Hemostasis-On-a-Chip: Impedance Spectroscopy Meets Microfluidics for Hemostasis Evaluation

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
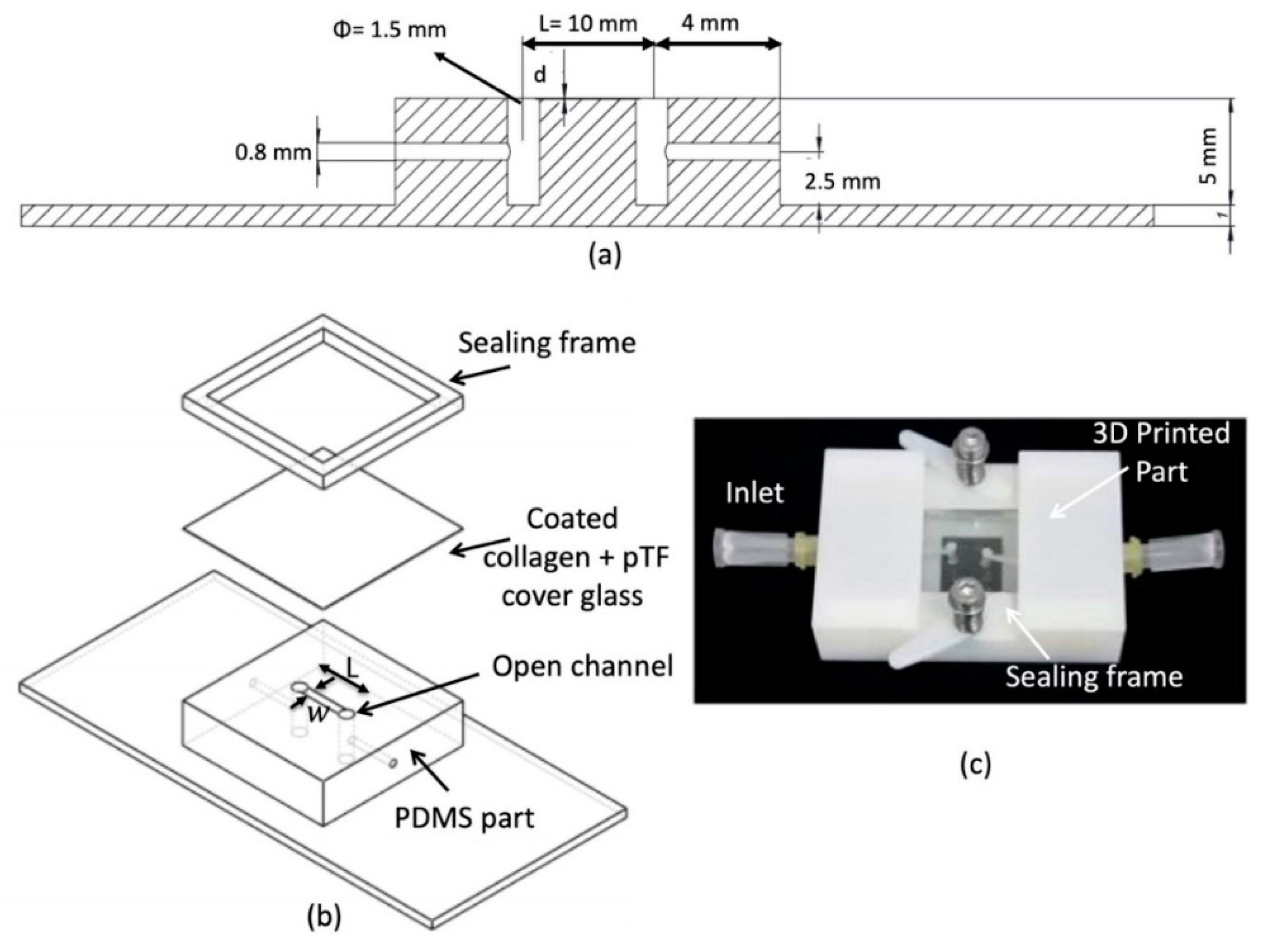
2.1. Microflow Chamber Design and Manufacturing
2.2. Biomimetic Coatings and Sample Preparation
2.3. Flow Assays
2.4. Image Capture and Analysis
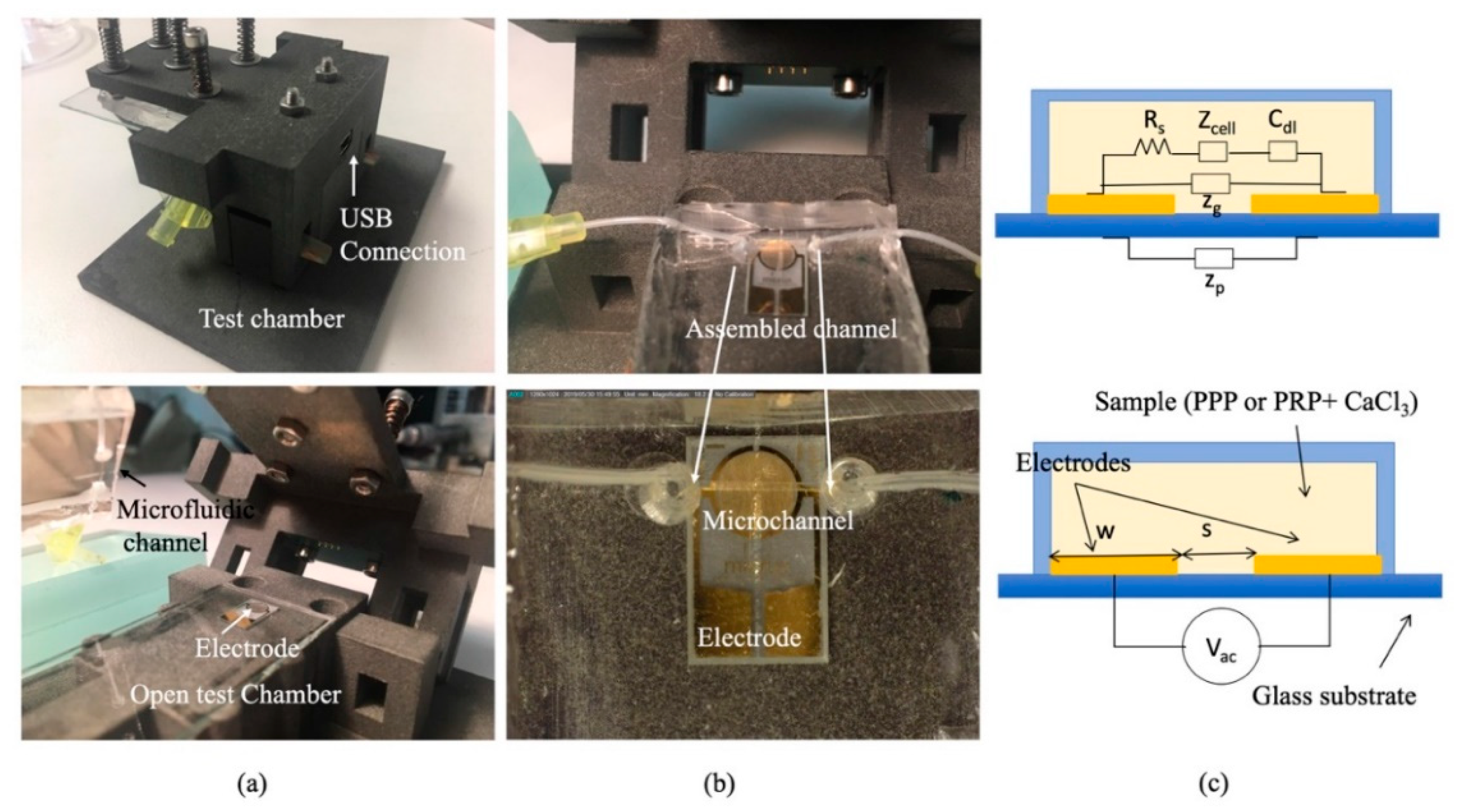
2.5. Impedance Characterization
- For low frequencies , dominates the impedance measured.
- For frequencies , is the dominant impedance.
- For frequencies , is the dominant impedance.
3. Results
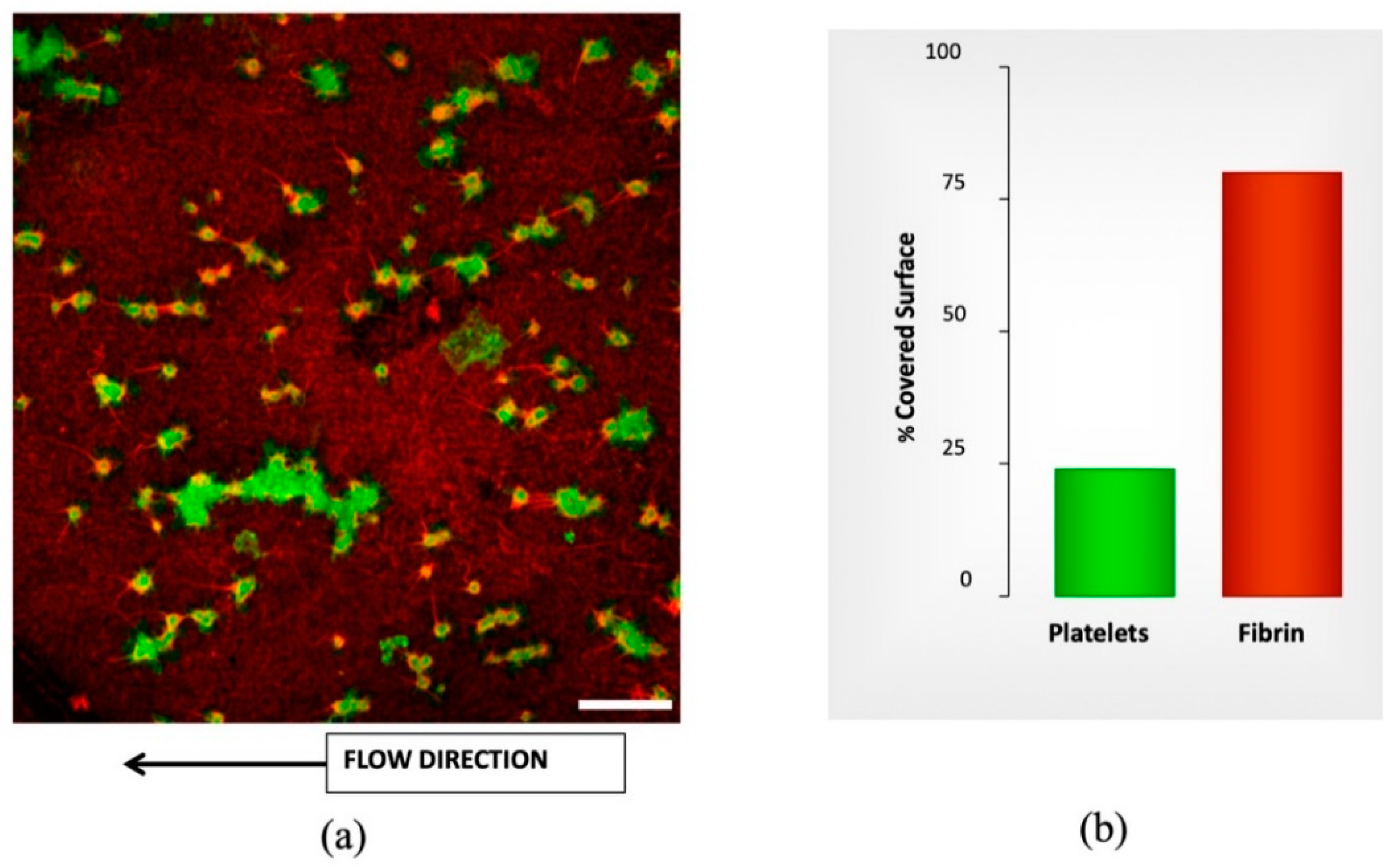
3.1. Flow Assay Results
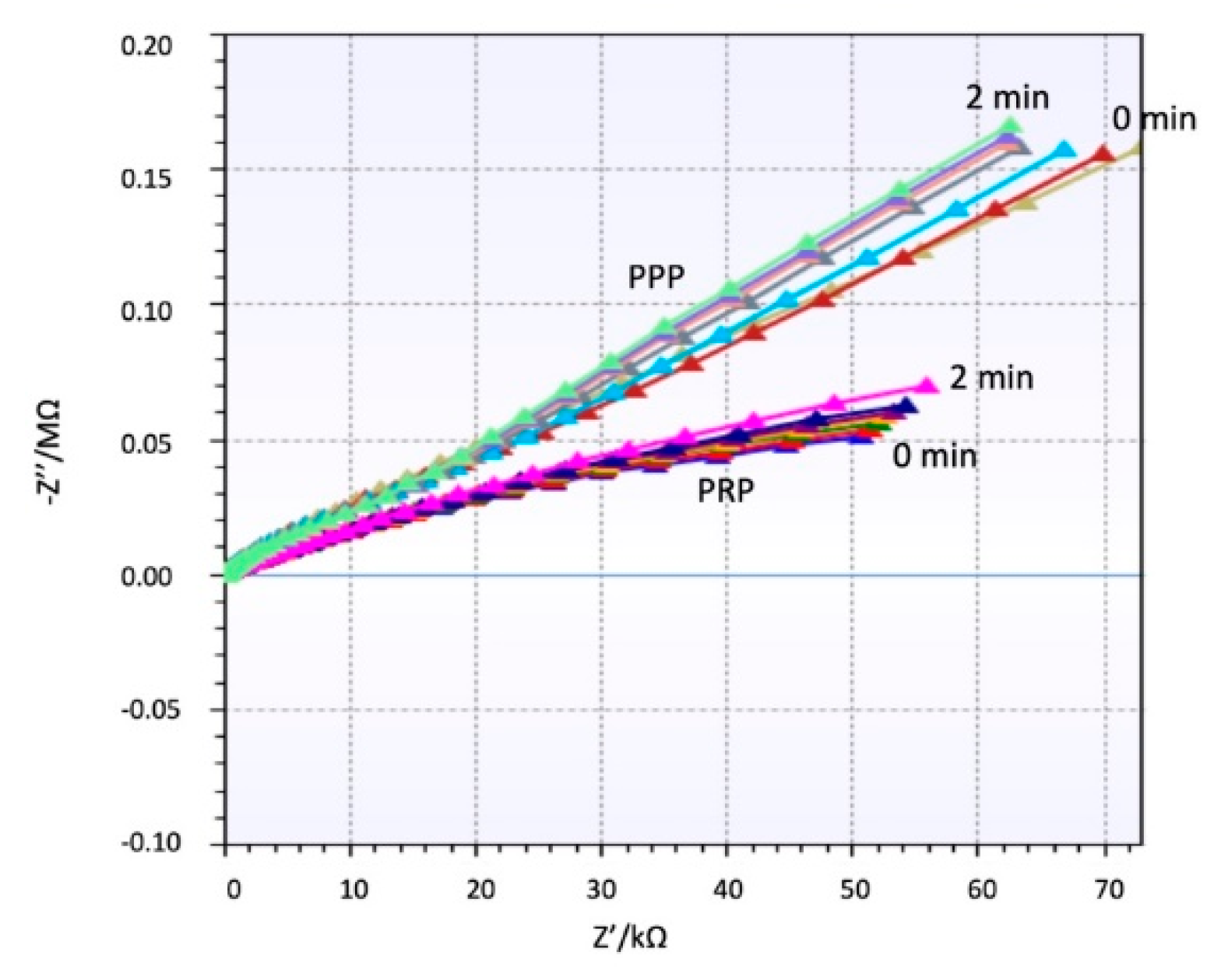
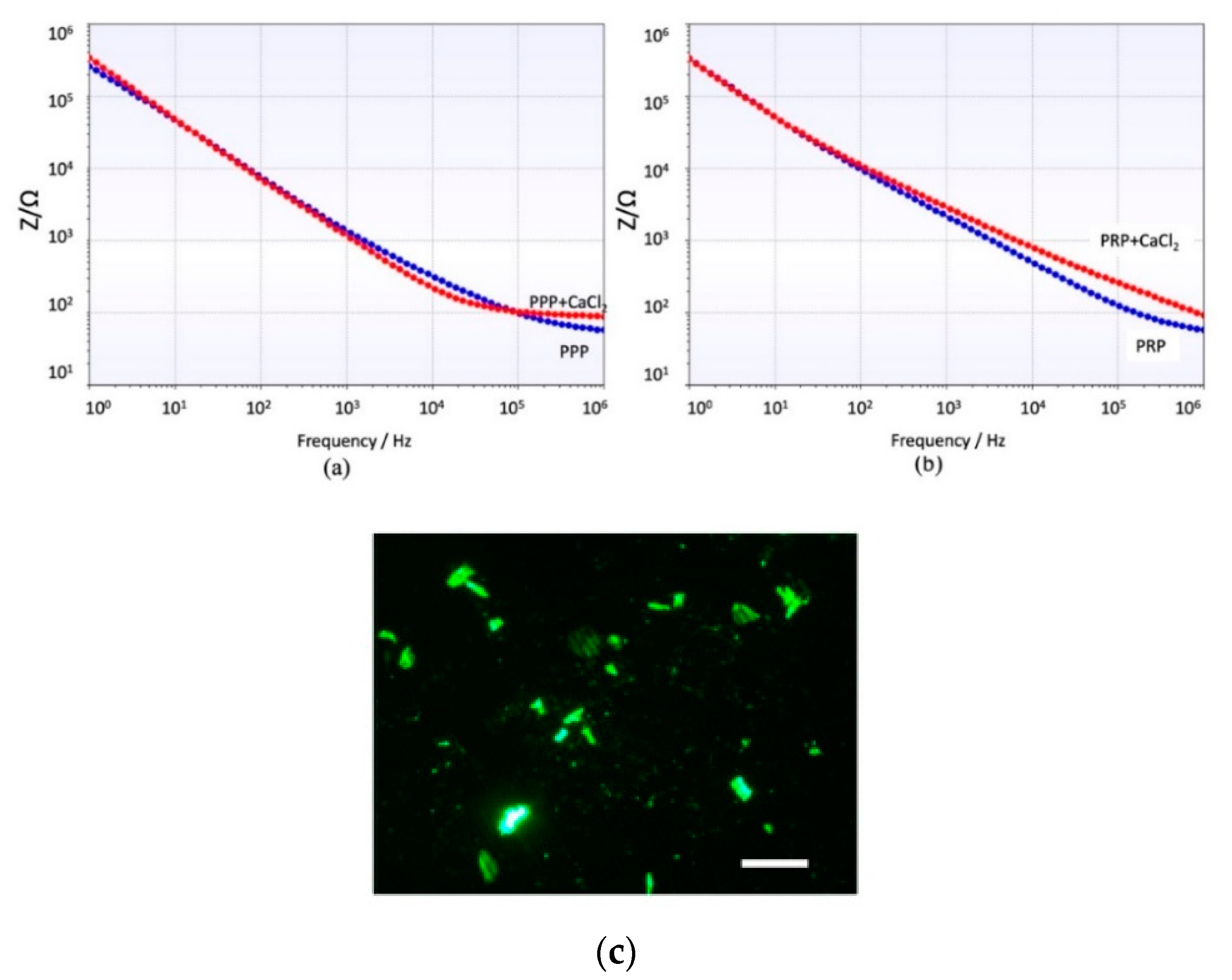
3.2. Impedance Spectroscopy Assay Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Neeves, K.B.; Onasoga, A.A.; Wufsus, A.R. The use of microfluidics in hemostasis: Clinical diagnostics and biomimetic models of vascular injury. Curr. Opin. Hematol. 2013, 20, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Kastrup, C.J.; Liu, Y.; Ismagilov, R.F. Threshold Response of Initiation of Blood Coagulation by Tissue Factor in Patterned Microfluidic Capillaries Is Controlled by Shear Rate. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 2035–2041. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Ku, D.N.; Forest, C.R. Microfluidic system for simultaneous optical measurement of platelet aggregation at multiple shear rates in whole blood. Lab Chip 2012, 12, 1355. [Google Scholar] [CrossRef] [PubMed]
- Michelson, A.D. Methods for the measurement of platelet function. Am. J. Cardiol. 2009, 103, 20A–26A. [Google Scholar] [CrossRef] [PubMed]
- Sakariassen, K.S.; Houdijk, W.P.; Sixma, J.J.; Aarts, P.A.; de Groot, P.G. A perfusion chamber developed to investigate platelet interaction in flowing blood with human vessel wall cells, their extracellular matrix, and purified components. J. Lab Clin. Med. 1983, 102, 522–535. [Google Scholar] [PubMed]
- Escolar, G.; Mazzara, R.; Castillo, R.; Ordinas, A. The role of the Baumgartner technique in transfusion medicine: Research and clinical applications. Transfusion 1994, 34, 542–549. [Google Scholar] [CrossRef]
- Nagy, M.; Heemskerk, J.W.; Swieringa, F. Use of microfluidics to assess the platelet-based control of coagulation. Platelets 2017, 28, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Onasoga-Jarvis, A.A.; Leiderman, K.; Fogelson, A.L.; Wang, M.; Manco-Johnson, M.J.; Di Paola, J.A.; Neeves, K.B. The Effect of Factor VIII Deficiencies and Replacement and Bypass Therapies on Thrombus Formation under Venous Flow Conditions in Microfluidic and Computational Models. PLoS ONE 2013, 8, e78732. [Google Scholar] [CrossRef]
- Fedosov, D.A.; Dao, M.; Karniadakis, G.E.; Suresh, S. Computational Biorheology of Human Blood Flow in Health and Disease. Ann. Biomed. Eng. 2014, 42, 368–387. [Google Scholar] [CrossRef]
- Jain, A.; van der Meer, A.D.; Papa, A.L.; Barrile, R.; Lai, A.; Schlechter, B.L.; Otieno, M.A.; Louden, C.S.; Hamilton, G.A.; Frelinger, A.L.; et al. Assessment of whole blood thrombosis in a microfluidic device lined by fixed human endothelium. Biomed. Microdevices 2016, 18, 73. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Davoudi, F.; Walch, P.; Manbachi, A.; Luo, X.; Dell’Erba, V.; Miri, A.K.; Albadawi, H.; Arneri, A.; Wang, X.; et al. Bioprinted thrombosis-on-a-chip. Lab Chip 2016, 16, 4097–4105. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Graveline, A.; Waterhouse, A.; Vernet, A.; Flaumenhaft, R.; Ingber, D.E. A shear gradient-activated microfluidic device for automated monitoring of whole blood haemostasis and platelet function. Nat. Commun. 2016, 7, 10176. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Hellkamp, A.S.; Fox, K.A. Point-of-Care Warfarin Monitoring in the ROCKET AF Trial. N. Engl. J. Med. 2016, 374, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Ohashi, Y.; Pan, G.; Kato, M.; Kajikawa, M. Point-of-Care Device for Warfarin Monitoring Used in the J-ROCKET AF Study. Circ. J. 2016, 80, 1488–1490. [Google Scholar] [PubMed]
- Cattaneo, M. Resistance to antiplatelet drugs: Molecular mechanisms and laboratory detection. J. Thromb. Haemost. 2007, 5, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Lenk, E.; Spannagl, M. Platelet Function Testing—Guided Antiplatelet Therapy. EJIFCC 2014, 24, 90. [Google Scholar]
- Lopez-Vilchez, I.; Tonda, R.; Hernandez, R.M.; Navalon, F.; Diaz-Ricart, M.; Galan, A.M.; Escolar, G. Relative contributions of collagen and tissue factor to thrombus formation on damaged vascular vessels: In-vitro studies with circulating blood. Coron. Artery Dis. 2009, 20, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.G.; Stefanadis, C. Vascular Wall shear stress: Basic principles and Methods. Hell. J. Cardiol 2005, 46, 9–15. [Google Scholar]
- Bruus, H. Theoretical Microfluidics; Oxford university press: College Park, MD, USA, 2008; Volume 18, p. 363. [Google Scholar]
- Yeom, E.; Kang, Y.J.; Lee, S.J. Changes in velocity profile according to blood viscosity in a microchannel. Biomicrofluidics 2014, 8, 034110. [Google Scholar] [CrossRef]
- Dak, P.; Ebrahimi, A.; Alam, M.A. Non-Faradaic Impedance Characterization of an Evaporating Droplet for Microfluidic and Biosensing Applications. Lab Chip 2015, 14, 2469–2479. [Google Scholar] [CrossRef]
- Ting, L.; Feghhi, S.; Karchin, A.; Tooley, W.; White, N.J. Clot-On-A-Chip: A Microfluidic Device to Study Platelet Aggregation and Contractility Under Shear. Blood 2013, 122, 2363. [Google Scholar]
- Lam, W.A. Thrombosis-on-a-Chip: A New Way to Model a Complex Process. Blood 2017, 130, SCI-10. [Google Scholar]
- Mallén-Alberdi, M.; Vigués, N.; Mas, J.; Fernández-Sánchez, C.; Baldi, A. Impedance spectral fingerprint of E. coli cells on interdigitated electrodes: A new approach for label free and selective detection. Sens. Bio-Sens. Res. 2016, 7, 100–106. [Google Scholar] [CrossRef]
- Van Duuren, J.B.; Müsken, M.; Karge, B.; Tomasch, J.; Wittmann, C.; Häussler, S.; Brönstrup, M. Use of Single-Frequency Impedance Spectroscopy to Characterize the Growth Dynamics of Biofilm Formation in Pseudomonas aeruginosa. Sci. Rep. 2017, 7, 5223. [Google Scholar] [CrossRef] [PubMed]
- Clausen, C.; Dimaki, M.; Bertelsen, C.; Skands, G.; Rodriguez-Trujillo, R.; Thomsen, J.; Svendsen, W. Bacteria Detection and Differentiation Using Impedance Flow Cytometry. Sensors (Basel) 2018, 18, 3496. [Google Scholar] [CrossRef] [PubMed]
- Eldarrat, A.; High, A.; Kale, G. Influence of sodium chloride content in electrolyte solution on electrochemical impedance measurements of human dentin. Dent. Res. J. (Isfahan) 2017, 14, 25–31. [Google Scholar] [CrossRef]
- Boumya, W.; Laghrib, F.; Lahrich, S.; Farahi, A.; Achak, M.; Bakasse, M.; El Mhammedi, M.A. Electrochemical impedance spectroscopy measurements for determination of derivatized aldehydes in several matrices. Heliyon 2017, 3, e00392. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| [APIX] ng/mL | Platelets | Fibrin |
|---|---|---|
| 0 | 23.0 ± 3.0 | 43.4 ± 4.8 |
| 10 | 17.9 ± 0.9 | 42.1 ± 1.9 |
| 40 | 14.0 ± 5.3 | 23.4 ± 7.7 |
| 160 | 5.4 ± 2.2 *# | 14.1 ± 4.9 *# |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karimi, S.; Farré-Lladós, J.; Mir, E.; Escolar, G.; Casals-Terré, J. Hemostasis-On-a-Chip: Impedance Spectroscopy Meets Microfluidics for Hemostasis Evaluation. Micromachines 2019, 10, 534. https://doi.org/10.3390/mi10080534
Karimi S, Farré-Lladós J, Mir E, Escolar G, Casals-Terré J. Hemostasis-On-a-Chip: Impedance Spectroscopy Meets Microfluidics for Hemostasis Evaluation. Micromachines. 2019; 10(8):534. https://doi.org/10.3390/mi10080534
Chicago/Turabian StyleKarimi, Shadi, Josep Farré-Lladós, Enrique Mir, Ginés Escolar, and Jasmina Casals-Terré. 2019. "Hemostasis-On-a-Chip: Impedance Spectroscopy Meets Microfluidics for Hemostasis Evaluation" Micromachines 10, no. 8: 534. https://doi.org/10.3390/mi10080534
APA StyleKarimi, S., Farré-Lladós, J., Mir, E., Escolar, G., & Casals-Terré, J. (2019). Hemostasis-On-a-Chip: Impedance Spectroscopy Meets Microfluidics for Hemostasis Evaluation. Micromachines, 10(8), 534. https://doi.org/10.3390/mi10080534