

Choline in Pregnancy and Lactation: Essential Knowledge for Clinical Practice


Abstract
1. Introduction
2. Choline: Functions, Metabolism, and Maternal Needs
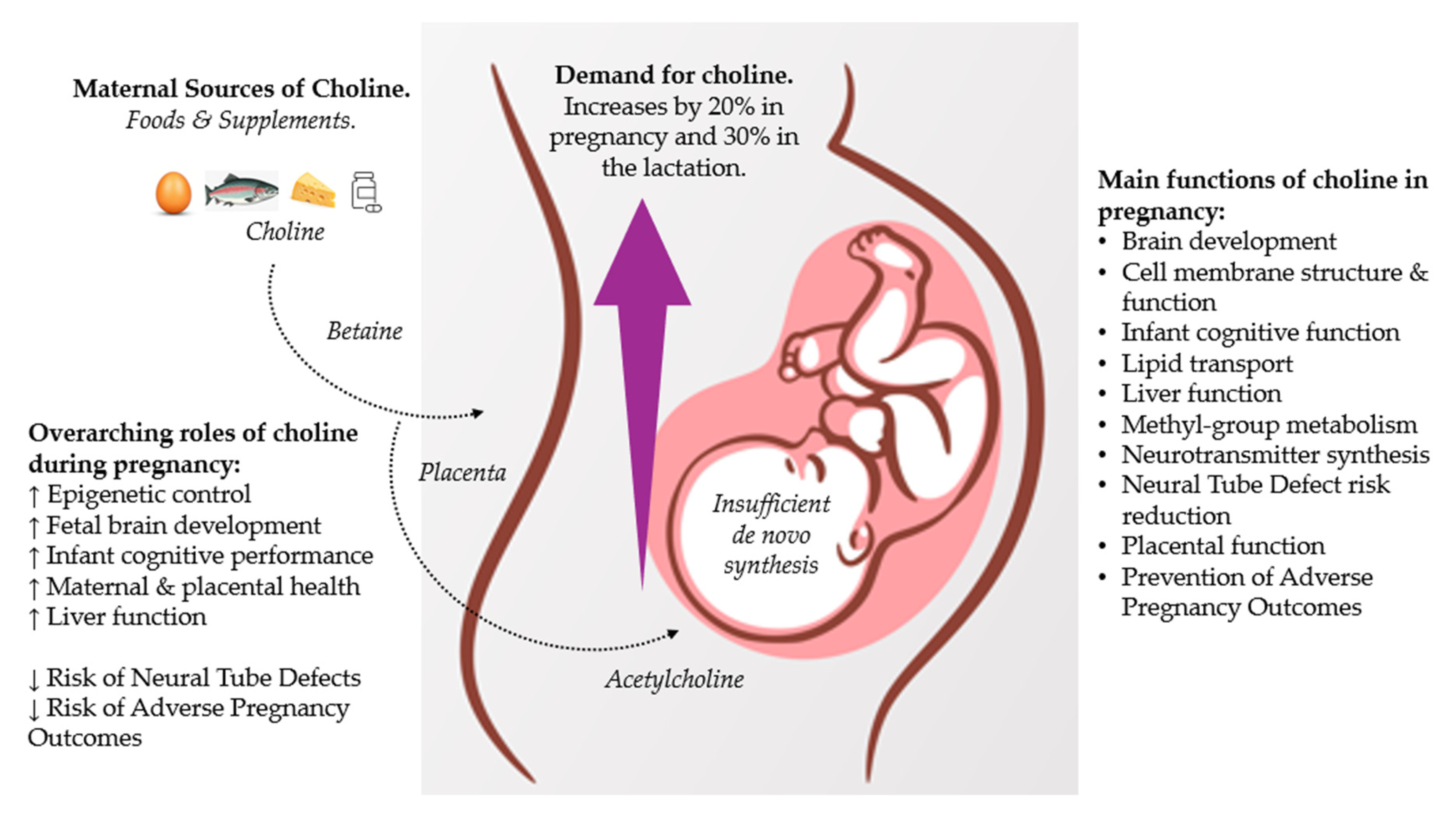
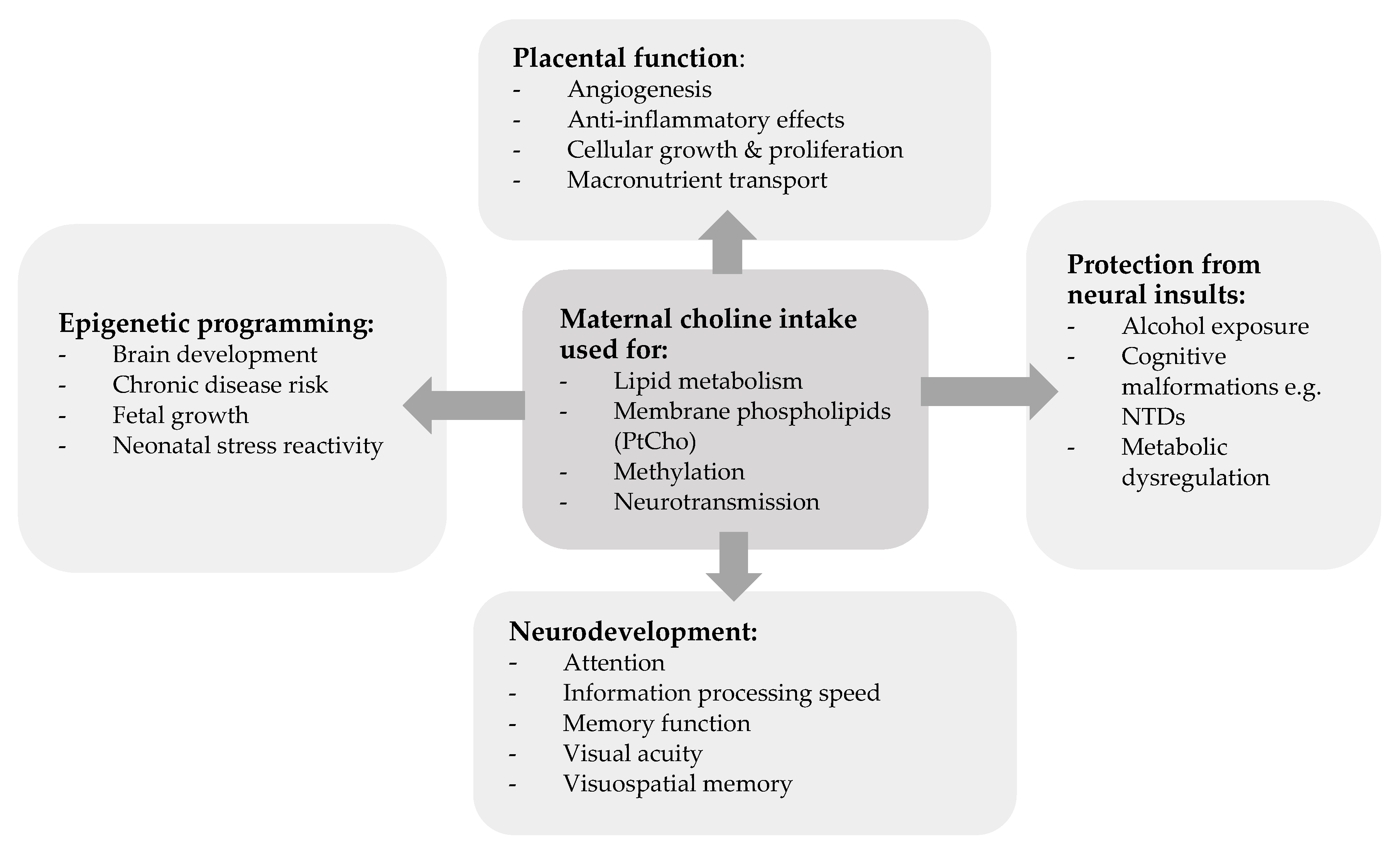
2.1. Functions
2.2. Metabolism
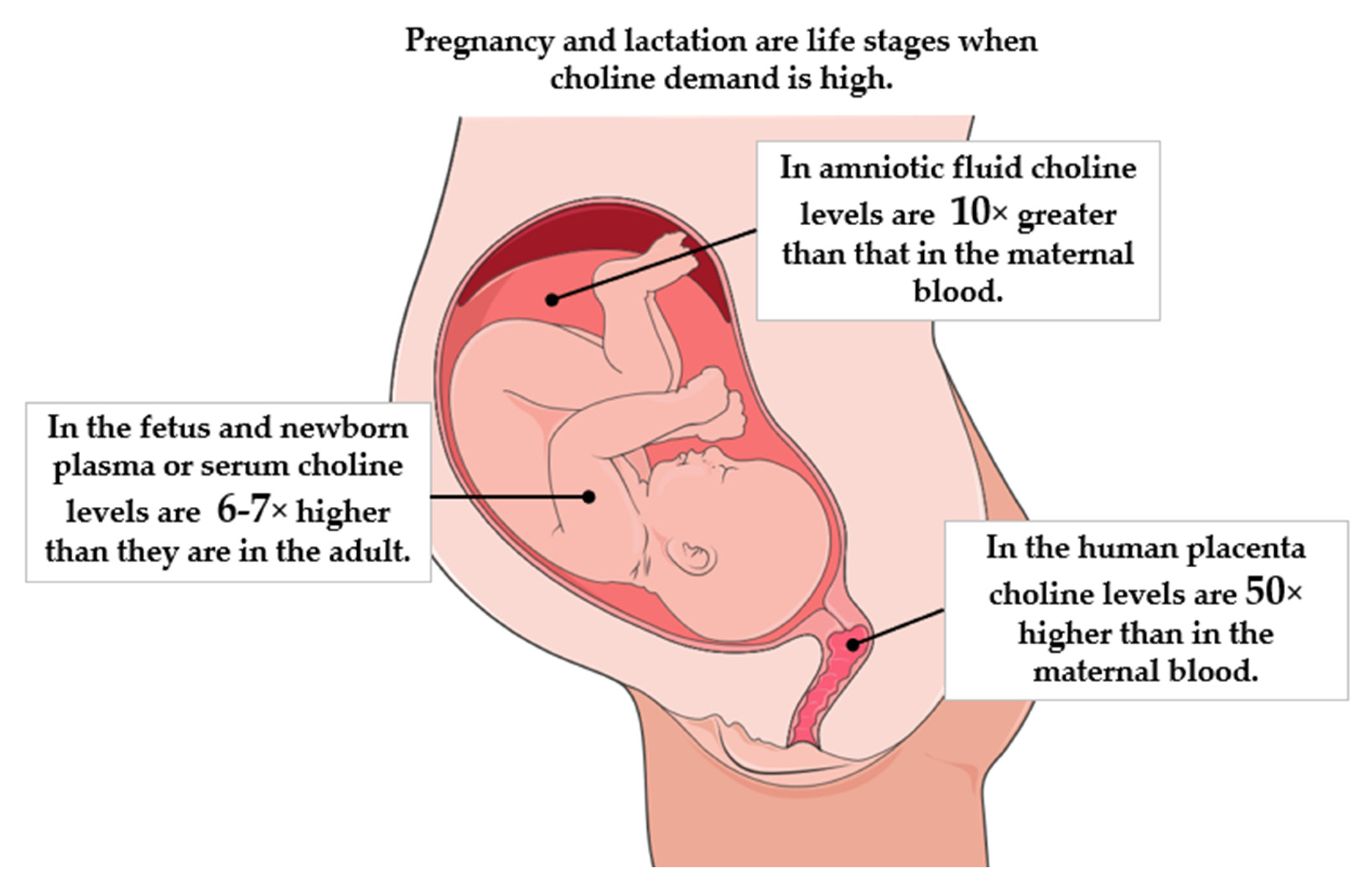
2.3. Maternal Needs
3. Approach
4. Choline: Latest Evidence
5. Choline: Intake Guidelines and Health Claims
6. Choline: Maternal Dietary Intakes
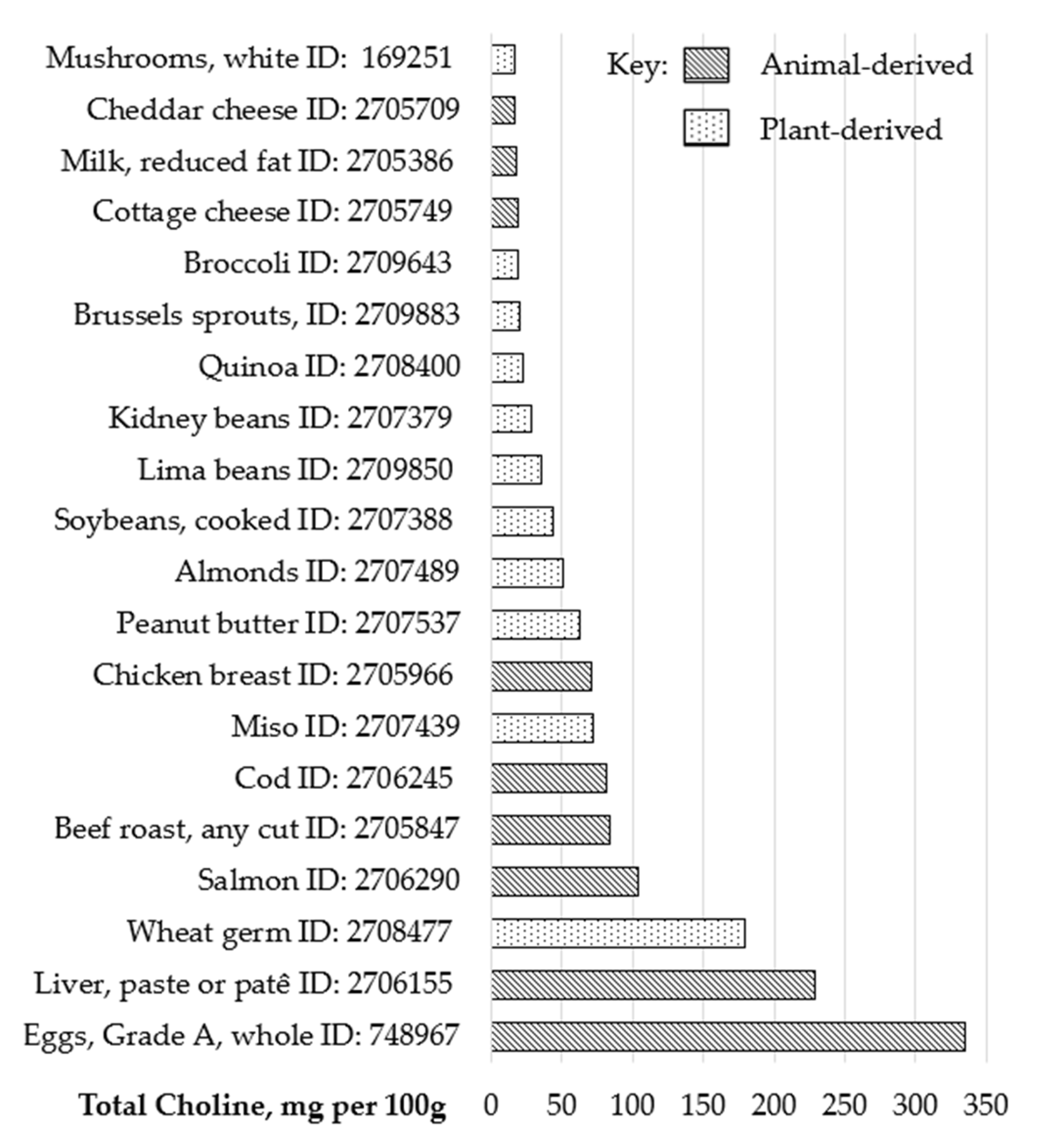
7. Choline: Food and Supplement Sources
8. Choline: Application for Clinical Practice
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| a-GPC | Alpha-glycerophosphocholine |
| ADHD | Attention Deficit Hyperactivity Disorder |
| AI | Adequate Intake |
| APOs | Adverse Pregnancy Outcomes |
| ASC | Autistic Spectrum Condition |
| EFSA | European Food Safety Authority |
| IoM | Institute of Medicine |
| NAFLD | Non-alcoholic Fatty Liver Disease |
| NTDs | Neural Tube Defects |
| NNR | Nordic Nutrition Recommendations |
| OR | Odds Ratio |
| PEMT | Phosphatidylethanolamine N-methyltransferase |
| PtdCho | Phosphatidylcholine |
Appendix A

References
- Marshall, N.E.; Abrams, B.; Barbour, L.A.; Catalano, P.; Christian, P.; Friedman, J.E.; Hay, W.W., Jr.; Hernandez, T.L.; Krebs, N.F.; Oken, E.; et al. The importance of nutrition in pregnancy and lactation: Lifelong consequences. Am. J. Obs. Gynecol. 2022, 226, 607–632. [Google Scholar] [CrossRef] [PubMed]
- Cetin, I.; Devlieger, R.; Isolauri, E.; Obeid, R.; Parisi, F.; Pilz, S.; van Rossem, L.; Maternal Nutrition Delphi Study Group; Steegers-Theunissen, R. International expert consensus on micronutrient supplement use during the early life course. BMC Pregnancy Childbirth 2025, 25, 44. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Albornoz, M.C.; Garcia-Guaqueta, D.P.; Velez-van-Meerbeke, A.; Talero-Gutierrez, C. Maternal Nutrition and Neurodevelopment: A Scoping Review. Nutrients 2021, 13, 3530. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of modern nutrition science-implications for current research, dietary guidelines, and food policy. BMJ 2018, 361, k2392. [Google Scholar] [CrossRef]
- Zeisel, S.H. A brief history of choline. Ann. Nutr. Metab. 2012, 61, 254–258. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; Food and Nutrition Board. Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press: Washington, DC, USA, 1998. [Google Scholar]
- Hollenbeck, C.B. An introduction to the nutrition and metabolism of choline. Cent. Nerv. Syst. Agents Med. Chem. 2012, 12, 100–113. [Google Scholar] [CrossRef]
- Lopez-Sobaler, A.M.; Lorenzo Mora, A.M.; Salas Gonzalez, M.f.; Peral Suarez, A.; Aparicio, A.; Ortega, R.M. Importance of choline in cognitive function. Nutr. Hosp. 2021, 37, 18–23. [Google Scholar] [CrossRef]
- Wallace, T.C.; Blusztajn, J.K.; Caudill, M.A.; Klatt, K.C.; Zeisel, S.H. Choline: The Neurocognitive Essential Nutrient of Interest to Obstetricians and Gynecologists. J. Diet. Suppl. 2020, 17, 733–752. [Google Scholar] [CrossRef]
- Zeisel, S.H. Choline: An important nutrient in brain development, liver function and carcinogenesis. J. Am. Coll. Nutr. 1992, 11, 473–481. [Google Scholar] [CrossRef]
- Obeid, R.; Schon, C.; Derbyshire, E.; Jiang, X.; Mellott, T.J.; Blusztajn, J.K.; Zeisel, S.H. A Narrative Review on Maternal Choline Intake and Liver Function of the Fetus and the Infant; Implications for Research, Policy, and Practice. Nutrients 2024, 16, 260. [Google Scholar] [CrossRef]
- Bernhard, W.; Poets, C.F.; Franz, A.R. Choline and choline-related nutrients in regular and preterm infant growth. Eur. J. Nutr. 2019, 58, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Van Echten-Deckert, G.; Alam, S. Sphingolipid metabolism—An ambiguous regulator of autophagy in the brain. Biol. Chem. 2018, 399, 837–850. [Google Scholar] [CrossRef]
- Goh, Y.Q.; Cheam, G.; Wang, Y. Understanding Choline Bioavailability and Utilization: First Step Toward Personalizing Choline Nutrition. J. Agric. Food Chem. 2021, 69, 10774–10789. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.S.; Shin, Y.J. Role of Choline in Ocular Diseases. Int. J. Mol. Sci. 2021, 22, 4733. [Google Scholar] [CrossRef]
- Derbyshire, E.; Obeid, R. Choline, Neurological Development and Brain Function: A Systematic Review Focusing on the First 1000 Days. Nutrients 2020, 12, 1731. [Google Scholar] [CrossRef]
- Korsmo, H.W.; Jiang, X.; Caudill, M.A. Choline: Exploring the Growing Science on Its Benefits for Moms and Babies. Nutrients 2019, 11, 1823. [Google Scholar] [CrossRef] [PubMed]
- Chen, V.; Schwartz, J.L.; Cho, C.E. Folate and Choline: Does It Take Two to Tango in Early Programming of Disease? Lifestyle Genom. 2023, 16, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Korsmo, H.W.; Edwards, K.; Dave, B.; Jack-Roberts, C.; Yu, H.; Saxena, A.; Salvador, M.; Dembitzer, M.; Phagoora, J.; Jiang, X. Prenatal Choline Supplementation during High-Fat Feeding Improves Long-Term Blood Glucose Control in Male Mouse Offspring. Nutrients 2020, 12, 144. [Google Scholar] [CrossRef]
- Nam, J.; Greenwald, E.; Jack-Roberts, C.; Ajeeb, T.T.; Malysheva, O.V.; Caudill, M.A.; Axen, K.; Saxena, A.; Semernina, E.; Nanobashvili, K.; et al. Choline prevents fetal overgrowth and normalizes placental fatty acid and glucose metabolism in a mouse model of maternal obesity. J. Nutr. Biochem. 2017, 49, 80–88. [Google Scholar] [CrossRef]
- Korsmo, H.W.; Kadam, I.; Reaz, A.; Bretter, R.; Saxena, A.; Johnson, C.H.; Caviglia, J.M.; Jiang, X. Prenatal Choline Supplement in a Maternal Obesity Model Modulates Offspring Hepatic Lipidomes. Nutrients 2023, 15, 965. [Google Scholar] [CrossRef]
- Taesuwan, S.; McDougall, M.Q.; Malysheva, O.V.; Bender, E.; Nevins, J.E.H.; Devapatla, S.; Vidavalur, R.; Caudill, M.A.; Klatt, K.C. Choline metabolome response to prenatal choline supplementation across pregnancy: A randomized controlled trial. FASEB J. 2021, 35, e22063. [Google Scholar] [CrossRef] [PubMed]
- Derbyshire, E. Nutrition in the Childbearing Years; John Wiley & Sons: Oxford, UK, 2011. [Google Scholar]
- Zeisel, S.H. Nutritional importance of choline for brain development. J. Am. Coll. Nutr. 2004, 23, 621S–626S. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Jiang, X.; West, A.A.; Perry, C.A.; Malysheva, O.V.; Brenna, J.T.; Stabler, S.P.; Allen, R.H.; Gregory, J.F., III; Caudill, M.A. Pregnancy alters choline dynamics: Results of a randomized trial using stable isotope methodology in pregnant and nonpregnant women. Am. J. Clin. Nutr. 2013, 98, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S.H. Choline: Critical role during fetal development and dietary requirements in adults. Annu. Rev. Nutr. 2006, 26, 229–250. [Google Scholar] [CrossRef]
- Caudill, M.A. Pre- and postnatal health: Evidence of increased choline needs. J. Am. Diet. Assoc. 2010, 110, 1198–1206. [Google Scholar] [CrossRef]
- Sweiry, J.H.; Page, K.R.; Dacke, C.G.; Abramovich, D.R.; Yudilevich, D.L. Evidence of saturable uptake mechanisms at maternal and fetal sides of the perfused human placenta by rapid paired-tracer dilution: Studies with calcium and choline. J. Dev. Physiol. 1986, 8, 435–445. [Google Scholar]
- Van der Aa, E.M.; Wouterse, A.C.; Peereboom-Stegeman, J.H.; Russel, F.G. Uptake of choline into syncytial microvillus membrane vesicles of human term placenta. Biochem. Pharmacol. 1994, 47, 453–456. [Google Scholar] [CrossRef]
- Ozarda Ilcol, Y.; Uncu, G.; Ulus, I.H. Free and phospholipid-bound choline concentrations in serum during pregnancy, after delivery and in newborns. Arch. Physiol. Biochem. 2002, 110, 393–399. [Google Scholar] [CrossRef]
- Zeisel, S.H.; Wurtman, R.J. Developmental changes in rat blood choline concentration. Biochem. J. 1981, 198, 565–570. [Google Scholar] [CrossRef]
- Holmes, H.C.; Snodgrass, G.J.; Iles, R.A. Changes in the choline content of human breast milk in the first 3 weeks after birth. Eur. J. Pediatr. 2000, 159, 198–204. [Google Scholar] [CrossRef]
- EFSA. Dietary Reference Values for choline EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2016, 14, 4484. [Google Scholar]
- Freedman, R.; Hunter, S.K.; Law, A.J.; Clark, A.M.; Roberts, A.; Hoffman, M.C. Choline, folic acid, Vitamin D, and fetal brain development in the psychosis spectrum. Schizophr. Res. 2022, 247, 16–25. [Google Scholar] [CrossRef]
- Nguyen, H.T.; Oktayani, P.P.I.; Lee, S.D.; Huang, L.C. Choline in pregnant women: A systematic review and meta-analysis. Nutr. Rev. 2025, 83, e273–e289. [Google Scholar] [CrossRef]
- Obeid, R.; Derbyshire, E.; Schon, C. Association between Maternal Choline, Fetal Brain Development, and Child Neurocognition: Systematic Review and Meta-Analysis of Human Studies. Adv. Nutr. 2022, 13, 2445–2457. [Google Scholar] [CrossRef]
- Gould, J.F.; Hines, S.; Best, K.P.; Grzeskowiak, L.E.; Jansen, O.; Green, T.J. Choline During Pregnancy and Child Neurodevelopment: A Systematic Review of Randomized Controlled Trials and Observational Studies. Nutrients 2025, 17, 886. [Google Scholar] [CrossRef]
- Akison, L.K.; Kuo, J.; Reid, N.; Boyd, R.N.; Moritz, K.M. Effect of Choline Supplementation on Neurological, Cognitive, and Behavioral Outcomes in Offspring Arising from Alcohol Exposure During Development: A Quantitative Systematic Review of Clinical and Preclinical Studies. Alcohol. Clin. Exp. Res. 2018, 42, 1591–1611. [Google Scholar] [CrossRef] [PubMed]
- Leermakers, E.T.; Moreira, E.M.; Kiefte-de Jong, J.C.; Darweesh, S.K.; Visser, T.; Voortman, T.; Bautista, P.K.; Chowdhury, R.; Gorman, D.; Bramer, W.M.; et al. Effects of choline on health across the life course: A systematic review. Nutr. Rev. 2015, 73, 500–522. [Google Scholar] [CrossRef] [PubMed]
- Lavery, A.M.; Brender, J.D.; Zhao, H.; Sweeney, A.; Felkner, M.; Suarez, L.; Canfield, M.A. Dietary intake of choline and neural tube defects in Mexican Americans. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 463–471. [Google Scholar] [CrossRef]
- Shaw, G.M.; Carmichael, S.L.; Yang, W.; Selvin, S.; Schaffer, D.M. Periconceptional dietary intake of choline and betaine and neural tube defects in offspring. Am. J. Epidemiol. 2004, 160, 102–109. [Google Scholar] [CrossRef]
- Carmichael, S.L.; Yang, W.; Shaw, G.M. Periconceptional nutrient intakes and risks of neural tube defects in California. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 670–678. [Google Scholar] [CrossRef]
- Petersen, J.M.; Parker, S.E.; Crider, K.S.; Tinker, S.C.; Mitchell, A.A.; Werler, M.M. One-Carbon Cofactor Intake and Risk of Neural Tube Defects Among Women Who Meet Folic Acid Recommendations: A Multicenter Case-Control Study. Am. J. Epidemiol. 2019, 188, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Shaw, G.M.; Finnell, R.H.; Blom, H.J.; Carmichael, S.L.; Vollset, S.E.; Yang, W.; Ueland, P.M. Choline and risk of neural tube defects in a folate-fortified population. Epidemiology 2009, 20, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Azzaroli, F.; Mazzella, G.; Marchesini, G.; Brodosi, L.; Petroni, M.L. Fatty liver in pregnancy: A narrative review of two distinct conditions. Expert. Rev. Gastroenterol. Hepatol. 2020, 14, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Hagstrom, H.; Simon, T.G.; Roelstraete, B.; Stephansson, O.; Soderling, J.; Ludvigsson, J.F. Maternal obesity increases the risk and severity of NAFLD in offspring. J. Hepatol. 2021, 75, 1042–1048. [Google Scholar] [CrossRef]
- Caudill, M.; Obeid, R.; Derbyshire, E.; Bernhard, W.; Lapid, K.; Walker, S.; Zeisel, S. Building better babies: Should choline supplementation be recommended for pregnant and lactating mothers? Literature overview and expert panel consensus. Eur. Gynecol. Obstet. 2020, 2, 149–161. [Google Scholar]
- Wallace, T.C.; Blusztajn, J.K.; Caudill, M.A.; Klatt, K.C.; Natker, E.; Zeisel, S.H.; Zelman, K.M. Choline: The Underconsumed and Underappreciated Essential Nutrient. Nutr. Today 2018, 53, 240–253. [Google Scholar] [CrossRef]
- Glade, M.J.; Crook, M.A. Choline deficiency: Is it being recognized? Nutrition 2022, 94, 111509. [Google Scholar] [CrossRef]
- Government of Canada. Dietary Reference Intake Tables: Reference Values for Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. 2025. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/healthy-eating/dietary-reference-intakes/tables/reference-values-vitamins.html#tbl3 (accessed on 21 March 2025).
- Ministry of Health. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes. Available online: https://www.nhmrc.gov.au/sites/default/files/images/nutrient-refererence-dietary-intakes.pdf (accessed on 21 March 2025).
- US Department of Agriculture; US Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025; US Government Publishing Office: Washington, DC, USA, 2021.
- US Food and Drug Administration. Food Labeling: Revision of the Nutrition and Supplement Facts Labels; Docket No. FDA–2012–N–1210; Office of Food Labeling, US Food and Drug Administration: Silver Spring, MD, USA, 2018.
- Hanson, M.A.; Bardsley, A.; De-Regil, L.M.; Moore, S.E.; Oken, E.; Poston, L.; Ma, R.C.; McAuliffe, F.M.; Maleta, K.; Purandare, C.N.; et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition: “Think Nutrition First”. Int. J. Gynaecol. Obs. 2015, 131, 213–253. [Google Scholar] [CrossRef]
- O’Connor, D.L.; Blake, J.; Bell, R.; Bowen, A.; Callum, J.; Fenton, S.; Gray-Donald, K.; Rossiter, M.; Adamo, K.; Brett, K.; et al. Canadian consensus on female nutrition: Adolescence, reproduction, menopause, and beyond. J. Obstet. Gynaecol. Can. 2016, 38, 508–554.e18. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Clinical Practice Guidelines: Pregnancy Care 2019. Australian Government Department of Health. Available online: https://www.health.gov.au/ (accessed on 20 April 2025).
- Schwarzenberg, S.J.; Georgieff, M.K.; Committee On, N. Advocacy for Improving Nutrition in the First 1000 Days to Support Childhood Development and Adult Health. Pediatrics 2018, 141, e20173716. [Google Scholar] [CrossRef]
- American Medical Association. AMA Backs Global Health Experts in Calling Infertility a Disease. 2017. Available online: https://www.ama-assn.org/delivering-care/public-health/ama-backs-global-health-experts-calling-infertility-disease (accessed on 25 February 2025).
- Nordic Co-Operation. Notdic Nutrition Recommendations 2023. Integrating Environmental Aspects. Available online: https://www.norden.org/en/publication/nordic-nutrition-recommendations-2023 (accessed on 20 April 2025).
- European Commission. EU Register of Health Claims. Available online: https://food.ec.europa.eu/food-safety/labelling-and-nutrition/nutrition-and-health-claims/eu-register-health-claims_en (accessed on 25 February 2025).
- EFSA. Choline and contribution to normal liver function of the foetus and exclusively breastfed infants: Evaluation of a health claim pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA J. 2023, 21, 8115. [Google Scholar]
- Derbyshire, E.; Obeid, R.; Schon, C. Habitual Choline Intakes across the Childbearing Years: A Review. Nutrients 2021, 13, 4390. [Google Scholar] [CrossRef] [PubMed]
- Zuk, E.; Nikrandt, G.; Chmurzynska, A. Dietary choline intake in European and non-european populations: Current status and future trends-a narrative review. Nutr. J. 2024, 23, 68. [Google Scholar] [CrossRef]
- Redruello-Requejo, M.; Carretero-Krug, A.; Rodriguez-Alonso, P.; Samaniego-Vaesken, M.L.; Partearroyo, T.; Varela-Moreiras, G. Dietary Intake Adequacy and Food Sources of Nutrients Involved in the Methionine-Methylation Cycle in Women of Childbearing Age from the ANIBES Spanish Population. Nutrients 2021, 13, 2958. [Google Scholar] [CrossRef] [PubMed]
- Roeren, M.; Kordowski, A.; Sina, C.; Smollich, M. Inadequate Choline Intake in Pregnant Women in Germany. Nutrients 2022, 14, 4862. [Google Scholar] [CrossRef]
- Gao, X.; Wang, Y.; Randell, E.; Pedram, P.; Yi, Y.; Gulliver, W.; Sun, G. Higher Dietary Choline and Betaine Intakes Are Associated with Better Body Composition in the Adult Population of Newfoundland, Canada. PLoS ONE 2016, 11, e0155403. [Google Scholar] [CrossRef]
- Derbyshire, E. Could we be overlooking a potential choline crisis in the United Kingdom? BMJ Nutr. Prev. Health 2019, 2, 86–89. [Google Scholar] [CrossRef]
- USDA. US Department of Agriculture Database. FoodData Central. 2024. Available online: https://fdc.nal.usda.gov/ (accessed on 28 February 2025).
- Patterson, K.; Bhagwat, S.; Williams, J.; Howe, J.; Holden, J. USDA Database for the Choline Content of Common Foods Release Two. 2008. Available online: https://www.ars.usda.gov/ARSUserFiles/80400525/Data/Choline/Choln02.pdf (accessed on 28 February 2025).
- Jaiswal, A.; Dewani, D.; Reddy, L.S.; Patel, A. Choline Supplementation in Pregnancy: Current Evidence and Implications. Cureus 2023, 15, e48538. [Google Scholar] [CrossRef]
- Hess, J.M.; Comeau, M.E.; Casperson, S.; Slavin, J.L.; Johnson, G.H.; Messina, M.; Raatz, S.; Scheett, A.J.; Bodensteiner, A.; Palmer, D.G. Dietary Guidelines Meet NOVA: Developing a Menu for A Healthy Dietary Pattern Using Ultra-Processed Foods. J. Nutr. 2023, 153, 2472–2481. [Google Scholar] [CrossRef]
- Kansakar, U.; Trimarco, V.; Mone, P.; Varzideh, F.; Lombardi, A.; Santulli, G. Choline supplements: An update. Front. Endocrinol. 2023, 14, 1148166. [Google Scholar] [CrossRef]
- Heras-Sola, J.; Gallo-Vallejo, J.L. Importance of choline during pregnancy and lactation: A systematic review. Semergen 2024, 50, 102089. [Google Scholar] [CrossRef]
- Spoelstra, S.K.; Eijsink, J.J.H.; Hoenders, H.J.R.; Knegtering, H. Maternal choline supplementation during pregnancy to promote mental health in offspring. Early Interv. Psychiatry 2023, 17, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Kirby, J.K.; Sorensen, J.C.; Pollard, E.L.; Audhya, T. Evidence based recommendations for an optimal prenatal supplement for women in the US: Vitamins and related nutrients. Matern. Health Neonatol. Perinatol. 2022, 8, 4. [Google Scholar] [CrossRef]
- Bragg, M.G.; Prado, E.L.; Stewart, C.P. Choline and docosahexaenoic acid during the first 1000 days and children’s health and development in low- and middle-income countries. Nutr. Rev. 2022, 80, 656–676. [Google Scholar] [CrossRef] [PubMed]
- Dymek, A.; Oleksy, L.; Stolarczyk, A.; Bartosiewicz, A. Choline-An Underappreciated Component of a Mother-to-Be’s Diet. Nutrients 2024, 16, 1767. [Google Scholar] [CrossRef] [PubMed]
- Drews, K. Folate metabolism--epigenetic role of choline and vitamin B12 during pregnancy. Ginekol. Pol. 2015, 86, 940–946. [Google Scholar] [CrossRef]
- Zeisel, S.H. Gene response elements, genetic polymorphisms and epigenetics influence the human dietary requirement for choline. IUBMB Life 2007, 59, 380–387. [Google Scholar] [CrossRef]
- Yki-Jarvinen, H.; Luukkonen, P.K.; Hodson, L.; Moore, J.B. Dietary carbohydrates and fats in nonalcoholic fatty liver disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 770–786. [Google Scholar] [CrossRef]
- Derbyshire, E.; Maes, M. The Role of Choline in Neurodevelopmental Disorders-A Narrative Review Focusing on ASC, ADHD and Dyslexia. Nutrients 2023, 15, 2876. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| US IOM (1998) [6] AI (mg/d) | Canada (2023) [50] AI (mg/d) | Australia (2006) [51] AI (mg/d) | EFSA (2016) [33] AI (mg/d) | NNR (2023) [59] AI (mg/d) | |
|---|---|---|---|---|---|
| Life Stage | Females ≥19 yrs | Females ≥19 yrs | Females ≥19 yrs | Females ≥18 yrs | Females ≥18 yrs |
| Adult | 425 | 425 | 425 | 400 | 400 |
| Pregnancy | 450 | 450 | 440 | 480 | - |
| Lactation | 500 | 550 | 550 | 520 | - |
| Evidence-Based Guidance Points | |
|---|---|
| Importance of choline for pregnancy and lactation |
|
| Choline food sources |
|
| Choline requirements | |
| Factors contributing to higher choline requirements |
These factors increase susceptibility to insufficient choline status |
| Choline dietary intakes |
|
| Consequences of inadequate choline intakes during pregnancy and lactation | |
| Supplementation guidance |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derbyshire, E.J. Choline in Pregnancy and Lactation: Essential Knowledge for Clinical Practice. Nutrients 2025, 17, 1558. https://doi.org/10.3390/nu17091558
Derbyshire EJ. Choline in Pregnancy and Lactation: Essential Knowledge for Clinical Practice. Nutrients. 2025; 17(9):1558. https://doi.org/10.3390/nu17091558
Chicago/Turabian StyleDerbyshire, E. J. 2025. "Choline in Pregnancy and Lactation: Essential Knowledge for Clinical Practice" Nutrients 17, no. 9: 1558. https://doi.org/10.3390/nu17091558
APA StyleDerbyshire, E. J. (2025). Choline in Pregnancy and Lactation: Essential Knowledge for Clinical Practice. Nutrients, 17(9), 1558. https://doi.org/10.3390/nu17091558