Short Term (14 Days) Consumption of Insoluble Wheat Bran Fibre-Containing Breakfast Cereals Improves Subjective Digestive Feelings, General Wellbeing and Bowel Function in a Dose Dependent Manner


Abstract
:1. Introduction
2. Materials and Methods
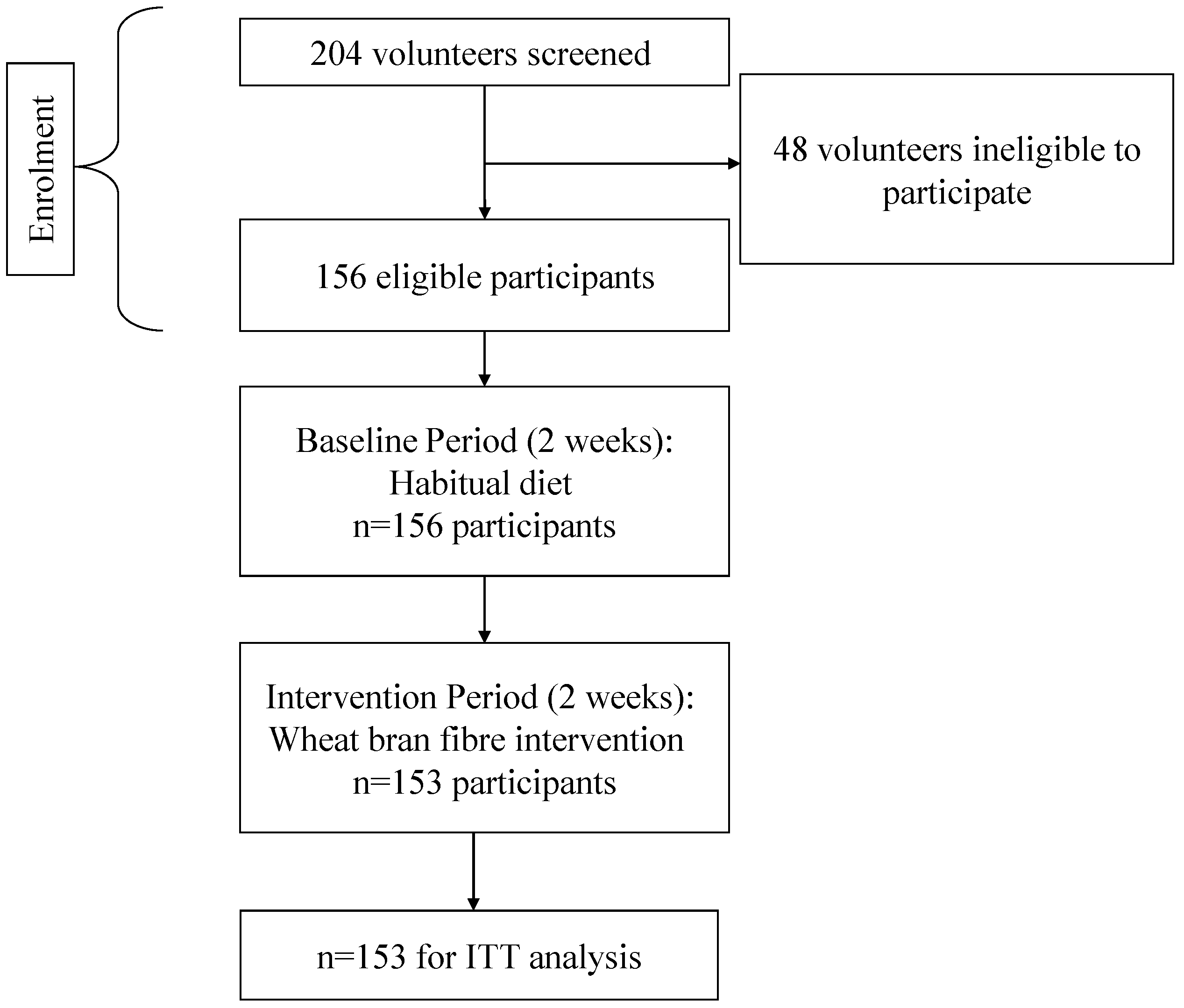
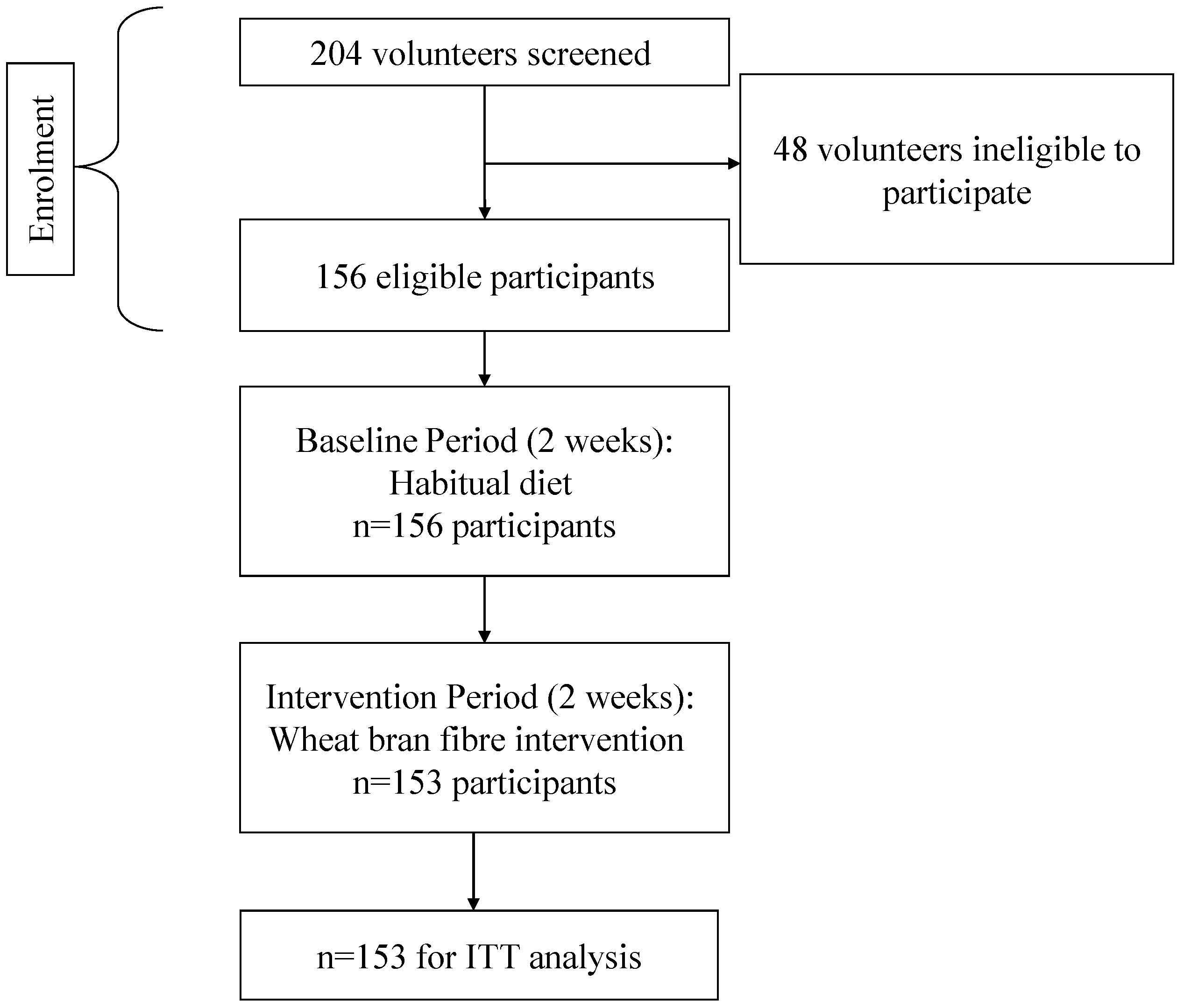
2.1. Participants
2.2. Study Design
2.3. Study Procedure

{kind=link}
| Breakfast Cereal Type | Fibre (g) per 100 g | Weight (g) Cereal per Scoop | Fibre (g) per Scoop |
|---|---|---|---|
| Bran Shreds | 27 | 36 | 9.72 |
| Wheat Bran Flakes | 15 | 30 | 4.50 |
| Wheat Bran Flakes with Sultanas | 13 | 30 | 3.90 |
| Frosted Mini Wheats | 9 | 30 | 2.70 |
| Raisin Mini Wheats | 9 | 30 | 2.70 |
| Chocolate Wheat Bran Flakes | 13 | 30 | 3.90 |
| Apple & Fig Wheat Bran Flakes | 15 | 40 | 6.00 |
| Mean | 14.4 | 32.3 | 4.8 |
2.4. Statistical Analysis
- Group 1 (n = 35): 2 scoops or fewer per day (i.e., scoops ≤ 2);
- Group 2 (n = 52): more than 2, but no more than 2.5 scoops (i.e., 2 < scoops ≤ 2.5);
- Group 3 (n = 29): more than 2.5, but no more than 3 scoops (i.e., 2.5 < scoops ≤ 3);
- Group 4 (n = 37): more than 3 scoops (i.e., scoops > 3).
- Decrease in symptoms (intervention response < baseline response, off diagonal response);
- No change (i.e., intervention response = baseline response, on diagonal response);
- Increase in symptoms (i.e., intervention response > baseline response, off diagonal response).
3. Results
3.1. Participant Characteristics
3.2. Breakfast Cereal and Fibre Intake
3.3. Digestive Feelings
| Baseline Period (day 1 to 14) | Fibre Intervention Period (day 15 to 28) | Wilcoxon Signed Rank (S) | Significance (p-value) | |
|---|---|---|---|---|
| Digestive Feelings | ||||
| Wind | 1.11 ± 0.95 | 1.22 ± 1.04 | 54,109.5 | <0.0001 |
| Constipation | 0.43 ± 0.80 | 0.36 ± 0.69 | −19,153.0 | 0.0002 |
| Indigestion | 0.29 ± 0.61 | 0.27 ± 0.58 | −4297.0 | NS |
| Bloated | 0.76 ± 0.97 | 0.57 ± 0.82 | −67,846.0 | <0.0001 |
| Sluggish | 0.66 ± 0.89 | 0.43 ± 0.71 | −81,060.5 | <0.0001 |
| Digestive discomfort | 0.46 ± 0.81 | 0.40 ± 0.72 | −19,829.5 | 0.0004 |
| Pain in the digestive system | 0.27 ± 0.64 | 0.29 ± 0.63 | 5001.5 | NS |
| Bowel Function | ||||
| Ease of defecation | 1.29 ± 1.01 | 1.06 ± 0.90 | −73,602.5 | <0.0001 |
| Satisfaction of bowel movement | 2.34 ± 1.13 | 2.53 ± 1.07 | 64,513.5 | <0.0001 |
| Stool Type | 3.49 ± 1.28 | 3.80 ± 1.14 | 84,255.5 | <0.0001 |
| Stool Quantity | 0.84 ± 0.61 | 0.90 ± 0.62 | 35,567.0 | <0.0001 |
| General Wellbeing | ||||
| Mental alertness | 1.91 ± 0.91 | 2.01 ± 0.88 | 37,017.0 | <0.0001 |
| Feeling slim | 1.37 ± 1.07 | 1.57 ± 1.11 | 82,233.5 | <0.0001 |
| Feeling happy | 2.07 ± 0.87 | 2.19 ± 0.86 | 54,553.5 | <0.0001 |
| Stress | 0.99 ± 0.99 | 0.82 ± 0.92 | −63,785.5 | <0.0001 |
| Mental tiredness | 1.18 ± 1.0 | 0.97 ± 0.91 | −92,963.5 | <0.0001 |
| Headache | 0.41 ± 0.81 | 0.33 ± 0.68 | −17,583.0 | 0.0005 |
| Feeling energetic | 1.61 ± 0.92 | 1.81 ± 0.91 | 88,172.5 | <0.0001 |
| Feeling fat | 0.95 ± 1.11 | 0.74 ± 0.95 | −65,848.0 | <0.0001 |
| Difficulty concentrating | 0.91 ± 0.98 | 0.71 ± 0.82 | −74,811.0 | <0.0001 |
| Physical tiredness | 1.27 ± 1.06 | 0.98 ± 0.94 | −131,389.0 | <0.0001 |
| Baseline Period (day 1 to 14) | Fibre Intervention Period (day 15 to 28) | |
|---|---|---|
| Digestive Feelings | ||
| Wind | ||
| None | 645 (30.3) | 622 (29.2) |
| Minimal | 791 (37.2) | 724 (34.0) |
| Moderate | 503 (23.7) | 514 (24.1) |
| A lot/Very | 178 (8.4) | 240 (11.2) |
| Extreme | 9 (0.4) | 32 (1.5) |
| Constipation | ||
| None | 1534 (72.3) | 1585 (74.5) |
| Minimal | 334 (15.8) | 362 (17.0) |
| Moderate | 191 (9.0) | 147 (6.9) |
| A lot/Very | 51 (2.4) | 29 (1.4) |
| Extreme | 11 (0.5) | 5 (0.2) |
| Indigestion | ||
| None | 1650 (78.0) | 1692 (79.5) |
| Minimal | 336 (15.9) | 314 (14.7) |
| Moderate | 105 (4.9) | 113 (5.3) |
| A lot/Very | 23 (1.1) | 11 (0.5) |
| Extreme | 1 (0.1) | 0 (0.0) |
| Bloated | ||
| None | 1137 (53.5) | 1299 (61.0) |
| Minimal | 517 (24.4) | 512 (24.0) |
| Moderate | 312 (14.7) | 255 (12.0) |
| A lot/Very | 146 (6.9) | 61 (2.9) |
| Extreme | 10 (0.5) | 2 (0.1) |
| Sluggish | ||
| None | 1212 (57.0) | 1458 (68.4) |
| Minimal | 522 (24.6) | 472 (22.2) |
| Moderate | 295 (13.9) | 166 (7.8) |
| A lot/Very | 87 (4.1) | 33 (1.5) |
| Extreme | 8 (0.4) | 1 (0.1) |
| Digestive discomfort | ||
| None | 1483 (70.0) | 1533 (71.9) |
| Minimal | 361 (17.0) | 400 (18.8) |
| Moderate | 207 (9.8) | 150 (7.0) |
| A lot/Very | 63 (3.0) | 47 ( 2.2) |
| Extreme | 5 (0.2) | 1 (0.1) |
| Pain in the digestive system | ||
| None | 1735 (81.7) | 1679 (78.8) |
| Minimal | 249 (11.7) | 311 (14.6) |
| Moderate | 104 (4.9) | 106 (5.1) |
| A lot/Very | 32 (1.5) | 31 (1.4) |
| Extreme | 5 (0.2) | 1 (0.1) |
| Bowel Function | ||
| Ease of defecation | ||
| 0: Very easy, effortless | 449 (24.3) | 590 (30.4) |
| 1: Fairly easy | 679 (36.7) | 757 (39.1) |
| 2: Moderate, little effort required | 491 (26.6) | 485 (25.0) |
| 3: Required effort | 192 (10.5) | 91 (4.7) |
| 4: Difficult, straining required | 36 (1.9) | 15 ( 0.8) |
| 5: Difficult, painful, force required | 0 (0.0) | 0 (0.0) |
| Satisfaction of bowel movement | ||
| 0: Dissatisfied, feels like there is more | 100 (5.5) | 69 (3.6) |
| 1: Still feel like I need to go | 317 (17.4) | 234 (12.1) |
| 2: No descriptor provided | 602 (33.0) | 639 (33.2) |
| 3: No descriptor provided | 458 (25.2) | 574 (29.8) |
| 4: Almost perfect | 343 (18.9) | 410 ( 21.3) |
| 5: It’s all gone, I feel empty | 0 (0.0) | 0 (0.0) |
| Stool Type | ||
| 1: hard to pass | 187 (7.7) | 90 (3.4) |
| 2: hard to pass | 289 (12.1) | 192 (7.3) |
| 3: ideal consistency | 700 (29.3) | 678 (25.7) |
| 4: ideal consistency | 749 (31.3) | 1073 (40.8) |
| 5: Difficult to control | 340 (14.2) | 409 (5.6) |
| 6: Difficult to control | 99 (4.2) | 168 (6.4) |
| 7: Difficult to control | 28 (1.2) | 21 (0.8) |
| Stool Quantity | ||
| 0: less than average | 668 (27.8) | 659 (24.6) |
| 1: average | 1451 (60.6) | 1618 (60.5) |
| 2: more than average | 277 (11.6) | 397 (14.9) |
| General Wellbeing | ||
| Mental alertness | ||
| None | 222 (10.4) | 176 (8.3) |
| Minimal | 273 (12.8) | 234 (11.0) |
| Moderate | 1157 (54.3) | 1150 (54.3) |
| A lot/Very | 432 (20.4) | 506 (23.9) |
| Extreme | 45 (2.1) | 53 (2.5) |
| Feeling slim | ||
| None | 582 (27.4) | 458 (21.6) |
| Minimal | 515 (24.3) | 513 (24.3) |
| Moderate | 724 (34.1) | 679 (32.1) |
| A lot/Very | 262 (12.4) | 411 (19.4) |
| Extreme | 38 (1.8) | 55 (2.6) |
| Feeling happy | ||
| None | 122 (5.8) | 99 (4.7) |
| Minimal | 301 (14.2) | 237 (11.2) |
| Moderate | 1089 (51.3) | 1020 (48.2) |
| A lot/Very | 537 (25.3) | 675 (31.9) |
| Extreme | 74 (3.4) | 84 (4.0) |
| Stress | ||
| None | 822 (38.6) | 974 (46.0) |
| Minimal | 719 (33.8) | 668 (31.6) |
| Moderate | 412 (19.4) | 365 (17.2) |
| A lot/Very | 143 (6.7) | 90 (4.3) |
| Extreme | 32 (1.5) | 18 (0.9) |
| Mental tiredness | ||
| None | 650 (30.6) | 783 (37.0) |
| Minimal | 677 (31.9) | 713 (33.7) |
| Moderate | 575 (27.1) | 515 (24.4) |
| A lot/Very | 207 (9.7) | 100 (4.7) |
| Extreme | 16 (0.7) | 4 (0.2) |
| Headache | ||
| None | 1571 (74.1) | 1628 (77.1) |
| Minimal | 325 (15.3) | 313 (14.8) |
| Moderate | 143 (6.8) | 131 (6.2) |
| A lot/Very | 59 (2.8) | 35 (1.7) |
| Extreme | 21 (1.0) | 4 (0.2) |
| Feeling energetic | ||
| None | 292 (3.7) | 207 (9.8) |
| Minimal | 559 (26.3) | 444 (21.1) |
| Moderate | 994 (46.8) | 1048 (49.7) |
| A lot/Very | 242 (11.4) | 360 (17.1) |
| Extreme | 38 (1.8) | 49 (2.3) |
| Feeling fat | ||
| None | 1020 (48.1) | 1134 (54.0) |
| Minimal | 465 (21.9) | 508 (24.2) |
| Moderate | 404 (19.0) | 331 (15.8) |
| A lot/Very | 185 (8.7) | 116 (5.5) |
| Extreme | 49 (2.3) | 10 (0.5) |
| Difficulty concentrating | ||
| None | 926 (43.6) | 1051 (49.8) |
| Minimal | 649 (30.5) | 661 (31.3) |
| Moderate | 404 (19.0) | 355 (16.8) |
| A lot/Very | 117 (5.5) | 44 (2.1) |
| Extreme | 30 (1.4) | 0 (0.0) |
| Physical tiredness | ||
| None | 634 (29.7) | 824 (39.0) |
| Minimal | 592 (27.8) | 634 (30.0) |
| Moderate | 626 (29.4) | 534 (25.2) |
| A lot/Very | 248 (11.6) | 118 (5.6) |
| Extreme | 31 (1.5) | 5 (0.2) |
| Cereal Intake Group | Group 1 | Group 2 | Group 3 | Group 4 | ||
|---|---|---|---|---|---|---|
| Scoops ≤ 2 (n = 35) | 2 < Scoops ≤ 2.5 (n = 52) | 2.5 < Scoops ≤ 3 (n = 29) | Scoops > 3 (n = 37) | |||
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Critical Value 3 | Significance (p-value) | |
| Fibre Intake (g) | 10.7 ± 2.13 | 11.9 ± 2.82 | 14.2 ± 2.90 | 19.9 ± 4.49 | 61.56 | <0.0001 |
| Digestive Feelings | ||||||
| Wind | 1.24 ± 1.10 | 1.13 ± 0.99 | 1.23 ± 1.00 | 1.31 ± 1.05 | 9.43 | 0.0241 |
| Adjusted Mean | 1.26 | 1.14 | 1.22 | 1.30 | 3.05 | 0.0275 |
| Constipation | 0.47 ± 0.81 | 0.30 ± 0.63 | 0.28 ± 0.59 | 0.39 ± 0.71 | 20.26 | 0.0002 |
| Indigestion | 0.41 ± 0.69 | 0.20 ± 0.50 | 0.26 ± 0.57 | 0.25 ± 0.55 | 41.23 | <0.0001 |
| Bloated | 0.73 ± 0.90 | 0.57 ± 0.81 | 0.52 ± 0.77 | 0.47 ± 0.76 | 26.94 | 0.0001 |
| Sluggish | 0.51 ± 0.78 | 0.43 ± 0.70 | 0.33 ± 0.60 | 0.42 ± 0.71 | 12.11 | 0.0070 |
| Digestive discomfort | 0.49 ± 0.74 | 0.38 ± 0.71 | 0.35 ± 0.68 | 0.37 ± 0.74 | 19.98 | 0.0002 |
| Pain in the digestive system | 0.37 ± 0.66 | 0.30 ± 0.64 | 0.21 ± 0.55 | 0.28 ± 0.65 | 21.95 | <0.0001 |
| Bowel Function | ||||||
| Ease of defecation | 1.14 ± 0.90 | 1.10 ± 0.91 | 0.92 ± 0.83 | 1.06 ± 0.93 | 12.40 | 0.0061 |
| Adjusted Mean | 1.09 | 1.08 | 0.90 | 1.09 | 4.13 | 0.0063 |
| Satisfaction of bowel movement | 2.51 ± 1.09 | 2.55 ± 1.00 | 2.60 ± 1.09 | 2.47 ± 1.10 | 3.29 | NS |
| Stool Type | 3.48 ± 1.26 | 3.85 ± 1.12 | 3.93 ± 1.07 | 3.93 ± 1.05 | 43.82 | <0.0001 |
| Stool Quantity | 0.85 ± 0.60 | 0.92 ± 0.60 | 0.90 ± 0.66 | 0.93 ± 0.63 | 5.95 | NS |
| Adjusted Mean | 0.92 | 0.95 | 1.01 | 0.94 | 1.53 | NS |
| General Wellbeing | ||||||
| Mental alertness | 1.90 ± 0.83 | 2.08 ± 0.92 | 2.00 ± 0.94 | 1.90 ± 0.83 | 16.53 | 0.0009 |
| Adjusted Mean | 1.92 | 2.05 | 2.07 | 1.99 | 3.55 | 0.0139 |
| Feeling slim | 1.35 ± 1.08 | 1.68 ± 1.11 | 1.57± 1.13 | 1.62 ± 1.08 | 22.33 | <0.0001 |
| Adjusted Mean | 1.49 | 1.67 | 1.47 | 1.58 | 6.15 | 0.0004 |
| Feeling happy | 2.15 ± 0.73 | 2.23 ± 0.84 | 2.06 ± 1.00 | 2.28 ± 0.88 | 16.29 | 0.0010 |
| Stress | 0.84 ± 0.97 | 0.88 ± 0.90 | 0.95 ± 1.04 | 0.63 ± 0.77 | 29.75 | <0.0001 |
| Mental tiredness | 0.95 ± 0.91 | 1.04 ± 0.90 | 1.02 ± 0.91 | 0.87 ± 0.90 | 12.69 | 0.0053 |
| Headache | 0.32 ± 0.68 | 0.40 ± 0.73 | 0.29 ± 0.66 | 0.27 ± 0.62 | 15.30 | 0.0016 |
| Feeling energetic | 1.77 ± 0.81 | 1.79 ± 0.94 | 1.76 ± 0.97 | 1.91 ± 0.90 | 8.91 | 0.0305 |
| Adjusted Mean | 1.75 | 1.82 | 1.75 | 1.89 | 3.01 | 0.0291 |
| Feeling fat | 0.81 ± 1.02 | 0.84 ± 1.00 | 0.82 ± 0.90 | 0.48 ± 0.77 | 53.13 | <0.0001 |
| Difficulty concentrating | 0.64 ± 0.79 | 0.73 ± 0.83 | 0.83 ± 0.84 | 0.66 ± 0.80 | 15.82 | 0.0012 |
| Physical tiredness | 0.93 ± 0.90 | 1.02 ± 0.94 | 1.06 ± 0.98 | 0.91 ± 0.95 | 9.01 | 0.0292 |
| Adjusted Mean | 0.95 | 0.97 | 1.05 | 0.96 | 1.14 | NS |
| Bloated scores | 0 None | 1 Minimal | 2 Moderate | 3 A Lot/Very | 4 Extreme | Total |
|---|---|---|---|---|---|---|
| All scores at baseline | ||||||
| Baseline period | 1131 | 514 | 310 | 145 | 10 | 2110 |
| Fibre intervention period | 1289 | 504 | 254 | 61 | 2 | 2110 |
| Higher scores at baseline | ||||||
| Baseline period | 145 | 10 | 155 | |||
| Fibre intervention period | 50 | 49 | 38 | 17 | 1 | 155 |
| Bloated | Decrease in symptoms | No Change | Increase in symptoms | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Change in digestive feeling | −4 | −3 | −2 | −1 | 0 | +1 | +2 | +3 | +4 | |
| All scores at baseline | ||||||||||
| Frequency | 2 | 50 | 151 | 391 | 1175 | 250 | 78 | 13 | 0 | 2110 |
| Higher scores at baseline | ||||||||||
| Frequency | 2 | 50 | 51 | 35 | 17 | 0 | 0 | 0 | 0 | 155 |
3.4. Bowel Function
3.5. General Wellbeing
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Department of Health, Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy; Report on Health and Social Subjects 41; The Stationary Office: London, UK, 1991.
- Buttriss, J.L.; Stokes, C.S. Dietary fibre and health: An overview. Nutr. Bull. 2008, 33, 186–200. [Google Scholar] [CrossRef]
- Pereira, M.A.; O’Reilly, E.; Augustsson, K.; Fraser, G.E.; Goldbourt, U.; Heitmann, B.L.; Hallmans, G.; Knekt, P.; Liu, S.; Pietinen, P.; et al. Dietary fiber and risk of coronary heart disease. A pooled analysis of cohort studies. Arch. Intern. Med. 2004, 164, 370–376. [Google Scholar] [CrossRef]
- Wanders, J.; van den Borne, J.J.G.C.; de Graaf, C.; Hulshof, T.; Jonathan, M.C.; Kristensen, M.; Mars, M.; Schols, H.A.; Feskens, E.J.M. Effects of dietary fibre on subjective appetite, energy intake and body weight: A systematic review of randomized controlled trials. Obes. Rev. 2011, 12, 724–739. [Google Scholar]
- Cade, J.E.; Burley, V.J.; Greenwood, D.C. Dietary fibre and risk of breast cancer in the UK Women’s Cohort Study. Int. J. Epidemiol. 2007, 36, 431–438. [Google Scholar] [CrossRef]
- Bingham, S.A.; Day, N.E.; Luben, R.; Ferrari, P.; Slimani, N.; Norat, T.; Clavel-Chapelton, F.; Kesse, E.; Nieters, A.; Boeing, H.; et al. Dietary fibre in food and protection against colorectal cancer in the european prospective investigation into cancer and nutrition (epic): An observational study. Lancet 2003, 361, 1496–501. [Google Scholar] [CrossRef]
- Aldoori, W.; Ryan-Harshman, M. Preventing diverticular disease. Review of recent evidence on high-fibre diets. Can. Fam. Phys. 2002, 48, 1632–1637. [Google Scholar]
- Baghurst, K.I.; Hope, A.K.; Down, E.C. Dietary intake in a group of institutionalised elderly and the effect of a fibre supplementation programme on nutrient intake and weight gain. Commun. Health Stud. 1985, 9, 99–108. [Google Scholar] [CrossRef]
- Jones, A.; Lydeard, S. Irritable bowel syndrome in the general population. Br. Med. J. 1992, 304, 87–90. [Google Scholar] [CrossRef]
- Van Kerkhoven, L.A. Gastrointestinal symptoms are still common in a general Western population. Neth. J. Med. 2008, 66, 18–22. [Google Scholar]
- Longstreth, G.F.; Thompson, W.G.; Chey, W.D.; Houghton, L.A. Functional bowel disorders. Gastroenterology 2006, 130, 1480–1491. [Google Scholar] [CrossRef]
- Grabitske, H.A.; Slavin, J.L. Laxation and the like: Assessing digestive health. Nutr. Today 2008, 43, 193–198. [Google Scholar] [CrossRef]
- Internal Report to Kellogg Marketing & Sales, 2010; Taylor Nelson & Sofres (TNS) Research International: London, UK, 2010.
- Vecht, J.; Symersky, T.; Lamers, C.B.H.W.; Masclee, A.A.M. Efficacy of lower than standard doses of pancreatic enzyme supplementation therapy during acid inhibition in patients with pancreatic exocrine insufficiency. J. Clin. Gastroenterol. 2006, 40, 721–725. [Google Scholar] [CrossRef]
- Ringel-Kulka, T.; Palsson, O.S.; Maier, D.; Carroll, I.; Galanko, J.A.; Leyer, G.; Ringel, Y. Probiotic bacteria Lactobacillus acidophilus NCFM and Bifidobacterium lactis Bi-07 versus placebo for the symptoms of bloating in patients with functional bowel disorders. J. Clin. Gastroenterol. 2011, 45, 518–525. [Google Scholar] [CrossRef]
- Smith, A.P. Breakfast cereal, fibre, digestive problems and well-being. Curr. Top. Nutraceutical Res. 2010, 8, 1–10. [Google Scholar]
- Smith, A.P. The concept of wellbeing: relevance to nutrition research. Br. J. Nutr. 2005, 93, S1–S5. [Google Scholar] [CrossRef]
- Henderson, L.; Gregory, J.; Irving, K.; Swan, G. Energy, Protein, Carbohydrate, Fat and Alcohol Intake. In The National Diet and Nutrition Survey: Adults Aged 19 to 64 Years; The Stationary Office: London, UK, 2003; Volume 2. [Google Scholar]
- Graham, D.Y.; Moser, S.E.; Estes, M.K. The effect of bran on bowel function in constipation. Am. J. Gastroenterol. 1982, 77, 599–603. [Google Scholar]
- O’Sullivan, K. The superior benefits of wheat bran fibre in digestive health. Eur. Gastroenterol. Hepatol. Rev. 2012, 8, 90–93. [Google Scholar]
- Smith, A.; Bazzoni, C.; Beale, J.; Elliott-Smith, J.; Tiley, M. High fibre breakfast cereals reduce fatigue. Appetite 2001, 37, 1–3. [Google Scholar] [CrossRef]
- Smith, A.P. An investigation of the effects of breakfast cereals on alertness, cognitive function and other aspects of the well-being of children. Nutr. Neurosci. 2010, 13, 230–236. [Google Scholar] [CrossRef]
- Smith, A.P. Breakfast cereal, digestive problems and well-being. Stress Health 2011, 27, 388–394. [Google Scholar] [CrossRef]
- Lawton, C.; Struthers, L.; Hoyland, A.; Myrissa, K.; Dye, L. Effects of increasing dietary fibre on psychological wellbeing. Ann. Nutr. Metab. 2011, 58, 266. [Google Scholar]
- Roe, L.; Strong, C.; Whiteside, C.; Neil, A.; Mant, D. Dietary intervention in primary care: Validity of the DINE method for diet assessment. Fam. Pract. 1994, 11, 375–381. [Google Scholar] [CrossRef]
- Myrissa, K. The effects of Increasing Daily Fibre Intake on Body Weight, Appetite Control, Biomarkers of Health and Subjective Wellbeing in Overweight Women. Master’s Thesis, Institute of Psychological Sciences, University of Leeds, Leeds, UK, March 2011. [Google Scholar]
- Food Standards Agency, Food Portion Sizes, 3rd edThe Stationary Office: London, UK, 2002.
- O’Donnell, L.J.D.; Virjee, J.; Heaton, K.W. Detection of pseudodiarrhoea by a simple clinical assessment of intestinal transit time. Br. Med. J. 1990, 300, 439–440. [Google Scholar] [CrossRef]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef]
- Floch, M.H.; Fuchs, H.M. Modification of stool content by increased bran intake. Am. J. Clin. Nutr. 1978, 31, S185–S189. [Google Scholar]
- SAS Software, version 9.2, SAS Institute, Inc.: Cary, NC, USA, 2008.
- European Food Safety Authority. Scientific Opinion on the substantiation of health claims related to wheat bran fibre and increase in faecal bulk (ID 3066), reduction in intestinal transit time (ID 828, 839, 3067, 4699) and contribution to the maintenance or achievement of a normal body weight (ID 829) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2010, 8, 1817. [CrossRef]
- Cummings, J.H.; Bingham, S.A.; Heaton, K.W.; Eastwood, M.A. Fecal weight, colon cancer risk, and dietary intake of nonstarch polysaccharides (dietary fiber). Gastroenterology 1992, 103, 1783–1789. [Google Scholar]
- Lewis, S.J.; Heaton, K.W. Roughage revisited: The effect on intestinal function of inert plastic particles of different sizes and shape. Dig. Dis. Sci. 1999, 44, 744–748. [Google Scholar]
- Lattimore, P.; Walton, J.; Bartlett, S.; Hackett, A.; Stevenson, L. Regular consumption of a cereal breakfast. Effects on mood and body image satisfaction in adult non-obese women. Appetite 2010, 55, 512–521. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lawton, C.L.; Walton, J.; Hoyland, A.; Howarth, E.; Allan, P.; Chesters, D.; Dye, L. Short Term (14 Days) Consumption of Insoluble Wheat Bran Fibre-Containing Breakfast Cereals Improves Subjective Digestive Feelings, General Wellbeing and Bowel Function in a Dose Dependent Manner. Nutrients 2013, 5, 1436-1455. https://doi.org/10.3390/nu5041436
Lawton CL, Walton J, Hoyland A, Howarth E, Allan P, Chesters D, Dye L. Short Term (14 Days) Consumption of Insoluble Wheat Bran Fibre-Containing Breakfast Cereals Improves Subjective Digestive Feelings, General Wellbeing and Bowel Function in a Dose Dependent Manner. Nutrients. 2013; 5(4):1436-1455. https://doi.org/10.3390/nu5041436
Chicago/Turabian StyleLawton, Clare L., Jenny Walton, Alexa Hoyland, Elaine Howarth, Peter Allan, David Chesters, and Louise Dye. 2013. "Short Term (14 Days) Consumption of Insoluble Wheat Bran Fibre-Containing Breakfast Cereals Improves Subjective Digestive Feelings, General Wellbeing and Bowel Function in a Dose Dependent Manner" Nutrients 5, no. 4: 1436-1455. https://doi.org/10.3390/nu5041436
APA StyleLawton, C. L., Walton, J., Hoyland, A., Howarth, E., Allan, P., Chesters, D., & Dye, L. (2013). Short Term (14 Days) Consumption of Insoluble Wheat Bran Fibre-Containing Breakfast Cereals Improves Subjective Digestive Feelings, General Wellbeing and Bowel Function in a Dose Dependent Manner. Nutrients, 5(4), 1436-1455. https://doi.org/10.3390/nu5041436