Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
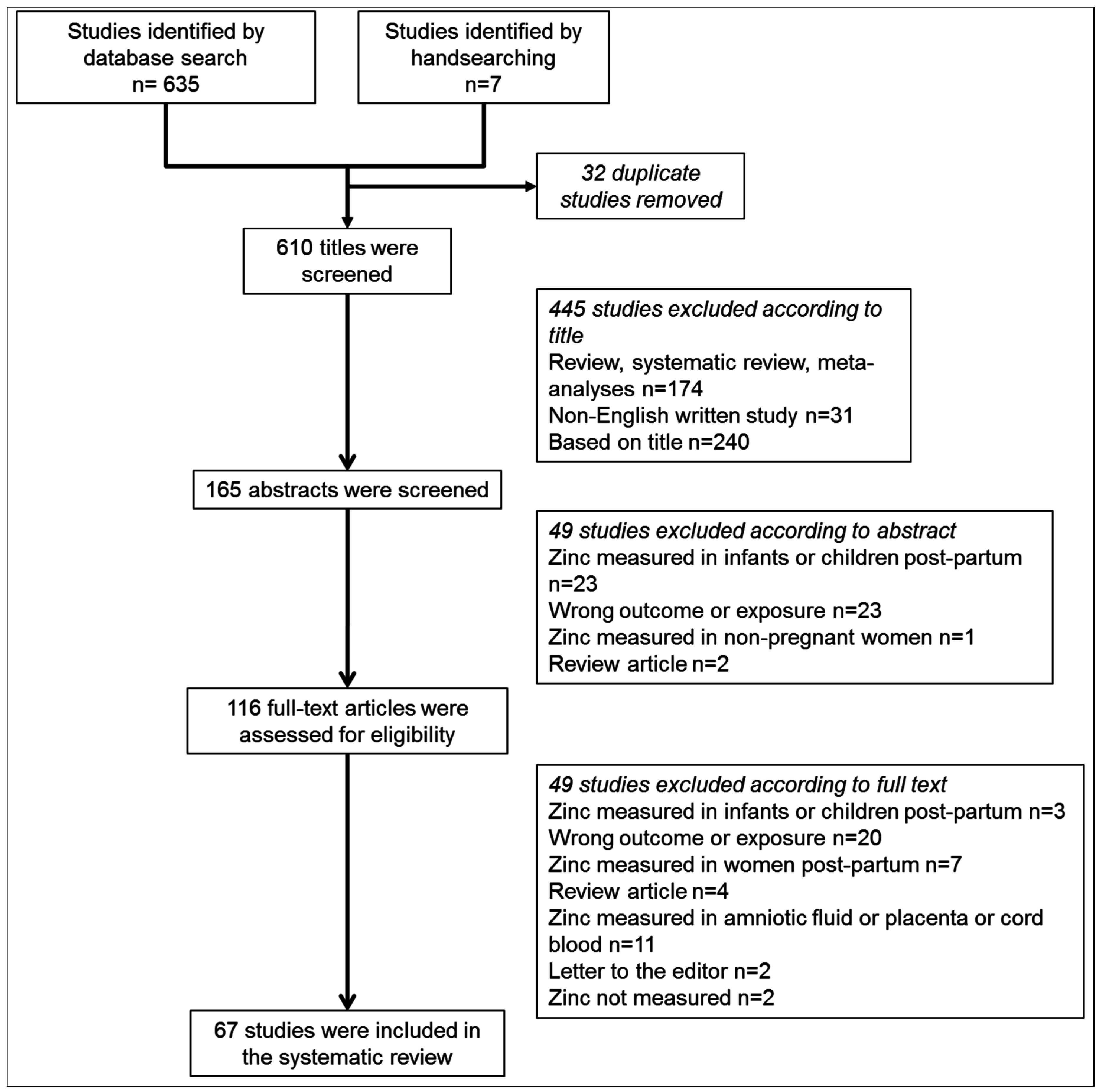
2.2. Information Sources and Search
2.3. Data Collection
3. Results
3.1. Infant Birthweight
3.2. Hypertensive Disorders of Pregnancy
3.3. Spontaneous Preterm Birth
3.4. Gestational Diabetes Mellitus
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
| Searches | Results | |
|---|---|---|
| 1 | exp Zinc/ or zinc.mp. | 108,695 |
| 2 | plasma zinc.mp. | 1365 |
| 3 | zinc intake.mp. | 679 |
| 4 | dietary zinc.mp. | 1158 |
| 5 | serum zinc.mp. | 2083 |
| 6 | 1 or 2 or 3 or 4 or 5 | 108,695 |
| 7 | preterm birth.mp. or exp Premature Birth/ | 14,642 |
| 8 | premature birth.mp. or Premature Birth/ | 11,131 |
| 9 | small for gestational age.mp. | 9255 |
| 10 | exp Infant, Small for Gestational Age/ | 5977 |
| 11 | gestational hypertension.mp. or exp Hypertension, Pregnancy-Induced/ | 32,078 |
| 12 | pre?eclampsia.mp. or exp Pre-Eclampsia/ | 30,863 |
| 13 | exp Pre-Eclampsia/ or exp Eclampsia/ or eclampsia.mp. | 32,471 |
| 14 | exp HELLP Syndrome/ or HELPP syndrome.mp. | 1613 |
| 15 | gestational diabetes.mp. or exp Diabetes, Gestational/ | 11,382 |
| 16 | fetal macrosomia.mp. or exp Fetal Macrosomia/ | 2369 |
| 17 | 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 | 69,148 |
| 18 | infant, low birth weight.mp. or Infant, Low Birth Weight/ | 16,571 |
| 19 | infant, very low birth weight.mp. or exp Infant, Very Low Birth Weight/ | 8491 |
| 20 | 17 or 18 or 19 | 89,771 |
| 21 | 6 and 20 | 380 |
| 22 | limit 21 to (english language and full text and humans) | 165 |
Appendix B
| Units | Conversion |
|---|---|
| μg/100 mL or μg/dL | Multiply 10 |
| μmol/L or μM | Divide 0.153 |
| mg/L | Multiply 1000 |
| μg/mL | Multiply 1000 |
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Grieger, J.A.; Clifton, V.L. A review of the impact of dietary intakes in human pregnancy on infant birthweight. Nutrients 2015, 7, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A. Developmental origins of disease paradigm: A mechanistic and evolutionary perspective. Pediatr. Res. 2004, 56, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Fischer Walker, C.L.; Ezzati, M.; Black, R.E. Global and regional child mortality and burden of disease attributable to zinc deficiency. Eur. J. Clin. Nutr. 2009, 63, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Organisation WH (2015) Fact Sheet No 290—Millennium Development Goals (MDGs). Available online: http://www.who.int/mediacentre/factsheets/fs290/en/# (accessed on 13 January 2016).
- Cousins, R.; Zinc, I.; Bowman, B.A.; Russell, R.M. Present Knowledge in Nutrition; DC ILSI Press: Washington, DC, USA, 2006; Volume 9, pp. 445–457. [Google Scholar]
- MacDonald, R.S. The role of zinc in growth and cell proliferation. J. Nutr. 2000, 130, 1500s–1508s. [Google Scholar] [PubMed]
- Maret, W. Molecular aspects of human cellular zinc homeostasis: Redox control of zinc potentials and zinc signals. Biometals 2009, 22, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Clinical, immunological, anti-inflammatory and antioxidant roles of zinc. Exp. Gerontol. 2008, 43, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Butler Walker, J.; Houseman, J.; Seddon, L.; McMullen, E.; Tofflemire, K.; Mills, C.; Corriveau, A.; Weber, J.-P.; LeBlanc, A.; Walker, M. Maternal and umbilical cord blood levels of mercury, lead, cadmium, and essential trace elements in Arctic Canada. Environ. Res. 2006, 100, 295–318. [Google Scholar] [CrossRef] [PubMed]
- Perveen, S.; Altaf, W.; Vohra, N.; Bautista, M.L.; Harper, R.G.; Wapnir, R.A. Effect of gestational age on cord blood plasma copper, zinc, magnesium and albumin. Early Hum. Dev. 2002, 69, 15–23. [Google Scholar] [CrossRef]
- Tsuzuki, S.; Morimoto, N.; Hosokawa, S.; Matsushita, T. Associations of maternal and neonatal serum trace element concentrations with neonatal birth weight. PLoS ONE 2013, 8, e75627. [Google Scholar] [CrossRef] [PubMed]
- Swanson, C.A.; King, J.C. Reduced serum zinc concentration during pregnancy. Obstet. Gynecol. 1983, 62, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Hurley, L.S.; Swenerton, H. Congenital malformations resulting from zinc deficiency in rats. Proc. Soc. Exp. Biol. Med. 1966, 123, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, C.; McCormick, N.H.; Croxford, T.P.; Seo, Y.A.; Grider, A.; Kelleher, S.L. Marginal maternal zinc deficiency in lactating mice reduces secretory capacity and alters milk composition. J. Nutr. 2012, 142, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Baek, S.H.; Lee, S.H.; Park, E.K.; Kim, E.C.; Kwun, I.S.; Shin, H.I. Zinc-deficient diet decreases fetal long bone growth through decreased bone matrix formation in mice. J. Med. Food 2009, 12, 118–123. [Google Scholar] [CrossRef] [PubMed]
- McCormick, N.H.; King, J.; Krebs, N.; Soybel, D.I.; Kelleher, S.L. Redistribution of tissue zinc pools during lactation and dyshomeostasis during marginal zinc deficiency in mice. J. Trace Elem. Med. Biol. 2014, 29, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Anthony, K.; Neuberger, T.; Diaz, F.J. Preconception zinc deficiency disrupts postimplantation fetal and placental development in mice. Biol. Reprod. 2014, 90, 83. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Wuehler, S.E.; Peerson, J.M. The importance of zinc in human nutrition and estimation of the global prevalence of zinc deficiency. Food Nutr. Bull. 2001, 22, 113–125. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand; NHMRC: Canberra, Australia, 2005.
- Food and Nutrition Board: Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Caulfield, L.E.; Zavaleta, N.; Shankar, A.H.; Merialdi, M. Potential contribution of maternal zinc supplementation during pregnancy to maternal and child survival. Am. J. Clin. Nutr. 1998, 68, 499s–508s. [Google Scholar] [PubMed]
- King, J.C. Determinants of maternal zinc status during pregnancy. Am. J. Clin. Nutr. 2000, 71, 1334s–1343s. [Google Scholar] [PubMed]
- Parr, R. Assessment of dietary intakes. Trace Elem. Hum. Nutr. Health 1996, 1996, 265–288. [Google Scholar]
- Caulfield, L.E.; Black, R.E. Zinc deficiency. In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors Geneva; World Health Organization: Geneva, Swizterland, 2004; pp. 257–279. [Google Scholar]
- Wessells, K.R.; Brown, K.H. Estimating the global prevalence of zinc deficiency: Results based on zinc availability in national food supplies and the prevalence of stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef] [PubMed]
- Ota, E.; Mori, R.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Miyazaki, C.; Bhutta, Z.A. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Shah, D.; Sachdev, H.P. Effect of gestational zinc deficiency on pregnancy outcomes: Summary of observation studies and zinc supplementation trials. Br. J. Nutr. 2001, 85, S101–S108. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Shen, X.; Zhang, D. The relationship between serum zinc level and preeclampsia: A Meta-Analysis. Nutrients 2015, 7, 7806–7820. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Adeniyi, F.A. The implications of hypozincemia in pregnancy. Acta Obstet. Gynecol. Scand. 1987, 66, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Akinloye, O.; Oyewale, O.J.; Oguntibeju, O.O. Evaluation of trace elements in pregnant women with pre-eclampsia. Afr. J. Biotechnol. 2010, 9, 5196–5202. [Google Scholar]
- Kumru, S.; Aydin, S.; Simsek, M.; Sahin, K.; Yaman, M.; Ay, G. Comparison of serum copper, zinc, calcium, and magnesium levels in preeclamptic and healthy pregnant women. Biol. Trace Elem. Res. 2003, 94, 105–112. [Google Scholar] [CrossRef]
- Wang, Y.; Tan, M.; Huang, Z.; Sheng, L.; Ge, Y.; Zhang, H.; Jiang, M.; Zhang, G. Elemental contents in serum of pregnant women with gestational diabetes mellitus. Biol. Trace Elem. Res. 2002, 88, 113–118. [Google Scholar] [CrossRef]
- Farzin, L.; Sajadi, F. Comparison of serum trace element levels in patients with or without pre-eclampsia. J. Res. Med. Sci. 2012, 17, 938–941. [Google Scholar] [PubMed]
- Gupta, S.; Jain, N.P.; Avasthi, K.; Wander, G.S. Plasma and erythrocyte zinc in pre-eclampsia and its correlation with foetal outcome. J. Assoc. Phys. India 2014, 62, 306–310. [Google Scholar]
- Hyvonen-Dabek, M.; Nikkinen-Vilkki, P.; Dabek, J.T. Selenium and other elements in human maternal and umbilical serum, as determined simultaneously by proton-induced X-ray emission. Clin. Chem. 1984, 30, 529–533. [Google Scholar] [PubMed]
- Jain, S.; Sharma, P.; Kulshreshtha, S.; Mohan, G.; Singh, S. The role of calcium, magnesium, and zinc in pre-eclampsia. Biol. Trace Elem. Res. 2010, 133, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Donangelo, C.M.; King, J.C. Maternal zinc intakes and homeostatic adjustments during pregnancy and lactation. Nutrients 2012, 4, 782–798. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Goldenberg, R.L. Zinc nutriture and pregnancy outcome. Nutr. Res. 1996, 16, 139–181. [Google Scholar] [CrossRef]
- Simmer, K.; Iles, C.A.; Slavin, B.; Keeling, P.W.; Thompson, R.P. Maternal nutrition and intrauterine growth retardation. Hum. Nutr. Clin. Nutr. 1987, 41, 193–197. [Google Scholar] [PubMed]
- Negandhi, P.H.; Negandhi, H.N.; Zodpey, S.P.; Ughade, S.N.; Biranjan, J.R. Risk factors for low birth weight in an Indian urban setting: A nested case control study. Asia Pac. J. Public Health 2014, 26, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O.; Hediger, M.L.; Schall, J.I.; Fischer, R.L.; Khoo, C.S. Low zinc intake during pregnancy: Its association with preterm and very preterm delivery. Am. J. Epidemiol. 1993, 137, 1115–1124. [Google Scholar] [PubMed]
- Neggers, Y.H.; Goldenberg, R.L.; Tamura, T.; Cliver, S.P.; Hoffman, H.J. The relationship between maternal dietary intake and infant birthweight. Acta Obstet. Gynecol. Scand. Suppl. 1997, 165, 71–75. [Google Scholar] [PubMed]
- Wang, H.; Hu, Y.-F.; Hao, J.-H.; Chen, Y.-H.; Su, P.-Y.; Wang, Y.; Yu, Z.; Fu, L.; Xu, Y.-Y.; Zhang, C.; et al. Maternal zinc deficiency during pregnancy elevates the risks of fetal growth restriction: A population-based birth cohort study. Sci. Rep. 2015, 5, 11262. [Google Scholar] [CrossRef] [PubMed]
- Voss Jepsen, L.; Clemmensen, K. Zinc in Danish women during late normal pregnancy and pregnancies with intra-uterine growth retardation. Acta Obstet. Gynecol. Scand. 1987, 66, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Borella, P.; Szilagyi, A.; Than, G.; Csaba, I.; Giardino, A.; Facchinetti, F. Maternal plasma concentrations of magnesium, calcium, zinc and copper in normal and pathological pregnancies. Sci. Total Environ. 1990, 99, 67–76. [Google Scholar] [CrossRef]
- Neggers, Y.H.; Cutter, G.R.; Acton, R.T.; Alvarez, J.O.; Bonner, J.L.; Goldenberg, R.L.; Go, R.C.; Roseman, J.M. A positive association between maternal serum zinc concentration and birth weight. Am. J. Clin. Nutr. 1990, 51, 678–684. [Google Scholar] [PubMed]
- Bro, S.; Berendtsen, H.; Norgaard, J.; Host, A.; Jorgensen, P.J. Serum zinc and copper concentrations in maternal and umbilical cord blood. Relation to course and outcome of pregnancy. Scand. J. Clin. Lab. Investig. 1988, 48, 805–811. [Google Scholar] [CrossRef]
- Mistry, H.D.; Kurlak, L.O.; Young, S.D.; Briley, A.L.; Pipkin, F.B.; Baker, P.N.; Poston, L. Maternal selenium, copper and zinc concentrations in pregnancy associated with small-for-gestational-age infants. Matern. Child. Nutr. 2014, 10, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Goldenberg, R.L.; Johnston, K.E.; Cliver, S.P.; Hoffman, H.J. Serum concentrations of zinc, folate, vitamins A and E, and proteins, and their relationships to pregnancy outcome. Acta Obstet. Gynecol. Scand. Suppl. 1997, 165, 63–70. [Google Scholar] [PubMed]
- Tamura, T.; Goldenberg, R.L.; Johnston, K.E.; DuBard, M. Maternal plasma zinc concentrations and pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, 109–113. [Google Scholar] [PubMed]
- Ghosh, A.; Fong, L.Y.; Wan, C.W.; Liang, S.T.; Woo, J.S.; Wong, V. Zinc deficiency is not a cause for abortion, congenital abnormality and small-for-gestational age infant in Chinese women. Br. J. Obstet. Gynaecol. 1985, 92, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Cherry, F.F.; Bennett, E.A.; Bazzano, G.S.; Johnson, L.K.; Fosmire, G.J.; Batson, H.K. Plasma zinc in hypertension/toxemia and other reproductive variables in adolescent pregnancy. Am. J. Clin. Nutr. 1981, 34, 2367–2375. [Google Scholar] [PubMed]
- Bogden, J.D.; Thind, I.S.; Kemp, F.W.; Caterini, H. Plasma concentrations of calcium, chromium, copper, iron, magnesium, and zinc in maternal and cord blood and their relationship to low birth weight. J. Lab. Clin. Med. 1978, 92, 455–462. [Google Scholar] [PubMed]
- Atinmo, T.; Mbofung, C.; Osinusi, B.O. Relationship of zinc and copper concentrations in maternal and cord blood and birth weight. Int. J. Gynaecol. Obstet. 1980, 18, 452–454. [Google Scholar] [PubMed]
- Abass, R.M.; Hamdan, H.Z.; Elhassan, E.M.; Hamdan, S.Z.; Ali, N.I.; Adam, I. Zinc and copper levels in low birth weight deliveries in Medani Hospital, Sudan. BMC Res. Notes 2014, 7, 386. [Google Scholar] [CrossRef] [PubMed]
- Rwebembera, A.A.-B.; Munubhi, E.K.D.; Manji, K.P.; Mpembeni, R.; Philip, J. Relationship between infant birth weight </=2000 g and maternal zinc levels at Muhimbili National Hospital, Dar Es Salaam, Tanzania. J. Trop. Pediatr. 2006, 52, 118–125. [Google Scholar] [PubMed]
- Bahl, L.; Chaudhuri, L.S.; Pathak, R.M. Study of serum zinc in neonates and their mothers in Shimla hills (Himachal Pradesh). Indian J. Pediatr. 1994, 61, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.P.; Khushlani, K.; Veerwal, P.C.; Gupta, R.C. Relationship between birth weight and zinc status of newly born infants and their mothers. Indian J. Physiol. Pharmacol. 1989, 33, 134–135. [Google Scholar] [PubMed]
- Prema, K. Predictive value of serum copper and zinc in normal and abnormal pregnancy. Indian J. Med. Res. 1980, 71, 554–560. [Google Scholar] [PubMed]
- Badakhsh, M.H.; Khamseh, M.E.; Seifoddin, M.; Kashanian, M.; Malek, M.; Shafiee, G.; Baradaran, H.R. Impact of maternal zinc status on fetal growth in an Iranian pregnant population. Gynecol. Endocrinol. 2011, 27, 1074–1076. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Misra, P.K. Study of plasma zinc in neonates and their mothers. Indian Pediatr. 1982, 19, 611–614. [Google Scholar] [PubMed]
- Srivastava, S.; Mehrotra, P.K.; Srivastava, S.P.; Siddiqui, M.K.J. Some essential elements in maternal and cord blood in relation to birth weight and gestational age of the baby. Biol. Trace Elem. Res. 2002, 86, 97–105. [Google Scholar] [PubMed]
- Jeswani, R.M.; Vani, S.N. A study of serum zinc levels in cord blood of neonates and their mothers. Indian J. Pediatr. 1991, 58, 683–686. [Google Scholar] [CrossRef] [PubMed]
- George, S.S.; Swaminathan, S.; Kanagasabapathy, A.S.; Seshadri, L. Maternal zinc indices and small babies. Natl. Med. J. India 1998, 11, 120–121. [Google Scholar] [PubMed]
- Akman, I.; Arioglu, P.; Koroglu, O.A.; Sakalli, M.; Ozek, E.; Topuzoglu, A.; Eren, S.; Bereket, A. Maternal zinc and cord blood zinc, insulin-like growth factor-1, and insulin-like growth factor binding protein-3 levels in small-for-gestational-age newborns. Clin. Exp. Obstet. Gynecol. 2006, 33, 238–240. [Google Scholar] [PubMed]
- Ozdemir, U.; Gulturk, S.; Aker, A.; Guvenal, T.; Imir, G.; Erselcan, T. Correlation between birth weight, leptin, zinc and copper levels in maternal and cord blood. J. Physiol. Biochem. 2007, 63, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Tande, D.L.; Ralph, J.L.; Johnson, L.K.; Scheett, A.J.; Hoverson, B.S.; Anderson, C.M. First trimester dietary intake, biochemical measures, and subsequent gestational hypertension among nulliparous women. J. Midwifery Womens Health 2013, 58, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Lazebnik, N.; Kuhnert, B.R.; Kuhnert, P.M. Zinc, cadmium, and hypertension in parturient women. Am. J. Obstet. Gynecol. 1989, 161, 437–440. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.J.; Lee, R.; Moon, J.H.; Jo, I. Serum levels of zinc, calcium, and iron are associated with the risk of preeclampsia in pregnant women. Nutr. Res. 2012, 32, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Kiilholma, P.; Paul, R.; Pakarinen, P.; Gronroos, M. Copper and zinc in pre-eclampsia. Acta Obstet. Gynecol. Scand. 1984, 63, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Araujo Brito, J.; do Nascimento Marreiro, D.; Moita Neto, J.M.; Michelle Costa e Silva, D.; Goncalves de Sousa Almondes, K.; Valadares Neto, J.D.D.; do Nascimento Nogueira, N. Enzyme activity of superoxide dismutase and zincemia in women with preeclampsia. Nutr. Hosp. 2013, 28, 486–490. [Google Scholar] [PubMed]
- Magri, J.; Sammut, M.; Savona-Ventura, C. Lead and other metals in gestational hypertension. Int. J. Gynaecol. Obstet. 2003, 83, 29–36. [Google Scholar] [CrossRef]
- Fenzl, V.; Flegar-Mestric, Z.; Perkov, S.; Andrisic, L.; Tatzber, F.; Zarkovic, N.; Duic, Z. Trace elements and oxidative stress in hypertensive disorders of pregnancy. Arch. Gynecol. Obstet. 2013, 287, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Katz, O.; Paz-Tal, O.; Lazer, T.; Aricha-Tamir, B.; Mazor, M.; Wiznitzer, A.; Sheiner, E. Severe pre-eclampsia is associated with abnormal trace elements concentrations in maternal and fetal blood. J. Matern. Fetal Neonatal Med. 2012, 25, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Gill, C.A.; Kurlak, L.O.; Seed, P.T.; Hesketh, J.E.; Meplan, C.; Schomburg, L.; Chappell, L.C.; Morgan, L.; Poston, L. Association between maternal micronutrient status, oxidative stress, and common genetic variants in antioxidant enzymes at 15 weeks gestation in nulliparous women who subsequently develop preeclampsia. Free Radic. Biol. Med. 2015, 78, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Lao, T.T.; Chin, R.K.; Swaminathan, R.; Mak, Y.T. Plasma and erythrocyte zinc concentrations in pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 1989, 30, 117–122. [Google Scholar] [CrossRef]
- Sarwar, M.S.; Ahmed, S.; Ullah, M.S.; Kabir, H.; Rahman, G.K.M.M.; Hasnat, A.; Islam, M.S. Comparative study of serum zinc, copper, manganese, and iron in preeclamptic pregnant women. Biol. Trace Elem. Res. 2013, 154, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Ilhan, N.; Ilhan, N.; Simsek, M. The changes of trace elements, malondialdehyde levels and superoxide dismutase activities in pregnancy with or without preeclampsia. Clin. Biochem. 2002, 35, 393–397. [Google Scholar] [CrossRef]
- Bakacak, M.; Kilinc, M.; Serin, S.; Ercan, O.; Kostu, B.; Avci, F.; Kiran, H.; Kiran, G. Changes in copper, zinc, and malondialdehyde levels and superoxide dismutase activities in pre-eclamptic pregnancies. Med. Sci. Monit. 2015, 21, 2414–2420. [Google Scholar] [PubMed]
- Al-Jameil, N.; Tabassum, H.; Al-Mayouf, H.; Aljohar, H.I.; Alenzi, N.D.; Hijazy, S.M.; Khan, F.A. Analysis of serum trace elements-copper, manganese and zinc in preeclamptic pregnant women by inductively coupled plasma optical emission spectrometry: A prospective case controlled study in Riyadh, Saudi Arabia. Int. J. Clin. Exp. Pathol. 2014, 7, 1900–1910. [Google Scholar] [PubMed]
- Bassiouni, B.A.; Foda, A.I.; Rafei, A.A. Maternal and fetal plasma zinc in pre-eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 1979, 9, 75–80. [Google Scholar] [CrossRef]
- Harma, M.; Harma, M.; Kocyigit, A. Correlation between maternal plasma homocysteine and zinc levels in preeclamptic women. Biol. Trace Elem. Res. 2005, 104, 97–105. [Google Scholar] [CrossRef]
- Rafeeinia, A.; Tabandeh, A.; Khajeniazi, S.; Marjani, A.J. Serum copper, zinc and lipid peroxidation in pregnant women with preeclampsia in gorgan. Open Biochem. J. 2014, 8, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Vafaei, H.; Dalili, M.; Hashemi, S.A. Serum concentration of calcium, magnesium and zinc in normotensive versus preeclampsia pregnant women: A descriptive study in women of Kerman province of Iran. Iran. J. Reprod. Med. 2015, 13, 23–26. [Google Scholar] [PubMed]
- Ahsan, T.; Banu, S.; Nahar, Q.; Ahsan, M.; Khan, M.N.; Islam, S.N. Serum trace elements levels in preeclampsia and eclampsia: Correlation with the pregnancy disorder. Biol. Trace Elem. Res. 2013, 152, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Gupta, A.; Batra, H.S.; Rathore, R. Comparative study of trace elements and serum ceruloplasmin level in normal and pre-eclamptic pregnancies with their cord blood. Biomed. Res. 2011, 22, 207–210. [Google Scholar]
- Kolusari, A.; Kurdoglu, M.; Yildizhan, R.; Adali, E.; Edirne, T.; Cebi, A.; Demir, H.; Yoruk, I.H. Catalase activity, serum trace element and heavy metal concentrations, and vitamin A, D and E levels in pre-eclampsia. J. Int. Med. Res. 2008, 36, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Atamer, Y.; Kocyigit, Y.; Yokus, B.; Atamer, A.; Erden, A.C. Lipid peroxidation, antioxidant defense, status of trace metals and leptin levels in preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 119, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Adam, B.; Malatyalioglu, E.; Alvur, M.; Talu, C. Magnesium, zinc and iron levels in pre-eclampsia. J. Matern. Fetal Med. 2001, 10, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Vigeh, M.; Yokoyama, K.; Ramezanzadeh, F.; Dahaghin, M.; Sakai, T.; Morita, Y.; Kitamura, F.; Sato, H.; Kobayashi, Y. Lead and other trace metals in preeclampsia: A case-control study in Tehran, Iran. Environ. Res. 2006, 100, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, S.L.; Yang, W.; Shaw, G.M.; National Birth Defects Prevention Sdudy. Maternal dietary nutrient intake and risk of preterm delivery. Am. J. Perinatol. 2013, 30, 579–588. [Google Scholar] [PubMed]
- Hsu, W.-Y.; Wu, C.-H.; Hsieh, C.T.-C.; Lo, H.-C.; Lin, J.-S.; Kao, M.-D. Low body weight gain, low white blood cell count and high serum ferritin as markers of poor nutrition and increased risk for preterm delivery. Asia Pac. J. Clin. Nutr. 2013, 22, 90–99. [Google Scholar] [PubMed]
- Wang, H.; Hu, Y.-F.; Hao, J.-H.; Chen, Y.-H.; Wang, Y.; Zhu, P.; Zhang, C.; Xu, Y.-Y.; Tao, F.-B.; Xu, D.-X. Maternal serum zinc concentration during pregnancy is inversely associated with risk of preterm birth in a Chinese population. J. Nutr. 2016, 146, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Lezo, A.; Menato, G.; Gallo, M.-L.; Bardelli, C.; Signorile, A.; Berutti, C.; Massobrio, M.; Pagano, G.F. Gestational hyperglycemia, zinc, selenium, and antioxidant vitamins. Nutrition 2005, 21, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Behboudi-Gandevani, S.; Safary, K.; Moghaddam-Banaem, L.; Lamyian, M.; Goshtasebi, A.; Goshtasbi, A.; Alian-Moghaddam, N. The relationship between maternal serum iron and zinc levels and their nutritional intakes in early pregnancy with gestational diabetes. Biol. Trace Elem. Res. 2013, 154, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wibell, L.; Gebre-Medhin, M.; Lindmark, G. Magnesium and zinc in diabetic pregnancy. Acta Paediatr. Scand. Suppl. 1985, 320, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Al-Saleh, E.; Nandakumaran, M.; Al-Shammari, M.; Al-Harouny, A. Maternal-fetal status of copper, iron, molybdenum, selenium and zinc in patients with gestational diabetes. J. Matern. Fetal Neonatal Med. 2004, 16, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Prema, K.; Ramalakshmi, B.A.; Babu, S. Serum copper and zinc in hormonal contraceptive users. Fertil. Steril. 1980, 33, 267–271. [Google Scholar] [CrossRef]
- Kristal, A.R.; Peters, U.; Potter, J.D. Is it time to abandon the food frequency questionnaire? Cancer Epidemiol. Biomark. Prev. 2005, 14, 2826–2828. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M. Physiology of zinc: General aspects. In Zinc in Human Biology; Springer: London, UK, 1989; pp. 1–14. [Google Scholar]
- Goode, H.F.; Kelleher, J.; Walker, B.E. The effects of acute infection on indices of zinc status. Clin. Nutr. 1991, 10, 55–59. [Google Scholar] [CrossRef]
- Halsted, J.A.; Hackley, B.M.; Smith, J.C., Jr. Plasma-zinc and copper in pregnancy and after oral contraceptives. Lancet 1968, 2, 278–279. [Google Scholar] [CrossRef]
- Prasad, A.S. Clinical, endocrinological and biochemical effects of zinc deficiency. Clin. Endocrinol. Metab. 1985, 14, 567–589. [Google Scholar] [CrossRef]
- Singh, A.; Smoak, B.L.; Patterson, K.Y.; LeMay, L.G.; Veillon, C.; Deuster, P.A. Biochemical indices of selected trace minerals in men: Effect of stress. Am. J. Clin. Nutr. 1991, 53, 126–131. [Google Scholar] [PubMed]
- Moran, V.H.; Skinner, A.L.; Medina, M.W.; Patel, S.; Dykes, F.; Souverein, O.W.; Dullemeijer, C.; Lowe, N.M. The relationship between zinc intake and serum/plasma zinc concentration in pregnant and lactating women: A systematic review with dose-response meta-analyses. J. Trace Elem. Med. Biol. 2012, 26, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Benes, B.; Spevackova, V.; Smid, J.; Batariova, A.; Cejchanova, M.; Zitkova, L. Effects of age, BMI, smoking and contraception on levels of Cu, Se and Zn in the blood of the population in the Czech Republic. Cent. Eur. J. Public Health 2005, 13, 202–207. [Google Scholar] [PubMed]
- Ghayour-Mobarhan, M.; Taylor, A.; New, S.A.; Lamb, D.J.; Ferns, G.A. Determinants of serum copper, zinc and selenium in healthy subjects. Ann. Clin. Biochem. 2005, 42, 364–375. [Google Scholar] [CrossRef] [PubMed]
- North, R.A.; McCowan, L.M.; Dekker, G.A.; Poston, L.; Chan, E.H.; Stewart, A.W.; Black, M.A.; Taylor, R.S.; Walker, J.J.; Baker, P.N.; et al. Clinical risk prediction for pre-eclampsia in nulliparous women: Development of model in international prospective cohort. BMJ 2011, 342, d1875. [Google Scholar] [CrossRef] [PubMed]
- Kenny, L.C.; Black, M.A.; Poston, L.; Taylor, R.; Myers, J.E.; Baker, P.N.; McCowan, L.M.; Simpson, N.A.; Dekker, G.A.; Roberts, C.T.; et al. Early pregnancy prediction of preeclampsia in nulliparous women, combining clinical risk and biomarkers: The Screening for Pregnancy Endpoints (SCOPE) international cohort study. Hypertension 2014, 64, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lonnerdal, B.; Ruel, M.T.; Sandtrom, B.; Wasantwisut, E.; Hotz, C. International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar] [PubMed]
- Burton, G.J.; Jauniaux, E. Placental oxidative stress: From miscarriage to preeclampsia. J. Soc. Gynecol. Investig. 2004, 11, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Marklund, S. Distribution of CuZn superoxide dismutase and Mn superoxide dismutase in human tissues and extracellular fluids. Acta Physiol. Scand. Suppl. 1980, 492, 19–23. [Google Scholar] [PubMed]
- Bruno, R.S.; Song, Y.; Leonard, S.W.; Mustacich, D.J.; Taylor, A.W.; Traber, M.G.; Ho, E. Dietary zinc restriction in rats alters antioxidant status and increases plasma F2 isoprostanes. J. Nutr. Biochem. 2007, 18, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Oteiza, P.I.; Clegg, M.S.; Zago, M.P.; Keen, C.L. Zinc deficiency induces oxidative stress and AP-1 activation in 3T3 cells. Free Radic. Biol. Med. 2000, 28, 1091–1099. [Google Scholar] [CrossRef]
- Prasad, A.S.; Beck, F.W.; Bao, B.; Fitzgerald, J.T.; Snell, D.C.; Steinberg, J.D.; Cardozo, L.J. Zinc supplementation decreases incidence of infections in the elderly: Effect of zinc on generation of cytokines and oxidative stress. Am. J. Clin. Nutr. 2007, 85, 837–844. [Google Scholar] [PubMed]
- Sankavaram, K.; Chong, L.; Bruno, R.S.; Freake, H.C. Zinc status alters growth and oxidative stress responses in rat hepatoma cells. Nutr. Cancer 2014, 66, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Leonard, S.W.; Traber, M.G.; Ho, E. Zinc deficiency affects DNA damage, oxidative stress, antioxidant defenses, and DNA repair in rats. J. Nutr. 2009, 139, 1626–1631. [Google Scholar] [CrossRef] [PubMed]
- Habib, Z.; Abdulla, M. Plasma levels of zinc, copper, magnesium and calcium during early weeks of gestation. Acta Pharmacol. Toxicol. 1986, 59 (Suppl. 7), 602–605. [Google Scholar] [CrossRef]
- Donangelo, C.M.; Zapata, C.L.; Woodhouse, L.R.; Shames, D.M.; Mukherjea, R.; King, J.C. Zinc absorption and kinetics during pregnancy and lactation in Brazilian women. Am. J. Clin. Nutr. 2005, 82, 118–124. [Google Scholar] [PubMed]
- Fung, E.B.; Ritchie, L.D.; Woodhouse, L.R.; Roehl, R.; King, J.C. Zinc absorption in women during pregnancy and lactation: A longitudinal study. Am. J. Clin. Nutr. 1997, 66, 80–88. [Google Scholar] [PubMed]
- Sherwood, L. Human Physiology: From Cells to Systems; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Bowen, J.M.; Chamley, L.; Keelan, J.A.; Mitchell, M.D. Cytokines of the placenta and extra-placental membranes: Roles and regulation during human pregnancy and parturition. Placenta 2002, 23, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Multiple micronutrients in pregnancy and lactation: An overview. Am. J. Clin. Nutr. 2005, 81, 1206S–1212S. [Google Scholar] [PubMed]
- Christian, P.; West, K.P., Jr. Interactions between zinc and vitamin A: An update. Am. J. Clin. Nutr. 1998, 68, 435S–441S. [Google Scholar] [PubMed]
- Lonnerdal, B. Dietary factors influencing zinc absorption. J. Nutr. 2000, 130, 1378S–1383S. [Google Scholar] [PubMed]
- Solomons, N.W. Competitive interaction of iron and zinc in the diet: Consequences for human nutrition. J. Nutr. 1986, 116, 927–935. [Google Scholar] [PubMed]
| Author, Country | Sample Size | Zinc Measure | Outcome of the Study |
|---|---|---|---|
| (1) Sample Type | |||
| (2) Time at Which Gestation Diet Was Assessed or Sample Collected | |||
| (3) Method of Analysis | |||
| [42] Simmer, United Kingdom a | 28 SGA 29 uncomplicated | Dietary zinc intake Third trimester of pregnancy 7 day dietary recall | ↓ mean (SEM) dietary intake in the SGA mothers compared to the women with uncomplicated pregnancies. SGA: 11.3 (0.5) vs. uncomplicated: 13.0 (0.6) mg/day, p < 0.05 |
| [43] Negandhi, India b | 144 LBW 240 uncomplicated | Dietary zinc intake 26–30 weeks 24 h dietary recall | ↓ mean dietary zinc intake in women with a LBW infant compared to those with an uncomplicated pregnancy. LBW: 5.39 mg/day vs. uncomplicated 6.77 mg/day, p < 0.001 |
| [44] Scholl, United States c | 115 with zinc intake ≤6 mg/day 699 with zinc intake ˃6 mg/day | Dietary zinc intake 28 and 36 weeks 24 h dietary recall | 2-fold ↓ risk of delivering a LBW infant with dietary zinc intake ˃6 mg/day. OR: 2.01, 95% CI: 1.11–3.66 |
| [45] Neggers, United States d | 180 LBW 1218 uncomplicated | Dietary zinc intake 18 and 30 weeks 24 h dietary recall using the nutrient data base developed by the University of Minnesota | NS association between low dietary zinc intake (less than median) and risk of LBW. OR: 1.4, 95% CI: 0.9–2.1 |
| Inadequate dietary zinc intake estimated to affect <17% of the studied population | |||
| [46] Wang, China b | 247 with serum zinc <560 µg/L 2940 with serum zinc ≥560 µg/L | Fasting serum zinc Across gestation Flame AAS | ↑ incidence of LBW in the mothers with serum zinc <560 µg/L compared to those with serum zinc ≥560 µg/L. Adjusted RR: 3.41, 95% CI: 1.97, 5.91 |
| [47] Voss Jepsen, Denmark a | 10 SGA 30 uncomplicated | Heparin plasma zinc Collected at 35–41 weeks AAS | ↑ mean (SD) plasma zinc between SGA mothers and those with uncomplicated pregnancies. SGA: 732 (85) vs. uncomplicated: 654 (78) μg/L, p = 0.03 |
| [48] Borella, Italy a | 16 SGA 35 uncomplicated | Heparin plasma zinc Collected in the third trimester Flame AAS | ↑ mean (SD) plasma zinc in SGA women compared to women with uncomplicated pregnancies. SGA: 685.6 (119.6) vs. uncomplicated: 627.5 (150) µg/L, p < 0.001 |
| [49] Neggers, USA e | 39 LBW 437 uncomplicated | Serum zinc Collected across gestation Flame AAS | 8-fold ↑ prevalence of LBW with serum zinc in the lowest quartile (457.5–797.4 µg/L) compared to the highest (1039.2–1660.1 µg/L). OR: 8.2, 95% CI:2.4–27.5 |
| [50] Bro, Denmark a | 47 SGA and 34 preterm 220 uncomplicated | Serum zinc Collected at delivery Flame AAS | NS mean (SD) serum zinc levels between SGA and women with uncomplicated pregnancies. SGA: 764.7 (119.6) vs. uncomplicated: 679.7 (98) µg/L |
| [38] Hyvonen-Dabek, Finland f | 4 SGA 10 uncomplicated | Serum zinc Collection time not specified Particle induced X-ray emission | NS mean (SD) serum zinc in SGA women compared to those with uncomplicated pregnancies. SGA: 1270 (320) vs. uncomplicated: 1150 (220) µg/L |
| [51] Mistry, UK a* | 19 SGA 107 uncomplicated | Heparin plasma zinc Collected at 28–32 weeks Inductively coupled plasma mass spectrometry | NS in mean (95% CI) plasma zinc between SGA women and those with uncomplicated pregnancies. SGA: 708.1 (510.4–905.8) vs. uncomplicated: 634.4 (580.5–688.2) μg/L |
| [52] Tamura, USA g | 80 SGA 80 uncomplicated | Serum zinc Collected at 18 weeks and 30 weeks Flame AAS | NS in mean (SD) plasma zinc between SGA and women with uncomplicated pregnancies at 18 weeks. SGA: 627 (118) vs. uncomplicated: 667 (98) µg/L NS in mean (SD) plasma zinc between SGA and women with uncomplicated pregnancies at 30 weeks. SGA: 562 (92) vs. uncomplicated: 575 (92) µg/L |
| [53] Tamura, USA a | 139 SGA 2038 uncomplicated | Non-fasting heparin plasma zinc Collected at first prenatal visit (6 to 34 weeks) Flame AAS | NS in the prevalence (n (%)) of SGA measured between the lowest quartile and upper 3 quartiles of zinc. Highest: 103 (4.4) vs. lowest: 36 (4.8) |
| [54] Ghosh, China a | 22 SGA 38 uncomplicated | Serum zinc Collected within 24 h of delivery AAS | NS in mean (SD) serum zinc levels between SGA and women with uncomplicated pregnancies. SGA: 508.1 (185.9) vs. uncomplicated: 542.3 (162.8) μg/L |
| [55] Cherry, USA b | 29 LBW 230 uncomplicated | Heparin plasma zinc Collected across gestation AAS | NS mean (SEM) plasma zinc in mothers with a LBW infant compared to mothers with uncomplicated pregnancies. LBW: 604.9 (22.4) vs. uncomplicated: 577.2 (7.7) μg/L |
| [56] Bogden, USA h | 22 LBW 50 uncomplicated | EDTA plasma zinc Collected at delivery Flame AAS | NS mean (SEM) plasma zinc in women with a LBW infant compared to women with uncomplicated pregnancies. LBW: 640 (20) vs. uncomplicated: 620 (20) µg/L |
| Inadequate dietary zinc intake estimated to affect ≥17% of the studied population | |||
| [57] Atinmo, Nigeria h | 20 LBW 30 uncomplicated | Heparin plasma zinc Collected at delivery AAS | ↓ mean (SD) serum zinc in women with a LBW infant compared to those with uncomplicated pregnancies. LBW: 663.1 (144.6) vs. uncomplicated: 731.5 (235.6) µg/L, p < 0.05 |
| [58] Abass, Sudan b | 50 LBW 50 uncomplicated | Serum zinc AAS Atomic absorption spectrometry | ↓ median (IQR) serum zinc in women with a LBW infant compared to those with uncomplicated pregnancies. LBW: 629 (363–968) vs. uncomplicated 962 (846–1257) µg/L, p < 0.001 |
| [59] Rwebembera, Tanzania c | 81 LBW 84 uncomplicated | EDTA plasma zinc Collected at delivery Flame AAS | 3-fold ↓ risk of delivering a LBW infant with serum zinc ≥ 392.2 µg/L OR: 3.07, 95% CI: 1.07–8.97 |
| [60] Bahl, India c | 19 LBW 56 uncomplicated | Serum zinc Collected at delivery Flame AAS | ↓ mean (SD) serum zinc in women with a LBW infant compared to those with uncomplicated pregnancies. LBW: 553 (43) vs. 692 (95) µg/L, p < 0.001 |
| [61] Singh, India e | 47 LBW 45 uncomplicated | Serum zinc Collected at delivery AAS | ↓ mean (SD) serum zinc in women with a LBW infant compared to those with uncomplicated pregnancies. LBW: 623 (330) vs. uncomplicated: 895 (514) μg/L, p < 0.001 |
| [62] Prema, India e | 23 LBW 208 uncomplicated | Serum zinc Collected at delivery between 9–11.30 a.m. Flame AAS | ↑ mean (SD) serum zinc in mothers with a LBW infant compared to mothers with an uncomplicated pregnancy. LBW: 660 (162) vs. uncomplicated: 620 (146) µg/L, p < 0.01 |
| [63] Badakhsh, Iran b | 30 LBW 110 uncomplicated | Serum zinc Collected at delivery AAS | ↑ mean (SD) serum zinc in mothers with a LBW infant compared to mothers with an uncomplicated pregnancy. LBW: 686.2 (204.8) vs. uncomplicated: 514.3 (138.8) µg/L, p < 0.001 |
| [64] Goel, India a | 20 LBW 25 uncomplicated | Heparin plasma zinc Collected at delivery AAS | NS mean (SD) plasma zinc in women with a LBW infant compared to those with an uncomplicated pregnancy. LBW: 726 (61) vs. uncomplicated: 763 (56) μg/L |
| [65] Srivastava, India b | 26 LBW 25 uncomplicated | Heparin plasma zinc Collected at delivery Flame AAS | NS mean (SD) plasma zinc between mothers with a LBW infant and mothers with uncomplicated pregnancies. LBW: 6470 (4860) vs. uncomplicated: 5670 (2490) µg/L |
| [66] Jeswani, India a | 10 SGA 25 uncomplicated | Serum zinc Collected at 28–40 weeks AAS | NS mean (SD) serum zinc in SGA women compared to those with uncomplicated pregnancies. SGA: 938 (76.2) vs. uncomplicated: 962.8 (194.8) µg/L |
| [67] George, India a | 65 SGA 51 uncomplicated | Heparin plasma zinc Collected before labor between 8–10 a.m. AAS | NS in mean (SD) plasma zinc between SGA and women with uncomplicated pregnancies. SGA: 675 (90) vs. uncomplicated: 706.7 (139) µg/L |
| [68] Akman, Turkey f | 22 SGA 34 uncomplicated | Serum zinc Collected at delivery AAS | NS mean (SD) serum zinc between SGA women and women with uncomplicated pregnancies. SGA: 1218 (543) vs. uncomplicated 1038 (343) µg/L |
| [69] Ozdemir, Turkey b | 16 LBW 59 uncomplicated | Serum zinc Collected at 38–42 weeks Flame AAS | NS mean (SD) serum zinc between mothers with a LBW infant and mothers with uncomplicated pregnancies. Data represented on graphs |
| Author, Country | SAMPLE SIZE | Zinc Measure | Outcome of the Study |
|---|---|---|---|
| (1) Sample Type | |||
| (2) Time at Which Gestation Diet Was Assessed or Sample Collected | |||
| (3) Method of Analysis | |||
| [70] Tande, United States a,b | 13 hypertensive (11 PE + 2 GH) 44 uncomplicated | Dietary and supplement intake First 3 months of pregnancy Harvard food frequency questionnaire | NS in mean (SEM) dietary zinc intake between those with and without gestational hypertension. Hypertensive: 16.9 (1.56) vs. uncomplicated: 15.4 (1.03) mg/day |
| Inadequate dietary zinc intake estimated to affect <17% of the studied population | |||
| [71] Lazebnik, United States a,b | 17 PE and 14 hypertensive 31 uncomplicated | Plasma zinc Collected within 1 h of delivery AAS | ↓ mean (SD) serum zinc in women with PE when compared to women with uncomplicated pregnancies. PE: 420 (100) vs. uncomplicated: 520 (130) µg/L, p < 0.05 NS mean (SD) plasma zinc in hypertensive women compared to those whose pregnancies remained uncomplicated. Hypertensive: 530 (110) vs. uncomplicated: 520 (110) µg/L |
| [55] Cherry, United States a | 48 toxemic/ hypertensive 207 uncomplicated | Heparin plasma zinc Collected across gestation AAS | ↓ mean (SEM) plasma zinc in women with toxemia/ hypertension compared to women with uncomplicated pregnancies. Toxemic: 541.5 (16.8) vs. uncomplicated: 590.7 (8) μg/L, p < 0.009 |
| [72] Kim, Korea a | 29 PE 30 uncomplicated | Serum zinc Collected at delivery Instrumental neutron activation analysis | ↓ mean (SEM) serum zinc in mothers with PE compared to women with uncomplicated pregnancies. PE: 700 (200) vs. uncomplicated: 1900 (500) μg/L, p < 0.0001 |
| [73] Kiilholma, Finland c,d | 10 mild PE and 10 severe PE 20 uncomplicated | Serum zinc Collected at delivery Particle induced X-ray emission | ↓ mean (SD) serum zinc in women with mild and severe PE compared to women with uncomplicated pregnancies. Mild PE: 510 (70) and severe PE: 370 (10) vs. uncomplicated: 630 (90) μg/L, p < 0.001 for both, respectively ↓ mean (SD) serum zinc in women with severe PE compared to those with mild PE. Severe PE: 370 (10) vs. mild PE: 510 (70) μg/L, p < 0.005 |
| [74] Araujo Brito, Brazil e | 20 mild PE and 24 severe PE 50 uncomplicated | Fasting sodium citrate plasma zinc Collected before delivery Flame AAS | ↓ mean (SD) plasma zinc in mothers with severe PE compared to mothers with uncomplicated pregnancies. Severe PE: 388 (82) vs. uncomplicated: (483 (83) µg/L, p < 0.05 NS mean (SD) plasma zinc in women with mild PE compared to women with uncomplicated pregnancies. Mild PE: 500 (94) vs. uncomplicated: (483 (83) µg/L |
| [75] Magri, Malta b | 33 GH 110 uncomplicated | Serum zinc Collected in third trimester Electro-thermal AAS | NS in mean (SD) serum zinc between women with GH and women with uncomplicated pregnancies. PE: 606 (80) vs. uncomplicated: 636 (100) μg/L |
| [76] Fenzl, Croatia a,b | 30 PE and 30 GH 37 uncomplicated | Fasting serum zinc Collected at the time of diagnosis Flame AAS | NS in mean (SD) serum zinc between both women with PE or GH women and women with uncomplicated pregnancies. PE: 603 (93) and GH: 599 (83) vs. uncomplicated: 578 (93) μg/L |
| [77] Katz, Israel d | 43 severe PE 80 uncomplicated | Plasma zinc Collected immediately after delivery Inductively coupled plasma mass spectrometry | NS mean (SD) plasma zinc in mothers with severe PE vs. mothers with uncomplicated pregnancies. Severe PE: 685 (875) vs. uncomplicated: 534 (139) µg/L |
| [38] Hyvonen-Dabek, Finland f | 10 hypertensive 10 uncomplicated | Serum zinc Collection time not specified Particle induced X-ray emission | NS mean (SD) serum zinc in women with PE compared to women with an uncomplicated pregnancy. PE: 1070 (320) and hypertensive: 1090 (170) vs. uncomplicated: 1150 (220) |
| [48] Borella, Italy a | 24 hypertensive 35 uncomplicated | Heparin plasma zinc Collected in the third trimester Flame AAS | NS mean (SD) plasma zinc in the hypertensive women compared to those who remained uncomplicated. Hypertensive: 685.6 (149) vs. uncomplicated: 627.5 (150) µg/L |
| [78] Mistry, United Kingdom a | 244 PE 472 uncomplicated | Non-fasting heparin plasma zinc Collected at 15 weeks gestation Inductively coupled plasma mass spectrometry | NS median (interquartile range) plasma zinc in women with PE women compared to those with uncomplicated pregnancies. PE: 579.6 (521.1–638.6) vs. uncomplicated: 575.7 (515.6–641.7) µg/L |
| [53] Tamura, United States a | 271 hypertensive 2038 uncomplicated | Non-fasting heparin plasma zinc Collected at first prenatal visit (6 to 34 weeks) Flame AAS | NS in the prevalence (n (%)) of hypertension measured between the lowest quartile and upper 3 quartiles of zinc. Highest: 205 (7.9) vs. Lowest: 66 (7.7) |
| [79] Lao TT, China a | 28 PE 28 uncomplicated | Heparin plasma zinc Collected after diagnosis, before delivery Flame AAS | NS mean (SD) plasma zinc in women with PE compared to women with uncomplicated pregnancies. PE: 641 (163) vs. uncomplicated: 647 (111) µg/L |
| Inadequate dietary zinc intake estimated to affect ≥17% of the studied population | |||
| [80] Sarwar, Bangladesh a | 50 PE 58 uncomplicated | Fasting serum zinc Collected ˃20 weeks gestation Flame AAS | ↓ mean (SEM) serum zinc in mothers with PE compared to mothers with uncomplicated pregnancies. PE: 770 (50) vs. uncomplicated: 980 (30) µg/L, p < 0.001 |
| [34] Kumru, Turkey a | 30 PE 30 uncomplicated | Serum zinc Collection time not specified AAS | ↓ mean serum zinc in women with PE when compared to women with uncomplicated pregnancies. Data represented on graphs, p < 0.001 |
| [81] IIhan, Turkey a | 21 PE 20 uncomplicated | Serum zinc Collected at 31–38 weeks Flame AAS | ↓ mean (SD) serum zinc in women with PE when compared to those with an uncomplicated pregnancy. PE: 829.4 (289.3) vs. uncomplicated: 1251.9 (242.3) μg/L, p < 0.001 |
| [82] Bakacak, Turkey a | 38 PE 40 uncomplicated | Fasting serum zinc 32–38 weeks Flame AAS | ↓ median (max-min) serum zinc in women with PE when compared to those with an uncomplicated pregnancy. PE: 812.4 (1106.5–624) vs. uncomplicated: 1084.5 (1385.5–881.2) μg/L, p < 0.001 |
| [36] Farzin, Iran a | 60 PE 60 uncomplicated | Fasting heparin plasma zinc Collection time not specified Flame AAS | ↓ mean (SEM) serum zinc in mothers with PE compared to mothers with uncomplicated pregnancies. PE: 764.9 (176.2) vs. uncomplicated: 1006.1 (201.2) µg/L, p < 0.001 |
| [83] Al-Jameil, Saudi Arabia a | 40 PE 40 uncomplicated | Serum zinc Collected in the third trimester Inductively coupled plasma optical emission spectrometry | ↓ mean (SD) serum zinc in mothers with PE compared to mothers with uncomplicated pregnancies. PE: 670 (590) vs. uncomplicated: 1300 (830) µg/L, p < 0.05 |
| [33] Akinloye, Nigeria a | 49 PE 40 uncomplicated | Serum zinc Collection time not specified Flame AAS | ↓ mean (SD) serum zinc between women with PE and women with uncomplicated pregnancies. PE: 562 (92) vs. uncomplicated: 614 (52) μg/L, p < 0.05 |
| [39] Jain, India e | 25 mild PE and 25 severe PE 50 uncomplicated | Serum zinc Collection time not specified AAS | ↓ mean (SD) serum zinc between women with mild PE and those with uncomplicated pregnancies. Mild PE: 831 (111) vs. uncomplicated: 1022 (157) μg/L, p < 0.05 ↓ mean (SD) serum zinc between women with severe PE and women with uncomplicated pregnancies. Severe PE: 787 (92) vs. uncomplicated: 1022 (157) μg/L, p < 0.05 |
| [37] Gupta, India b,e | 47 mild PE and. 18 severe PE and 10 eclamptic 74 uncomplicated | Non-fasting heparin plasma zinc Collection time not specified AAS | ↓ mean (SD) serum zinc in mothers with severe PE and eclampsia compared to mothers with uncomplicated pregnancies. Severe PE: 607 (107) and eclampsia: 607 (171) vs. uncomplicated: 695 (119) μg/L, p < 0.01 NS in mean (SD) serum zinc between women with mild PE and women with uncomplicated pregnancies. Mild PE: 684 (134) vs. uncomplicated: 695 (119) μg/L |
| [84] Bassiouni, Egypt g,d | 52 PE (28 mild and 24 severe) 20 uncomplicated | Heparin plasma zinc Collected at delivery AAS | NS in mean (SD) plasma zinc in women with mild PE compared to women with uncomplicated pregnancies. Mild PE: 604.2 (162.7) vs. uncomplicated: 646 (173.7) μg/L ↓ mean (SD) plasma zinc in women with severe PE compared to the women with uncomplicated pregnancies. Severe PE: 410.8 (116.5) vs. uncomplicated: 646.0 (173.7 μg/L, p < 0.001 |
| [85] Harma, Turkey a | 24 PE 44 uncomplicated | Heparin plasma zinc Collected just during the latent phase of labor AAS | ↑ mean (SD) plasma zinc levels in women with PE when compared to women with uncomplicated pregnancies. PE: 15.53 (4.92) vs. uncomplicated: 11.93 (3.11) μg/g protein, p = 0.003 |
| [86] Rafeeinia, Iran h | 35 PE and 15 severe PE 50 uncomplicated | Fasting serum zinc Collected in the third trimester AAS | NS mean (SD) serum zinc in mothers with PE or severe PE and uncomplicated pregnancies. Mild PE: 690 (40) and severe PE: 780 (80) vs. uncomplicated: 720 (40) µg/L |
| [87] Vafaei, Iran e | 20 mild PE and 20 severe PE 40 uncomplicated | Serum zinc Collected at 28–40 weeks Auto-analyser | NS mean (SD) serum zinc in either the mild or severe PE women compared to women with uncomplicated pregnancies. Data represented on graphs |
| [88] Ahsan, Bangladesh a,i | 44 PE and 33 eclampsia 27 uncomplicated | Serum zinc Collected at 28–42 weeks Flame AAS | NS mean (SD) serum zinc in PE or eclamptic women compared to women with uncomplicated pregnancies. PE: 1045.8 (131) and eclampsia: 915 (131) vs. uncomplicated: 980.4 (131) µg/L |
| [89] Rathore, India a | 14 PE 47 uncomplicated | Serum zinc Collected at delivery Flame AAS | NS mean (SD) serum zinc between women with PE and those with uncomplicated pregnancies. PE: 492 (178) vs. uncomplicated: 575 (216) μg/L |
| [90] Kolusari, Turkey a | 47 PE 48 uncomplicated | Serum zinc Collected between 29 and 38 weeks AAS | NS mean (SD) serum zinc between women with PE women and those with uncomplicated pregnancies. PE: 10.6 (4.4) vs. uncomplicated: 12.7 (4.1) µg/L |
| [91] Atamer, Turkey a | 32 PE 28 uncomplicated | Fasting serum zinc Collected at 28–29 weeks Flame AAS | NS in mean (SD) serum zinc between women with PE and women with uncomplicated pregnancies. PE: 792 (180) vs. uncomplicated: 1086 (199) μg/L |
| [92] Adam, Turkey a | 20 PE 20 uncomplicated | Plasma zinc Collected before the onset of labor Flame AAS | NS mean (SD) plasma zinc in women with PE compared to women with an uncomplicated pregnancy. PE: 313 (47) vs. uncomplicated: 341 (44) µg/L |
| [93] Vigeh, Iran a | 31 PE 365 uncomplicated | Heparin plasma zinc Collected at delivery Inductively coupled plasma mass spectrometry | NS mean (SD) plasma zinc between women with PE women and women with uncomplicated pregnancies. PE: 5200 (1444) vs. uncomplicated: 5561 (1057) µg/L |
| [32] Adeniyi, Nigeria a | 55 pregnant women | Plasma zinc Collection time not specified AAS | NS mean (SD) plasma zinc in women with PE compared to women with uncomplicated pregnancies. PE: 940 (270) vs. uncomplicated: 970 (230) μg/L |
| Author, Country | Sample Size | Zinc Measure | Outcome of the Study |
|---|---|---|---|
| (1) Sample Type | |||
| (2) Time at Which Gestation Diet Was Assessed or Sample Collected | |||
| (3) Method of Analysis | |||
| [44] Scholl, United States a | 115 with zinc intake ≤6 mg/day 699 with zinc intake ˃6 mg/day | Dietary zinc intake 28 and 36 weeks 24 h dietary recall | 2-fold ↓ risk of delivering a preterm infant with dietary zinc intake ˃6 mg/day. OR (LMP): 1.85, 95% CI: 1.09–3.12, OR (OE): 2.13, 95% CI: 1.20–3.79 2.75 to 3.44-fold ↓ risk of delivering a very preterm infant with dietary zinc intake ˃9 mg/day. OR (LMP): 2.75, 95% Cl: 1.31–5.77, OR (OE): 3.44, 95% Cl: 1.39–8.55 |
| [94] Carmichael, United States a,b | 413 preterm and 58 early preterm 5267 term | Dietary zinc intake Harvard food frequency questionnaires | 2-fold ↓ for preterm birth <32 weeks with zinc intake ˃ 8.0 mg/day compared to 8.0–14.2 mg/day. OR: 2.3, 95% CI: 1.2–4.5 |
| [45] Neggers, United States a | 238 preterm 1160 term | Dietary zinc intake 18 and 30 weeks 24 h dietary recall using the nutrient database developed by the University of Minnesota | NS association between low dietary zinc intake (less than median) and risk of PTB. OR: 1.1, 95% CI: 0.7–1.7 |
| [95] Hsu, Taiwan c | 28 preterm 423 term | Dietary zinc intake Each trimester 24 h dietary recall | NS in dietary zinc intake between each of the trimesters and in those who delivered preterm versus term. Preterm: 9.6–10.8 mg/day vs. term: 8.90–10.9 mg/day |
| Inadequate dietary zinc intake estimated to affect <17% of the studied population | |||
| [96] Wang, China a | 169 preterm 2912 uncomplicated | Fasting serum zinc First and second trimester Flame AAS | ↑ risk of preterm birth with serum zinc <767 μg/L and serum zinc between 767 and 996 μg/L. aOR: 2.41, 95% CI: 1.57, 3.70; aOR: 1.97, 95% CI: 1.27, 3.05, p < 0.001 for both, respectively |
| [50] Bro, Denmark c | 34 preterm 220 uncomplicated | Serum zinc Collected at delivery Flame AAS | NS mean (SD) serum zinc levels in women who delivered preterm compared to term women. Preterm: 666.7 (104.6) vs. term: 679.7 (98) μg/L |
| [54] Tamura, United States c | 505 preterm and 136 early preterm 2038 uncomplicated | Non-fasting heparin plasma zinc Collected at first prenatal visit (6 to 34 weeks) Flame AAS | NS in the prevalence or n (%) of PTB measured between the lowest quartile and upper three quartiles of zinc. Highest: 373 (14.5) vs. lowest: 132 (15.3) NS in the prevalence (n (%)) of early PTB measured between the lowest quartile and upper three quartiles of zinc. Highest: 107 (4.2) vs. lowest: 29 (3.4) |
| Inadequate dietary zinc intake estimated to affect ≥17% of the studied population | |||
| [66] Jeswani, India c | 25 preterm 25 term | Serum zinc Collected at 28–40 weeks AAS | ↑ mean (SD) serum zinc in women who delivered preterm women compared to term. Preterm: 1154.4 (154.1) vs. uncomplicated: 962.8 (194.8) µg/L, p ˂ 0.01 |
| [64] Goel, India d | 20 preterm 25 term | Heparin plasma zinc Collected at delivery AAS | ↑ mean (SD) plasma zinc in mothers who delivered preterm compared to term mothers. Preterm: 842 (43) vs. term: 744 (51) μg/L, p ˂ 0.001 |
| [60] Bahl, India a | 10 preterm 97 term | Serum zinc Collected at delivery Flame AAS | NS mean (SD) in women who delivered Preterm that were an appropriate weight for date compared to uncomplicated. Preterm: 627 (212) vs. uncomplicated: 670 (96) µg/L |
| [65] Srivastava, India c | 26 preterm 23 term | Heparin plasma zinc Collected at delivery Flame AAS | NS mean (SD) plasma zinc between preterm and term mothers. Preterm: 6350 (2640) vs. term: 6310 (5090) μg/L |
| Author, Country | Sample Size | Zinc Measure | Outcome of the Study |
|---|---|---|---|
| (1) Sample Type | |||
| (2) Time at Which Gestation Diet Was Assessed or Sample Collected | |||
| (3) Method of Analysis | |||
| [97] Bo, Italy a,b | 126 GDM and 84 aOGTT 294 uncomplicated | Dietary zinc intake 24–28 weeks Food frequency questionnaire | ↓ mean (SD) daily zinc intake between GDM and aOGTT women and women with uncomplicated pregnancies. GDM: 8.5 (2.4) and aOGTT: 8.7 (2.5) vs. uncomplicated: 9.4 (2.8) mg/day, p = 0.007 |
| [98] Behboudi-Gandevani S, Iran a | 72 with GDM 961 uncomplicated | Dietary zinc intake 14–20 weeks Semi-quantitative food frequency questionnaire | NS in mean (SD) daily zinc intake between GDM and those with uncomplicated pregnancies. GDM: 6.91 (3.42) vs. uncomplicated: 10.1 (7.45) mg/day |
| Inadequate dietary zinc intake estimated to affect <17% of the studied population | |||
| [48] Borella, Italy a | 18 GDM 35 uncomplicated | Heparin plasma zinc Collected in the third trimester Flame AAS | ↑ mean (SD) plasma zinc in GDM women compared to women with uncomplicated pregnancies. GDM: 766.6 (117.6) vs. uncomplicated: 627.5 (150) µg/L, p ˂0.001 |
| [35] Wang, China a,c | 46 GDM and 98 IGT 90 uncomplicated | Plasma zinc Collection time not specified Inductively coupled plasma atomic emission spectroscopy | NS in mean (SD) plasma zinc between women with IGT and women with uncomplicated pregnancies. IGT: 1080 (270) vs. uncomplicated: 1130 (330) μg/L NS mean (SD) plasma zinc between women with GDM and those with uncomplicated pregnancies. GDM:1020 (190) vs. uncomplicated: 1130 (330) μg/L |
| [38] Hyvonen-Dabek, Finland d | 5 GDM 10 uncomplicated | Serum zinc Collection time not specified Particle induced X-ray emission | NS mean (SD) serum zinc in women with GDM compared to women with uncomplicated pregnancies. GDM: 1070 (190) vs. uncomplicated: 1150 (220) µg/L |
| [99] Wibell, Sweden d | 20 GDM 13 uncomplicated | Serum zinc Collected across gestation AAS | NS mean (SD) serum zinc between women with GDM and those with uncomplicated pregnancies. GDM: 700 (100) vs. uncomplicated: 700 (80) μg/L |
| Inadequate dietary zinc intake estimated to affect ≥17% of the studied population | |||
| [98] Behboudi-Gandevani, Iran a | 72 with GDM 961 uncomplicated | Serum zinc Collected 14–20 weeks Flame AAS | NS mean serum zinc between GDM and women with uncomplicated pregnancies. GDM: 844 (440) vs. uncomplicated: 835 (444) μg/L |
| [100] Al-Saleh, Kuwait a | 30 GDM 30 uncomplicated | Serum zinc Collected at delivery Furnace AAS | NS mean (SEM) serum zinc in women with GDM compared to women with uncomplicated pregnancies. GDM: 610.3 (60.1) vs. uncomplicated: 656.2 (241.4) µg/L |
| Dietary Zinc Intake | ||||
| Total No. Reference | LBW/SGA | Hypertensive Disorders of Pregnancy | sPTB | GDM |
| 9 | 4 | 1 | 4 | 2 |
| 3 reported a negative association [42,43,44] | Reported no association [70] | 2 reported a negative association [44,93] | 1 reported a negative association [96] | |
| 1 reported no association [45] | 2 reported no association [45,94] | 1 reported no association [97] | ||
| Serum/Plasma Zinc | ||||
| Total No. Reference | LBW/SGA | Hypertensive Disorders of Pregnancy | sPTB | GDM |
| 58 | 26 | 33 | 7 | 6 |
| No. where inadequate zinc intake affects <17% of the population | ||||
| 12 | 13 | 3 | 4 | |
| 2 reported a negative association [46,49] | 5 reported a negative association [55,71,72,73,74] | 1 reported a positive association [95] | 1 reported a positive association [48] | |
| 2 reported a positive association [47,48] | 8 reported no association [38,48,53,75,76,77,78,79] | 2 reported no association [50,53] | 3 reported no association [35,38,98] | |
| 8 reported no association [38,50,51,52,53,54,55,56] | ||||
| No. where inadequate zinc intake affects ≥17% of the population | ||||
| 14 | 20 | 4 | 2 | |
| 5 reported a negative association [57,58,59,60,61] | 10 reported a negative association [33,34,36,37,39,80,81,82,83,100] | 2 reported a positive association [64,66] | 2 reported no association [97,99] | |
| 2 reported a positive association [63,101] | 1 reported a positive association [84] | 2 reported no association [60,65] | ||
| 6 reported no association [64,65,66,67,68,69] | 9 reported no association [32,85,86,87,88,89,90,91,92] | |||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, R.L.; Grieger, J.A.; Bianco-Miotto, T.; Roberts, C.T. Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients 2016, 8, 641. https://doi.org/10.3390/nu8100641
Wilson RL, Grieger JA, Bianco-Miotto T, Roberts CT. Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients. 2016; 8(10):641. https://doi.org/10.3390/nu8100641
Chicago/Turabian StyleWilson, Rebecca L., Jessica A. Grieger, Tina Bianco-Miotto, and Claire T. Roberts. 2016. "Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review" Nutrients 8, no. 10: 641. https://doi.org/10.3390/nu8100641
APA StyleWilson, R. L., Grieger, J. A., Bianco-Miotto, T., & Roberts, C. T. (2016). Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients, 8(10), 641. https://doi.org/10.3390/nu8100641