Effects of Long-Chain Omega-3 Polyunsaturated Fatty Acids on Endothelial Vasodilator Function and Cognition—Are They Interrelated?



Abstract
:1. Introduction
2. Effects of LCn-3 PUFA Supplementation on Endothelial Vasodilator Function
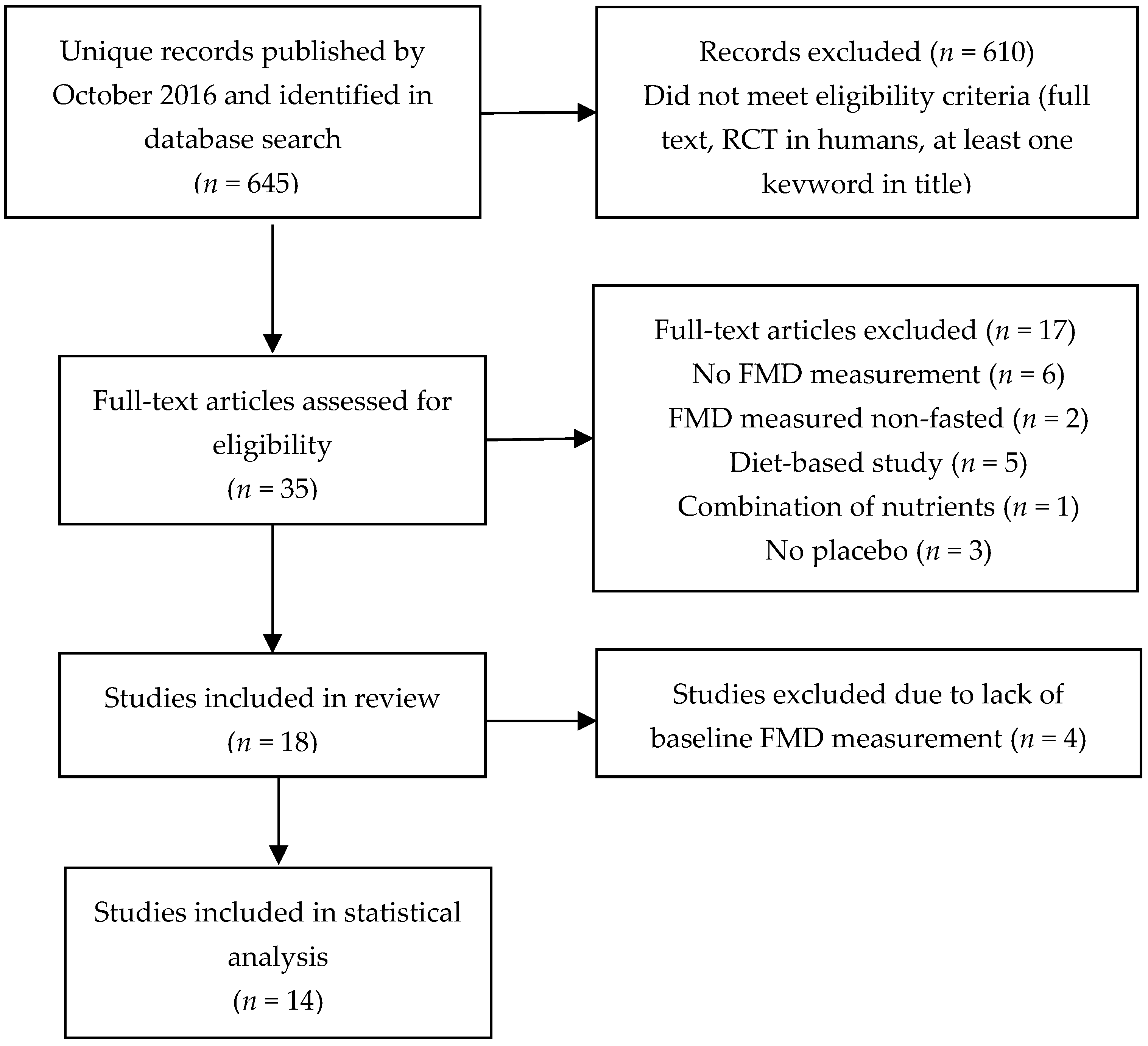
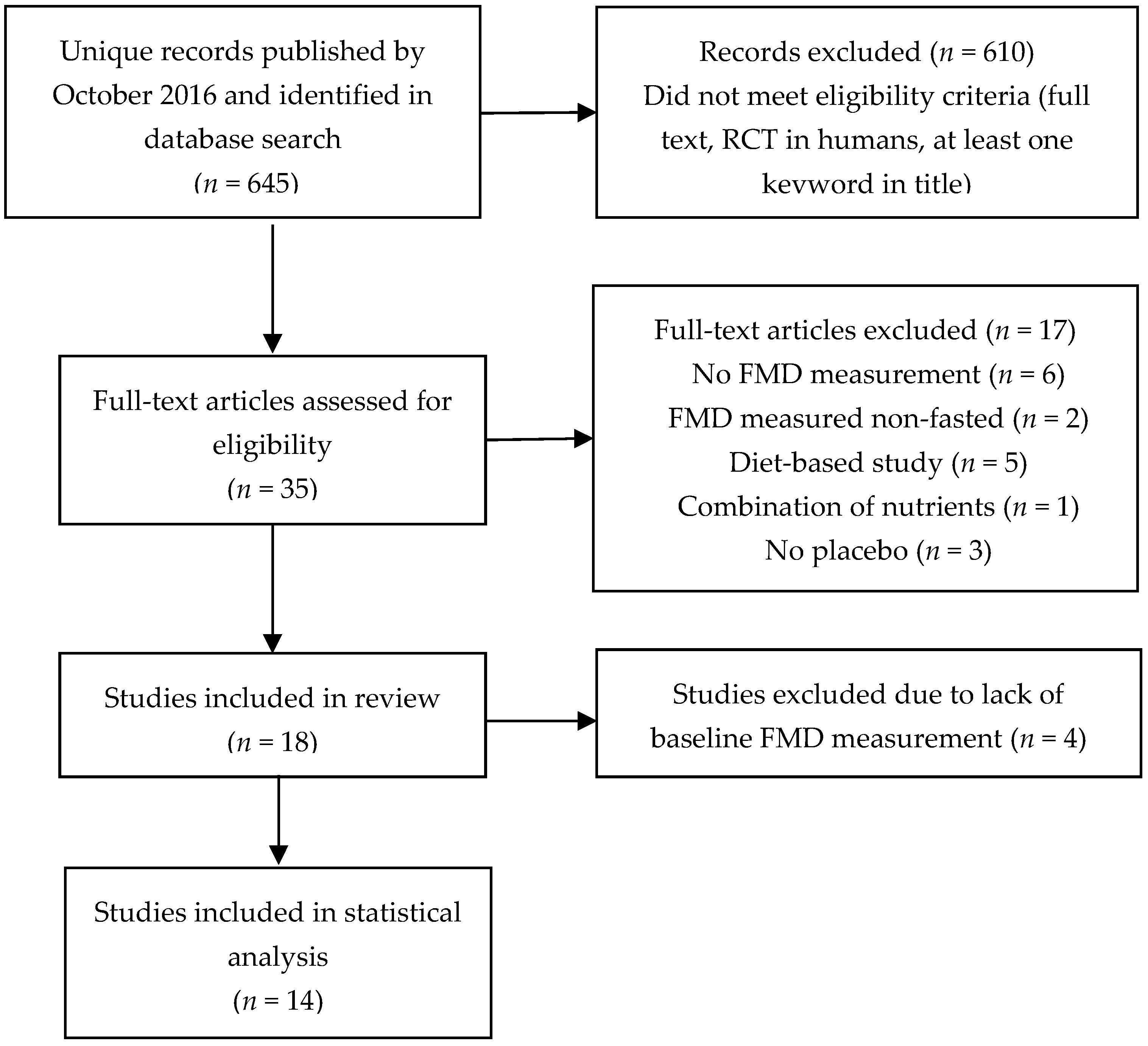
2.1. Literature Search Strategy and Study Selection
2.2. Pooled Analysis
2.3. Results of Statistical Analysis
2.4. Possible Explanations for the Lack of Significant Results
3. Effects of LCn-3 PUFA Supplementation on Cognitive Function
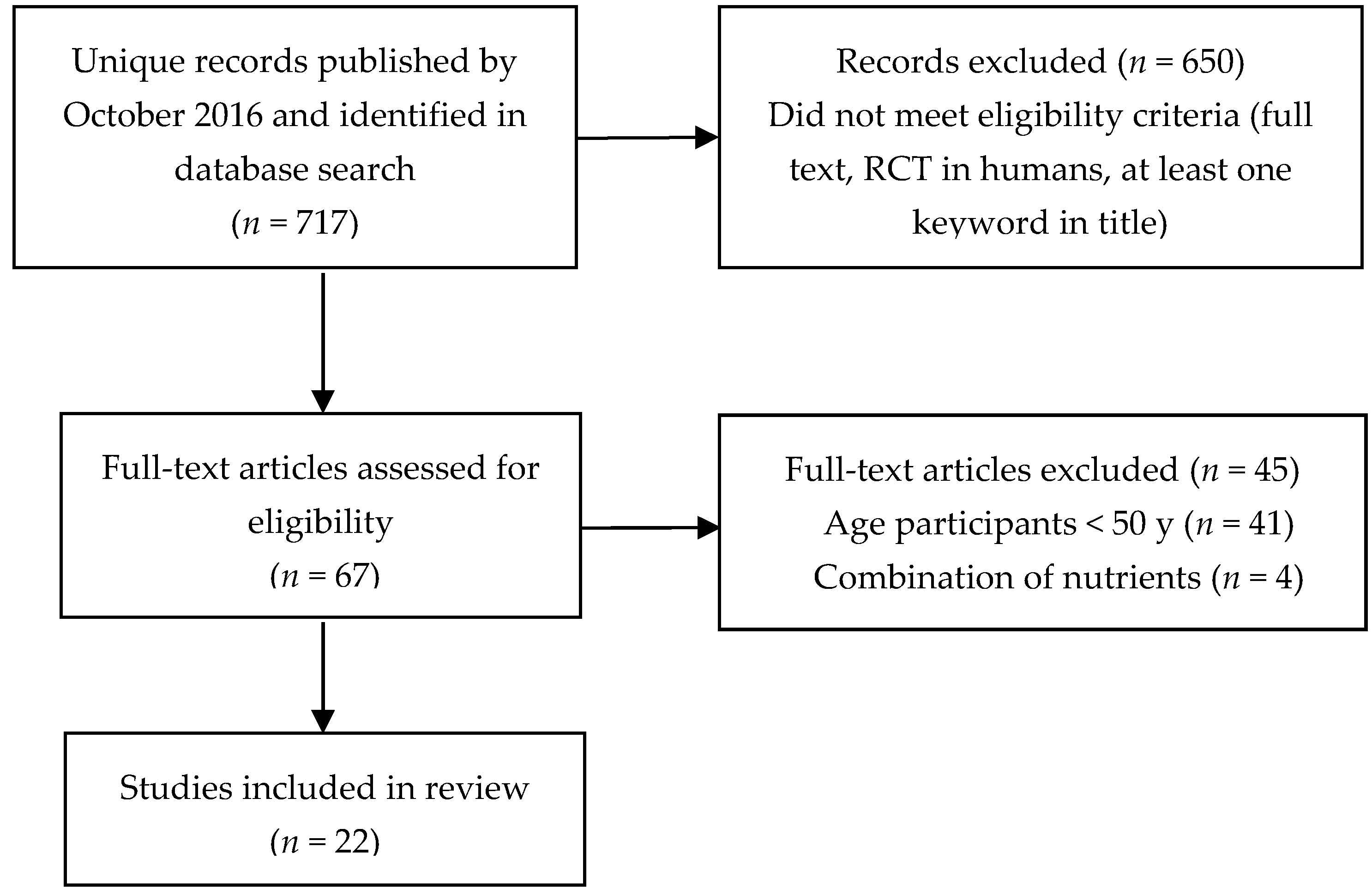
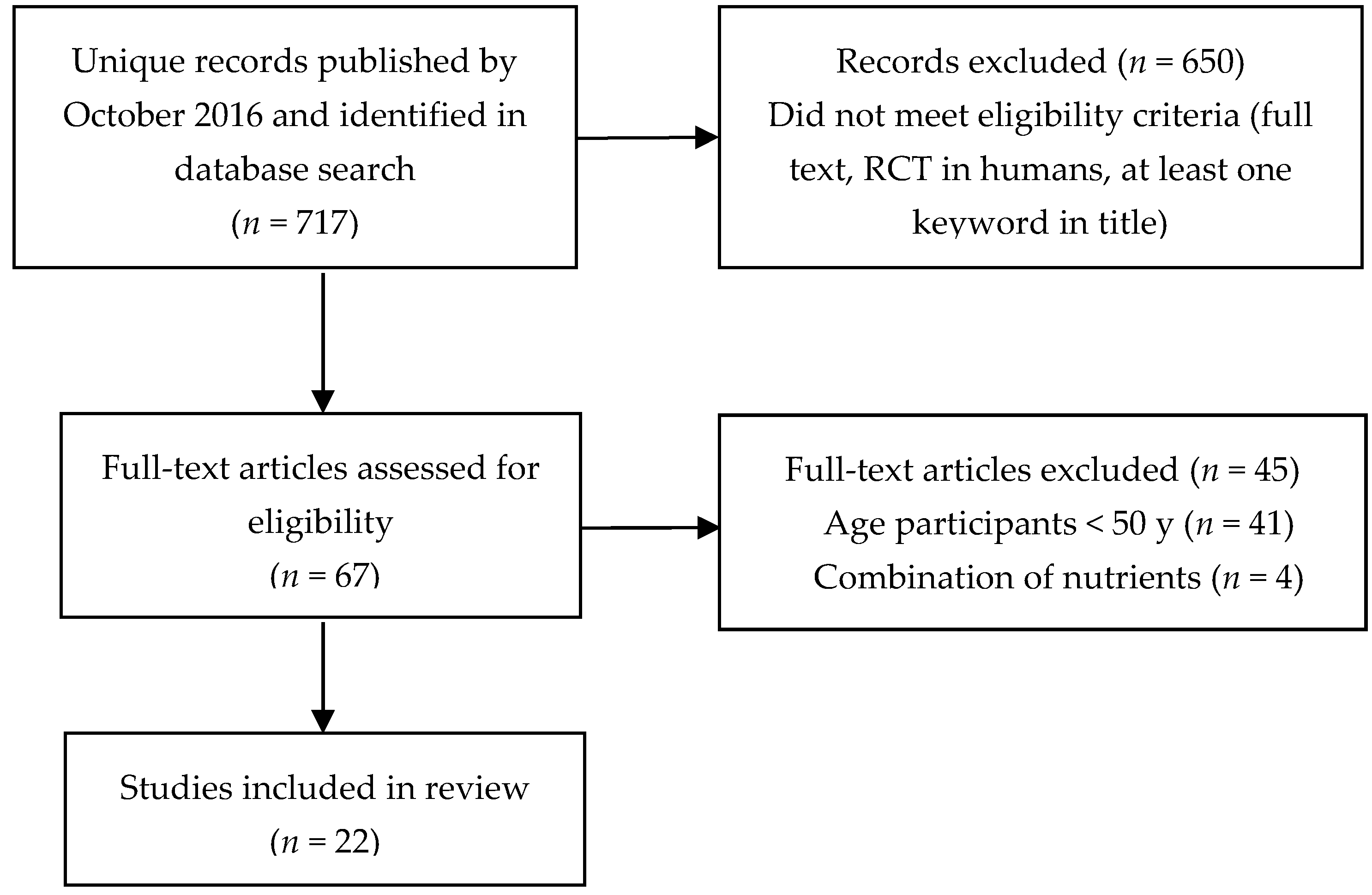
3.1. Literature Search Strategy and Study Selection
3.2. Pooled Analysis
3.3. Results of Statistical Analysis
3.4. Study Limitations
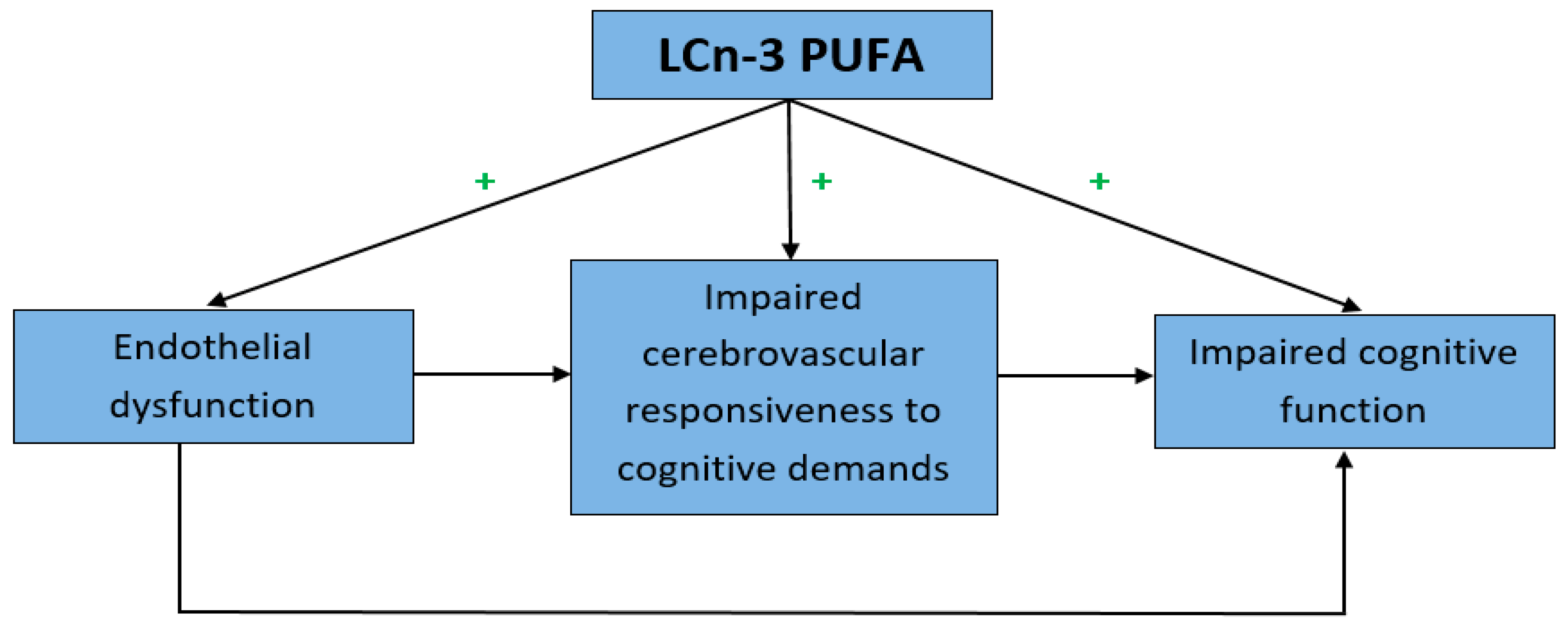
4. Relationship between Endothelial Vasodilator Function and Cognition
4.1. Endothelial Dysfunction and Impaired Cognitive Function
4.2. Decreased Cerebral Blood Flow and Impaired Cognitive Function
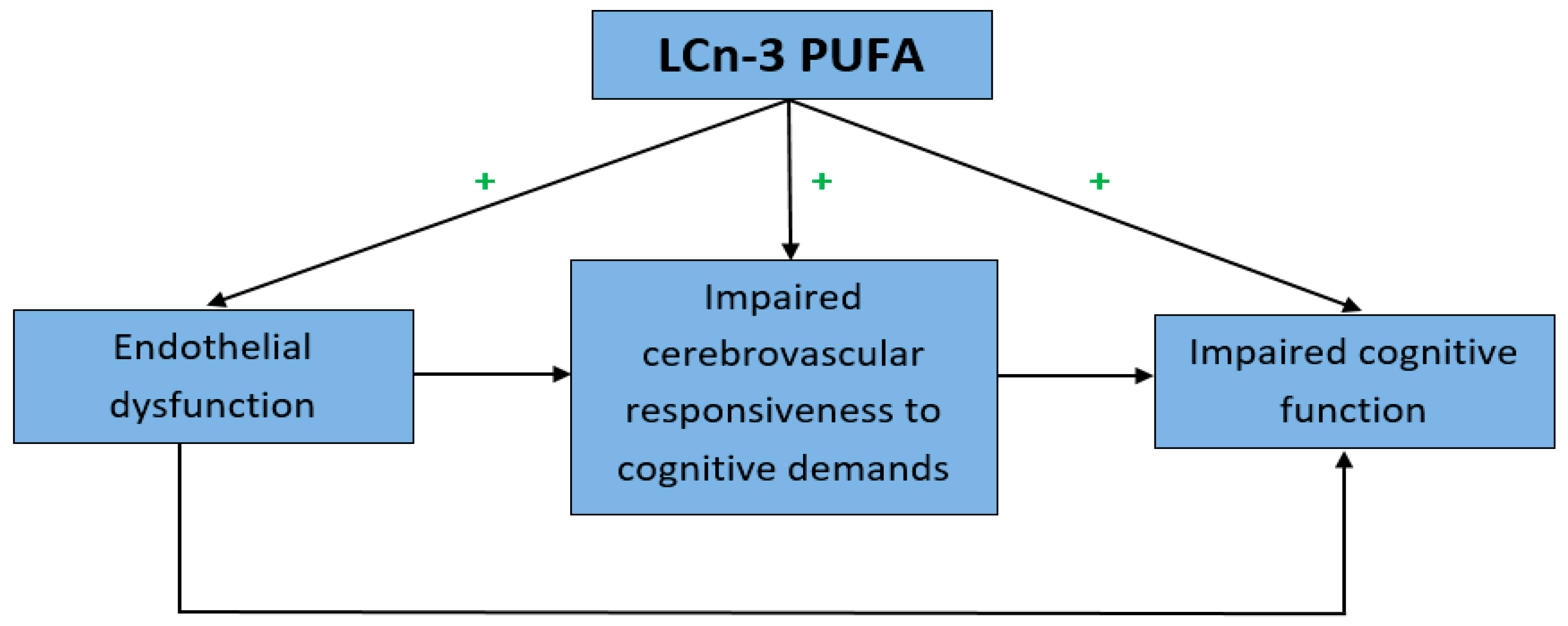
4.3. Decreased Cerebral Blood Flow: A Possible Link between Endothelial Dysfunction and Impaired Cognitive Function?
5. Evidence to Link LCn-3 PUFA, Vasodilator Function and Cognition
5.1. Effects of Vasoactive Nutrients on Brain Function
5.2. Effects of LCn-3 PUFA Supplementation
5.3. Effect of LCn-3 PUFA on Cerebrovascular Function
5.4. Gap in Literature
6. Future Perspective
6.1. Implications for Future Studies
6.2. Testing the Hypothesis of Sinn and Howe
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Dementia in Australia; AIHW: Canberra, Australia, 2012. [Google Scholar]
- Efimova, I.Y.; Efimova, N.Y.; Triss, S.V.; Lishmanov, Y.B. Brain perfusion and cognitive function changes in hypertensive patients. Hypertens. Res. 2008, 31, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, R.J.; Soiza, R.L. Evidence of endothelial dysfunction in the development of Alzheimer’s disease: Is Alzheimer’s a vascular disorder? Am. J. Cardiovasc. Dis. 2013, 3, 197–226. [Google Scholar] [PubMed]
- Ruitenberg, A.; den Heijer, T.; Bakker, S.L.M.; van Swieten, J.C.; Koudstaal, P.J.; Hofman, A.; Breteler, M.M.B. Cerebral hypoperfusion and clinical onset of dementia: The Rotterdam study. Ann. Neurol. 2005, 57, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Perry, G.; Smith, M.A.; Friedland, R.P. Vascular abnormalities: The insidious pathogenesis of Alzheimer’s disease. Neurobiol. Aging 2000, 21, 357–361. [Google Scholar] [CrossRef]
- Sun, Z.W.; Zhu, Y.X.; Liu, H.Y.; Liu, J.; Zhu, X.Q.; Zhou, J.N. Decreased cerebral blood flow velocity in apolipoprotein E epsilon4 allele carriers with mild cognitive impairment. Eur. J. Neurol. 2007, 14, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Cipolla, M.J. The Cerebral Circulation San Rafael; Morgan & Claypool Life Sciences: San Rafael, CA, USA, 2009. [Google Scholar]
- Dunn, K.M.; Nelson, M.T. Neurovascular signaling in the brain and the pathological consequences of hypertension. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1–H14. [Google Scholar] [CrossRef] [PubMed]
- Girouard, H.; Iadecola, C. Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. J. Appl. Physiol. 2006, 100, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Howe, P.R.C. Mental health benefits of omega-3 fatty acids may be mediated by improvements in cerebral vascular function. Biosci. Hypotheses 2008, 1, 103–118. [Google Scholar] [CrossRef]
- Flock, M.R.; Harris, W.S.; Kris-Etherton, P.M. Long-chain omega-3 fatty acids: Time to establish a dietary reference intake. Nutr. Rev. 2013, 71, 692–707. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. The omega-6/omega-3 ratio and dementia or cognitive decline: A systematic review on human studies and biological evidence. J. Nutr. Gerontol. Geriatr. 2013, 32, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Schacky, V. Omega-3 index and cardiovascular disease prevention: Prinicple and rationale. Lipid Technol. 2010, 22, 151–154. [Google Scholar] [CrossRef]
- Van der Wurff, I.S.M.; von Schacky, C.; Berge, K.; Zeegers, M.P.; Kirschner, P.A.; de Groot, R.H.M. Association between blood omega-3 index and cognition in typically developing Dutch adolescents. Nutrients 2016, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Mazereeuw, G.; Lanctot, K.L.; Chau, S.A.; Swardfager, W.; Herrmann, N. Effects of omega-3 fatty acids on cognitive performance: A meta-analysis. Neurobiol. Aging 2012, 33, 1482. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, M.; Grillo, A.; Losurdo, P.; Panizon, E.; Mearelli, F.; Cattin, L.; Barazzoni, R.; Carretta, R. Omega-3 polyunsaturated fatty acids: Structural and functional effects on the vascular wall. BioMed Res. Int. 2015, 2015, 791978. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liang, X.; Wang, L.; Lu, X.; Huang, J.; Cao, J.; Li, H.; Gu, D. Effect of omega-3 fatty acids supplementation on endothelial function: A meta-analysis of randomized controlled trials. Atherosclerosis 2012, 221, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Xin, W.; Wei, W.; Li, X. Effect of fish oil supplementation on fasting vascular endothelial function in humans: A meta-analysis of randomized controlled trials. PLoS ONE 2012, 7, e46028. [Google Scholar] [CrossRef] [PubMed]
- Jackson, P.A.; Forster, J.S.; Bell, J.G.; Dick, J.R.; Younger, I.; Kennedy, D.O. DHA supplementation alone or in combination with other nutrients does not modulate cerebral hemodynamics or cognitive function in healthy older adults. Nutrients 2016, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Jackson, P.A.; Reay, J.L.; Scholey, A.B.; Kennedy, D.O. Docosahexaenoic acid-rich fish oil modulates the cerebral hemodynamic response to cognitive tasks in healthy young adults. Biol. Psychol. 2012, 89, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Konagai, C.; Yanagimoto, K.; Hayamizu, K.; Han, L.; Tsuji, T.; Koga, Y. Effects of krill oil containing n-3 polyunsaturated fatty acids in phospholipid form on human brain function: A randomized controlled trial in healthy elderly volunteers. Clin. Interv. Aging 2013, 8, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Milte, C.; Howe, P.R. Oiling the brain: A review of randomized controlled trials of omega-3 fatty acids in psychopathology across the lifespan. Nutrients 2010, 2, 128–170. [Google Scholar] [CrossRef] [PubMed]
- Engler, M.M.; Engler, M.B.; Malloy, M.; Chiu, E.; Besio, D.; Paul, S.; Stuehlinger, M.; Morrow, J.; Ridker, P.; Rifai, N.; et al. Docosahexaenoic acid restores endothelial function in children with hyperlipidemia: Results from the EARLY study. Int. J. Clin. Pharmacol. Ther. 2004, 42, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.M.; Buckley, J.D.; Murphy, K.J.; Howe, P.R.C. Combining fish-oil supplements with regular aerobic exercise improves body composition and cardiovascular disease risk factors. Am. J. Clin. Nutr. 2007, 85, 1267–1274. [Google Scholar] [PubMed]
- Shah, A.P.; Ichiuji, A.M.; Han, J.K.; Traina, M.; El-Bialy, A.; Meymandi, S.K.; Wachsner, R.Y. Cardiovascular and endothelial effects of fish oil supplementation in healthy volunteers. J. Cardiovasc. Pharmacol. Ther. 2007, 12, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Siasos, G.; Tousoulis, D.; Oikonomou, E.; Zaromitidou, M.; Verveniotis, A.; Plastiras, A.; Kioufis, S.; Maniatis, K.; Miliou, A.; Siasou, Z.; et al. Effects of Omega-3 fatty acids on endothelial function, arterial wall properties, inflammatory and fibrinolytic status in smokers: A cross over study. Int. J. Cardiol. 2013, 166, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Plastiras, A.; Siasos, G.; Oikonomou, E.; Verveniotis, A.; Kokkou, E.; Maniatis, K.; Gouliopoulos, N.; Miliou, A.; Paraskevopoulos, T.; et al. Omega-3 PUFAs improved endothelial function and arterial stiffness with a parallel antiinflammatory effect in adults with metabolic syndrome. Atherosclerosis 2014, 232, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Zebrowska, A.; Mizia-Stec, K.; Mizia, M.; Mizia, M.; Gąsior, Z.; Poprzęcki, S. Omega-3 fatty acids supplementation improves endothelial function and maximal oxygen uptake in endurance-trained athletes. Eur. J. Sport Sci. 2015, 15, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Moertl, D.; Hammer, A.; Steiner, S.; Hutuleac, R.; Vonbank, K.; Berger, R. Dose-dependent effects of omega-3-polyunsaturated fatty acids on systolic left ventricular function, endothelial function, and markers of inflammation in chronic heart failure of nonischemic origin: A double-blind, placebo-controlled, 3-arm study. Am. Heart J. 2011, 161, 915. [Google Scholar] [CrossRef] [PubMed]
- Oh, P.C.; Koh, K.K.; Sakuma, I.; Lim, S.; Lee, Y.; Lee, S.; Lee, K.; Han, S.H.; Shin, E.K. Omega-3 fatty acid therapy dose-dependently and significantly decreased triglycerides and improved flow-mediated dilation, however, did not significantly improve insulin sensitivity in patients with hypertriglyceridemia. Int. J. Cardiol. 2014, 176, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Rizza, S.; Tesauro, M.; Cardillo, C.; Galli, A.; Iantorno, M.; Gigli, F.; Sbraccia, P.; Federici, M.; Quon, M.J.; Lauro, D. Fish oil supplementation improves endothelial function in normoglycemic offspring of patients with type 2 diabetes. Atherosclerosis 2009, 206, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Wright, S.A.; O’Prey, F.M.; McHenry, M.T.; Leahey, W.J.; Devine, A.B.; Duffy, E.M.; Johnston, D.G.; Finch, M.B.; Bell, A.L.; McVeigh, G.E. A randomised interventional trial of omega-3-polyunsaturated fatty acids on endothelial function and disease activity in systemic lupus erythematosus. Ann. Rheum. Dis. 2008, 67, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Dyerberg, J.; Eskesen, D.C.; Andersen, P.W.; Astrup, A.; Buemann, B.; Christensen, J.H.; Clausen, P.; Rasmussen, B.F.; Schmidt, E.B.; Tholstrup, T.; et al. Effects of trans- and n-3 unsaturated fatty acids on cardiovascular risk markers in healthy males. An 8 weeks dietary intervention study. Eur. J. Clin. Nutr. 2004, 58, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Skulas-Ray, A.C.; Kris-Etherton, P.M.; Harris, W.S.; Heuvel, J.P.V.; Wagner, P.R.; West, S.G. Dose-response effects of omega-3 fatty acids on triglycerides, inflammation, and endothelial function in healthy persons with moderate hypertriglyceridemia. Am. J. Clin. Nutr. 2011, 93, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Woodman, R.J.; Mori, T.A.; Burke, V.; Puddeya, I.B.; Bardena, A.; Wattsa, G.F.; Beilina, L.J. Effects of purified eicosapentaenoic acid and docosahexaenoic acid on platelet, fibrinolytic and vascular function in hypertensive type 2 diabetic patients. Atherosclerosis 2003, 166, 85–93. [Google Scholar] [CrossRef]
- Wong, C.-Y.; Yiu, K.-H.; Li, S.-W.; Lee, S.; Tam, S.; Lau, C.-P.; Tse, H.F. Fish-oil supplement has neutral effects on vascular and metabolic function but improves renal function in patients with Type 2 diabetes mellitus. Diabet. Med. J. Br. Diabet. Assoc. 2010, 27, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.A.B.; Hall, W.L.; Maniou, Z.; Lewis, F.; Seed, P.T.; Chowienczyk, P.J. Effect of low doses of long-chain n-3 PUFAs on endothelial function and arterial stiffness: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Hileman, C.O.; Carman, T.L.; Storer, N.J.; Labbato, E.D.; White, C.A.; McComsey, G.A. Omega-3 fatty acids do not improve endothelial function in virologically suppressed HIV-infected men: A randomized placebo-controlled trial. AIDS Res. Hum. Retrovir. 2012, 28, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Bello, K.J.; Fang, H.; Fazeli, P.; Bolad, W.; Corretti, M.; Magder, L.S.; Petri, M. Omega-3 in SLE: A double-blind, placebo-controlled randomized clinical trial of endothelial dysfunction and disease activity in systemic lupus erythematosus. Rheumatol. Int. 2013, 33, 2789–2796. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A.; Lanigan, J.; Storry, C.; Low, S.; Birbara, T.; Lucas, A.; Deanfield, J. Docosahexaenoic acid supplementation, vascular function and risk factors for cardiovascular disease: A randomized controlled trial in young adults. J. Am. Heart Assoc. 2013, 2, e000283. [Google Scholar] [CrossRef] [PubMed]
- Stark, K.D.; Van Elswyk, M.E.; Higgins, M.R.; Weatherford, C.A.; Salem, N. Global survey of the omega-3 fatty acids, docosahexaenoic acid and eicosapentaenoic acid in the blood stream of healthy adults. Prog. Lipid Res. 2016, 63, 132–152. [Google Scholar] [CrossRef] [PubMed]
- Luk, T.H.; Dai, Y.L.; Siu, C.W.; Yiu, K.-H.; Chan, H.-T.; Lee, S.W.L.; Li, S.-W.; Fong, B.; Wong, W.-K.; Tam, S.; et al. Effect of exercise training on vascular endothelial function in patients with stable coronary artery disease: A randomized controlled trial. Eur. J. Prev. Cardiol. 2012, 19, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.; Berry, N.M.; Coates, A.M.; Buckley, J.D.; Bryan, J.; Kunz, I.; Howe, P.R.C. Chronic resveratrol consumption improves brachial flow-mediated dilatation in healthy obese adults. J. Hypertens. 2013, 31, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Phang, M.; Sinclair, A.J.; Lincz, L.F.; Garga, M.L. Gender-specific inhibition of platelet aggregation following omega-3 fatty acid supplementation. Nutr. Metab. Cardiovasc. Dis. NMCD 2012, 22, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.J. Prognostic significance of brachial flow-mediated vasodilation. Circulation 2007, 115, 2373–2375. [Google Scholar] [CrossRef] [PubMed]
- Dede, D.S.; Yavuz, B.; Yavuz, B.B.; Cankurtaran, M.; Halil, M.; Ulger, Z.; Cankurtaran, E.S.; Aytemir, K.; Kabakci, G.; Ariogul, S. Assessment of endothelial function in Alzheimer’s disease: Is Alzheimer’s disease a vascular disease? J. Am. Geriatr. Soc. 2007, 55, 1613–1617. [Google Scholar] [CrossRef] [PubMed]
- Vendemiale, G.; Romano, A.D.; Dagostino, M.; Dagostino, M.; de Matthaeis, A.; Serviddio, G. Endothelial dysfunction associated with mild cognitive impairment in elderly population. Aging Clin. Exp. Res. 2013, 25, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.X.; Howe, P.R.C.; Coates, A.M.; Buckley, J.D.; Berry, N.M. Chronic consumption of a wild green oat extract (Neuravena) improves brachial flow-mediated dilatation and cerebrovascular responsiveness in older adults. J. Hypertens. 2013, 31, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Freund-Levi, Y.; Eriksdotter-Jonhagen, M.; Cederholm, T.; Cederholm, T. Omega-3 fatty acid treatment in 174 patients with mild to moderate Alzheimer disease: OmegAD study: A randomized double-blind trial. Arch. Neurol. 2006, 63, 1402–1408. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Schwichtenberg, K.A.; Hanson, N.Q.; Tsai, M.Y. Incorporation and clearance of omega-3 fatty acids in erythrocyte membranes and plasma phospholipids. Clin. Chem. 2006, 52, 2265–2272. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.-C.; Su, K.-P.; Cheng, T.C.; Cheng, T.C.; Liu, H.-C.; Chang, C.-J.; Dewey, M.E.; Stewart, R.; Huang, S.-Y. The effects of omega-3 fatty acids monotherapy in Alzheimer’s disease and mild cognitive impairment: A preliminary randomized double-blind placebo-controlled study. Prog. Neuro-Psychopharmacol. Boil. Psychiatry 2008, 32, 1538–1544. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.J.; McDonald, K.; Caldarella, S.M.; Chung, H.Y.; Troen, A.M.; Snodderly, D.M. Cognitive findings of an exploratory trial of docosahexaenoic acid and lutein supplementation in older women. Nutr. Neurosci. 2008, 11, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Kulzow, N.; Witte, A.V.; Kerti, L.; Grittner, U.; Schuchardt, J.P.; Hahn, A.; Flöel, A. Impact of Omega-3 Fatty Acid Supplementation on Memory Functions in Healthy Older Adults. J. Alzheimers Dis. JAD 2016, 51, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Radeborg, K.; Salo, I.; Björck, I. Effects of supplementation with n-3 polyunsaturated fatty acids on cognitive performance and cardiometabolic risk markers in healthy 51 to 72 years old subjects: A randomized controlled cross-over study. Nutr. J. 2012, 11, 99. [Google Scholar] [CrossRef] [PubMed]
- Strike, S.C.; Carlisle, A.; Gibson, E.L.; Dyall, S.C. A high omega-3 fatty acid multinutrient supplement benefits cognition and mobility in older women: A randomized, double-blind, placebo-controlled pilot study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, H.; Sueyasu, T.; Kontani, M.; Kawashima, H.; Shibata, H.; Koga, Y. Low doses of long-chain polyunsaturated fatty acids affect cognitive function in elderly Japanese men: A randomized controlled trial. J. Oleo Sci. 2015, 64, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Witte, A.V.; Kerti, L.; Hermannstadter, H.M.; Fiebach, J.B.; Schreiber, S.J.; Schuchardt, J.P.; Hahn, A.; Flöel, A. Long-chain omega-3 fatty acids improve brain function and structure in older adults. Cereb. Cortex 2014, 24, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Yurko-Mauro, K.; McCarthy, D.; Rom, D.; Nelson, E.B.; Ryan, A.S.; Blackwell, A.; Salem, N.; Stedman, M.; MIDAS Investigators. Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimers Dement. J. Alzheimers Assoc. 2010, 6, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Eriksdotter, M.; Vedin, I.; Falahati, F.; Freund-Levi, Y.; Hjorth, E.; Faxen-Irving, G.; Wahlund, L.O.; Schultzberg, M.; Basun, H.; Cederholm, T.; et al. Plasma fatty acid profiles in relation to cognition and gender in Alzheimer’s Disease patients during oral omega-3 fatty acid supplementation: The OmegAD study. J. Alzheimers Dis. JAD 2015, 48, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.K.; Shahar, S.; Chin, A.V.; Yusoff, N.A. Docosahexaenoic acid-concentrated fish oil supplementation in subjects with mild cognitive impairment (MCI): A 12-month randomised, double-blind, placebo-controlled trial. Psychopharmacology 2013, 225, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Sinn, N.; Milte, C.M.; Street, S.J.; Buckley, J.D.; Coates, A.M.; Petkov, J.; Howe, P.R.C. Effects of n-3 fatty acids, EPA v. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: A 6-month randomised controlled trial. Br. J. Nutr. 2012, 107, 1682–1693. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.P.; Miao, R.; Li, Q.; Wu, T.; Ma, F. Effects of DHA supplementation on hippocampal volume and cognitive function in older adults with mild cognitive impairment: A 12-month randomized, double-blind, placebo-controlled trial. J. Alzheimers Dis. 2017, 55, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A. Omega-3s and Cognition: Dosage Matters; Global Organization for EPA and DHA Omega-3s: Salt Lake City, UT, USA, 2015. [Google Scholar]
- Quinn, J.F.; Raman, R.; Thomas, R.G.; Yurko-Mauro, K.; Nelson, E.B.; Van Dyck, C.; Galvin, J.E.; Emond, J.; Jack, C.R., Jr.; Weiner, M.; et al. Docosahexaenoic acid supplementation and cognitive decline in Alzheimer disease: A randomized trial. JAMA 2010, 304, 1903–1911. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y.; Clemons, T.E.; Agron, E.; Launer, L.J.; Grodstein, F.; Bernstein, P.S.; Age-Related Eye Disease Study 2 (AREDS2) Research Group. Effect of omega-3 fatty acids, lutein/zeaxanthin, or other nutrient supplementation on cognitive function: The AREDS2 randomized clinical trial. JAMA 2015, 314, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Dangour, A.D.; Allen, E.; Elbourne, D.; Fasey, N.; Fletcher, A.E.; Hardy, P.; Holder, G.E.; Knight, R.; Letley, L.; Richards, M.; Uauy, R. Effect of 2-y n-3 long-chain polyunsaturated fatty acid supplementation on cognitive function in older people: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2010, 91, 1725–1732. [Google Scholar] [CrossRef] [PubMed]
- Pase, M.P.; Grima, N.; Cockerell, R.; Stough, C.; Scholey, A.; Sali, A.; Pipingas, A. The effects of long-chain omega-3 fish oils and multivitamins on cognitive and cardiovascular function: A randomized, controlled clinical trial. J. Am. Coll. Nutr. 2015, 34, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Dullemeijer, C.; Olderikkert, M.G.; Beekman, A.T.; de Groot, C.P. Effect of fish oil on cognitive performance in older subjects: A randomized, controlled trial. Neurology 2008, 71, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Stough, C.; Downey, L.; Silber, B.; Lloyd, J.; Kure, C.; Wesnes, K.; Camfield, D. The effects of 90-day supplementation with the omega-3 essential fatty acid docosahexaenoic acid (DHA) on cognitive function and visual acuity in a healthy aging population. Neurobiol. Aging 2012, 33, 824. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.A.; Childs, C.E.; Calder, P.C.; Rogers, P.J. No effect of omega-3 fatty acid supplementation on cognition and mood in individuals with cognitive impairment and probable Alzheimer’s Disease: A randomised controlled trial. Int. J. Mol. Sci. 2015, 16, 24600–24613. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Y.J.; Zhang, M.; Xu, Z.Q.; Gao, C.Y.; Fang, C.Q.; Yan, J.C.; Zhou, H.D.; Chongqing Ageing Study Group. Vascular risk factors promote conversion from mild cognitive impairment to Alzheimer disease. Neurology 2011, 76, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.E.; Cohen, R.A.; Hoth, K.F.; Haley, A.P.; Poppas, A.; Moser, D.J.; Gunstad, J.; Paul, R.H.; Jefferson, A.L.; Tate, D.F.; et al. Vascular Health and Cognitive Function in Older Adults with Cardiovascular Disease. Artery Res. 2008, 2, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Gunstad, J.; Jerskey, B.A.; Xu, X.; Clark, U.S.; Hassenstab, J.; Cote, D.M.; Walsh, E.G.; Labbe, D.R.; Hoge, R.; et al. The adverse effects of reduced cerebral perfusion on cognition and brain structure in older adults with cardiovascular disease. Brain Behav. 2013, 3, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Jennings, J.R.; Muldoon, M.F.; Ryan, C.; Price, J.C.; Greer, P.; Sutton-Tyrrell, K.; van der Veen, F.M.; Meltzer, C.C. Reduced cerebral blood flow response and compensation among patients with untreated hypertension. Neurology 2005, 64, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.R.; Kozberg, M.G.; Bouchard, M.B.; Shaik, M.A.; Hillman, E.M. A critical role for the vascular endothelium in functional neurovascular coupling in the brain. J. Am. Heart Assoc. 2014, 3, e000787. [Google Scholar] [CrossRef] [PubMed]
- Lavi, S.; Gaitini, D.; Milloul, V.; Jacob, G. Impaired cerebral CO2 vasoreactivity: Association with endothelial dysfunction. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H1856–H1861. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, A.L.; Thompson, M. Cardiovascular disease and cognitive aging. In Chronic Medical Disease and Cognitive Aging; Yaffe, K., Ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Zeevi, N.; Pachter, J.; McCullough, L.D.; Wolfson, L.; Kuchel, G.A. The blood-brain barrier: Geriatric relevance of a critical brain-body interface. J. Am. Geriatr. Soc. 2010, 58, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, H.; Mu, H.; Zhu, W.; Jiang, X.; Hu, X.; Shi, Y.; Leak, R.K.; Dong, Q.; Chen, J.; et al. Omega-3 polyunsaturated fatty acids mitigate blood-brain barrier disruption after hypoxic-ischemic brain injury. Neurobiol. Dis. 2016, 91, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Galle, J.; Quaschning, T.; Seibold, S.; Wanner, C. Endothelial dysfunction and inflammation: What is the link? Kidney Int. Suppl. 2003, 63, S45–S49. [Google Scholar] [CrossRef] [PubMed]
- Sartori, A.C.; Vance, D.E.; Slater, L.Z.; Crowe, M. The impact of inflammation on cognitive function in older adults: Implications for healthcare practice and research. J. Neurosci. Nurs. 2012, 44, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.; Howe, P.R.; Buckley, J.D.; Coates, A.M.; Kunz, I.; Berry, N.M. Acute resveratrol supplementation improves flow-mediated dilatation in overweight/obese individuals with mildly elevated blood pressure. Nutr. Metab. Cardiovasc. Dis. NMCD 2011, 21, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.M.; Howe, P.R.; Wong, R.H. Effects of Resveratrol on Cognitive Performance, Mood and Cerebrovascular Function in Post-Menopausal Women; A 14-Week Randomised Placebo-Controlled Intervention Trial. Nutrients 2017, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Njike, V.Y.; Millet, J.; Dutta, S.; Doughty, K.; Treu, J.A. Effects of walnut consumption on endothelial function in type 2 diabetic subjects: A randomized controlled crossover trial. Diabetes Care 2010, 33, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Nunez, I.; Perez-Heras, A.; Serra, M.; Gilabert, R.; Casals, E.; Deulofeuet, R. A walnut diet improves endothelial function in hypercholesterolemic subjects: A randomized crossover trial. Circulation 2004, 109, 1609–1614. [Google Scholar] [CrossRef] [PubMed]
- Barbour, J.A.; Howe, P.R.; Buckley, J.D.; Bryan, J.; Coates, A.M. Cerebrovascular and cognitive benefits of high-oleic peanut consumption in healthy overweight middle-aged adults. Nutr. Neurosci. 2016. [Google Scholar] [CrossRef] [PubMed]
- Oveisgharan, S.; Hachinski, V. Hypertension, executive dysfunction, and progression to dementia: The Canadian study of health and aging. Arch. Neurol. 2010, 67, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Cukierman, T.; Gerstein, H.C.; Williamson, J.D. Cognitive decline and dementia in diabetes—systematic overview of prospective observational studies. Diabetologia 2005, 48, 2460–2469. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, E.; Kloppenborg, R.P.; Kessels, R.P.; Kappelle, L.J.; Biessels, G.J. Type 2 diabetes mellitus, hypertension, dyslipidemia and obesity: A systematic comparison of their impact on cognition. Biochim. Biophys. Acta 2009, 1792, 470–481. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Reference | Year | Participants | Sample Size | Male/Female (%) | Intervention | Dose EPA/DHA (mg) | Duration (Weeks) | Baseline FMD (%) | Absolute Change in FMD * (%) | Outcomes | Baseline Omega-3 Index? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cross-over study design | |||||||||||
| Engler et al. (USA) [23] | 2004 | Children with FH or FCH, aged 9–19 years | 20 | NR | 1200 mg/day DHA or placebo (corn oil) | 0/1200 | 6 each, 6 weeks wash-out | 6.3 | 1.1 | Significantly increased FMD compared to placebo (p = 0.012) | No |
| Skulas-Ray et al. (USA) [34] | 2010 | Healthy adults with moderately elevated triglycerides, average age 44 years | 26 | 88:12 | 850 mg/day or 3400 mg/day LCn-3 PUFA or placebo (corn oil) | 465/375 | 8 each, 6 weeks wash-out | NR | NR | No significant difference in FMD between treatment and placebo group (p = 0.11) | Yes Low |
| 1860/1500 | |||||||||||
| Siasos et al. (Greece) [26] | 2013 | Healthy smokers, average age 28 years | 20 | 65:35 | 1680 mg/day LCn-3 PUFA or placebo | 920/760 | 12 each, 4 weeks wash-out | 7.3 | 3.0 | Significantly increased FMD compared to placebo (p < 0.05) | No |
| Tousoulis et al. (Greece) [27] | 2014 | Adults with metabolic syndrome, average age 44 years | 29 | 52:48 | 1680 mg/day LCn-3 PUFA or placebo | 920/760 | 12 each, 4 weeks wash-out | 3.7 | 4.2 | Significantly increased FMD compared to placebo (p < 0.001) | No |
| Zebrowska et al. (Poland) [28] | 2015 | Healthy endurance-trained male athletes, average age 23 years | 13 | 100:0 | 1100 mg/day LCn-3 PUFA or placebo (lactose) | 660/440 | 3 each, 2 weeks wash-out | 10.3 | 5.2 | Significantly increased FMD compared to placebo (p < 0.050) | No |
| Parallel study design | |||||||||||
| Woodman et al. (Australia) [35] | 2003 | Adults with type 2 diabetes and hypertension, average age 61 years | 30 | 76:24 | 4000 mg/day EPA or DHA or placebo (olive oil) | 4000/0 | 6 | 3.1 | −0.6 | No significant difference in FMD between treatment (EPA and DHA) and placebo group | No |
| 0/4000 | |||||||||||
| Dyerberg et al. (Denmark) [33] | 2004 | Healthy males, average age 38 years | 50 | 100:0 | 4000 mg/day LCn-3 PUFA or placebo | NR | 8 | NR | NR | No significant difference in FMD between treatment and placebo group | No |
| Hill et el. (Australia) [24] | 2007 | Overweight adults with ≥1 CVD risk factor, average age 52 years | 35 | 39:63 | 1920 mg/day LCn-3 PUFA or placebo (sunflower oil) | 360/1560 | 12 | NR | NR | Significantly increased FMD compared to placebo (p < 0.010) | Yes Moderate |
| Shah et al. (USA) [25] | 2007 | Healthy adults, average age 32 years | 26 | 65:35 | 500 mg/day LCn-3 PUFA or placebo (corn oil) | 300/200 | 2 | NR | NR | Significantly increased FMD within the treatment group (p = 0.036), no comparison to placebo | No |
| Wright et al. (UK) [32] | 2008 | Adults with SLE, average age 48 years | 60 | 7:93 | 3000 mg/day LCn-3 PUFA or placebo (olive oil) | 1800/1200 | 24 | 3.0 | 5.6 | Significantly increased FMD within the treatment group (p < 0.001), no comparison to placebo; significant positive correlation between FMD and % DHA (p = 0.002) and % EPA (p = 0.026) | No Platelet FA very low |
| Rizza et al. (Italy) [31] | 2009 | Healthy adults (OPD), average age 30 years | 50 | 50:50 | 1700 mg/day LCn-3 PUFA or placebo (olive oil) | 1020/680 | 12 | 7.9 | 4.0 | Significantly increased FMD compared to placebo (p < 0.010) | No |
| Wong et al. (China) [36] | 2010 | Adults with type 2 diabetes, average age 60 years | 97 | 44:56 | 2680 mg/day LCn-3 PUFA or placebo (olive oil) | 1680/1000 | 12 | 3.0 | 0.4 | No significant difference in FMD between treatment and placebo group (p = 0.830) | No |
| Moertl et al. (Austria) [29] | 2011 | Adults with severe, nonischemic HF, average age 59 years | 43 | 86:14 | 840 or 3360 mg/day LCn-3 PUFA or placebo (gelatine) | 465/375 | 12 | 8.4 | 3.3 | Within treatment group: 840 mg: trend to increase FMD (p = 0.070) | No |
| 1860/1500 | 3360 mg: increase in FMD (p = 0.010) No comparison with placebo | ||||||||||
| Sanders et al. (UK) [37] | 2011 | Healthy adults, average age 55 years | 312 | 39:61 | 450, 900 or 1800 mg/day LCn-3 PUFA or placebo (olive oil) | 270/180 | 48 | 5.2 | −0.6 | No significant difference in FMD between treatment (all concentrations) and placebo group (p = 0.781) | Yes Moderate |
| 540/360 | |||||||||||
| 1080/720 | |||||||||||
| Hileman et al. (USA) [38] | 2012 | HIV infected males with moderate CVD risk, average age 51 years | 35 | 100:0 | 1660 mg/day LCn-3 PUFA or placebo | 930/730 | 24 | 3.2 | −1.6 | No significant difference in FMD between treatment and placebo group (p = 0.210) | No |
| Bello et al. (USA) [39] | 2013 | Adults with SLE, average age 47 years | 85 | 9:81 | 3000 mg/day LCn-3 PUFA or placebo (corn starch) | 1800/1200 | 12 | 12.5 | −0.1 | No significant difference in FMD between treatment and placebo group (p = 0.380) | No |
| Singhal et al. (UK) [40] | 2013 | Healthy adults, average age 28 years | 274 | 40:60 | 1600 mg/day DHA or placebo (olive oil) | 0/1600 | 16 | 8.4 | −0.8 | No significant difference in FMD between treatment and placebo group (p = 0.200) | Yes Moderate |
| Oh et al. (South Korea) [30] | 2014 | Healthy adults with hyperglyceridemia, average age 55 years | 173 | 53:47 | 1000, 2000 or 4000 mg/day LCn-3 PUFA or placebo | Not specified | 8 | 5.8 | 2.0 | All LCn-3 PUFA concentrations significantly increased FMD compared to placebo (p < 0.050) | No |
| Reference | Year | Participants | Sample Size | Male/Female (%) | Intervention | Dose EPA/DHA (mg) | Design and Duration | Outcomes | Baseline Omega-3 Index? |
|---|---|---|---|---|---|---|---|---|---|
| Non-cognitively impaired | |||||||||
| Johnson et al. (USA) [52] | 2008 | Healthy women, average age 68 years | 24 | 0:100 | 800 mg/day DHA or placebo | 0/800 | Parallel-group, 4 months | Within treatment group: significantly improved verbal fluency (p = 0.030) | No |
| Van de Rest et al. (Netherlands) [68] | 2008 | Healthy adults, average age 70 years | 300 | 55:45 | 400 or 1800 mg/day LCn-3 PUFA or placebo (sunflower oil) | 226/176 | Parallel-group, 6.5 months | No significant effect on any cognitive domains | No |
| 1093/847 | Plasma FA: very low | ||||||||
| Dangour et al. (UK) [66] | 2010 | Healthy adults, average age 75 years | 744 | 55:45 | 700 mg/day LCn-3 PUFA or placebo (olive oil) | 200/500 | Parallel-group, 24 months | No significant effect on any cognitive domains | No |
| Nilsson et al. (Sweden) [54] | 2012 | Healthy adults, average age 63 years | 38 | 30:70 | 2550 mg/day LCn-3 PUFA or placebo | 1500/1050 | CO, 5 weeks each with 5 week wash-out | Significantly improved word memory test performance at 60 min compared to placebo (p = 0.040) | No |
| Stough et al. (UK) [69] | 2012 | Healthy adults, aged 45–77 years | 74 | 42:58 | 312 mg/day LCn-3 PUFA or placebo (soybean oil) | 252/60 | Parallel-group, 3 months | No significant effect on CDR cognitive outcomes measure compared to placebo | No Plasma PL: moderate |
| Konagai et al. (Japan) [21] | 2013 | Healthy men, average age 67 years | 42 | 100:0 | Krill oil, sardine oil or placebo (medium-chain triglycerides) | Krill oil: 193/92 | Parallel-group, 3 months | Krill oil significantly decreased P300 latency compared to placebo (p = 0.030) | No Plasma FA in µg/mL |
| Sardine oil: 491/251 | |||||||||
| Witte et al. (Germany) [57] | 2014 | Healthy adults, average age 64 years | 65 | 54:46 | 2200 mg/day LCn-3 PUFA + 15 mg vitamin E or placebo (sunflower oil) | 1320/880 | Parallel-group, 6.5 months | Significantly improved executive functions (26%, p = 0.005) compared to placebo, improvements in verbal fluency correlated with increase in EPA content (p = 0.009) | Yes Adequate |
| Chew et al. (USA) [65] | 2015 | Healthy adults, average age 73 years | 2461 | 43:57 | 1000 mg/day LCn-3 PUFA + combination of vitamins or placebo | 650/350 | Parallel-group, 5 years | No significant effect on composite cognitive function score (p = 0.630) | No |
| Pase et al. (Australia) [67] | 2015 | Healthy adults, average age 59 years | 70 | 46:54 | 960 mg/day LCn-3 PUFA or placebo (Sunola oil) | 480/480 | Parallel-group, 4 months | Increase in omega 3/6 ratio associated with improvement in spatial working memory response time (p < 0.050) | Yes Low |
| Tokuda et al. (Japan) [56] | 2015 | Healthy men, average age 60 years | 69 | 100:0 | 400 mg/day LCn-3 PUFA or placebo (olive oil) | 100/300 | Parallel-group, 1 month | P300 latency significantly lower compared to placebo (p = 0.013) | No Plasma PL: adequate |
| Kulzow et al. (Germany) [53] | 2016 | Healthy adults, average age 62 years | 42 | 52:48 | 2200 mg/day LCn-3 PUFA + 15 mg vitamin E or placebo (sunflower oil) | 1320/880 | Parallel-group, 6.5 months | Significantly improved recall of correct object-location-associations compared to placebo (p = 0.049) | Yes Adequate |
| Strike et al. (UK) [55] | 2016 | Healthy women, aged 60–84 years | 27 | 0:100 | 1160 mg/day LCn-3 PUFA combined with multi-nutrients or placebo (oil blend) | 160/1000 | Parallel-group, 6 months | Within treatment group: significantly improved MOT latency (p = 0.038) and VRM immediate free recall (p = 0.029) | No |
| Cognitively impaired | |||||||||
| Freund-Levi et al. (Sweden) [49] | 2006 | Adults with mild to moderate AD, average age 73 years | 174 | 48:52 | 2300 mg/day LCn-3 PUFA or placebo (corn oil) | 600/1700 | Parallel-group, 6 months | No significant effect on ADAS-Cog, MMSE or CDR scale Subgroup of very mild cognitive dysfunction: significant reduction in MMSE decline rate (p < 0.050) | No Plasma FA: moderate |
| Chiu et al. (Taiwan) [51] | 2008 | Adults with MCI or mild to moderate AD, average age 75 years | 29 | 44:56 | 1800 mg/day LCn-3 PUFA or placebo (olive oil) | 1080/720 | Parallel-group, 6 months | Higher % EPA associated with better ADAS-cog scores (p = 0.003), Subgroup: adults with MCI treated with LCn-3 PUFA had an improved ADAs-cog score, compared to placebo (p = 0.030) | Yes Moderate |
| Quinn et al. (USA) [64] | 2010 | Adults with mild to moderate AD, average age 76 years | 264 | 48:52 | 1000 mg/day DHA or placebo (corn oil) | 0/1000 | Parallel-group, 18 months | No significant effect on ADAS-cog, MMSE or CDR sum of boxes | No (only plasma DHA) |
| Yurko-Mauro et al. (USA) [58] | 2010 | Adults with age-related cognitive decline, average age 70 years | 437 | 42:58 | 900 mg/day DHA or placebo (corn/soy oil) | 0/900 | Parallel-group, 6 months | Significant improvements in CANTAB PAL (p = 0.032), VRM immediate (p = 0.018) and delayed recall (p = 0.012) compared to placebo Cognitive changes significantly correlated with week 24 log plasma DHA levels | No (only plasma DHA) |
| Sinn et al. (Australia) [61] | 2011 | Adults with MCI, average age 74 years | 40 | 67:33 | EPA-rich or DHA-rich supplement or placebo (safflower oil) | 1670/160 | Parallel-group, 6 months | DHA significantly improved Initial Letter Fluency (p = 0.040) | Yes Low |
| 400/1550 | |||||||||
| Lee et al. (Malaysia) [60] | 2013 | Adults with MCI, average age 65 years | 36 | 25:75 | 1750 mg/day DHA rich fish oil or placebo (corn oil) | 450/1300 | Parallel-group, 12 months | Significant improvement in digit span, visual reproduction and delayed recall compared to placebo (p < 0.05 or p < 0.001) | No Plasma FA: very low |
| Significant improvement in executive and attention function (p = 0.025) in intervention group | |||||||||
| Significantly improved memory compared to placebo (p = 0.010) | |||||||||
| Eriksdotter et al. (Sweden) [59] | 2015 | Adults with AD, average age 74 years | 165 | 48:52 | 2300 mg/day LCn-3 PUFA or placebo (corn oil) | 600/1720 | Parallel-group, 6 months | Significant positive association between plasma DHA levels and changes of total scores of ADAS-cog (p = 0.016) | No Plasma FA: moderate |
| Phillips et al. (UK) [70] | 2015 | Adults with CIND or AD, average age 71 years | 76 | 45:55 | 1225 mg/day LCn-3 PUFA or placebo (olive oil) | 600/625 | Parallel-group, 4 months | No significant effect on cognitive function | No Plasma FA: adequate |
| Jackson et al. (UK) [19] | 2016 | Healthy adults with subjective memory deficits, aged 50–70 years | 54 | 38:62 | 1024 mg/day DHA-rich fish oil or placebo (high oleic acid sunflower oil + 120 mg fish oil) | 128/896 | Parallel-group, 6 months | No significant effect cognitive function | No Plasma FA: low |
| Zhang et al. (China) [62] | 2016 | Adults with MCI, average age 75 years | 219 | 35:65 | 2000 mg/day DHA or placebo (corn oil) | 0/2000 | Parallel-group, 12 months | Significant improvements in Full-Scale Intelligence Quotient (p = 0.039), Information (p < 0.001), Digit Span (p < 0.001) compared to placebo | No |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuszewski, J.C.; Wong, R.H.X.; Howe, P.R.C. Effects of Long-Chain Omega-3 Polyunsaturated Fatty Acids on Endothelial Vasodilator Function and Cognition—Are They Interrelated? Nutrients 2017, 9, 487. https://doi.org/10.3390/nu9050487
Kuszewski JC, Wong RHX, Howe PRC. Effects of Long-Chain Omega-3 Polyunsaturated Fatty Acids on Endothelial Vasodilator Function and Cognition—Are They Interrelated? Nutrients. 2017; 9(5):487. https://doi.org/10.3390/nu9050487
Chicago/Turabian StyleKuszewski, Julia C., Rachel H. X. Wong, and Peter R. C. Howe. 2017. "Effects of Long-Chain Omega-3 Polyunsaturated Fatty Acids on Endothelial Vasodilator Function and Cognition—Are They Interrelated?" Nutrients 9, no. 5: 487. https://doi.org/10.3390/nu9050487
APA StyleKuszewski, J. C., Wong, R. H. X., & Howe, P. R. C. (2017). Effects of Long-Chain Omega-3 Polyunsaturated Fatty Acids on Endothelial Vasodilator Function and Cognition—Are They Interrelated? Nutrients, 9(5), 487. https://doi.org/10.3390/nu9050487