Are Reductions in Population Sodium Intake Achievable?

{kind=link}
Abstract
1. Introduction
2. Can Reducing Sodium in Packaged and Restaurant Foods Reduce Population Sodium Intake?
3. Significant Reductions in Mean Population Sodium Intake Can Be Achieved with Gradual Reduction of Sodium in the Food Supply
4. Sodium in Certain Foods Can be Gradually Reduced without Affecting Taste or Changing Consumer Consumption Patterns
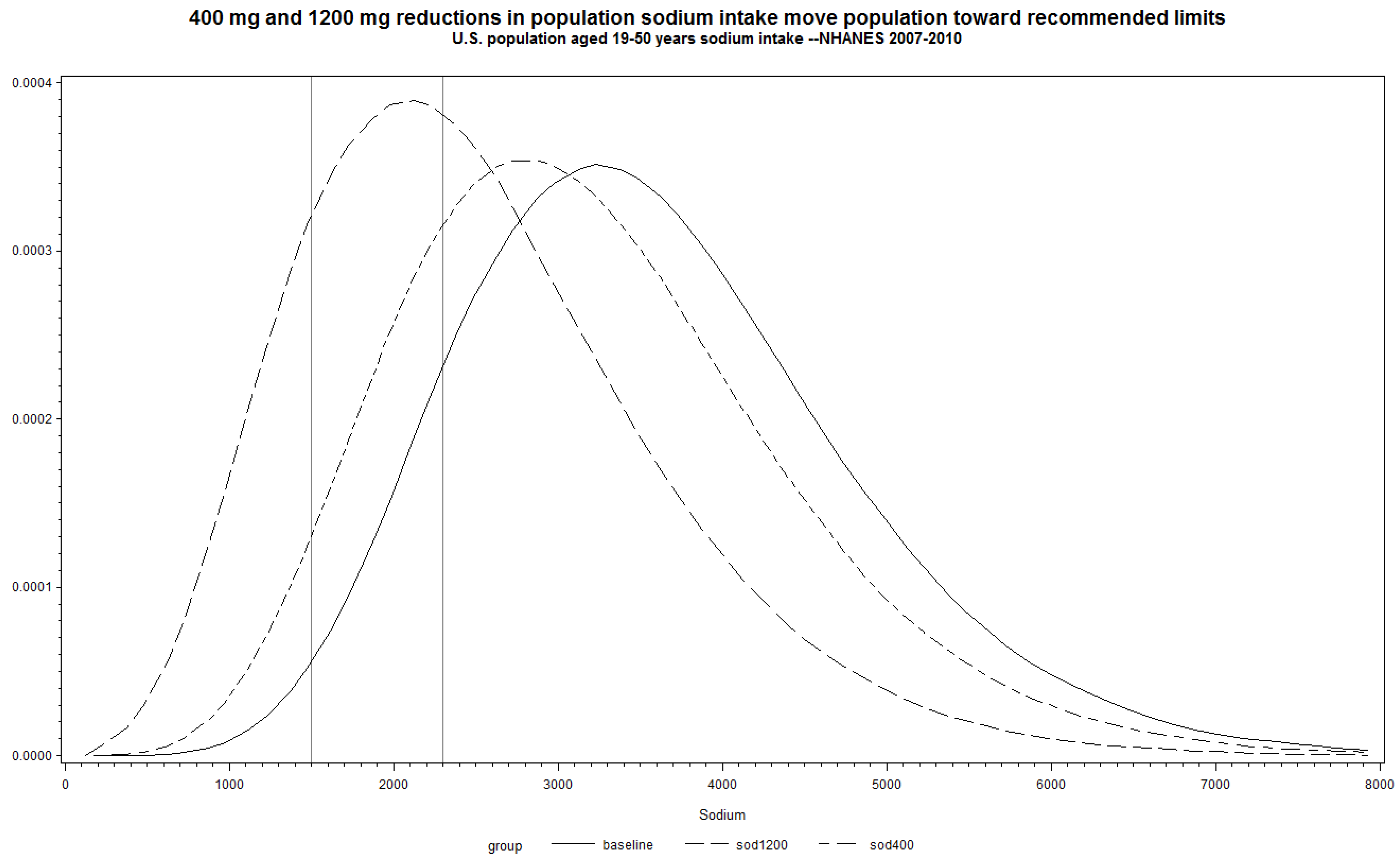
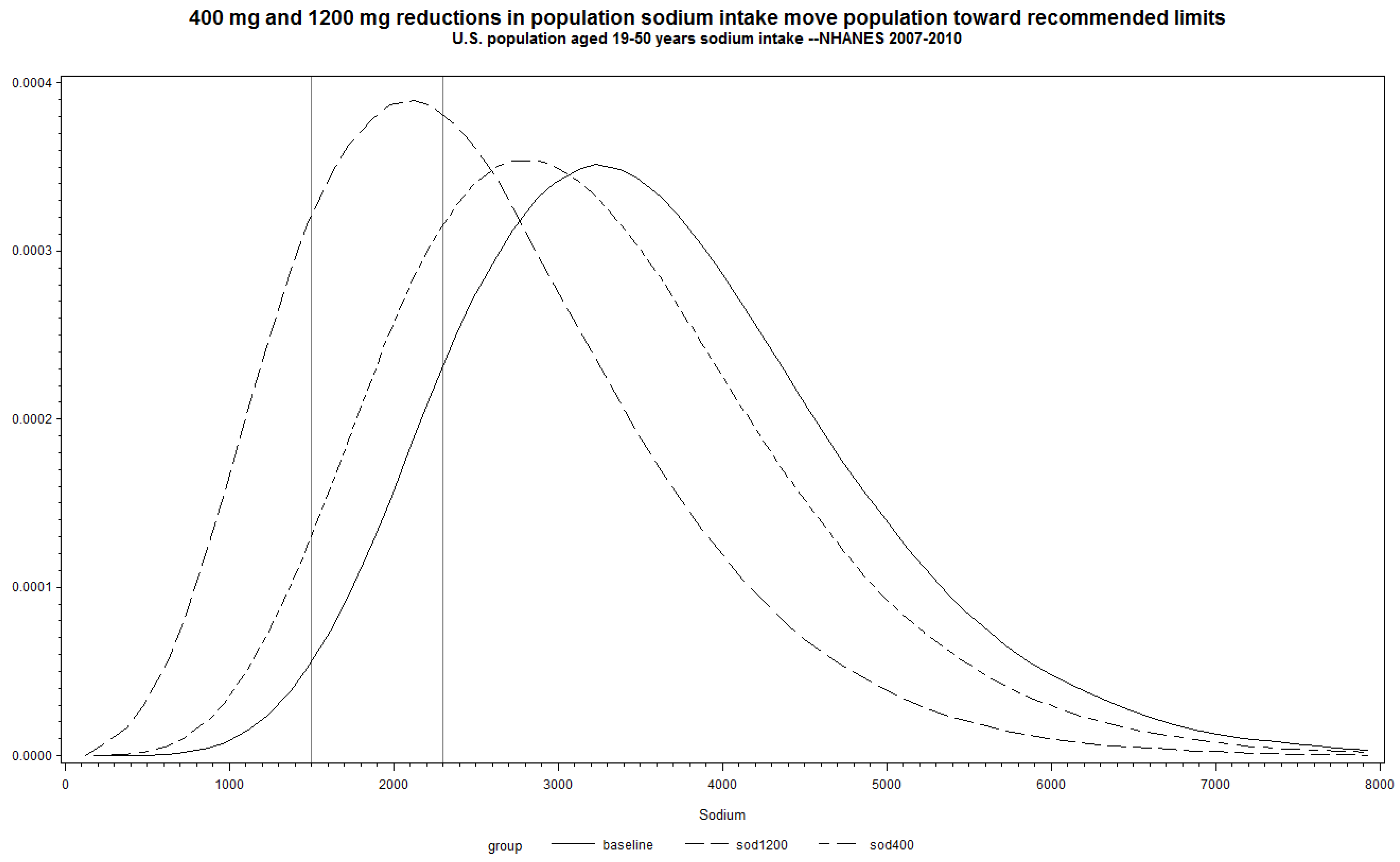
5. Shifting Mean Population Sodium Intake Can Move US toward Meeting the Current Individual Guidelines for Sodium Intake
6. Conclusion
Acknowledgements
Author Contributions
Conflicts of Interest
References and Notes
- Institute of Medicine. Strategies to Reduce Sodium Intake in the United States; National Academies: Washington, DC, USA, 2010. [Google Scholar]
- Mattes, R.D.; Donnelly, D. Relative contributions of dietary sodium sources. J. Am. Coll. Nutr. 1991, 10, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Sodium Intake in Populations: Assessment of Evidence; National Academies: Washington, DC, USA, 2013. [Google Scholar]
- U.S. Department of Health and Human Services. Available online: http://healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=29#149 (accessed on 23 May 2014).
- This manuscript uses both sodium and salt. To convert from mg sodium to mg salt, multiply the mg sodium by 2.5.
- McCarron, D.; Drüeke, T.; Stricker, E. Science trumps politics: Urinary sodium data challenge US dietary sodium guideline. Am. J. Clin. Nutr. 2010, 92, 1005–1006. [Google Scholar] [CrossRef] [PubMed]
- Coxson, P.; Cook, N.; Joffres, M.; Hong, Y.; Orenstein, D.; Schmidt, S.; Bibbins-Domingo, K. Mortality benefits from US population—Wide reduction in sodium consumption—Projections from three modeling approaches. Hypertension 2013, 61, 564–570. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ayala, C.; Gillespie, C.; Cogswell, M.; Keenan, N.L.; Merritt, R. Sodium consumption among hypertensive adults advised to reduce their intake—National health and nutrition examination survey, 1999–2004. J. Clin. Hypertens. 2012, 14, 447–454. [Google Scholar] [CrossRef]
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and potassium intake among US adults—National health and nutrition examination survey, 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Tian, N.; Zhang, Z.; Loustalot, F.; Yang, Q.; Cogswell, M.E. Sodium and potassium intake among infants and preschool children, United States, 2001–2008. Am. J. Clin. Nutr. 2013, 98, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Usual sodium intakes compared with current dietary guidelines, United States, 2005–2008. Morb. Mortal. Wkly. Rep. 2011, 60, 1413–1417. [Google Scholar]
- Centers for Disease Control and Prevention. Vital signs: Food categories contributing the most to sodium consumption, United States, 2007–2008. Morb. Mortal. Wkly. Rep. 2012, 61, 92–98. [Google Scholar]
- Centers for Disease Control and Prevention. Vital Signs: Where’s the Sodium. Available online: http://www.cdc.gov/vitalsigns/sodium/ (accessed on 17 June 2014).
- World Action on Salt and Health. International Products Survey. Available online: http://www.worldactiononsalt.com/less/surveys/2009/international/index.html (accessed on 17 June 2014).
- Dunford, E.; Webster, J.; Woodward, M.; Czernichow, S.; Yuan, WL.; Jenner, K.; Ni, Mhurchu C.; Jacobson, M.; Campbell, N.; Neal, B. The variability of reported salt levels in fast foods across six countries: Opportunities for salt reduction. Can. Med. Assoc. J. 2012, 184, 1023–1028. [Google Scholar] [CrossRef]
- Webster, J.L.; Dunford, E.K.; Hawkes, C.; Neal, B.C. Salt reduction initiatives around the world. J. Hypertens. 2011, 29, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- World Action on Salt and Health. Finland: Salt Action Summary. Available online: http://www.worldactiononsalt.com/worldaction/europe/53774.html (accessed on 2 June 2014).
- Pietinen, P.; Valsta, L.M.; Hirvonen, T.; Sinkko, H. Labelling the salt content in foods: A useful tool in reducing sodium intake in Finland. Public Health Nutr. 2008, 11, 335–340. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Pombo-Rodrigues, S.; MacGregor, G.A. Salt reduction in England from 2003 to 2011: Its relationship to blood pressure, stroke and ischaemic heart disease mortality. BMJ Open 2014, 4, e004549. [Google Scholar] [CrossRef] [PubMed]
- Brinsden, H.C.; He, F.J.; Jenner, K.H.; Macgregor, G.A. Surveys of the salt content in UK bread: Progress made and further reductions possible. BMJ Open 2013, 3, e002936. [Google Scholar] [CrossRef] [PubMed]
- Food Safety Authority of Ireland. Positive Update on National Programme to Reduce Salt—More Effort Needed to Protect Consumer Health Says FSAI. Available online: http://www.fsai.ie/news_centre/press_releases/19092007.html (accessed on 26 June 2014).
- Drake, S.L.; Lopetcharat, K.; Drake, M.A. Salty taste in dairy foods: Can we reduce the salt? J. Dairy Sci. 2011, 94, 636–645. [Google Scholar] [CrossRef]
- Grummer, J.; Bobowski, N.; Karalus, M.; Vickers, Z.; Schoenfuss, T. Use of potassium chloride and flavor enhancers in low sodium Cheddar cheese. J. Dairy Sci. 2013, 96, 1401–1418. [Google Scholar] [CrossRef] [PubMed]
- Ayyash, M.; Sherkat, F.; Shah, N. Effect of partial NaCl substitution with KCl on the texture profile, microstructure, and sensory properties of low-moisture mozzarella cheese. J. Dairy Res. 2013, 80, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Apro, N.; Ferreira, V.; Virgolini, M.; Aguilar, V.; Sosa, M.; Perel, P.; Casas, J. Feasibility of salt reduction in processed foods in Argentina. Rev. Panam. Salud Publica 2011, 29, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Bolhuis, D.; Temme, E.; Koeman, F.; Noort, M.; Stefanie, K.S.; Janssen, A. Salt reduction of 50% in bread does not decrease bread consumption or increase sodium intake by the choice of sandwich fillings. J. Nutr. 2011, 141, 2249–2255. [Google Scholar] [CrossRef] [PubMed]
- Braschi, A.; Gill, L.; Naismith, D. Partial substitution of sodium with potassium in white bread: Feasibility and bioavailability. Int. J. Food Sci. Nutr. 2009, 60, 507–521. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, R.; Farleigh, C.A.; Wharf, S.G. Limited compensation by table salt for reduced salt within a meal. Appetite 1989, 13, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, G.K.; Bertino, M.; Engelman, K. Failure to compensate decreased dietary sodium with increased table salt usage. J. Am. Med. Assoc. 1987, 258, 3275–3278. [Google Scholar] [CrossRef]
- Sasaki, N. The relationship of salt intake to hypertension in the Japanese. Geriatrics 1964, 19, 735–744. [Google Scholar] [PubMed]
- Usual Dietary Intakes: SAS Macros for the NCI Method. Available online: http://appliedresearch.cancer.gov/diet/usualintakes/macros.html (accessed on 23 June 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levings, J.L.; Cogswell, M.E.; Gunn, J.P. Are Reductions in Population Sodium Intake Achievable? Nutrients 2014, 6, 4354-4361. https://doi.org/10.3390/nu6104354
Levings JL, Cogswell ME, Gunn JP. Are Reductions in Population Sodium Intake Achievable? Nutrients. 2014; 6(10):4354-4361. https://doi.org/10.3390/nu6104354
Chicago/Turabian StyleLevings, Jessica L., Mary E. Cogswell, and Janelle Peralez Gunn. 2014. "Are Reductions in Population Sodium Intake Achievable?" Nutrients 6, no. 10: 4354-4361. https://doi.org/10.3390/nu6104354
APA StyleLevings, J. L., Cogswell, M. E., & Gunn, J. P. (2014). Are Reductions in Population Sodium Intake Achievable? Nutrients, 6(10), 4354-4361. https://doi.org/10.3390/nu6104354