; Gilabert, M.; Bruix, J.; Raoul, J.L. Treatment of intermediate-stage hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2014, 11, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Murikami, K. Preliminary neoplasms of the liver. Results of radiation therapy. Cancer 1960, 13, 714–720. [Google Scholar] [CrossRef]
- Emami, B.; Lyman., J.; Brown, A.; Coia., L.; Goitein, M.; Munzenrider, J.E.; Shank, B.; Solin, L.J.; Wesson, M. Tolerance of normal tissue to therapeutic irradiation. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 109–122. [Google Scholar] [CrossRef]
- Komatsu, S.; Fukumoto, T.; Demizu, Y.; Miyawaki, D.; Terashima, K.; Sasaki, R.; Hori, Y.; Hishikawa, Y.; Ku, Y.; Murakami, M. Clinical results and risk factors of proton and carbon ion therapy for hepatocellular carcinoma. Cancer 2011, 117, 4890–4904. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Sugahara, S.; Tokita, M.; Fukuda, K.; Mizumoto, M.; Abei, M.; Shoda, J.; Sakurai, H.; Tsuboi, K.; Tokuuye, K. Proton beam therapy for hepatocellular carcinoma: The University of Tsukuba experience. Cancer 2009, 115, 5499–5506. [Google Scholar] [CrossRef] [PubMed]
- Chiba, T.; Tokuuye, K.; Matsuzaki, Y.; Sugahara, S.; Chuganji, Y.; Kagei, K.; Shoda, J.; Hata, M.; Abei, M.; Igaki, H.; et al. Proton beam therapy for hepatocellular carcinoma: A retrospective review of 162 patients. Clin. Cancer Res. 2005, 11, 3799–3805. [Google Scholar] [CrossRef] [PubMed]
- Onishi, H.; Ozaki, M.; Kuriyama, K.; Komiyama, T.; Marino, K.; Araya, M.; Saito, R.; Aoki, S.; Maehata, Y.; Tomiaga, L.; et al. Serious gastric ulcer event after stereotactic body radiotherapy (SBRT) delivered with concomitant vinorelbine in a patient with left adrenal metastasis of lung cancer. Acta Oncol. 2010, 51, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Ohara, K.; Okumura, T.; Akisada, M.; Inada, T.; Mori, T.; Yokota, H.; Calaguas, M.J. Irradiation synchronized with respiration gate. Int. J. Radiat. Oncol. Biol. Phys. 1989, 17, 853–857. [Google Scholar] [CrossRef]
- Gabryś, D.; Kulik, R.; Trela, K.; Ślosarek, K. Dosimetric comparison of liver tumour radiotherapy in all respiratory phases and in one phase using 4DCT. Radiother. Oncol. 2011, 100, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.T.; Apisarnthanarax, S.; Yin, L.; Zou, W.; Rosen, M.; Plastaras, J.P.; Ben-Josef, E.; Metz, J.M.; Teo, B.K. Comparative assessment of liver tumor motion using cine-magnetic resonance imaging versus 4-dimensional computed tomography. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Toramatsu, C.; Katoh, N.; Shimizu, S.; Nihongi, H.; Matsuura, T.; Takao, S.; Miyamoto, N.; Suzuki, R.; Sutherland, K.; Kinoshita, R.; et al. What is the appropriate size criterion for proton radiotherapy for hepatocellular carcinoma? A dosimetric comparison of spot-scanning proton therapy versus intensity-modulated radiation therapy. Radiat. Oncol. 2013, 8, 48. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.X.; Fu, S.; Zhang, Q.; Guo, X.M. Charged particle therapy versus photon therapy for patients with hepatocellular carcinoma: A systematic review and meta-analysis. Radiother. Oncol. 2015, 114, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Lin, S.H.; Simone, C.B.; Mehta, M.P. Clinical outcomes and toxicities of proton radiotherapy for gastrointestinal neoplasms: A systematic review. J. Gastrointest. Oncol. 2016, 7, 644–664. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Okumura, T.; Abei, M.; Fukumitsu, N.; Ishige, K.; Mizumoto, M.; Hasegawa, N.; Numajiri, H.; Ohnishi, K.; Ishikawa, H.; et al. Long-term outcomes of proton beam therapy in patients with previously untreated hepatocellular carcinoma. Cancer Sci. 2017, 108, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Fukumitsu, N.; Sugahara, S.; Nakayama, H.; Fukuda, K.; Mizumoto, M.; Abei, M.; Shoda, J.; Thono, E.; Tsuboi, K.; Tokuuye, K. A prospective study of hypofractionated proton beam therapy for patients with hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, M.; Furuse, J.; Nishio, T.; Konishi, M.; Ishii, H.; Kinoshita, T.; Nagase, M.; Nihei, K.; Ogino, T. Phase II study of radiotherapy employing proton beam for hepatocellular carcinoma. J. Clin. Oncol. 2005, 23, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Saitoh, J.; Kobayashi, D.; Shibuya, K.; Koyama, Y.; Shimada, H.; Shirai, K.; Ohno, T.; Nakano, T. Dosimetric comparison of carbon ion radiotherapy and stereotactic body radiotherapy with photon beams for the treatment of hepatocellular carcinoma. Radiat. Oncol. 2015, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Sugahara, S.; Fukuda, K.; Abei, M.; Shoda, J.; Sakurai, H.; Tsuboi, K.; Matsuzaki, Y.; Tokuuye, K. Proton beam therapy for hepatocellular carcinoma located adjacent to the alimentary tract. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 992–995. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, S.; Murakami, M.; Fukumoto, T.; Hori, Y.; Hishikawa, Y.; Ku, Y. Risk factors for survival and local recurrence after particle radiotherapy for single small hepatocellular carcinoma. Br. J. Surg. 2011, 98, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Tangkijvanich, P.; Mahachai, V.; Suwangool, P.; Poovorawan, Y. Gender difference in clinicopathologic features and survival of patients with hepatocellular carcinoma. World J. Gastroenterol. 2004, 10, 1547–1550. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, M.; Okumura, T.; Hashimoto, T.; Fukuda, K.; Oshiro, Y.; Fukumitsu, N.; Abei, M.; Kawaguchi, A.; Hayashi, Y.; Ookawa, A.; et al. Proton beam therapy for hepatocellular carcinoma: a comparison of three treatment protocols. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Hata, M.; Tokuuye, K.; Sugahara, S.; Fukumitsu, N.; Hashimoto, T.; Ohnishi, K.; Nemoto, K.; Ohara, K.; Matsuzaki, Y.; Akine, Y. Proton beam therapy for hepatocellular carcinoma with limited treatment options. Cancer 2006, 107, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, M.; Tokuuye, K.; Sugahara, S.; Nakayama, H.; Fukumitsu, N.; Ohara, K.; Abei, M.; Shoda, J.; Tohno, E.; Minami, M. Proton beam therapy for hepatocellular carcinoma adjacent to the porta hepatis. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Khalsa, B.; Lord, B.; Sandrasegaran, K.; Lall, C. Planting the seeds of success: CT-guided gold seed fiducial marker placement to guide robotic radiosurgery. J. Med. Imaging Radiat. Oncol. 2013, 57, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Brook, O.R.; Gourtsoyianni, S.; Mendiratta-Lala., M.; Mahadevan, A.; Siewert, B.; Sheiman, R.R. Safety profile and technical success of imaging-guided percutaneous fiducial seed placement with and without core biopsy in the abdomen and pelvis. Am. J. Roentgenol. 2012, 198, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Balter, J.M.; Dawson, L.A.; Kazanjian, S.; McGinn, C.; Brock, K.K.; Lawrence, T.; Ten, H.R. Determination of ventilatory liver movement via radiographic evaluation of diaphragm position. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 267–270. [Google Scholar] [CrossRef]
- Yang, J.; Cai, J.; Wang, H.; Chang, Z.; Czito, B.G.; Bashir, M.R.; Palta, M.; Yin, F.F. Is diaphragm motion a good surrogate for liver tumor motion? Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Mageras, G.S.; Yorke, E. Deep Inspiration Breath Hold and Respiratory Gating Strategies for Reducing Organ Motion in Radiation Treatment. Semin. Radiat. Oncol. 2004, 14, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, H.; Tsuji, H.; Inada, T.; Maruhashi, A.; Hayakawa, Y.; Takada, Y.; Tada, J.; Fukumoto, S.; Tatuzaki, H.; Ohara, K.; et al. Clinical results of fractionated proton therapy. Int. J. Radiat. Oncol. Biol. Phys. 1993, 25, 49–60. [Google Scholar] [CrossRef]
- Takamatsu, S.; Yamamoto, K.; Maeda, Y.; Kawamura, M.; Shibata, S.; Sato, Y.; Terashima, K.; Shimizu, Y.; Tameshige, Y.; Sasaki, M.; et al. Evaluation of Focal Liver Reaction after Proton Beam Therapy for Hepatocellular Carcinoma Examined Using Gd-EOB-DTPA Enhanced Hepatic Magnetic Resonance Imaging. PLoS ONE 2016, 11, 0167155. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, M.; Okumura, T.; Hashimoto, T.; Fukuda, K.; Oshiro, Y.; Fukumitsu, N.; Abei, M.; Kawaguchi, A.; Hayashi, Y.; Ohkawa, A.; et al. Evaluation of liver function after proton beam therapy for hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Terashima, K.; Demizu, Y.; Hashimoto, N.; Jin, D.; Mima, M.; Fujii, O.; Niwa, Y.; Takatori, K.; Kitajima, N.; Sirakawa, S.; et al. A phase I/II study of gemcitabine-concurrent proton radiotherapy for locally advanced pancreatic cancer without distant metastasis. Radiother. Oncol. 2012, 103, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M.; Sasaki, R.; Miyawaki, D.; Nishimura, H.; Demizu, Y.; Akagi, T.; Suga, D.; Sakamoto, H.; Murakami, M.; Sugimura, K.; et al. Physiologic reactions after proton beam therapy in patients with prostate cancer: significance of urinary autoactivation. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 580–586. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n |
|---|---|
| Patients | 40 |
| Gender, male/female | 28/12 |
| Median age (range), years | 72 (38–87) |
| PS 0,1/2 | 38/2 |
| Median tumor size (range), mm | 37 (11–124) |
| <50 mm/50–100 mm/>100 mm | 27/8/5 |
| Chronic hepatitis HCV/HBV/alcoholic/NASH/none | 15/5/10/1/9 |
| Child Pugh A/B | 28/12 |
| Tumor thrombus PV/HV/bile duct | 12/2/10 |
| Prior treatment TACE/RFA/PEIT/surgery | 16/11/1/8 |
| Operable / inoperable | 4/36 |
| Comorbidities anticoagulation/esophageal varices/history of GI bleeding or ulcers/none | 2/9/3/26 |
| T1/2/3/4 | 10/12/18/0 |
| Solitary/multiple | 10/30 |
| Median GTV volume (range), cm3 | 21.4 (1.5–882.9) |
| Median liver volume (range), cm3 | 1259.2 (554.9–2198.6) |
| The GI-tract close to the tumorEsophagus/stomach and duodenum/colon | 4/20/16 |
| Total Dose(CGE) | Number of Fractions | Dose per Fractions | Equivalent Total Doses(2Gy/fraction) | Cases | The Number of Times of the Replanned Cases (number of cases replanned twice) | Fractions at Replanned (cases) | |
|---|---|---|---|---|---|---|---|
| α/β = 10 | α/β = 3 | ||||||
| 80.0 | 25 | 3.2 | 88.0 | 99.2 | 1 | - | - |
| 76.0 | 38 | 2 | 76 | 76 | 5 | 6(1) | 5(1),20(3),30(2) |
| 76.0 | 20 | 3.8 | 87.4 | 103.4 | 17 | 3 | 6(1),10(1),12(1) |
| 74.8 | 34 | 2.2 | 76 | 77.8 | 3 | 3(1) | 10(1),18(1), 20(1) |
| 70.4 | 32 | 2.2 | 71.6 | 73.2 | 8 | 8 | 14(1),20(1),22(6) |
| 70.0 | 35 | 2 | 70 | 70 | 3 | 4(1) | 15(1),20(1),25(1), 30(1) |
| 67.5 | 25 | 2.5 | 65.1 | 68.8 | 1 | - | - |
| 66.0 | 30 | 2.2 | 67.1 | 68.6 | 1 | 1 | 23(1) |
| 52.8 | 24 | 2.2 | 53.7 | 54.9 | 1 | - | - |
| Variables | p-Value | HR | HR 95% CI | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.232 | 1.034 | 0.979 | 1.093 |
| Tumor number | 0.912 | 1.096 | 0.216 | 5.561 |
| sex (female) | 0.003 | 11.903 | 2.319 | 61.088 |
| PS | 0.006 | 38.858 | 2.797 | 539.897 |
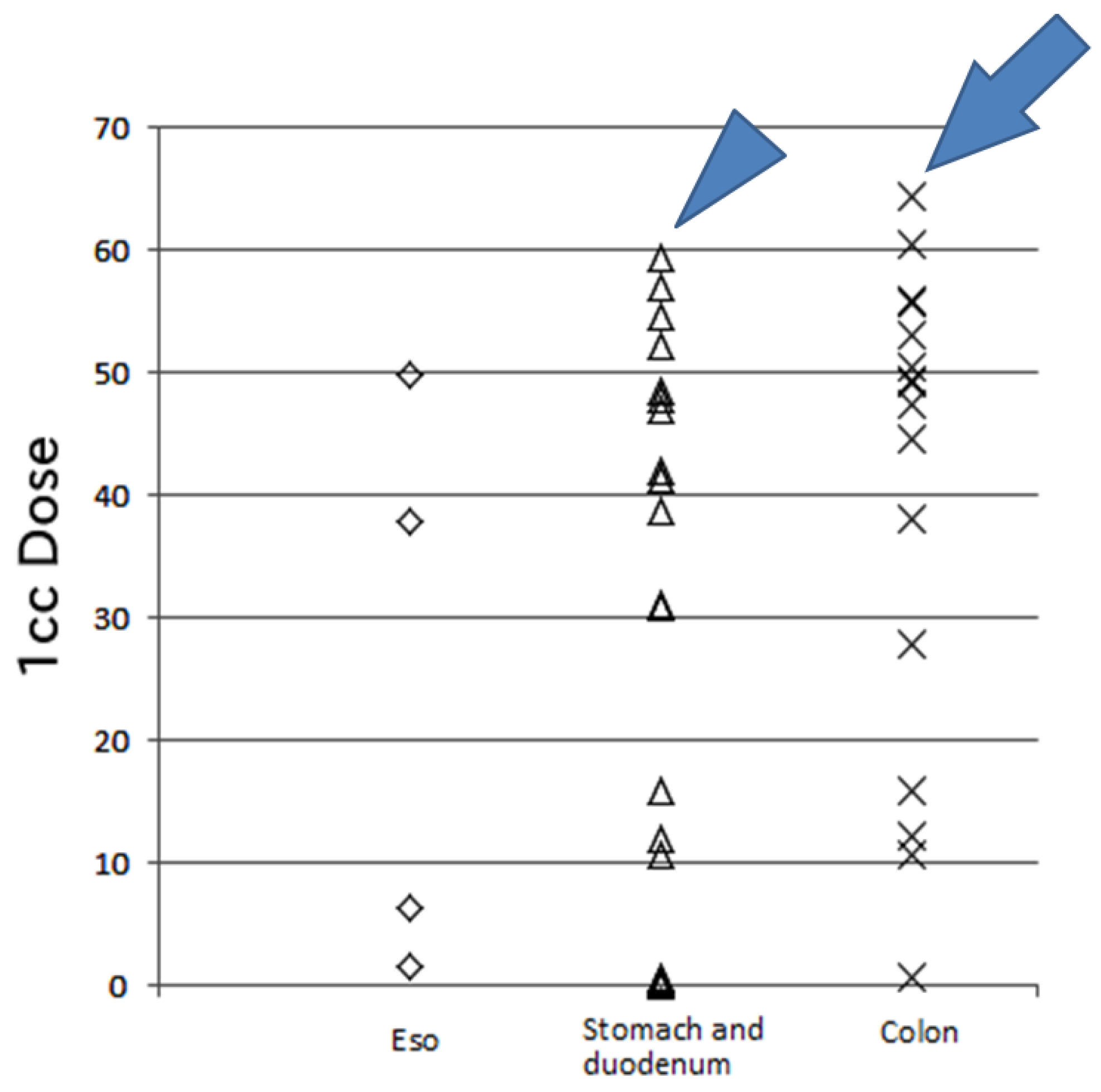
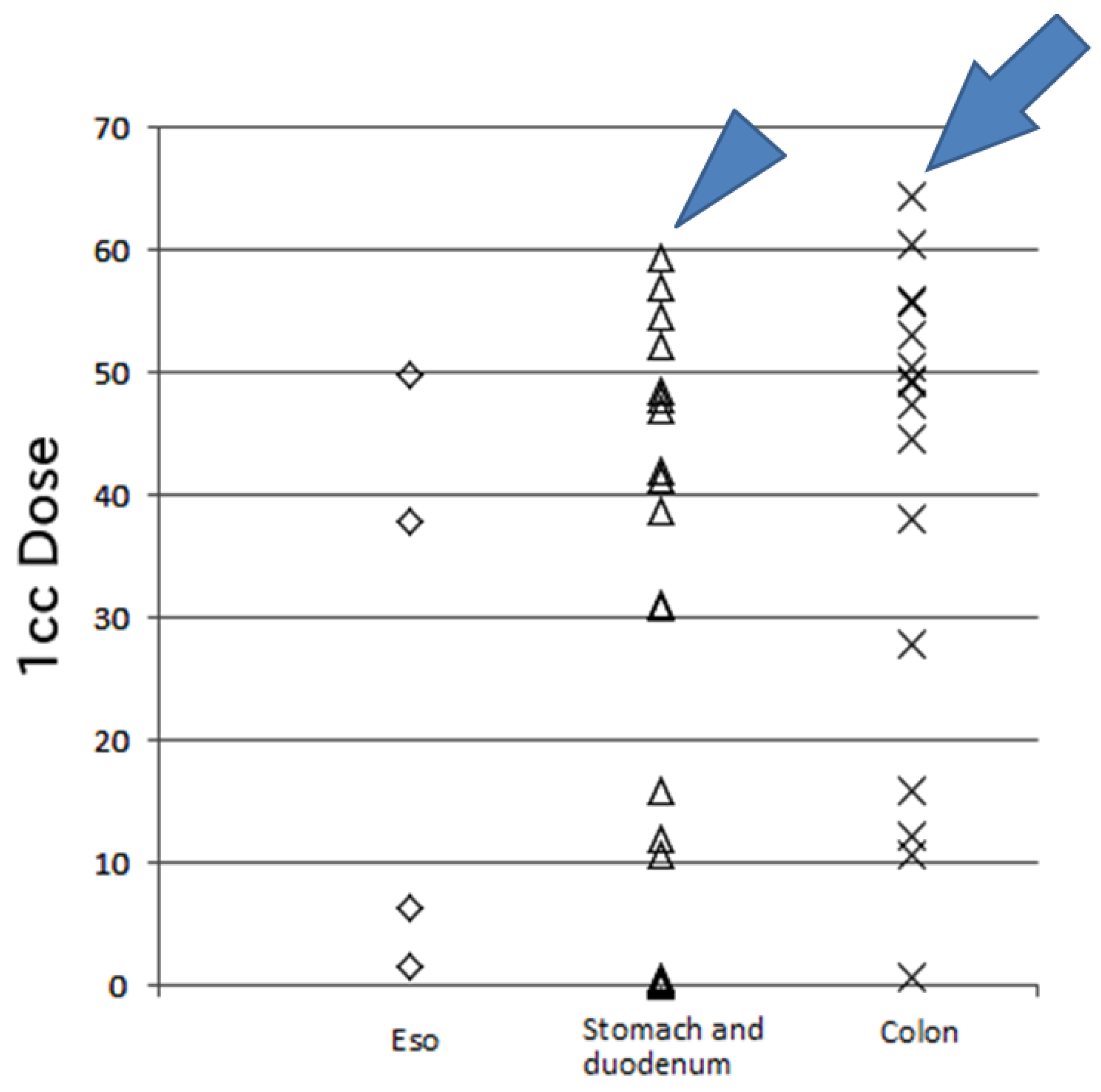
| Organ | Distance (mm) | Max Dose (CGE) | 1-cc Dose (CGE) | n |
|---|---|---|---|---|
| Esophagus | 7(0–18) | 43.4(15.3–54.4) | 22.1(1.5–49.7) | 4 |
| Stomach and duodenum | 11(4–19) | 48.8(0.6–70.6) | 34.9(0–59.3) | 20 |
| Colon | 9(0–17) | 53.4(12.9–71.6) | 48.4(0.5–64.4) | 16 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mizuhata, M.; Takamatsu, S.; Shibata, S.; Bou, S.; Sato, Y.; Kawamura, M.; Asahi, S.; Tameshige, Y.; Maeda, Y.; Sasaki, M.; et al. Respiratory-Gated Proton Beam Therapy for Hepatocellular Carcinoma Adjacent to the Gastrointestinal Tract without Fiducial Markers. Cancers 2018, 10, 58. https://doi.org/10.3390/cancers10020058
Mizuhata M, Takamatsu S, Shibata S, Bou S, Sato Y, Kawamura M, Asahi S, Tameshige Y, Maeda Y, Sasaki M, et al. Respiratory-Gated Proton Beam Therapy for Hepatocellular Carcinoma Adjacent to the Gastrointestinal Tract without Fiducial Markers. Cancers. 2018; 10(2):58. https://doi.org/10.3390/cancers10020058
Chicago/Turabian StyleMizuhata, Miu, Shigeyuki Takamatsu, Satoshi Shibata, Sayuri Bou, Yoshitaka Sato, Mariko Kawamura, Satoko Asahi, Yuji Tameshige, Yoshikazu Maeda, Makoto Sasaki, and et al. 2018. "Respiratory-Gated Proton Beam Therapy for Hepatocellular Carcinoma Adjacent to the Gastrointestinal Tract without Fiducial Markers" Cancers 10, no. 2: 58. https://doi.org/10.3390/cancers10020058
APA StyleMizuhata, M., Takamatsu, S., Shibata, S., Bou, S., Sato, Y., Kawamura, M., Asahi, S., Tameshige, Y., Maeda, Y., Sasaki, M., Kumano, T., Kobayashi, S., Yamamoto, K., Tamamura, H., & Gabata, T. (2018). Respiratory-Gated Proton Beam Therapy for Hepatocellular Carcinoma Adjacent to the Gastrointestinal Tract without Fiducial Markers. Cancers, 10(2), 58. https://doi.org/10.3390/cancers10020058