1. Introduction
Benign essential blepharospasm (BEB), a focal dystonia, is characterized by increased blinking due to overactivity of the orbicularis oculi muscle. In the course of time the involuntary muscle contractions may be prolonged, causing functional blindness [
1,
2,
3,
4], and may spread to neighboring muscles (Meiges syndrome) [
5,
6]. Up until now the underlying cause of the disease remains unknown. Depending on the geographical region, the prevalence of BEB varies between 1.7 and 13.3 per 100,000 [
7,
8]. Women are predominantly found among those affected. The first symptoms usually appear between the fifth and seventh decade of life [
9,
10].
Hemifacial spasm (HFS) is characterized by mostly unilateral, involuntary contractions of the facial muscles innervated by the facial nerve. These can appear as slight muscle tremors, significant twitching or long-lasting muscle spasms of individual facial muscle groups or half of the face [
11,
12,
13,
14]. HFS usually occurs due to compression of the facial nerve [
15] caused by neighboring arterial vessels of the brainstem and cerebellum as well as masses, cysts, or bony abnormalities [
16,
17,
18]. According to Rosenstengel et al. (2012), approximately 8000–9000 people in Germany suffer from HFS [
19], corresponding to a prevalence of 9.9–11.8 per 100,000 inhabitants. Women are particularly affected [
19,
20], as are people over the age of 40 years [
20,
21].
The unsatisfactory effects of numerous oral drugs [
13,
22] and a significantly higher complication rate of surgical interventions [
1,
13] make regular injections of BoNT/A the therapy of first choice for BEB and HSF [
22,
23]. For this purpose, three different preparations of BoNT/A are currently available in Germany: onabotulinum toxin (Botox
®, Allergan Pharmaceuticals, Dublin, Ireland), incobotulinum toxin (Xeomin
®, Merz Pharmaceuticals GmbH, Frankfurt/Main, Germany) and abobotulinum toxin (Dysport
®, Ipsen Pharma, Paris, France). To treat BEB and HFS, a combined subcutaneous-intramuscular injection of the toxin in affected muscles is carried out. Since the paralytic effect is only temporary, the treatment must be repeated at regular intervals of usually eight to twelve weeks [
24].
Compared to the high therapeutic effect, adverse effects of BoNT/A treatment occur rarely, are mostly mild, and are only of short duration [
13,
25]. This also applies to subcutaneous bleeding and hematomas around the injection sites. However, there is concern that patients on antithrombotic medication are at higher risk of subcutaneous bleeding and hematoma. Antithrombotic therapy is used to prevent or treat thrombosis in patients in a variety of clinical situations of different cardiovascular conditions [
26], and includes two major classes of drugs: anticoagulants and platelet aggregation inhibitors. Antiplatelet agents prevent or delay the activation and aggregation of platelets and include acetylsalicylic acid (ASA) and ADP receptor antagonists (ADP-RA) [
27,
28], while a combination of platelet aggregation inhibitor drug groups is referred to as dual antiplatelet therapy (DAPT). Anticoagulants prevent or delay the formation of a red thrombus through activated coagulation factors and include vitamin K antagonists (VKA) and direct oral anticoagulants (DOAC).
According to the manufacturers of vitamin K antagonists (VKA), the subcutaneous-intramuscular injection of BoNT/A in patients undergoing therapy with these preparations is contraindicated “due to the risk of massive bleeding” (direction for use Marcumar® 3 mg tablets, MEDA Pharma GmbH & Co. KG, Bad Homburg, Germany, 2018; direction for use Phenpro.-ratiopharm® 3 mg tablets, ratiopharm GmbH, Ulm, Germany 2018). The respective directions for use of other antithrombotics do not include this contraindication explicitly but include a warning about hematoma. However, due to lifestyle and demographic changes with an aging population, the number of patients with antithrombotic medication is expected to increase. At the same time, the number of studies investigating the risk of bleeding after BoNT/A injection in patients on antithrombotic medication is limited to date. The aim of this study was to assess the frequency and severity of hemorrhagic side effects of BoNT/A treatment for BEB and HFS in patients on antithrombotic medication. Special attention was paid to the medical relevance of these adverse effects and their influence on the physical and psychological well-being of the affected patients.
2. Results
2.1. Demographic Data
A total of 140 patients were included in the study between May and November 2019. Overall, the mean (±SD) age of the participants was 70 ± 12 [37;91] years, with 65% (n = 91) being women. Most participants underwent BoNT/A treatment for BEB (75%, 105/140). In median, participants had already been treated at the University Eye Clinic Bonn for 9 [0;33] years. The number of past BoNT/A treatments, including the current treatment, varied between two and 155 treatments, with a median of 35 treatments per study participant. For the current treatment, 70% (73/105) of the participants suffering from BEB were treated with Xeomin®, whereas Botox® was mostly used to treat HFS (69%, 24/35). The median total dose of the BoNT/A preparation administered for the treatment of BEB was 35.0 [7.5;75.0] units of Botox® or 30.0 [5.0;85.0] units of Xeomin®. A median of 12.5 [7.5;30.0] units of Botox® and 20.0 [7.5;65.0] units of Xeomin® were administered for the treatment of HFS. Antithrombotic medication was taken by 41% (58/140) of the participants.
Table 1 shows demographic and treatment characteristics of patients in the control group and the ATD group. Apart from age (
p < 0.01) and the applied BoNT/A preparation (
p = 0.04), there were no significant differences between groups. The most frequently used antithrombotic drug was ASA (52%, 30/58). Almost every fourth participant on antithrombotic medication claimed to be on DOAC (24%, 14/58). The regular intake of VKA, ADP-RA or DAPT was much less common.
Table 2 shows demographic and treatment characteristics of patients in the ATD group subgroups. Except for gender distribution (
p = 0.01), there was no significant difference between the subgroups of the ATD group.
2.2. Hematoma Frequency
More than one-third of patients had at least once experienced a hematoma after treatment with BoNT/A in the past (HF
retro) in both the control and the ATD group (control: 39%, 31/80; ATD: 38%, 22/58). Adjusting for the number of past BoNT/A treatments, HF
retro averaged 3% (154/5298, [0.0;100]) of treatments, with a mean of 4% (109/2744), [0.0;100] within the control group and 2% (45/2554, [0.0:33.3] in the ATD group (
Table 3). The files of two participants in the control group were incomplete regarding the history of side effects and were not included in the analysis.
Overall, the proportion of patients with hematoma after current BoNT/A treatment (HF
actual) was 30.4% (38/125). Participants in both the control and ATD group were equally affected by hematoma after current BoNT/A treatment (HF
actual: control: 31%, 22/72; ATD: 30%, 16/53). Within the subgroups ADP-RA and DAPT, half of all participants suffered a hematoma after current BoNT/A injection (ADP-RA: 50%, 2/4; DAPT: 50%, 1/2), whereas for the participants who regularly took a DOAC the HF
actual was 8% (1/13). Despite the evidence of these tendencies, a significant connection between the intake of certain antithrombotic drugs and the occurrence of a hematoma after current treatment could not be demonstrated (
Table 3). A total of 15 participants (control: 10; ATD: 5) did not complete the questionnaire on current BoNT/A treatment and were not included in the analysis.
2.3. Hematoma Intensity
The majority of participants (42%, 15/36) reported that the hematoma occurred immediately after treatment or on the same day (47%, 17/36). Only 11% (4/36) of the patients with hematoma, all of whom belonged to the ATD group, stated that the hematoma appeared one or more days after the BoNT/A injection. The hematomas were visible for a mean period (±SD) of 9.9 ± 7.4 [3.0;33.0] days. There was no significant difference between the control and ATD group or between the ATD subgroups regarding the duration of the hematoma. Two participants in the control group did not provide information on the duration of the hematoma and were therefore not included in this analysis.
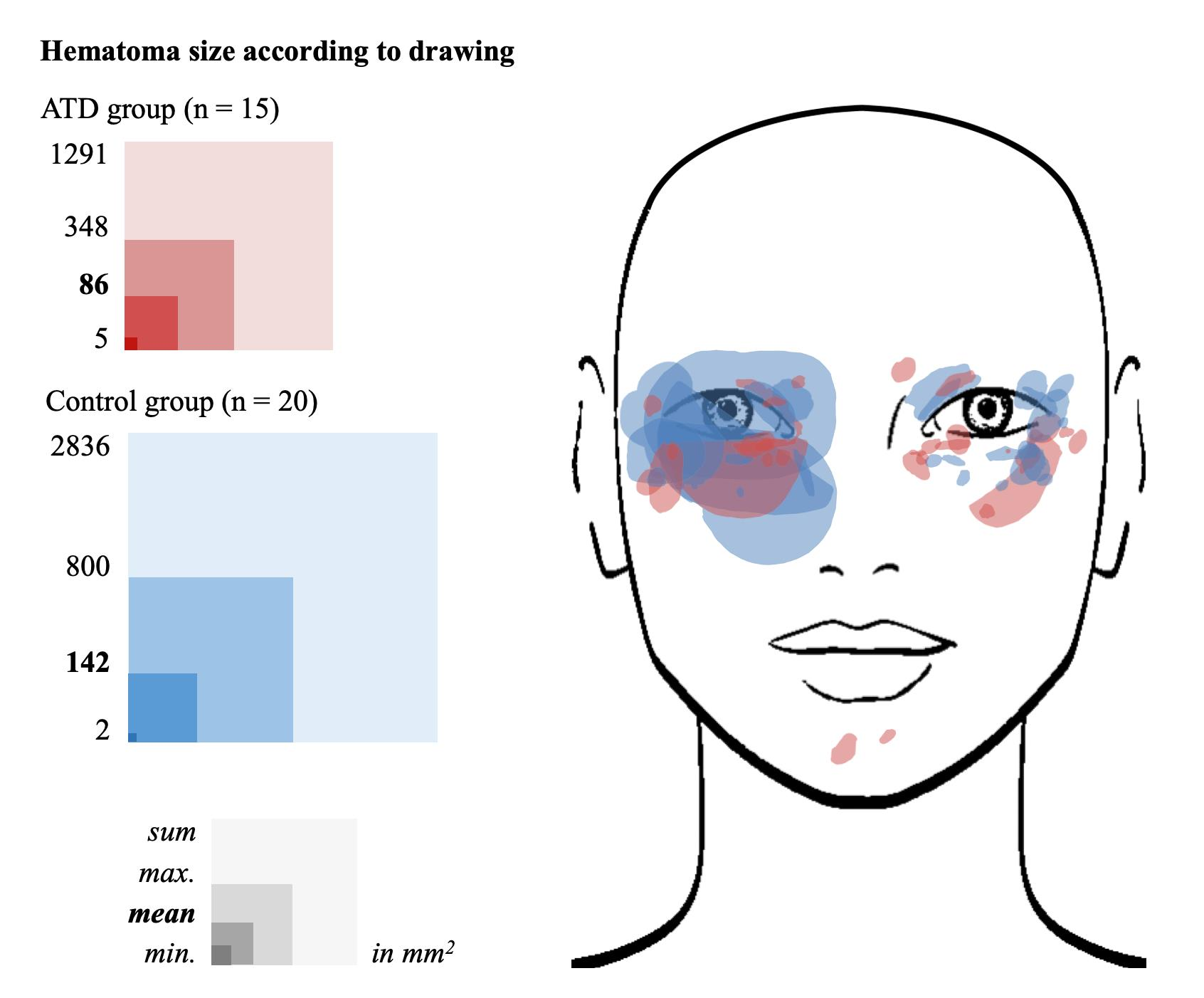
More than half of the participants stated that the hematoma was punctiform and ≤1.5 cm in diameter (57%, 21/37). The other participants reported more pronounced hematomas, however mostly ≤2.5 cm in diameter (24%, 9/37). The size of the hematoma drawn in a facial image varied between two and 800 mm
2 per participant, with a mean (±SD) of 118 ± 203 mm
2. There was no significant difference between the control and ATD group or between the ATD subgroups regarding the size of the hematoma based on drawings (
Figure 1). One participant in the control group did not provide information on the size of the hematoma and was therefore not included in this analysis.
Overall, 58 individual hematomas were drawn by 35 participants. Accordingly, a mean of 1.6 ± 0.8 [1;4] hematomas occurred per affected participant. The number of hematomas following current BoNT/A injection differed significantly (p = 0.02) between control and ATD groups. Participants in the control group reported a mean of 1.4 ± 0.7 [1;3] individual hematomas, while participants in the ATD group suffered from a mean of 2.0 ±0.9 [1;4] hematomas. However, no significant difference in the number of hematomas after current BoNT/A treatment was observed between ATD subgroups.
2.4. Hematoma Consequence
On a visual analogue scale (VAS) the mean (±SD) impairment caused by the hematoma was reported as 1.4 ± 2.2 [0.0;7.6], with most of the participants (49%, 16/33) feeling completely unaffected (VAS: 0). There was no significant difference between the ATD group (VAS: 1.4 ± 2.3 [0.0;7.0]) and the control group (VAS: 1.4 ± 2.2 [0;7.6.0]) or between ATD subgroups. Cosmetic reasons (21%, 7/33), pain, or a feeling of pressure (9%, 3/33) were given as reasons for the impairment caused by the hematoma. To deal with the disturbing side effects, 27% (10/37) of those affected took further measures such as cooling affected areas (22%, 8/37). Five participants (control: 4; ATD: 1) did not provide information about impairment and were therefore not included in this analysis.
2.5. Non-Hemorrhaghic Side Effects
Regarding past BoNT/A treatments in 84% (118/138) of patients records other side effects than hematoma were noted. The most common were ptosis (34%, 47/139), lacrimation (33%, 46/139), and unspecified visual disturbances (27%, 38/139). For two patients, this information was not available.
Regarding the current BoNT/A treatment, most participants (60%, 74/124) reported no side effects apart from hematoma. The most common included tearing (6%, 7/124) and burning, pain, and dry eye sensation (4% each, 5/124).
3. Discussion
Our study shows that BoNT/A injections for the treatment of BEB and HFS are not associated with more frequent hemorrhagic side effects in patients on ATD, regardless of the agent, than in patients without—both in the retrospective analysis of past BoNT/A treatments and in the prospective survey on current BoNT/A injections. Except the number of single hematomas per patient, there is also no significant difference in the severity of hematomas occurring after BoNT/A treatment between patients on ATD, regardless of the agent, and patients without.
However, the retrospectively determined hematoma frequency of past BoNT/A treatments (HFretro) was significantly lower than of the current BoNT/A injection (HFactual)—both in the overall cohort of participants (p < 0.01) and within the control (p < 0.01) and ATD group (p < 0.01).
Regarding past BoNT/A treatments (HF
retro), overall, a hematoma frequency of 3% was determined. Various studies on the effectiveness and safety of different BoNT/A preparations for the treatment of BEB and HFS revealed comparable results (
Table 4). Bentivoglio et al. (2009) retrospectively determined a hematoma frequency of 3.2% (43/1341) after treatment of BEB [
29]. Jankovic and colleagues (2011) also observed a comparable hematoma frequency in patients with HFS [
30]. In contrast, the hematoma frequency of 25.0% (16/64), determined by Wabbels et al. (2010) was considerably higher and corresponds to HFS
actual (30%) in our study [
31].
The heterogeneous data on frequency of hematoma after BoNT/A treatment within our study and within the literature (
Table 4) could be explained by different study designs. Presumably, small, only briefly visible and non-burdening hematomas are often forgotten and therefore only remembered when asked explicitly and in time, as in the case of determination of HF
actual. In contrast to this, determination of the HF
retro as well as the hematoma frequency in numerous other studies was carried out by an open-ended questioning about side effects of past BoNT/A treatments without particular attention to hemorrhagic complications. In addition, the data collection usually took place several weeks after the treatment in question. It can therefore be assumed that, both in determination of the HF
retro in our study and the hematoma frequency in comparable studies that followed a retrospective study design, fewer hematomas were recorded than actually occurred.
Given the large difference between HFactual and Hfretro, we consider it unlikely that the higher hematoma frequency of current BoNT/A treatments was randomly generated by case number differences (current treatment: n = 125; past treatments: n = 5298). Since participants received the current BoNT/A injection by different physicians, a physician-related increased hematoma frequency can also be ruled out.
To date, very few studies investigated the hematoma frequency after BoNT/A treatment in patients on antithrombiotic medication. Schrader and colleagues (2018) retrospectively determined the hematoma frequency of BoNT/A treatment for BEB, HFS, cervical dystonia and stroke-related spasticity in patients on phenprocoumon. After a total of 231 and 206 BoNT/A treatments for BEB and HFS, respectively, there was no significant difference in hematoma frequency between patients on phenprocoumon and their matched controls (BEB: 5.2% vs. 2.6%; HFS: 3.9% vs. 2.9%). These results largely correspond to the HFretro of the control and VKA group in our study. In contrast, the HFactual of both groups in our study is considerably higher. The comparison of these results confirms the already discussed assumption that an open-ended and delayed questioning of patients, as performed when determining the hematoma frequency in the study of Schrader et al. and the HFretro in our study, underestimates the real hematoma frequency.
Furthermore, Jagatsinh and George (2012) investigated the safety of different BoNT/A preparations for the treatment of spastic disorders on warfarin [
41]. After a total of 103 intramuscular injections, none of the 14 participants registered hemorrhagic complications. The hematoma frequency to be calculated would therefore be 0%, and corresponds to the HF
retro of the VKA group in our study. Again, the HF
actual of the VKA group determined in our study is considerably higher than the hematoma frequency determined by Jagatsinh and George. However, in view of the small number of participants on phenprocoumon in our study, the comparison of the results is only possible to a very limited extent. In addition, the comparability of the study results might be limited by the different pharmacological properties of the VKA warfarin and phenprocoumon [
24,
42,
43,
44].
There are no studies on the frequency of hematomas after BoNT/A treatment on other antithrombotics such as DOAC, ADP-RA or ASA. However, according to the direction for use for the preparations in question, hematomas or bleeding generally after medical interventions and injections or punctures occur “rarely” to “frequently” (≥1/10,000 to <1/10) depending on the respective preparation. This corresponds to a hematoma frequency between ≥0.01% and <10.0%, and is therefore comparable to the HFretro determined in our study to be between 0% (ADP-RA) and 2% (ASA).
4. Conclusions
In view of the results of our study, pausing antithrombotic medication with ASA, VKA or DOAC in the context of BoNT/A treatment for BEB and HFS does not seem justified. However, since only a small number of patients on ADP-RA and DAPT were included in our study, subsequent studies are necessary to be able to make a recommendation for these agents. For future studies, it should be considered that timing and questioning technique may lead to significant differences in the reported frequency and description of hemorrhagic side effects.
Overall, our study showed that hemorrhagic side effects of the BoNT/A treatment for BEB and HFS are mild and non-disabling.
5. Materials and Methods
The study was approved by the local ethics committee of the “Rheinische Friedrichs-Wilhelms-Universität Bonn” and has been performed in accordance with the ethical standards of the Declaration of Helsinki and its later amendments. All participants provided a signed informed consent form for participation in this study. Participation did not affect the patient’s medical care. Antithrombotic treatment was continued as prescribed and therefore was not influenced by the study.
Patients with BEB or HFS undergoing regular treatment with BoNT/A at the University Eye Clinic in Bonn were consecutively included in the study. According to their medication, the participants were assigned to the following study groups: the control group (no intake of antithrombotic drugs), the ATD group (regular intake of antithrombotic drugs), and their subgroups regarding the antithrombotic agent (ASA, ADP-RA, DAPT, DOAC or VKA).
The frequency of hematomas caused by BoNT/A treatment for BEB and HFS was recorded for two separate periods: in a retrospective analysis of past BoNT/A treatments (HFretro), and in a prospective survey on one single BoNT/A treatment (HFactual).
The HFretro was calculated for each participant and each study group from the absolute number of past BoNT/A treatments that caused a hematoma in relation to the total number of BoNT/A treatments in our clinic. Information on adverse events including hematoma following past BoNT/A treatments was collected from patient records. Adverse events are queried in a standardized manner at every follow-up visit in our clinic (about 8–12 weeks after the respective treatment) and documented in the patient file. The patient records were also used to collect data on demographics, diagnosis (BEB or HFS), specifics of the BoNT/A therapy performed in our eye clinic (duration, number of injections administered, type of BoNT/A), comorbidities, and medication.
The HF
actual was calculated for each study group from the number of participants who suffered a hematoma after a single, currently performed BoNT/A treatment in relation to the total number of participants in the group. The mentioned BoNT/A treatment was performed by different physicians according to the patient’s current treatment regimen. In order to ensure that the injection was carried out as usual and without special care, the attending physician was not informed about the patient’s participation in the study. Post-treatment, participants were given a questionnaire to assess the occurrence, size, location, onset, and duration of hematoma, as well as the occurrence of non-hemorrhagic adverse events after this single BoNT/A injection. To assess the hematoma size in an objective way, participants were asked to compare the hematoma to a 1 cent coin (about 1.5 cm in diameter, 207 mm
2), a 2 euro coin (about 2.5 cm in diameter, 520 mm
2) or a quarter of the face. In addition, the area of hematomas drawn in the facial image was calculated by creating representative polygons using the SketchAndClac software (Dobbs, Elliott M. “
www.SketchAndCalc.com” (accessed on 12th November 2021). SketchAndCalc. Elliott M Dobbs, 20 February 2011. Web, version 4.1.8.11.). A visual analogue scale (VAS) ranging from 0 (no impairment) to 10 (worst impairment) was used to assess how much the hematoma bothered the patients. Patients were asked to complete the questionnaire within two weeks of the treatment in question and to return it to our clinic.
Statistical analysis of the pseudonymized data was performed using the statistical program IBM SPSS Statistics, version 26 (IBM Corp., Armonk, NY, USA). Results were expressed as mean, standard deviation, minimum, median, quartiles, and maximum. For determining statistical significance between groups, the Mann-Whitney-Test (control vs. ATD group) and the Kruskall-Wallis-Test (between ATD subgroups) were performed (p < 0.05 considered statistically significant).
Author Contributions
Conception and design of the study, B.W.; data acquisition, F.C.W.; statistical analysis and interpretation of the data, F.C.W. and B.W.; draft of the paper and critical revision, F.C.W. and B.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study has been performed in accordance with the ethical standards of the Declaration of Helsinki and its later amendments, was approved by the local ethics committee of the “Rheinische Friedrichs-Wilhelms-Universität Bonn”(Approved code: 127/19; approved date: 11 June 2019), and all participants provided a signed informed consent form for participation in this study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data and materials can be provided by the authors upon reasonable request. The original data is included in paper files.
Acknowledgments
The authors would like to thank Eva Stetzer for assistance with the preparation of the manuscript.
Conflicts of Interest
F.C.W. has no relevant financial or non-financial interests to disclose. B.W. received travel grants and speaker honoraria from Desitin and Merz and research funding from Allergan and Merz.
References
- Grandas, F.; Elston, J.; Quinn, N.; Marsden, C.D. Blepharospasm: A review of 264 patients. J. Neurol. Neurosurg. Psychiatry 1988, 51, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Havins, W.E.; Wilkins, R.B. Blinking and Blepharospasm. JAMA 1982, 248, 3160–3164. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Orman, J. Blepharospasm: Demographic and clinical survey of 250 patients. Ann. Ophthalmol. 1984, 16, 371–376. [Google Scholar]
- Evalls-Sole, J.; Edefazio, G. Blepharospasm: Update on Epidemiology, Clinical Aspects, and Pathophysiology. Front. Neurol. 2016, 7, 45. [Google Scholar] [CrossRef]
- Abbruzzese, G.; Berardelli, A.; Girlanda, P.; Marchese, R.; Martino, D.; Morgante, F.; Avanzino, L.; Colosimo, C.; Defazio, G. Long-term assessment of the risk of spread in primary late-onset focal dystonia. J. Neurol. Neurosurg. Psychiatry 2008, 79, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Ba, E.M.W.; Hershey, T.; Karimi, M.; Racette, B.; Tabbal, S.D.; Mink, J.W.; Paniello, R.C.; Perlmutter, J.S. Relative risk of spread of symptoms among the focal onset primary dystonias. Mov. Disord. 2006, 21, 1175–1181. [Google Scholar] [CrossRef]
- Defazio, G.; Abbruzzese, G.; Livrea, P.; Berardelli, A. Epidemiology of primary dystonia. Lancet Neurol. 2004, 3, 673–678. [Google Scholar] [CrossRef]
- DeFazio, G.; Berardelli, A.; Hallett, M. Do primary adult-onset focal dystonias share aetiological factors? Brain 2007, 130, 1183–1193. [Google Scholar] [CrossRef]
- Defazio, G.; Hallett, M.; Jinnah, H.A.; Conte, A.; Berardelli, A. Blepharospasm 40 Years Later. Mov. Disord. 2017, 32, 498–509. [Google Scholar] [CrossRef]
- The Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group. A prevalence study of primary dystonia in eight European countries. J. Neurol. 2000, 247, 787–792. [Google Scholar] [CrossRef]
- Digre, K.; Corbett, J.J. Hemifacial spasm: Differential diagnosis, mechanism, and treatment. Adv. Neurol. 1988, 49, 151–176. [Google Scholar] [PubMed]
- Tan, E.K.; Jankovic, J. Bilateral hemifacial spasm: A report of five cases and a literature review. Mov. Disord. 1999, 14, 345–349. [Google Scholar] [CrossRef]
- Wang, A.; Jankovic, J. Hemifacial spasm: Clinical findings and treatment. Muscle Nerve 1998, 21, 1740–1747. [Google Scholar] [CrossRef]
- Wartenberg, R. Hemifacial spasm. Trans. Am. Neurol. Assoc. 1950, 51, 276–277. [Google Scholar] [PubMed]
- Nielsen, V.K. Electrophysiology of the facial nerve in hemifacial spasm: Ectopic/ephaptic excitation. Muscle Nerve 1985, 8, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Adler, C.H.; Zimmerman, R.A.; Savino, P.J.; Bernardi, B.; Bosley, T.M.; Sergott, R.C. Hemifacial spasm: Evaluation by magnetic resonance imaging and magnetic resonance tomographic angiography. Ann. Neurol. 1992, 32, 502–506. [Google Scholar] [CrossRef]
- Gálvez-Jiménez, N.; Hanson, M.R.; Desai, M. Unusual causes of hemifacial spasm. Semin. Neurol. 2001, 21, 75–83. [Google Scholar] [CrossRef]
- Jannetta, P.J.; Abbasy, M.; Maroon, J.C.; Ramos, F.M.; Albin, M.S. Etiology and definitive microsurgical treatment of hemifacial spasm. Operative techniques and results in 47 patients. J. Neurosurg. 1977, 47, 321–328. [Google Scholar] [CrossRef]
- Rosenstengel, C.; Matthes, M.; Baldauf, J.; Fleck, S.; Schroeder, H. Hemifacial spasm: Conservative and surgical treatment options. Dtsch. Arztebl. Int. 2012, 109, 667–673. [Google Scholar] [CrossRef]
- Auger, R.G.; Whisnant, J.P. Hemifacial Spasm in Rochester and Olmsted County, Minnesota, 1960 to 1984. Arch. Neurol. 1990, 47, 1233–1234. [Google Scholar] [CrossRef]
- Nilsen, B.; Le, K.-D.; Dietrichs, E. Prevalence of hemifacial spasm in Oslo, Norway. Neurology 2004, 63, 1532–1533. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Barnes, M.P.; Bhatia, K.P.; Fernandez-Alvarez, E.; Filippini, G.; Gasser, T.; Krauss, J.K.; Newton, A.; Rektor, I.; Savoiardo, M.; et al. A systematic review on the diagnosis and treatment of primary (idiopathic) dystonia and dystonia plus syndromes: Report of an EFNS/MDS-ES Task Force. Eur. J. Neurol. 2006, 13, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Kenney, C.; Jankovic, J. Botulinum toxin in the treatment of blepharospasm and hemifacial spasm. J. Neural Transm. 2007, 115, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Kaltenmaier, M.; Vanselow, K.; Rollnik, J.; Maschke, M. Therapie des essentiellen Blepharospasmus mit Botulinumtoxin. Fortschritte Neurol. Psychiatr. 2019, 87, 355–360. [Google Scholar] [CrossRef]
- Naumann, M.; Jankovic, J. Safety of botulinum toxin type A: A systematic review and meta-analysis. Curr. Med. Res. Opin. 2004, 20, 981–990. [Google Scholar] [CrossRef]
- Favaloro, E.J. Anticoagulant and antithrombotic therapy: Globally applied according to local geographical selection criiteria. Ann. Blood. 2020, 5, 22. [Google Scholar] [CrossRef]
- Antithrombotic Trialists’ (ATT) Collaboration; Baigent, C.; Blackwell, L.; Collins, R.; Emberson, J.; Godwin, J.; Peto, R.; Buring, J.; Hennekens, C.; Kearney, P.; et al. Aspirin in the primary and secondary prevention of vascular disease: Collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009, 373, 1849–1860. [Google Scholar] [CrossRef]
- Paikin, J.S.; Eikelboom, J.W. Aspirin. Circulation 2012, 125, e439-42. [Google Scholar] [CrossRef]
- Bentivoglio, A.R.; Fasano, A.; Ialongo, T.; Soleti, F.; Fermo, S.L.; Albanese, A. Fifteen-Year Experience in Treating Blepharospasm with Botox or Dysport: Same Toxin, Two Drugs. Neurotox. Res. 2009, 15, 224–231. [Google Scholar] [CrossRef]
- Jankovic, J.; Comella, C.; Hanschmann, A.; Grafe, S. Efficacy and safety of incobotulinumtoxinA (NT 201, Xeomin) in the treatment of blepharospasm-A randomized trial. Mov. Disord. 2011, 26, 1521–1528. [Google Scholar] [CrossRef]
- Wabbels, B.; Reichel, G.; Fulford-Smith, A.; Wright, N.; Roggenkämper, P. Double-blind, randomised, parallel group pilot study comparing two botulinum toxin type A products for the treatment of blepharospasm. J. Neural Transm. 2011, 118, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Schrader, C.; Ebke, M.; Saberi, F.A.; Dressler, D. Botulinum toxin therapy in patients with oral anticoagulation: Is it safe? J. Neural Transm. 2017, 125, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Jagatsinh, Y.; George, J. Audit of Safety of Intramuscular Botulinum Toxin Injections among Patients Receiving Warfarin Anticoagulation Therapy. Indian J. Phys. Med. Rehabil. 2012, 23, 101–104. [Google Scholar] [CrossRef]
- Wabbels, B.; Fimmers, R.; Roggenkämper, P. Ultra-Long-Term Therapy of Benign Essential Blepharospasm with Botulinumtoxin A—30 Years of Experience in a Tertiary Care Center. Toxins 2022, 14, 120. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Schwartz, K.; Donovan, D.T. Botulinum toxin treatment of cranial-cervical dystonia, spasmodic dysphonia, other focal dystonias and hemifacial spasm. J. Neurol. Neurosurg. Psychiatry 1990, 53, 633–639. [Google Scholar] [CrossRef]
- Park, Y.C.; Lim, J.K.; Lee, D.K.; Yi, S.D. Botulinum a toxin treatment of hemifacial spasm and blepharospasm. J. Korean Med. Sci. 1993, 8, 334–340. [Google Scholar] [CrossRef]
- Hsiung, G.-Y.; Das Mbbs, S.; Ranawaya, R.; Lafontaine, A.-L.; Suchowersky, O. Long-term efficacy of botulinum toxin A in treatment of various movement disorders over a 10-year period. Mov. Disord. 2002, 17, 1288–1293. [Google Scholar] [CrossRef]
- Cillino, S.; Raimondi, G.; Guépratte, N.; Damiani, S.; Cillino, M.; Di Pace, F.; Casuccio, A. Long-term efficacy of botulinum toxin A for treatment of blepharospasm, hemifacial spasm, and spastic entropion: A multicentre study using two drug-dose escalation indexes. Eye 2009, 24, 600–607. [Google Scholar] [CrossRef]
- Ababneh, O.H.; Cetinkaya, A.; Kulwin, D.R. Long-term efficacy and safety of botulinum toxin A injections to treat blepharospasm and hemifacial spasm. Clin. Exp. Ophthalmol. 2013, 42, 254–261. [Google Scholar] [CrossRef]
- Kollewe, K.; Mohammadi, B.; Köhler, S.; Pickenbrock, H.; Dengler, R.; Dressler, D. Blepharospasm: Long-term treatment with either Botox®, Xeomin® or Dysport®. J. Neural Transm. 2015, 122, 427–431. [Google Scholar] [CrossRef]
- Kelly, J.G.; O’Malley, K. Clinical Pharmacokinetics of Oral Anticoagulants. Clin. Pharmacokinet. 1979, 4, 1–15. Available online: http://link.springer.com/10.2165/00003088-197904010-00001 (accessed on 3 June 2019). [CrossRef] [PubMed]
- Palareti, G.; Legnani, C. Warfarin Withdrawal. Clin. Pharmacokinet. 1996, 30, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Ufer, M. Comparative Pharmacokinetics of Vitamin K Antagonists. Clin. Pharmacokinet. 2005, 44, 1227–1246. [Google Scholar] [CrossRef] [PubMed]
- Lolekha, P.; Choolam, A.; Kulkantrakorn, K. A comparative crossover study on the treatment of hemifacial spasm and blepharospasm: Preseptal and pretarsal botulinum toxin injection techniques. Neurol. Sci. 2017, 38, 2031–2036. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}