
The Influences of Oral Probiotics on the Immunometabolic Response During Pregnancy and Lactation: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
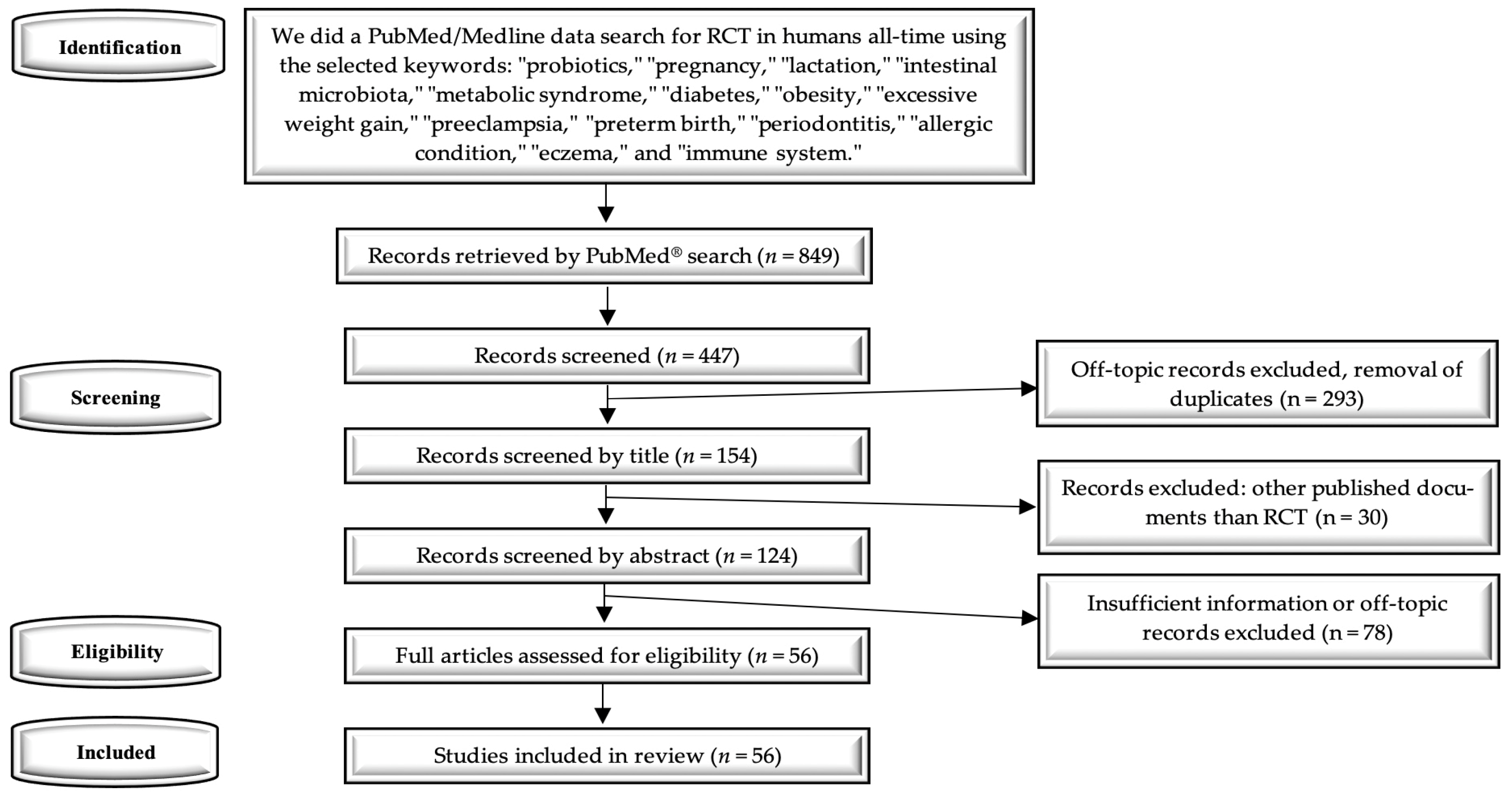
2.2. Database Sources and Electronic Search Strategy
2.3. Study Design
2.4. Data Extraction, Analysis, and Assessment of Quality and Risk of Bias
3. Results
3.1. Search Results
3.2. Main Characteristics of the Selected Studies
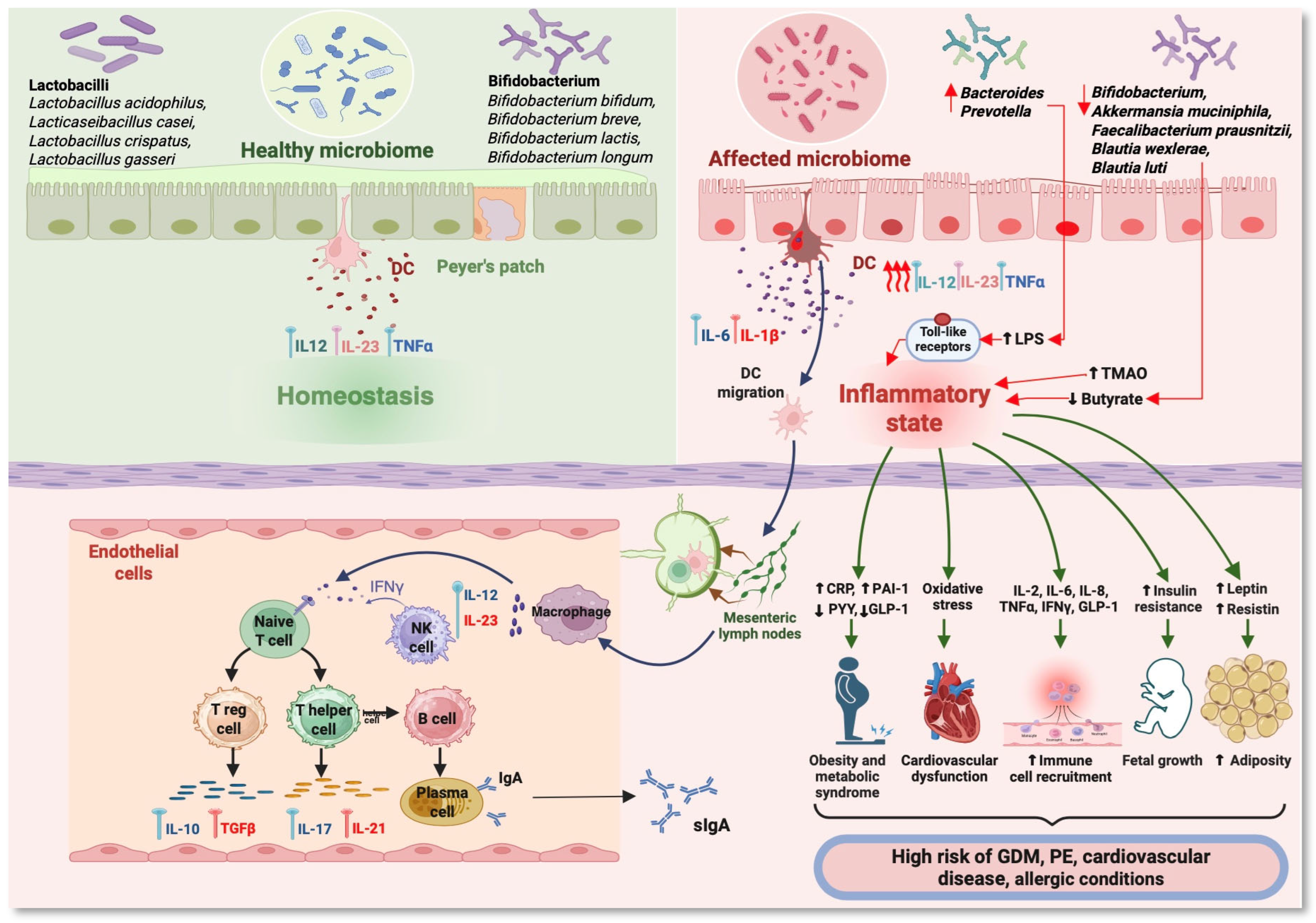
4. The Maternal Microbiome—The Key to Immunometabolic Responses and Influence on Infant Microbiota
5. The Changes of the Probiotic Intervention on the Immune Response During Pregnancy and Lactation
6. The Influence of Probiotic Intervention on Allergic Conditions
7. Probiotics Intervention Improves Glucose and Lipid Metabolism in Pregnant Women
8. The Effects of Probiotics on Obesity and Excessive Gestational Weight Gain
9. The Action of Probiotics Regarding the Prevention and Evolution of GDM
10. The Roles of Probiotics in the Prevention of Preeclampsia
11. Other Possible Actions of Probiotics to Improve the Perinatal Outcomes
12. Discussions
13. Conclusions
14. Take Home Messages
- Probiotic intervention during pregnancy and lactation may help reduce the risks of allergic diseases, preeclampsia, obesity, overweight, and GDM. However, study outcomes vary due to differences in methodologies, probiotic types, intervention timing, and risk identification.
- Infant immune system development. Transitioning from a sterile fetal gut to one colonized by environmental microorganisms is essential for strengthening the infant’s immune system, influencing long-term health.
- Immune system modulation. Probiotics can modulate the gut microbiota, affecting cytokine production and immune responses. The specific effects depend on the bacterial strains, enhancing infection resistance and reducing pro-inflammatory cytokine production.
- Probiotics and gut health. Appropriate probiotic use supports a balanced gut microbiota, reducing the impact of certain diseases. Studies indicate that probiotics, particularly Bifidobacterium, may exert anti-inflammatory effects and improve the IL-10/IL-12 ratio.
- Immunomodulatory roles. Various strains of Lactobacilli and Bifidobacterium have immunomodulatory effects, enhancing both innate and adaptive immunity, alleviating lactose intolerance, and increasing nutrient bioavailability.
- Mixed evidence on allergic disease reduction. Evidence regarding probiotics’ effect on reducing eczema and atopic dermatitis is mixed, though prenatal use may lower allergy rates in high-risk infants.
- Conflicting results on metabolic health. Studies show varying results on probiotics’ impact on obesity, FPG, excessive weight gain, and metabolic health in pregnant women. The probiotic strain, intervention duration, and other factors influence these outcomes.
- Limited effects on gestational diabetes. The benefit of probiotic use in reducing GDM remains unclear. Some studies show minor improvements in insulin sensitivity, while others report no effect.
- No standard probiotic recommendations. Due to the variability in study findings, there are no standardized recommendations for probiotic supplementation during pregnancy. However, probiotics appear safe for use in pregnant women and infants.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martín-Peláez, S.; Cano-Ibáñez, N.; Pinto-Gallardo, M.; Amezcua-Prieto, C. The Impact of Probiotics, Prebiotics, and Synbiotics During Pregnancy or Lactation on the Intestinal Microbiota of Children Born by Cesarean Section: A Systematic Review. Nutrients 2022, 14, 341. [Google Scholar] [CrossRef] [PubMed]
- Stinson, L.F.; Boyce, M.C.; Payne, M.S.; Keelan, J.A. The Not-so-Sterile Womb: Evidence That the Human Fetus Is Exposed to Bacteria Prior to Birth. Front. Microbiol. 2019, 10, 1124. [Google Scholar] [CrossRef]
- Lu, X.; Shi, Z.; Jiang, L.; Zhang, S. Maternal Gut Microbiota in the Health of Mothers and Offspring: From the Perspective of Immunology. Front. Immunol. 2024, 15, 1362784. [Google Scholar] [CrossRef] [PubMed]
- Kartjito, M.S.; Yosia, M.; Wasito, E.; Soloan, G.; Agussalim, A.F.; Basrowi, R.W. Defining the Relationship of Gut Microbiota, Immunity, and Cognition in Early Life—A Narrative Review. Nutrients 2023, 15, 2642. [Google Scholar] [CrossRef]
- Mor, G.; Aldo, P.; Alvero, A.B. The Unique Immunological and Microbial Aspects of Pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raya, B.; Michalski, C.; Sadarangani, M.; Lavoie, P.M. Maternal Immunological Adaptation During Normal Pregnancy. Front. Immunol. 2020, 11, 575197. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Rinne, M.; Kalliomaki, M.; Arvilommi, H.; Salminen, S.; Isolauri, E. Effect of Probiotics and Breastfeeding on the Bifidobacterium and Lactobacillus/Enterococcus Microbiota and Humoral Immune Responses. J. Pediatr. 2005, 147, 186–191. [Google Scholar] [CrossRef]
- Marschan, E.; Kuitunen, M.; Kukkonen, K.; Poussa, T.; Sarnesto, A.; Haahtela, T.; Korpela, R.; Savilahti, E.; Vaarala, O. Probiotics in Infancy Induce Protective Immune Profiles That Are Characteristic for Chronic Low-Grade Inflammation. Clin. Exp. Allergy 2008, 38, 611–618. [Google Scholar] [CrossRef]
- Kopp, M.V.; Goldstein, M.; Dietschek, A.; Sofke, J.; Heinzmann, A.; Urbanek, R. Lactobacillus GG Has in Vitro Effects on Enhanced Interleukin-10 and Interferon-Gamma Release of Mononuclear Cells but No in Vivo Effects in Supplemented Mothers and Their Neonates. Clin. Exp. Allergy 2008, 38, 602–610. [Google Scholar] [CrossRef]
- Rautava, S.; Collado, M.C.; Salminen, S.; Isolauri, E. Probiotics Modulate Host-Microbe Interaction in the Placenta and Fetal Gut: A Randomized, Double-Blind, Placebo-Controlled Trial. Neonatology 2012, 102, 178–184. [Google Scholar] [CrossRef]
- Rø, A.D.B.; Simpson, M.R.; Rø, T.B.; Storrø, O.; Johnsen, R.; Videm, V.; Øien, T. Reduced Th22 Cell Proportion and Prevention of Atopic Dermatitis in Infants Following Maternal Probiotic Supplementation. Clin. Exp. Allergy 2017, 47, 1014–1021. [Google Scholar] [CrossRef]
- Forsberg, A.; Abrahamsson, T.R.; Nilsson, L.; Ernerudh, J.; Duchén, K.; Jenmalm, M.C. Changes in Peripheral Immune Populations During Pregnancy and Modulation by Probiotics and ω-3 Fatty Acids. Sci. Rep. 2020, 10, 18723. [Google Scholar] [CrossRef] [PubMed]
- Soukka, J.; Polari, L.; Kalliomäki, M.; Saros, L.; Laajala, T.D.; Vahlberg, T.; Toivola, D.M.; Laitinen, K. The Effect of a Fish Oil and/or Probiotic Intervention from Early Pregnancy Onwards on Colostrum Immune Mediators: A Randomized, Placebo-Controlled, Double-Blinded Clinical Trial in Overweight/Obese Mothers. Mol. Nutr. Food Res. 2023, 67, e2200446. [Google Scholar] [CrossRef]
- Killeen, S.L.; Mealy, G.; Brennan, K.; Cotter, P.D.; Yelverton, C.; Saldova, R.; Groeger, D.; VanSinderen, D.; Doyle, S.; McAuliffe, F.M. Impact of Bifidobacterium Longum1714® on Maternal Cytokine Response in Peripheral Blood Mononuclear Cells. Cytokine 2024, 174, 156458. [Google Scholar] [CrossRef] [PubMed]
- Kalliomäki, M.; Salminen, S.; Arvilommi, H.; Kero, P.; Koskinen, P.; Isolauri, E. Probiotics in Primary Prevention of Atopic Disease: A Randomised Placebo-Controlled Trial. Lancet 2001, 357, 1076–1079. [Google Scholar] [CrossRef]
- Kukkonen, K.; Savilahti, E.; Haahtela, T.; Juntunen-Backman, K.; Korpela, R.; Poussa, T.; Tuure, T.; Kuitunen, M. Probiotics and Prebiotic Galacto-Oligosaccharides in the Prevention of Allergic Diseases: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Allergy Clin. Immunol. 2007, 119, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, T.R.; Jakobsson, T.; Böttcher, M.F.; Fredrikson, M.; Jenmalm, M.C.; Björkstén, B.; Oldaeus, G. Probiotics in Prevention of IgE-Associated Eczema: A Double-Blind, Randomized, Placebo-Controlled Trial. J. Allergy Clin. Immunol. 2007, 119, 1174–1180. [Google Scholar] [CrossRef]
- Huurre, A.; Laitinen, K.; Rautava, S.; Korkeamäki, M.; Isolauri, E. Impact of Maternal Atopy and Probiotic Supplementation During Pregnancy on Infant Sensitization: A Double-Blind Placebo-Controlled Study. Clin. Exp. Allergy 2008, 38, 1342–1348. [Google Scholar] [CrossRef]
- Niers, L.; Martín, R.; Rijkers, G.; Sengers, F.; Timmerman, H.; van Uden, N.; Smidt, H.; Kimpen, J.; Hoekstra, M. The Effects of Selected Probiotic Strains on the Development of Eczema (the PandA Study). Allergy 2009, 64, 1349–1358. [Google Scholar] [CrossRef]
- Kuitunen, M.; Kukkonen, K.; Juntunen-Backman, K.; Korpela, R.; Poussa, T.; Tuure, T.; Haahtela, T.; Savilahti, E. Probiotics Prevent IgE-Associated Allergy until Age 5 Years in Cesarean-Delivered Children but Not in the Total Cohort. J. Allergy Clin. Immunol. 2009, 123, 335–341. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kwon, J.H.; Ahn, S.H.; Lee, S.I.; Han, Y.S.; Choi, Y.O.; Lee, S.Y.; Ahn, K.M.; Ji, G.E. Effect of Probiotic Mix (Bifidobacterium Bifidum, Bifidobacterium Lactis, Lactobacillus Acidophilus) in the Primary Prevention of Eczema: A Double-Blind, Randomized, Placebo-Controlled Trial. Pediatr. Allergy Immunol. 2010, 21, e386–e393. [Google Scholar] [CrossRef]
- Dotterud, C.K.; Storrø, O.; Johnsen, R.; Oien, T. Probiotics in Pregnant Women to Prevent Allergic Disease: A Randomized, Double-Blind Trial. Br. J. Dermatol. 2010, 163, 616–623. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ismail, I.H.; Kivivuori, S.; Licciardi, P.V.; Robins-Browne, R.M.; Mah, L.-J.; Axelrad, C.; Moore, S.; Donath, S.; Carlin, J.B.; et al. Lactobacillus GG Treatment During Pregnancy for the Prevention of Eczema: A Randomized Controlled Trial. Allergy 2011, 66, 509–516. [Google Scholar] [CrossRef]
- Wickens, K.; Black, P.; Stanley, T.V.; Mitchell, E.; Barthow, C.; Fitzharris, P.; Purdie, G.; Crane, J. A Protective Effect of Lactobacillus Rhamnosus HN001 Against Eczema in the First 2 Years of Life Persists to Age 4 Years. Clin. Exp. Allergy 2012, 42, 1071–1079. [Google Scholar] [CrossRef]
- Ismail, I.H.; Oppedisano, F.; Joseph, S.J.; Boyle, R.J.; Robins-Browne, R.M.; Tang, M.L.K. Prenatal Administration of Lactobacillus Rhamnosus Has No Effect on the Diversity of the Early Infant Gut Microbiota. Pediatr. Allergy Immunol. 2012, 23, 255–258. [Google Scholar] [CrossRef]
- Kuitunen, M.; Kukkonen, A.K.; Savilahti, E. Impact of Maternal Allergy and Use of Probiotics During Pregnancy on Breast Milk Cytokines and Food Antibodies and Development of Allergy in Children until 5 Years. Int. Arch. Allergy Immunol. 2012, 159, 162–170. [Google Scholar] [CrossRef]
- Rautava, S.; Kainonen, E.; Salminen, S.; Isolauri, E. Maternal Probiotic Supplementation During Pregnancy and Breast-Feeding Reduces the Risk of Eczema in the Infant. J. Allergy Clin. Immunol. 2012, 130, 1355–1360. [Google Scholar] [CrossRef]
- Allen, S.J.; Jordan, S.; Storey, M.; Thornton, C.A.; Gravenor, M.B.; Garaiova, I.; Plummer, S.F.; Wang, D.; Morgan, G. Probiotics in the Prevention of Eczema: A Randomised Controlled Trial. Arch. Dis. Child. 2014, 99, 1014–1019. [Google Scholar] [CrossRef]
- Kim, H.K.; Rutten, N.B.M.M.; Besseling-van der Vaart, I.; Niers, L.E.M.; Choi, Y.H.; Rijkers, G.T.; van Hemert, S. Probiotic Supplementation Influences Faecal Short Chain Fatty Acids in Infants at High Risk for Eczema. Benef. Microbes 2015, 6, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.R.; Dotterud, C.K.; Storrø, O.; Johnsen, R.; Øien, T. Perinatal Probiotic Supplementation in the Prevention of Allergy Related Disease: 6 Year Follow up of a Randomised Controlled Trial. BMC Dermatol. 2015, 15, 13. [Google Scholar] [CrossRef]
- Barthow, C.; Wickens, K.; Stanley, T.; Mitchell, E.A.; Maude, R.; Abels, P.; Purdie, G.; Murphy, R.; Stone, P.; Kang, J.; et al. The Probiotics in Pregnancy Study (PiP Study): Rationale and Design of a Double-Blind Randomised Controlled Trial to Improve Maternal Health During Pregnancy and Prevent Infant Eczema and Allergy. BMC Pregnancy Childbirth 2016, 16, 133. [Google Scholar] [CrossRef]
- Wickens, K.; Barthow, C.; Mitchell, E.A.; Stanley, T.V.; Purdie, G.; Rowden, J.; Kang, J.; Hood, F.; van den Elsen, L.; Forbes-Blom, E.; et al. Maternal Supplementation Alone with Lactobacillus Rhamnosus HN001 During Pregnancy and Breastfeeding Does Not Reduce Infant Eczema. Pediatr. Allergy Immunol. 2018, 29, 296–302. [Google Scholar] [CrossRef]
- Davies, G.; Jordan, S.; Brooks, C.J.; Thayer, D.; Storey, M.; Morgan, G.; Allen, S.; Garaiova, I.; Plummer, S.; Gravenor, M. Long Term Extension of a Randomised Controlled Trial of Probiotics Using Electronic Health Records. Sci. Rep. 2018, 8, 7668. [Google Scholar] [CrossRef]
- Shipton, E.V.; Foxcroft, K.; Dekker Nitert, M.; McIntyre, H.D.; Barrett, H.; Tang, M.; Callaway, L. OFFSPRING: A SPRING Follow-Up Study Assessing the Efficacy of Maternal Probiotics and Allergic Disease in the Child. Int. Arch. Allergy Immunol. 2024, 185, 212–217. [Google Scholar] [CrossRef]
- Vähämiko, S.; Laiho, A.; Lund, R.; Isolauri, E.; Salminen, S.; Laitinen, K. The Impact of Probiotic Supplementation During Pregnancy on DNA Methylation of Obesity-Related Genes in Mothers and Their Children. Eur. J. Nutr. 2019, 58, 367–377. [Google Scholar] [CrossRef]
- Houttu, N.; Mokkala, K.; Koivuniemi, E.; Pellonperä, O.; Juhila, J.; Sorsa, T.; Laitinen, K. The Impacts of Fish Oil and/or Probiotic Intervention on Low-Grade Inflammation, IGFBP-1 and MMP-8 in Pregnancy: A Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Biomolecules 2020, 11, 5. [Google Scholar] [CrossRef]
- Mokkala, K.; Paulin, N.; Houttu, N.; Koivuniemi, E.; Pellonperä, O.; Khan, S.; Pietilä, S.; Tertti, K.; Elo, L.L.; Laitinen, K. Metagenomics Analysis of Gut Microbiota in Response to Diet Intervention and Gestational Diabetes in Overweight and Obese Women: A Randomised, Double-Blind, Placebo-Controlled Clinical Trial. Gut 2021, 70, 309–318. [Google Scholar] [CrossRef]
- Pellonperä, O.; Vahlberg, T.; Mokkala, K.; Houttu, N.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Weight Gain and Body Composition During Pregnancy: A Randomised Pilot Trial with Probiotics and/or Fish Oil. Br. J. Nutr. 2021, 126, 541–551. [Google Scholar] [CrossRef]
- Hasain, Z.; Raja Ali, R.A.; Ahmad, H.F.; Abdul Rauf, U.F.; Oon, S.F.; Mokhtar, N.M. The Roles of Probiotics in the Gut Microbiota Composition and Metabolic Outcomes in Asymptomatic Post-Gestational Diabetes Women: A Randomized Controlled Trial. Nutrients 2022, 14, 3878. [Google Scholar] [CrossRef] [PubMed]
- Saros, L.; Vahlberg, T.; Koivuniemi, E.; Houttu, N.; Niinikoski, H.; Tertti, K.; Laitinen, K. Fish Oil And/Or Probiotics Intervention in Overweight/Obese Pregnant Women and Overweight Risk in 24-Month-Old Children. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 218–226. [Google Scholar] [CrossRef]
- Halkjær, S.I.; de Knegt, V.E.; Kallemose, T.; Jensen, J.-E.B.; Cortes, D.; Gluud, L.L.; Wewer Albrechtsen, N.J.; Petersen, A.M. No Effect of Multi-Strain Probiotic Supplementation on Metabolic and Inflammatory Markers and Newborn Body Composition in Pregnant Women with Obesity: Results from a Randomized, Double-Blind Placebo-Controlled Study. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 2444–2454. [Google Scholar] [CrossRef] [PubMed]
- Luoto, R.; Kalliomäki, M.; Laitinen, K.; Isolauri, E. The Impact of Perinatal Probiotic Intervention on the Development of Overweight and Obesity: Follow-up Study from Birth to 10 Years. Int. J. Obes. 2010, 34, 1531–1537. [Google Scholar] [CrossRef]
- Nitert, M.D.; Barrett, H.L.; Foxcroft, K.; Tremellen, A.; Wilkinson, S.; Lingwood, B.; Tobin, J.M.; McSweeney, C.; O’Rourke, P.; McIntyre, H.D.; et al. SPRING: An RCT Study of Probiotics in the Prevention of Gestational Diabetes Mellitus in Overweight and Obese Women. BMC Pregnancy Childbirth 2013, 13, 50. [Google Scholar] [CrossRef]
- Lindsay, K.L.; Kennelly, M.; Culliton, M.; Smith, T.; Maguire, O.C.; Shanahan, F.; Brennan, L.; McAuliffe, F.M. Probiotics in Obese Pregnancy Do Not Reduce Maternal Fasting Glucose: A Double-Blind, Placebo-Controlled, Randomized Trial (Probiotics in Pregnancy Study). Am. J. Clin. Nutr. 2014, 99, 1432–1439. [Google Scholar] [CrossRef]
- Dolatkhah, N.; Hajifaraji, M.; Abbasalizadeh, F.; Aghamohammadzadeh, N.; Mehrabi, Y.; Abbasi, M.M. Is There a Value for Probiotic Supplements in Gestational Diabetes Mellitus? A Randomized Clinical Trial. J. Health Popul. Nutr. 2015, 33, 25. [Google Scholar] [CrossRef]
- Lindsay, K.L.; Brennan, L.; Kennelly, M.A.; Maguire, O.C.; Smith, T.; Curran, S.; Coffey, M.; Foley, M.E.; Hatunic, M.; Shanahan, F.; et al. Impact of Probiotics in Women with Gestational Diabetes Mellitus on Metabolic Health: A Randomized Controlled Trial. Am. J. Obstet. Gynecol. 2015, 212, 496.e1–496.e11. [Google Scholar] [CrossRef]
- Karamali, M.; Dadkhah, F.; Sadrkhanlou, M.; Jamilian, M.; Ahmadi, S.; Tajabadi-Ebrahimi, M.; Jafari, P.; Asemi, Z. Effects of Probiotic Supplementation on Glycaemic Control and Lipid Profiles in Gestational Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Diabetes Metab. 2016, 42, 234–241. [Google Scholar] [CrossRef]
- Jafarnejad, S.; Saremi, S.; Jafarnejad, F.; Arab, A. Effects of a Multispecies Probiotic Mixture on Glycemic Control and Inflammatory Status in Women with Gestational Diabetes: A Randomized Controlled Clinical Trial. J. Nutr. Metab. 2016, 2016, 5190846. [Google Scholar] [CrossRef]
- Halkjaer, S.I.; Nilas, L.; Carlsen, E.M.; Cortes, D.; Halldórsson, T.I.; Olsen, S.F.; Pedersen, A.E.; Krogfelt, K.A.; Petersen, A.M. Effects of Probiotics (Vivomixx®) in Obese Pregnant Women and Their Newborn: Study Protocol for a Randomized Controlled Trial. Trials 2016, 17, 491. [Google Scholar] [CrossRef] [PubMed]
- Wickens, K.L.; Barthow, C.A.; Murphy, R.; Abels, P.R.; Maude, R.M.; Stone, P.R.; Mitchell, E.A.; Stanley, T.V.; Purdie, G.L.; Kang, J.M.; et al. Early Pregnancy Probiotic Supplementation with Lactobacillus Rhamnosus HN001 May Reduce the Prevalence of Gestational Diabetes Mellitus: A Randomised Controlled Trial. Br. J. Nutr. 2017, 117, 804–813. [Google Scholar] [CrossRef]
- Hajifaraji, M.; Jahanjou, F.; Abbasalizadeh, F.; Aghamohammadzadeh, N.; Abbasi, M.M.; Dolatkhah, N. Effect of Probiotic Supplements in Women with Gestational Diabetes Mellitus on Inflammation and Oxidative Stress Biomarkers: A Randomized Clinical Trial. Asia Pac. J. Clin. Nutr. 2018, 27, 581–591. [Google Scholar] [CrossRef]
- Pellonperä, O.; Mokkala, K.; Houttu, N.; Vahlberg, T.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Efficacy of Fish Oil and/or Probiotic Intervention on the Incidence of Gestational Diabetes Mellitus in an At-Risk Group of Overweight and Obese Women: A Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Diabetes Care 2019, 42, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Sahhaf Ebrahimi, F.; Homayouni Rad, A.; Mosen, M.; Abbasalizadeh, F.; Tabrizi, A.; Khalili, L. Effect of L. Acidophilus and B. Lactis on Blood Glucose in Women with Gestational Diabetes Mellitus: A Randomized Placebo-Controlled Trial. Diabetol. Metab. Syndr. 2019, 11, 75. [Google Scholar] [CrossRef]
- Callaway, L.K.; McIntyre, H.D.; Barrett, H.L.; Foxcroft, K.; Tremellen, A.; Lingwood, B.E.; Tobin, J.M.; Wilkinson, S.; Kothari, A.; Morrison, M.; et al. Probiotics for the Prevention of Gestational Diabetes Mellitus in Overweight and Obese Women: Findings From the SPRING Double-Blind Randomized Controlled Trial. Diabetes Care 2019, 42, 364–371. [Google Scholar] [CrossRef]
- Kijmanawat, A.; Panburana, P.; Reutrakul, S.; Tangshewinsirikul, C. Effects of Probiotic Supplements on Insulin Resistance in Gestational Diabetes Mellitus: A Double-Blind Randomized Controlled Trial. J. Diabetes Investig. 2019, 10, 163–170. [Google Scholar] [CrossRef]
- Jamilian, M.; Amirani, E.; Asemi, Z. The Effects of Vitamin D and Probiotic Co-Supplementation on Glucose Homeostasis, Inflammation, Oxidative Stress and Pregnancy Outcomes in Gestational Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. 2019, 38, 2098–2105. [Google Scholar] [CrossRef]
- Babadi, M.; Khorshidi, A.; Aghadavood, E.; Samimi, M.; Kavossian, E.; Bahmani, F.; Mafi, A.; Shafabakhsh, R.; Satari, M.; Asemi, Z. The Effects of Probiotic Supplementation on Genetic and Metabolic Profiles in Patients with Gestational Diabetes Mellitus: A Randomized, Double-Blind, Placebo-Controlled Trial. Probiotics Antimicrob. Proteins 2019, 11, 1227–1235. [Google Scholar] [CrossRef]
- Asgharian, H.; Homayouni-Rad, A.; Mirghafourvand, M.; Mohammad-Alizadeh-Charandabi, S. Effect of Probiotic Yoghurt on Plasma Glucose in Overweight and Obese Pregnant Women: A Randomized Controlled Clinical Trial. Eur. J. Nutr. 2020, 59, 205–215. [Google Scholar] [CrossRef]
- Shahriari, A.; Karimi, E.; Shahriari, M.; Aslani, N.; Khooshideh, M.; Arab, A. The Effect of Probiotic Supplementation on the Risk of Gestational Diabetes Mellitus among High-Risk Pregnant Women: A Parallel Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Biomed. Pharmacother. 2021, 141, 111915. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, J.; Wickens, K.; Stanley, T.; Maude, R.; Stone, P.; Barthow, C.; Crane, J.; Mitchell, E.A.; Merien, F.; et al. Effect of Lactobacillus Rhamnosus Probiotic in Early Pregnancy on Plasma Conjugated Bile Acids in a Randomised Controlled Trial. Nutrients 2021, 13, 209. [Google Scholar] [CrossRef] [PubMed]
- Amirani, E.; Asemi, Z.; Taghizadeh, M. The Effects of Selenium plus Probiotics Supplementation on Glycemic Status and Serum Lipoproteins in Patients with Gestational Diabetes Mellitus: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. Nutr. ESPEN 2022, 48, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Nachum, Z.; Perlitz, Y.; Shavit, L.Y.; Magril, G.; Vitner, D.; Zipori, Y.; Weiner, E.; Alon, A.S.; Ganor-Paz, Y.; Nezer, M.; et al. The Effect of Oral Probiotics on Glycemic Control of Women with Gestational Diabetes Mellitus—A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial. Am. J. Obstet. Gynecol. MFM 2024, 6, 101224. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O. Diabetogenically Beneficial Gut Microbiota Alterations in Third Trimester of Pregnancy. Reprod. Fertil. 2021, 2, R1–R12. [Google Scholar] [CrossRef]
- Yang, H.; Guo, R.; Li, S.; Liang, F.; Tian, C.; Zhao, X.; Long, Y.; Liu, F.; Jiang, M.; Zhang, Y.; et al. Systematic Analysis of Gut Microbiota in Pregnant Women and Its Correlations with Individual Heterogeneity. NPJ Biofilms Microbiomes 2020, 6, 32. [Google Scholar] [CrossRef]
- DiGiulio, D.B.; Callahan, B.J.; McMurdie, P.J.; Costello, E.K.; Lyell, D.J.; Robaczewska, A.; Sun, C.L.; Goltsman, D.S.A.; Wong, R.J.; Shaw, G.; et al. Temporal and Spatial Variation of the Human Microbiota During Pregnancy. Proc. Natl. Acad. Sci. USA 2015, 112, 11060–11065. [Google Scholar] [CrossRef]
- Koren, O.; Goodrich, J.K.; Cullender, T.C.; Spor, A.; Laitinen, K.; Bäckhed, H.K.; Gonzalez, A.; Werner, J.J.; Angenent, L.T.; Knight, R.; et al. Host Remodeling of the Gut Microbiome and Metabolic Changes During Pregnancy. Cell 2012, 150, 470–480. [Google Scholar] [CrossRef]
- Lopez-Tello, J.; Schofield, Z.; Kiu, R.; Dalby, M.J.; van Sinderen, D.; Le Gall, G.; Sferruzzi-Perri, A.N.; Hall, L.J. Maternal Gut Microbiota Bifidobacterium Promotes Placental Morphogenesis, Nutrient Transport and Fetal Growth in Mice. Cell. Mol. Life Sci. 2022, 79, 386. [Google Scholar] [CrossRef]
- Rautava, S.; Selma-Royo, M.; Oksanen, T.; Collado, M.C.; Isolauri, E. Shifting Pattern of Gut Microbiota in Pregnant Women Two Decades Apart—An Observational Study. Gut Microbes 2023, 15, 2234656. [Google Scholar] [CrossRef]
- Li, N.; Liang, S.; Chen, Q.; Zhao, L.; Li, B.; Huo, G. Distinct Gut Microbiota and Metabolite Profiles Induced by Delivery Mode in Healthy Chinese Infants. J. Proteom. 2021, 232, 104071. [Google Scholar] [CrossRef] [PubMed]
- Rutayisire, E.; Huang, K.; Liu, Y.; Tao, F. The Mode of Delivery Affects the Diversity and Colonization Pattern of the Gut Microbiota During the First Year of Infants’ Life: A Systematic Review. BMC Gastroenterol. 2016, 16, 86. [Google Scholar] [CrossRef] [PubMed]
- Reznik, S.E.; Akinyemi, A.J.; Harary, D.; Latuga, M.S.; Fuloria, M.; Charron, M.J. The Effect of Cesarean Delivery on the Neonatal Gut Microbiome in an Under-Resourced Population in the Bronx, NY, USA. BMC Pediatr. 2024, 24, 450. [Google Scholar] [CrossRef]
- Zhou, L.; Qiu, W.; Wang, J.; Zhao, A.; Zhou, C.; Sun, T.; Xiong, Z.; Cao, P.; Shen, W.; Chen, J.; et al. Effects of Vaginal Microbiota Transfer on the Neurodevelopment and Microbiome of Cesarean-Born Infants: A Blinded Randomized Controlled Trial. Cell Host Microbe 2023, 31, 1232–1247.e5. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.R.; Gustafsson, H.C.; DeCapo, M.; Takahashi, D.L.; Bagley, J.L.; Dean, T.A.; Kievit, P.; Fair, D.A.; Sullivan, E.L. Maternal Diet, Metabolic State, and Inflammatory Response Exert Unique and Long-Lasting Influences on Offspring Behavior in Non-Human Primates. Front. Endocrinol. 2018, 9, 161. [Google Scholar] [CrossRef]
- Jeurink, P.V.; Knipping, K.; Wiens, F.; Barańska, K.; Stahl, B.; Garssen, J.; Krolak-Olejnik, B. Importance of Maternal Diet in the Training of the Infant’s Immune System During Gestation and Lactation. Crit. Rev. Food Sci. Nutr. 2019, 59, 1311–1319. [Google Scholar] [CrossRef]
- Karaivazoglou, K.; Triantos, C.; Aggeletopoulou, I. The Role of Maternal and Early-Life Diet in Inflammatory Bowel Disease. Nutrients 2024, 16, 4292. [Google Scholar] [CrossRef]
- Honda, K.; Littman, D.R. The Microbiota in Adaptive Immune Homeostasis and Disease. Nature 2016, 535, 75–84. [Google Scholar] [CrossRef]
- Gil, A.; Rueda, R.; Ozanne, S.E.; van der Beek, E.M.; van Loo-Bouwman, C.; Schoemaker, M.; Edwards, C.A. Is There Evidence for Bacterial Transfer via the Placenta and Any Role in the Colonization of the Infant Gut?—A Systematic Review. Crit. Rev. Microbiol. 2020, 46, 493–507. [Google Scholar] [CrossRef]
- Walker, R.W.; Clemente, J.C.; Peter, I.; Loos, R.J.F. The Prenatal Gut Microbiome: Are We Colonized with Bacteria in Utero? Pediatr. Obes. 2017, 12, 3–17. [Google Scholar] [CrossRef]
- Chen, H.J.; Gur, T.L. Intrauterine Microbiota: Missing, or the Missing Link? Trends Neurosci. 2019, 42, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, E.; Fernández, L.; Marín, M.L.; Martín, R.; Odriozola, J.M.; Nueno-Palop, C.; Narbad, A.; Olivares, M.; Xaus, J.; Rodríguez, J.M. Isolation of Commensal Bacteria from Umbilical Cord Blood of Healthy Neonates Born by Cesarean Section. Curr. Microbiol. 2005, 51, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Zhao, F. Microbial Transmission, Colonisation and Succession: From Pregnancy to Infancy. Gut 2023, 72, 772–786. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Li, Z.; Tye, K.D.; Luo, H.; Tang, X.; Liao, Y.; Wang, D.; Zhou, J.; Yang, P.; Li, Y.; et al. Probiotic Supplementation During Human Pregnancy Affects the Gut Microbiota and Immune Status. Front. Cell. Infect. Microbiol. 2019, 9, 254. [Google Scholar] [CrossRef]
- Chen, X.; Shi, Y. Determinants of Microbial Colonization in the Premature Gut. Mol. Med. 2023, 29, 90. [Google Scholar] [CrossRef]
- Huoman, J.; Martínez-Enguita, D.; Olsson, E.; Ernerudh, J.; Nilsson, L.; Duchén, K.; Gustafsson, M.; Jenmalm, M.C. Combined Prenatal Lactobacillus Reuteri and ω-3 Supplementation Synergistically Modulates DNA Methylation in Neonatal T Helper Cells. Clin. Epigenetics 2021, 13, 135. [Google Scholar] [CrossRef]
- Mealy, G.; Brennan, K.; Killeen, S.L.; Kilbane, M.; Yelverton, C.; Saldova, R.; Groeger, D.; VanSinderen, D.; Cotter, P.D.; Doyle, S.L.; et al. Impact of Previous Pregnancy and BMI on Cellular and Serum Immune Activity from Early to Late Pregnancy. Sci. Rep. 2024, 14, 16055. [Google Scholar] [CrossRef]
- Jenmalm, M.C. The Mother-Offspring Dyad: Microbial Transmission, Immune Interactions and Allergy Development. J. Intern. Med. 2017, 282, 484–495. [Google Scholar] [CrossRef]
- Xi, Z.; Fenglin, X.; Yun, Z.; Chunrong, L. Efficacy of Probiotics in the Treatment of Allergic Diseases: A Meta-Analysis. Front. Nutr. 2025, 12, 1502390. [Google Scholar] [CrossRef]
- Mubanga, M.; Lundholm, C.; D’Onofrio, B.M.; Stratmann, M.; Hedman, A.; Almqvist, C. Association of Early Life Exposure to Antibiotics with Risk of Atopic Dermatitis in Sweden. JAMA Netw. Open 2021, 4, e215245. [Google Scholar] [CrossRef]
- Tuniyazi, M.; Li, S.; Hu, X.; Fu, Y.; Zhang, N. The Role of Early Life Microbiota Composition in the Development of Allergic Diseases. Microorganisms 2022, 10, 1190. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Zhao, D.; Cheng, Q.; Zhang, Y.; Wang, S.; Zhang, H.; Xie, M.; He, R.; Su, H. Trimester-Specific Association Between Antibiotics Exposure During Pregnancy and Childhood Asthma or Wheeze: The Role of Confounding. Ann. Epidemiol. 2019, 30, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kuper, C.F.; van Bilsen, J.; Cnossen, H.; Houben, G.; Garthoff, J.; Wolterbeek, A. Development of Immune Organs and Functioning in Humans and Test Animals: Implications for Immune Intervention Studies. Reprod. Toxicol. 2016, 64, 180–190. [Google Scholar] [CrossRef]
- Spencer, J.; MacDonald, T.T.; Finn, T.; Isaacson, P.G. The Development of Gut Associated Lymphoid Tissue in the Terminal Ileum of Fetal Human Intestine. Clin. Exp. Immunol. 1986, 64, 536–543. [Google Scholar]
- Xiao, L.; Gong, C.; Ding, Y.; Ding, G.; Xu, X.; Deng, C.; Ze, X.; Malard, P.; Ben, X. Probiotics Maintain Intestinal Secretory Immunoglobulin A Levels in Healthy Formula-Fed Infants: A Randomised, Double-Blind, Placebo-Controlled Study. Benef. Microbes 2019, 10, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Ding, G.; Ding, Y.; Deng, C.; Ze, X.; Chen, L.; Zhang, Y.; Song, L.; Yan, H.; Liu, F.; et al. Effect of Probiotics on Digestibility and Immunity in Infants: A Study Protocol for a Randomized Controlled Trial. Medicine 2017, 96, e5953. [Google Scholar] [CrossRef]
- Han, M.-M.; Sun, J.-F.; Su, X.-H.; Peng, Y.-F.; Goyal, H.; Wu, C.-H.; Zhu, X.-Y.; Li, L. Probiotics Improve Glucose and Lipid Metabolism in Pregnant Women: A Meta-Analysis. Ann. Transl. Med. 2019, 7, 99. [Google Scholar] [CrossRef]
- Homayoni Rad, A.; Mehrabany, E.V.; Alipoor, B.; Mehrabany, L.V.; Javadi, M. Do Probiotics Act More Efficiently in Foods than in Supplements? Nutrition 2012, 28, 733–736. [Google Scholar] [CrossRef]
- Miao, T.; Yu, Y.; Sun, J.; Ma, A.; Yu, J.; Cui, M.; Yang, L.; Wang, H. Decrease in Abundance of Bacteria of the Genus Bifidobacterium in Gut Microbiota May Be Related to Pre-Eclampsia Progression in Women from East China. Food Nutr. Res. 2021, 65, 5781. [Google Scholar] [CrossRef]
- Ma, G.; Yan, H.; Tye, K.D.; Tang, X.; Luo, H.; Li, Z.; Xiao, X. Effect of Probiotic Administration During Pregnancy on the Functional Diversity of the Gut Microbiota in Healthy Pregnant Women. Microbiol. Spectr. 2024, 12, e0041324. [Google Scholar] [CrossRef]
- Hoppu, U.; Isolauri, E.; Koskinen, P.; Laitinen, K. Maternal Dietary Counseling Reduces Total and LDL Cholesterol Postpartum. Nutrition 2014, 30, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Layden, B.T.; Angueira, A.R.; Brodsky, M.; Durai, V.; Lowe, W.L. Short Chain Fatty Acids and Their Receptors: New Metabolic Targets. Transl. Res. 2013, 161, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Yadav, H.; Lee, J.-H.; Lloyd, J.; Walter, P.; Rane, S.G. Beneficial Metabolic Effects of a Probiotic via Butyrate-Induced GLP-1 Hormone Secretion. J. Biol. Chem. 2013, 288, 25088–25097. [Google Scholar] [CrossRef]
- Mokkala, K.; Gustafsson, J.; Vahlberg, T.; Vreugdenhil, A.C.E.; Ding, L.; Shiri-Sverdlov, R.; Plat, J.; Laitinen, K. Serum CathepsinD in Pregnancy: Relation with Metabolic and Inflammatory Markers and Effects of Fish Oils and Probiotics. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Feng, Q.; Zheng, S.; Xiao, X. The Effects of Probiotics Supplementation on Metabolic Health in Pregnant Women: An Evidence Based Meta-Analysis. PLoS ONE 2018, 13, e0197771. [Google Scholar] [CrossRef]
- Barz, M.L.; Anhê, F.F.; Varin, T.V.; Desjardins, Y.; Levy, E.; Roy, D.; Urdaci, M.C.; Marette, A. Probiotics as Complementary Treatment for Metabolic Disorders. Diabetes Metab. J. 2015, 39, 291–303. [Google Scholar] [CrossRef]
- Kemgang, T.S.; Kapila, S.; Shanmugam, V.P.; Kapila, R. Cross-Talk Between Probiotic Lactobacilli and Host Immune System. J. Appl. Microbiol. 2014, 117, 303–319. [Google Scholar] [CrossRef]
- Kelly, A.C.; Powell, T.L.; Jansson, T. Placental Function in Maternal Obesity. Clin. Sci. 2020, 134, 961–984. [Google Scholar] [CrossRef]
- Gomez Arango, L.F.; Barrett, H.L.; Callaway, L.K.; Nitert, M.D. Probiotics and Pregnancy. Curr. Diabetes Rep. 2015, 15, 567. [Google Scholar] [CrossRef]
- Halkjær, S.I.; de Knegt, V.E.; Lo, B.; Nilas, L.; Cortes, D.; Pedersen, A.E.; Mirsepasi-Lauridsen, H.C.; Andersen, L.O.; Nielsen, H.V.; Stensvold, C.R.; et al. Multistrain Probiotic Increases the Gut Microbiota Diversity in Obese Pregnant Women: Results from a Randomized, Double-Blind Placebo-Controlled Study. Curr. Dev. Nutr. 2020, 4, nzaa095. [Google Scholar] [CrossRef]
- Chatzakis, C.; Goulis, D.G.; Mareti, E.; Eleftheriades, M.; Zavlanos, A.; Dinas, K.; Sotiriadis, A. Prevention of Gestational Diabetes Mellitus in Overweight or Obese Pregnant Women: A Network Meta-Analysis. Diabetes Res. Clin. Pract. 2019, 158, 107924. [Google Scholar] [CrossRef]
- Halkjær, S.I.; Refslund Danielsen, M.; de Knegt, V.E.; Andersen, L.O.; Stensvold, C.R.; Nielsen, H.V.; Mirsepasi-Lauridsen, H.C.; Krogfelt, K.A.; Cortes, D.; Petersen, A.M. Multi-Strain Probiotics During Pregnancy in Women with Obesity Influence Infant Gut Microbiome Development: Results from a Randomized, Double-Blind Placebo-Controlled Study. Gut Microbes 2024, 16, 2337968. [Google Scholar] [CrossRef]
- Edwards, S.M.; Cunningham, S.A.; Dunlop, A.L.; Corwin, E.J. The Maternal Gut Microbiome During Pregnancy. MCN Am. J. Matern. Child Nurs. 2017, 42, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Zouiouich, S.; Vanderbauwhede, B.; Vanacker, J.; Indave Ruiz, B.I.; Huybrechts, I. Human Microbiome and Metabolic Health: An Overview of Systematic Reviews. Obes. Rev. 2022, 23, e13409. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.L.; Woodfall, G.E.; Sheedy, K.E.; O’Riley, M.L.; Rainbow, K.A.; Bramwell, E.L.; Kellow, N.J. Effect of Probiotics on Metabolic Outcomes in Pregnant Women with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2017, 9, 461. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hu, X.; Wang, Y.; He, C.; Yu, J.; Fang, X.; Zhang, Y.; Xu, X.; Yang, J. Effects of Probiotic Supplementation on Glucose Metabolism in Pregnant Women without Diabetes: A Systematic Review and Meta-Analysis. Food Funct. 2022, 13, 8388–8398. [Google Scholar] [CrossRef]
- Sun, J.; Gajurel, D.; Buys, N.; Yin, C. Chapter 17—Effects of Probiotics on Improvement of Metabolic Factors in Pregnant Women: A Metaanalysis of Randomized Placebo-Controlled Trials. In Microbiome and Metabolome in Diagnosis, Therapy, and Other Strategic Applications; Faintuch, J., Faintuch, S., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 167–176. [Google Scholar] [CrossRef]
- Mahdizade Ari, M.; Teymouri, S.; Fazlalian, T.; Asadollahi, P.; Afifirad, R.; Sabaghan, M.; Valizadeh, F.; Ghanavati, R.; Darbandi, A. The Effect of Probiotics on Gestational Diabetes and Its Complications in Pregnant Mother and Newborn: A Systematic Review and Meta-Analysis During 2010–2020. J. Clin. Lab. Anal. 2022, 36, e24326. [Google Scholar] [CrossRef]
- Obuchowska, A.; Gorczyca, K.; Standyło, A.; Obuchowska, K.; Kimber-Trojnar, Ż.; Wierzchowska-Opoka, M.; Leszczyńska-Gorzelak, B. Effects of Probiotic Supplementation During Pregnancy on the Future Maternal Risk of Metabolic Syndrome. Int. J. Mol. Sci. 2022, 23, 8253. [Google Scholar] [CrossRef]
- Wang, J.; Gu, X.; Yang, J.; Wei, Y.; Zhao, Y. Gut Microbiota Dysbiosis and Increased Plasma LPS and TMAO Levels in Patients with Preeclampsia. Front. Cell Infect. Microbiol. 2019, 9, 409. [Google Scholar] [CrossRef]
- Olaniyi, K.S.; Moodley, J.; Mahabeer, Y.; Mackraj, I. Placental Microbial Colonization and Its Association with Pre-Eclampsia. Front. Cell Infect. Microbiol. 2020, 10, 413. [Google Scholar] [CrossRef]
- Liu, Y.; Gao, S.; Zhao, Y.; Wang, H.; Pan, Q.; Shao, Q. Decidual Natural Killer Cells: A Good Nanny at the Maternal-Fetal Interface During Early Pregnancy. Front. Immunol. 2021, 12, 663660. [Google Scholar] [CrossRef] [PubMed]
- Bellos, I.; Daskalakis, G.; Pergialiotis, V. Helicobacter Pylori Infection Increases the Risk of Developing Preeclampsia: A Meta-Analysis of Observational Studies. Int. J. Clin. Pract. 2018, 72, e13064. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Stout, M.J.; Lee, I.; Mysorekar, I.U. Placental Microbiome and Its Role in Preterm Birth. Neoreviews 2014, 15, e537–e545. [Google Scholar] [CrossRef] [PubMed]
- Panzer, J.J.; Romero, R.; Greenberg, J.M.; Winters, A.D.; Galaz, J.; Gomez-Lopez, N.; Theis, K.R. Is There a Placental Microbiota? A Critical Review and Re-Analysis of Published Placental Microbiota Datasets. BMC Microbiol. 2023, 23, 76. [Google Scholar] [CrossRef]
- Theis, K.R.; Romero, R.; Winters, A.D.; Greenberg, J.M.; Gomez-Lopez, N.; Alhousseini, A.; Bieda, J.; Maymon, E.; Pacora, P.; Fettweis, J.M.; et al. Does the Human Placenta Delivered at Term Have a Microbiota? Results of Cultivation, Quantitative Real-Time PCR, 16S rRNA Gene Sequencing, and Metagenomics. Am. J. Obstet. Gynecol. 2019, 220, 267.e1–267.e39. [Google Scholar] [CrossRef]
- Rybak-Krzyszkowska, M.; Staniczek, J.; Kondracka, A.; Bogusławska, J.; Kwiatkowski, S.; Góra, T.; Strus, M.; Górczewski, W. From Biomarkers to the Molecular Mechanism of Preeclampsia—A Comprehensive Literature Review. Int. J. Mol. Sci. 2023, 24, 13252. [Google Scholar] [CrossRef]
- Nordqvist, M.; Jacobsson, B.; Brantsæter, A.-L.; Myhre, R.; Nilsson, S.; Sengpiel, V. Timing of Probiotic Milk Consumption During Pregnancy and Effects on the Incidence of Preeclampsia and Preterm Delivery: A Prospective Observational Cohort Study in Norway. BMJ Open 2018, 8, e018021. [Google Scholar] [CrossRef]
- Crusell, M.K.W.; Hansen, T.H.; Nielsen, T.; Allin, K.H.; Rühlemann, M.C.; Damm, P.; Vestergaard, H.; Rørbye, C.; Jørgensen, N.R.; Christiansen, O.B.; et al. Gestational Diabetes Is Associated with Change in the Gut Microbiota Composition in Third Trimester of Pregnancy and Postpartum. Microbiome 2018, 6, 89. [Google Scholar] [CrossRef]
- Taylor, B.D.; Ness, R.B.; Olsen, J.; Hougaard, D.M.; Skogstrand, K.; Roberts, J.M.; Haggerty, C.L. Serum Leptin Measured in Early Pregnancy Is Higher in Women with Preeclampsia Compared with Normotensive Pregnant Women. Hypertension 2015, 65, 594–599. [Google Scholar] [CrossRef]
- Davidson, S.J.; Barrett, H.L.; Price, S.A.; Callaway, L.K.; Dekker Nitert, M. Probiotics for Preventing Gestational Diabetes. Cochrane Database Syst. Rev. 2021, 4, CD009951. [Google Scholar] [CrossRef]
- Swati, P.; Ambika Devi, K.; Thomas, B.; Vahab, S.A.; Kapaettu, S.; Kushtagi, P. Simultaneous Detection of Periodontal Pathogens in Subgingival Plaque and Placenta of Women with Hypertension in Pregnancy. Arch. Gynecol. Obstet. 2012, 285, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, A.; Cutler, C.; Farnham, G.; Liddle, L.; Burleigh, M.; Rodiles, A.; Sillitti, C.; Kiernan, M.; Moore, M.; Hickson, M.; et al. Dietary Intake of Inorganic Nitrate in Vegetarians and Omnivores and Its Impact on Blood Pressure, Resting Metabolic Rate and the Oral Microbiome. Free Radic. Biol. Med. 2019, 138, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Shi, Z.-H.; Yang, J.; Wei, Y.; Wang, X.-Y.; Zhao, Y.-Y. Gut Microbiota Dysbiosis in Preeclampsia Patients in the Second and Third Trimesters. Chin. Med. J. 2020, 133, 1057–1065. [Google Scholar] [CrossRef]
- Bezirtzoglou, E.; Stavropoulou, E. Immunology and Probiotic Impact of the Newborn and Young Children Intestinal Microflora. Anaerobe 2011, 17, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Hadders-Algra, M.; Bouwstra, H.; van Goor, S.A.; Dijck-Brouwer, D.A.J.; Muskiet, F.A.J. Prenatal and Early Postnatal Fatty Acid Status and Neurodevelopmental Outcome. J. Perinat. Med. 2007, 35 (Suppl. S1), S28–S34. [Google Scholar] [CrossRef]
- Vitali, B.; Cruciani, F.; Baldassarre, M.E.; Capursi, T.; Spisni, E.; Valerii, M.C.; Candela, M.; Turroni, S.; Brigidi, P. Dietary Supplementation with Probiotics During Late Pregnancy: Outcome on Vaginal Microbiota and Cytokine Secretion. BMC Microbiol. 2012, 12, 236. [Google Scholar] [CrossRef]
- Gao, Z.; Daquinag, A.C.; Yu, Y.; Kolonin, M.G. Endothelial Prohibitin Mediates Bidirectional Long-Chain Fatty Acid Transport in White and Brown Adipose Tissues. Diabetes 2022, 71, 1400–1409. [Google Scholar] [CrossRef]
- Daskalakis, G.J.; Karambelas, A.K. Vaginal Probiotic Administration in the Management of Preterm Premature Rupture of Membranes. Fetal Diagn. Ther. 2016, 42, 92–98. [Google Scholar] [CrossRef]
- Welp, A.; Laser, E.; Seeger, K.; Haiß, A.; Hanke, K.; Faust, K.; Stichtenoth, G.; Fortmann-Grote, C.; Pagel, J.; Rupp, J.; et al. Effects of Multistrain Bifidobacteria and Lactobacillus Probiotics on HMO Compositions After Supplementation to Pregnant Women at Threatening Preterm Delivery: Design of the Randomized Clinical PROMO Trial. Mol. Cell. Pediatr. 2024, 11, 6. [Google Scholar] [CrossRef]
- Grev, J.; Berg, M.; Soll, R. Maternal Probiotic Supplementation for Prevention of Morbidity and Mortality in Preterm Infants. Cochrane Database Syst. Rev. 2018, 12, CD012519. [Google Scholar] [CrossRef]
- Husain, S.; Allotey, J.; Drymoussi, Z.; Wilks, M.; Fernandez-Felix, B.; Whiley, A.; Dodds, J.; Thangaratinam, S.; McCourt, C.; Prosdocimi, E.; et al. Effects of Oral Probiotic Supplements on Vaginal Microbiota During Pregnancy: A Randomised, Double-Blind, Placebo-Controlled Trial with Microbiome Analysis. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.V. Chemical Mechanisms of Colonization Resistance by the Gut Microbial Metabolome. ACS Chem. Biol. 2020, 15, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Mazurel, D.; Carda-Diéguez, M.; Langenburg, T.; Žiemytė, M.; Johnston, W.; Martínez, C.P.; Albalat, F.; Llena, C.; Al-Hebshi, N.; Culshaw, S.; et al. Nitrate and a Nitrate-Reducing Rothia Aeria Strain as Potential Prebiotic or Synbiotic Treatments for Periodontitis. NPJ Biofilms Microbiomes 2023, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Dawe, J.P.; McCowan, L.M.E.; Wilson, J.; Okesene-Gafa, K.A.M.; Serlachius, A.S. Probiotics and Maternal Mental Health: A Randomised Controlled Trial among Pregnant Women with Obesity. Sci. Rep. 2020, 10, 1291. [Google Scholar] [CrossRef]
- Kwok, K.O.; Fries, L.R.; Silva-Zolezzi, I.; Thakkar, S.K.; Iroz, A.; Blanchard, C. Effects of Probiotic Intervention on Markers of Inflammation and Health Outcomes in Women of Reproductive Age and Their Children. Front. Nutr. 2022, 9, 889040. [Google Scholar] [CrossRef]
- De Andrés, J.; Manzano, S.; García, C.; Rodríguez, J.M.; Espinosa-Martos, I.; Jiménez, E. Modulatory Effect of Three Probiotic Strains on Infants’ Gut Microbial Composition and Immunological Parameters on a Placebo-Controlled, Double-Blind, Randomised Study. Benef. Microbes 2018, 9, 573–584. [Google Scholar] [CrossRef]
- Azad, M.A.K.; Sarker, M.; Wan, D. Immunomodulatory Effects of Probiotics on Cytokine Profiles. Biomed Res. Int. 2018, 2018, 8063647. [Google Scholar] [CrossRef]
- Tsai, Y.-T.; Cheng, P.-C.; Pan, T.-M. The Immunomodulatory Effects of Lactic Acid Bacteria for Improving Immune Functions and Benefits. Appl. Microbiol. Biotechnol. 2012, 96, 853–862. [Google Scholar] [CrossRef]
- Colquitt, A.S.; Miles, E.A.; Calder, P.C. Do Probiotics in Pregnancy Reduce Allergies and Asthma in Infancy and Childhood? A Systematic Review. Nutrients 2022, 14, 1852. [Google Scholar] [CrossRef]
- Garcia-Larsen, V.; Ierodiakonou, D.; Jarrold, K.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Ruparelia, A.; Devani, P.; Trivella, M.; et al. Diet During Pregnancy and Infancy and Risk of Allergic or Autoimmune Disease: A Systematic Review and Meta-Analysis. PLoS Med. 2018, 15, e1002507. [Google Scholar] [CrossRef]
- Okesene-Gafa, K.A.M.; Li, M.; McKinlay, C.J.D.; Taylor, R.S.; Rush, E.C.; Wall, C.R.; Wilson, J.; Murphy, R.; Taylor, R.; Thompson, J.M.D.; et al. Effect of Antenatal Dietary Interventions in Maternal Obesity on Pregnancy Weight-Gain and Birthweight: Healthy Mums and Babies (HUMBA) Randomized Trial. Am. J. Obstet. Gynecol. 2019, 221, 152.e1–152.e13. [Google Scholar] [CrossRef] [PubMed]
- Kadooka, Y.; Sato, M.; Ogawa, A.; Miyoshi, M.; Uenishi, H.; Ogawa, H.; Ikuyama, K.; Kagoshima, M.; Tsuchida, T. Effect of Lactobacillus Gasseri SBT2055 in Fermented Milk on Abdominal Adiposity in Adults in a Randomised Controlled Trial. Br. J. Nutr. 2013, 110, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Ilmonen, J.; Isolauri, E.; Poussa, T.; Laitinen, K. Impact of Dietary Counselling and Probiotic Intervention on Maternal Anthropometric Measurements During and After Pregnancy: A Randomized Placebo-Controlled Trial. Clin. Nutr. 2011, 30, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Masulli, M.; Vitacolonna, E.; Fraticelli, F.; Della Pepa, G.; Mannucci, E.; Monami, M. Effects of Probiotic Supplementation During Pregnancy on Metabolic Outcomes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Diabetes Res. Clin. Pract. 2020, 162, 108111. [Google Scholar] [CrossRef]
- Gomez-Arango, L.F.; Barrett, H.L.; McIntyre, H.D.; Callaway, L.K.; Morrison, M.; Dekker Nitert, M.; SPRING Trial Group. Connections Between the Gut Microbiome and Metabolic Hormones in Early Pregnancy in Overweight and Obese Women. Diabetes 2016, 65, 2214–2223. [Google Scholar] [CrossRef]
- Li, P.; Wang, H.; Guo, L.; Gou, X.; Chen, G.; Lin, D.; Fan, D.; Guo, X.; Liu, Z. Association Between Gut Microbiota and Preeclampsia-Eclampsia: A Two-Sample Mendelian Randomization Study. BMC Med. 2022, 20, 443. [Google Scholar] [CrossRef]
- International Scientific Association for Probiotics and Prebiotics (ISAPP). Can Probiotics Cause Harm? The Example of Pregnancy. Available online: https://isappscience.org/can-probiotics-cause-harm-the-example-of-pregnancy/ (accessed on 1 November 2023).

{kind=link}
{kind=link}
| Authors, Reference, Year | Study Design | Cases (Probiotics/Placebo) | BMI | Age | Probiotic Intervention | Dose CFU/Day | Intervention Period | Outcomes | Results | Overall Bias Risk |
|---|---|---|---|---|---|---|---|---|---|---|
| Rinne [9], 2005 | D-B, P-CCT | 96 | N/A | N/A | - Lacticaseibacillus rhamnosus GG | >1 × 1010 | 4 wks before expected delivery, and 6 m postpartum in infants | To assess the impact of intervention and breastfeeding on gut microecology. | Probiotics in the mother’s diet before delivery and in the infant’s diet during breastfeeding may positively influence the maturation process of gut immunity. |  |
| Marschan [10], 2008 | D-B, P-CCT | 98 (52/46) | N/A | N/A | - Lcb. rhamnosus (GG, LC705) - B. breve Bb99 - Propionibacterium freudenreichii subsp. shermanii JS | 5 × 109 5 × 109 2 × 108 3 × 109, 2 cps/day | 4 wks before delivery, and < 6 m postnatally in infants (family history of allergy) | Effect on in vivo cytokine, antibody, and inflammatory responses in allergy-prone infants. | The elevation of IgE, IgA, and IL-10 characterized probiotic-induced low-grade inflammation. ↑ Plasma CRP levels at 6 m was associated with a decreased risk of eczema and allergic disease at 2 yrs. |  |
| Kopp [11], 2008 | Prospective, D-B, P-CCT | 68 (40/28) | N/A | N/A | - Lcb. rhamnosus GG | 5 × 109, twice daily | 4–6 wks before expected delivery, and postnatal for 6 m | Proliferative response and cytokine release in cultures of isolated mononuclear cells. | No difference in proliferative capacity or cytokine pattern of maternal or neonatal cord blood cells in response to IL-2, β-lactoglobulin, or LGG. |  |
| Rautava [12], 2012 | D-B, P-CCT | 43 (28/15) | N/A | N/A | - Lcb. rhamnosus GG - B. lactis | 1 × 109, each | 14 days before elective cesarean at full-term | Innate immune gene expression profiles in the placenta and fetal gut may be modulated during late pregnancy. | Significantly modulated the expression of TLR-related genes both in the placenta and in the fetal gut. | |
| Rø [13], 2017 | D-B, P-CCT | 415 (211/204) | 29.3/29.7 | 30.8/ 30.4 | - Lcb. rhamnosus GG - B. animalis subsp. lactis Bb-12 - L. acidophilus La-5 | 5 × 1010 5 × 1010 5 × 109 | From 36 wks to 3 m postnatally while breastfeeding | Modifying Th cell proportions could mediate the preventive effect of probiotics on AD. | Perinatal intervention with probiotics reduced the proportion of Th22 cells in 3-month-old children, which may explain the partial protective effect on Alzheimer’s disease. | |
| Forsberg [14], 2020 | Prospective, D-B, P-CCT | 88 | N/A | N/A | - Limosilactobacillus reuteri (formerly Lactobacillus reuteri) | 1 × 109, plus ω-3 PUFA 3 capsules twice daily | From 20 wks until delivery | Maternal peripheral immunity. | Some immunomodulatory effects were observed among circulating activated and resting T cells. | |
| Soukka [15], 2023 | D-B, P-CCT | 439 fish oil + probiotics n = 109 placebo n = 110 | 28.8/28.9 | 30.7/31 | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010, each | From early pregnancy (<18 wks) until 6 m postnatally in women with pre-pregnancy BMI ≥ 25 and ≥30 kg/m2 | Modified concentrations of colostrum immune mediators and associations with perinatal clinical factors on mothers with overweight/obesity. | The fish oil + probiotics group had higher levels of IL-12p70, FLT-3L, and IFNα2. Intervention exerted a minor effect on concentrations of colostrum immune mediators and may contribute to immune system development in the infant. | |
| Killeen [16], 2024 | D-B, P-CCT | 72 (36/36) | 36/36 | 36/36 | - B. lactis NCIMB 30435 (formerly B. longum subsp. longum 1714) | >1 × 109 | From 16–20 wks until delivery | Change in IL-10 production after stimulation with lipopolysaccharide. | Not alter cytokine production by maternal PBMCs in response to PAMPs or anti-CD3/28/2 | |
Low risk; Moderate risk; High risk.| Authors, Reference, Year |
Study
Design | Cases (Probiotics/Placebo) | BMI | Age |
Probiotic
Intervention |
Dose
CFU/Day |
Intervention
Period | Outcomes | Results | Overall Bias Risk |
|---|---|---|---|---|---|---|---|---|---|---|
| Kalliomäki [17], 2001 | D-B, P-CCT | 159 (270/270) | N/A | N/A | - Lcb. rhamnosus GG | >1 × 109 | For 2–4 wks before expected delivery, and 6 m postnatally in women if breastfeeding | Preventing early atopic disease. | Effective in prevention of early atopic disease in children at high risk. | |
| Kukkonen [18], 2007 | D-B, P-CCT | 1223 (610/613) | N/A | N/A | - Lcb. rhamnosus (GG, LC705) - B. breve Bb99 - P. freudenreichii subsp. shermanii JS | 5 × 109 5 × 109 2 × 108 2 × 109 | For 2–4 wks before delivery and 3 m postnatally in infants | Preventing allergic diseases. | No effect on all allergic diseases by age 2 yrs, but prevented eczema and AD; results suggest an inverse association between atopic diseases and gut colonization by probiotics. | |
| Abrahamsson [19], 2007 | Prospective, multicenter, D-B, P-CCT | 232 (117/115) | N/A | N/A | - Limosilactobacillus reuteri | 1 × 108 | From 36 wks until delivery, and postnatal for 12 m to their infants | Allergic disease with or without a positive skin prick test or circulating IgE to food allergens. | No preventive effect of eczema; the treated infants had less IgE-associated eczema at 2 yrs and possibly a reduced risk of developing later respiratory allergic disease. | |
| Huurre [20], 2008 | D-B, P-CCT | 171 (72/99) | N/A | N/A | - Lcb. rhamnosus GG (ATCC 53103) - B. lactis Bb-12 | 1 × 1010, each | From the first trimester to the end of exclusive breastfeeding | Maternal allergy prevention, infant sensitization. | Infants of atopic mothers, when breastfed exclusively over 2.5 m or a total over 6 m, had a higher risk of AS at 12 m; the risk was reduced by the use of probiotics. | |
| Niers [21], 2009 | D-B, P-CCT | 156 (78/78) | N/A | 31.4/32.3 | - B. bifidum W23 - B. lactis W52 - Lactococcus lactis W58 | 1 × 109, each | During the last 6 wks before expected delivery, and postnatal for 12 m to their infants | Effects on the development of eczema in the first 2 yrs, and on early microbial colonization and immune responses. | Preventive effect of early administration on the incidence of eczema in the first 3 m, with significant changes in the intestinal microbiota and decreased IL-5 production. | |
| Kuitunen [22], 2009 | D-B, P-CCT | 1223 (991 children) (445/446) | N/A | N/A | - Lcb. rhamnosus (LC705, GG) - B. breve Bb99, - P. freudenreichii subsp. shermanii JS | 5 × 109 5 × 109 2 × 108 2 × 109 2 cps/day | During last month, and 6 m postnatally in infants | Preventing allergic diseases. | No allergy-preventive effect during the last month of pregnancy and for infants 6 m after birth, with evaluation at 5 yrs. Protection only to cesarean-delivered children. | |
| Kim [23], 2010 | D-B, P-CCT | 112 (57/55) | N/A | 29.9/29.5 | - B. bifidum BGN4, - B. lactis AD011 - L. acidophilus AD031 | 1.6 × 109, each | For 4–8 wks before delivery, and 6 m postnatally in women if breastfeeding | Preventing the development of eczema and AS against food allergens in infants at high risk of atopic disease. | Beneficial effect to prevent development of eczema in infants at high risk during their first year of life. | |
| Dotterud [24], 2010 | D-B | 415 (138/140) | N/A | 29.9/29.7 | - Lcb. rhamnosus GG - L. acidophilus La-5 - B. animalis subsp. lactis Bb-12 | 5 × 1010 5 × 109 5 × 1010 | From 36 wks until delivery to 3 m postnatally during breastfeeding | Preventing AS or allergic diseases during the child’s first 2 yrs. | Reduced the cumulative incidence of atopic dermatitis but did not affect AS. | |
| Boyle [25], 2011 | Controlled trial | 250 (125/125) | N/A | N/A | - Lcb. rhamnosus GG | 1.8 × 1010 | From 36 wks until delivery | Preventing the development of eczema. | No reduced risk of eczema or IgE-associated eczema. No change in cord blood immune markers. ↓ Breast milk CD14/IgA levels. | |
| Wickens [26], 2012 | D-B, P-CCT | 474 (315/159) | N/A | N/A | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis HN019 | 6 × 109 9 × 1010 | From 35 wks until delivery, and 6 m postnatally in women if breastfeeding, and until 2 yrs in infants | Prevalence of eczema and allergic diseases at 4 yrs. | Reduced the cumulative prevalence of eczema and rhinoconjunctivitis at 4 years. | |
| Ismail [27], 2012 | D-B, P-CCT | 98 (50/48) | N/A | N/A | - Lcb. rhamnosus GG | 1.8 × 1010 | From 36 wks until delivery | Preventing the development of eczema in infants at high risk of allergic disease. | Administration of probiotics to mothers failed to modulate the diversity of infant gut microbiota in the first week of life. | |
| Kuitunen [28], 2012 | Prospective, D-B, P-CCT | 346 (166/180) | N/A | N/A | - Lcb. rhamnosus (GG, LC705) - B. breve Bb99 - P. freudenreichii subsp. shermanii JS | 5 × 109 5 × 109 2 × 108 2 × 109 | From 36 wks until delivery in women with allergic disease, and postnatal for 6 m to their infants | Preventing allergic disease/IgE-associated allergic disease cumulatively and eczema/AD until ages 2 and 5. | Increased IL-10 and decreased casein IgA antibodies in colostrum. Minor effects on allergy development in children until the ages of 2 and 5. | |
| Rautava [29], 2012 | Prospective, parallel group, D-B, P-CCT | 241 (163/78) | N/A | N/A | (1)— - Lcb. rhamnosus LPR - B. longum BL999 (LPR + BL999) (2)— - Lcb. paracasei ST11 (formerly Lactobacillus paracasei) - B. longum BL999 (ST11 + BL999) | 1 × 109, each | From 2 m until delivery, and 2 m postnatally if breastfeeding in women with allergic disease/AS. | Cumulative incidence of eczema in the infant up to 2 yrs. AS in the infants. | Prevention probiotics administered prenatally/postnatally are safe and effective in reducing the risk of eczema and have no effect on the risk of AS in infants with allergic mothers. | |
| Allen [30], 2014 | D-B, P-CCT, parallel-group | 454 (220/234) | N/A | N/A | - Ligilactobacillus salivarius CUL61 - Lcb. paracasei CUL08 - B. animalis subsp. lactis CUL34, - B. bifidum CUL20 | 6.25 × 109 1.25 × 109 1.25 × 109 1.25 × 109 | From 36 wks until expected delivery, and 6 m postnatally in infants | Cumulative frequency of diagnosed eczema at 2 yr follow-up. | Prevent AS to common food allergens and reduce the incidence of atopic eczema in early childhood. | |
| Kim [31], 2015 | D-B, P-CCT | 123 (60/63) | N/A | N/A | - B. bifidum W23, - B. animalis subsp. lactis W52 - Lactococcus lactis W58 | 1 × 109, each | For 6 wks until delivery (family history of allergic disease), and postnatal for 12 m to their infants | Preventing the development of eczema until 2 yrs. | Induced higher levels of lactate and SCFAs and lower levels of lactose and succinate. Bacterial metabolites may play a role in developing the immune system and have temporary preventive effects on the development of eczema. | |
| Simpson [32], 2015 | D-B, P-CCT | 415 (211/204) | N/A | N/A | - Lcb. rhamnosus GG - L. acidophilus La-5 - B. animalis subsp. lactis Bb-12 | 5 × 1010 5 × 109 5 × 1010 | From 36 wks before expected delivery until 3 m postnatally | Incidence of AD, allergic rhinoconjunctivitis, AS; prevalence of asthma at 12 m. | Long-term reduction in the cumulative incidence of AD, but not other allergy-related conditions (asthma, AS). | |
| Barthow [33], 2016 | D-B, P-CCT | 400 (200/200) | 31.9/ 31.6 | 31.3/ 31.7 | - Lcb. rhamnosus HN001 | 6 × 109 | From 14–16 wks until delivery, and 6 m postnatally if women breastfeeding | Prevalence of infant eczema and AS, GDM, maternal postpartum depression and anxiety. | Probiotic action prevents infant eczema, atopic disease, and GDM at one year. | |
| Wickens [34], 2018 | D-B, P-CCT, parallel-group | 423 (212/211) | N/A | N/A | - Lcb. rhamnosus HN001 | 6 × 109 | From 14–16 wks before delivery, and 6 m postnatally if women breastfeeding | Prevalence of infant eczema and AS. | Maternal and infant probiotic supplementation may be effective for preventing infant eczema. No significant effect on eczema, wheeze, or AS in the child by age 12 m. No effect on the levels of breast milk proteins, TGFβ1, TGFβ2, and IgA. | |
| Davies [35], 2018 | D-B, P-CCT, parallel-group | 452 (220/234) | N/A | N/A | - Lgb. salivarius CUL61 - Lcb. paracasei CUL08 - B. animalis subsp. lactis CUL34 - B. bifidum CUL20 | 1 × 1010, each | From 36 wks until delivery, and postnatal for 6 m to their infants | Prevalence of eczema and asthma at or before 2 yrs of age. | The 5-year electronic follow-up did not find support for the effect of early use of probiotics on childhood eczema or asthma. | |
| Shipton [36], 2024 | D-B, P-CCT | 411 (207/204) | 32.6/32.9 | 37/37.9 | - Lcb. rhamnosus GG - B. animalis subsp. lactis Bb-12 | NS | From <16 wks until delivery, in women with pre-pregnancy BMI of >25 kg/m2 | Prevalence of childhood allergic diseases. | Infants do not appear to have any pediatric health advantages regarding allergic diseases. | |
Low risk; Moderate risk; High risk.| Authors, Year |
Study
Design | Cases (Probiotics/Placebo) | BMI | Age |
Probiotic
Intervention |
Dose
CFU/Day |
Intervention
Period | Outcomes | Results | Overall Bias Risk |
|---|---|---|---|---|---|---|---|---|---|---|
| Vähämiko [37], 2019 | D-B, P-CCT | 15 (7/8) | 21.7/24.5 | 29.5/28.6 | - Lcb. rhamnosus GG - B. lactis Bb-12 | 1 × 109, each | From early pregnancy (≤18 wks) and family history of allergic disease | DNA methylation status of the promoters of obesity and weight gain-related genes in mothers and their children. | Probiotics may affect the DNA methylation status of certain promoters of obesity and weight gain-related genes. | |
| Houttu [38], 2020 | D-B, P-CCT | 439 probiotics + placebo n = 110 | N/A | 30.6 | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010, each; plus 2 fish oil capsules | From early pregnancy (≤18 wks) until 6 m postnatally in women with pre-pregnancy BMI of >25 kg/m2 | Impact on serum/vaginal inflammatory and metabolic proteins and relation to the onset of GDM. | The intervention did not impact the proteins, but obesity and GDM may modify the effect. | |
| Mokkala [39], 2021 | D-B, P-CCT | 358 probiotics + placebo n = 91 | 28 | 31 | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010, each; plus 2 fish oil capsules | From the first visit (≤18 wks) until 6 m postnatally in women with pre-pregnancy BMI of >25 kg/m2 | Metabolic alterations in pregnant women with overweight or obesity. | In women with GDM, no effects on any metabolites. Fish oil and probiotics modified serum lipids (VLDL, LDL). | |
| Pellonperä [40], 2021 | P-CCT intervention pilot | 439 (211/204) | N/A | N/A | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010, each; plus 2 fish oil capsules | In late pregnancy >35 wks | Gestational weight gain and body composition. | Adiposity was reduced in women with GDM, irrespective of the dietary intervention. | |
| Hassain [41], 2022 | 12-wks, D-B, P-CCT, parallel-group | 132 (66/66) | N/A | N/A | - L. acidophilus - L. lactis - Lacticaseibacillus casei subsp. BCMC 12313 - B. bifidum - B. lactis NCIMB 30436 (formerly B. infantis) - B. lactis NCIMB 30435 | 3 × 1010, twice daily | 12 wks (at 4–8 wks postnatally in asymptomatic post-GDM women) | Metabolic and inflammatory effects. | Improved metabolic and inflammatory outcomes in post-GDM women by modulating gut dysbiosis. | |
| Saros [42], 2023 | D-B, P-CCT | 439 (211/204) | N/A | N/A | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010, each; plus 2 fish oil capsules | From early pregnancy (≤18 wks) until 6 m postpartum | The tendency of children <24 m to become overweight; change body fat percentage. | Probiotics, alone or in combination with fish oil, during pregnancy to overweight/obese women lowered overweight incidence. | |
| Halkjær [43], 2023 | D-B | 50 | N/A | N/A | Vivomixx—L. acidophilus, Lcb. paracasei, Lactiplantibacillus plantarum, L. helveticus NCIMB 30440, B. lactis NCIMB 30435, B. breve, B. lactis NCIMB 30436, S. thermophilus | 4.5 × 1011 | From 14–20 wks until delivery in women with pre-pregnancy BMI of >30 kg/m2 and <35 kg/m2 | The effect during pregnancy on the offspring’s metabolic and inflammatory markers and body composition. | No significant effect of supplementation in mothers or babies on metabolic or inflammatory biomarkers. | |
Low risk; Moderate risk; High risk.| Authors, Year | Study Design | Cases (Probiotics/Placebo) | BMI | Age | Probiotic Intervention | Dose CFU/Day | Intervention Period | Outcomes | Results | Overall Bias Risk |
| Luoto [44], 2010 | D-B, P-CCT | 159 (77/82) | N/A | N/A | - Lcb. rhamnosus GG | >1 × 1010 | 4 wks before expected delivery and postpartum for 6 m | Prevalence of GDM; the impact of perinatal intervention on childhood growth patterns; the development of overweight during a 10-yr follow-up. | ↓ Risk of GDM from 34% to 13% moderated the initial phase of excessive weight gain, with impact at 4 yrs. Early gut microbiota modulation may restrain excessive weight gain during the first years of life. | |
| Nitert [45], 2013 | Prospective, multicenter, D-B, controlled trial | 540 (270/270) | N/A | N/A | - Lcb. rhamnosus GG - B. animalis subsp. lactis Bb-12 | >1 × 109, each | From 16 wks until delivery, in women with BMI of >25 kg/m2 | Prevalence of GDM, weight gain, gut microbiome, macrosomia, infant body composition. | The efficacy of probiotic ingestion from early pregnancy to prevent GDM in overweight/obese women. | |
| Lindsay [46], 2014 | D-B, P-CCT | 138/63 (211/204) | 32.9/34.1 | 31.4/31 | - Lgb. salivarius UCC118 | 1 × 109 | 4 wks (at 24–28 wks in women with BMI 30–39.9 kg/m2) | Maternal FPG in obese pregnant women. | 4 wks of treatment did not influence maternal FPG, the metabolic profile, or pregnancy outcomes. | |
| Dolatkhah [47], 2015 | D-B, P-CCT | 64 (29/27) | 31.4/29.8 | 28.1/ 26.4 | - L. acidophilus LA-5 - L. helveticus NCIMB 30440 - B. lactis Bb-12 - Streptococcus thermophilus STY-31 | >4 × 109 | 8 wks (at 24−28 wks + 6 days, in women with GDM) | Glucose metabolism, weight gain among GDM patients. | ↓ FPG | |
| Lindsay [48], 2015 | D-B, P-CCT | 100 (48/52) | N/A | N/A | - Lgb. salivarius UCC118 | 1 × 109 | From diagnosis of GDM at <34 wks until delivery | FPG in GDM patients. | No impact on glycemic control or pregnancy outcome. | |
| Karamali [49], 2016 | Prospective, D-B, P-CCT | 60 (30/30) | N/A | N/A |
- L. acidophilus - Lbs. casei - B. bifidum | 2 × 109, each | 6 wks (at 24–28 wks, in women with GDM) | Glycemic control, lipid profiles in primigravida with GDM. | ↓ FPG, serum insulin, insulin resistance, triglycerides, and VLDL cholesterol. | |
| Jafarnejad [50], 2016 | Multicenter, prospective, D-B, P-CCT | 82 (41/41) | N/A | N/A | VSL#3—S. thermophilus, L. acidophilus, Lpb. plantarum, Lcb. paracasei, L. helveticus NCIMB 30440, B. breve, B. lactis NCIMB 30435, B. lactis NCIMB 30436 | 1.13 ×1011, twice daily | 8 wks (from the third trimester until delivery in women with GDM) | Glycemic control and inflammatory parameters. | There were no changes in FPG, Il-10, HbA1c, HOMA-IR, or insulin levels. ↓ IL-6, TNF-∝, and hs-CRP. Modulated inflammatory markers; benefits on glycemic control. | |
| Halkjaer [51], 2016 | D-B, P-CCT | 50 (25/25) | 22.7/22.0 | 32.5/30.7 | Vivomixx—L. acidophilus, Lpb. plantarum, Lcb. paracasei, L. helveticus NCIMB 30440, S. thermophilus, B. breve, B. lactis NCIMB 30435, B. lactis NCIMB 30436 | 1.12 × 1011/ capsule, 2 capsules twice daily | 18–24 wks (from 14–20 wks until delivery in women with BMI 30–35 kg/m2) | Maternal weight gain, glycated hemoglobin (HbA1c) levels, glucose homeostasis, pregnancy outcomes. | Control weight gain and reduce complications during pregnancy in obese patients. | |
| Wickens [52], 2017 | Two-centre, D-B, P-CCT, parallel | 423 (212/211) | 25/26 | 34 | - Lcb. rhamnosus HN001 | 6 × 109 | > 22 wks (from 14–16 wks, until 6 m postnatally if women still breastfeeding) | Prevalence of GDM. | ↓ GDM prevalence, particularly among older patients and those with previous GDM. | |
| Hajifaraji [53], 2018 | D-B, P-CCT | 64 | N/A | N/A | - L. acidophilus LA-5 - L. helveticus NCIMB 30440 - B. Bb-12 - S. thermophilus STY-31 | > 4 × 109 | 8 wks (at 24–28 wk + 6 days, in women with GDM) | Inflammation and oxidative stress biomarkers in newly diagnosed GDM women. | It appears to improve several inflammation and oxidative stress biomarkers in women with GDM. | |
| Pellonperä [54], 2019 | D-B, P-CCT | 439 (27/22) | 29.3/30.0 | 30.8/30.4 | - Lcb. rhamnosus HN001 - B. animalis subsp. lactis 420 | 1 × 1010 | From the first obstetrical visit (<18 wks mean 13.9 ± 2.1 wks) until 6 m postnatally | The incidence of GDM and change in FPG. | No change in FPG, insulin resistance HOMA2-IR index, neonatal birth weight, or maternal weight gain. No benefits in reducing the risk of GDM or improving glucose metabolism in overweight/obese women. | |
| Sahhaf Ebrahimi [55], 2019 | D-B, P-CCT | 84 (42/42) | 30.7 | 31.6 |
-
L. acidophilus - B. lactis | 300 mg/probiotic yoghurt (1 × 106) | 8 wks | Glycemic control, neonatal outcomes in women with GDM. | ↓ FPG, HbA1c, and incidence of macrosomia | |
| Callaway [56], 2019 | D-B, controlled trial | 411 (207/204) | 31.6/31.9 | 31.3/31.7 | - Lcb. rhamnosus GG - B. animalis subsp. lactis Bb-12 | 1 × 109, each | From <20 wks until delivery, in women with BMI > 25 kg/m2 | GDM prevention—in overweight/obese pregnant women in T2. | No benefit in GDM prevention. ↓ Excessive weight gain and SGA; no differences in other secondary outcomes. | |
| Kijmanawat [57], 2019 | D-B, P-CCT | 57 (28/29) | N/A | N/A |
-
L. acidophilus - B. bifidum | 1 × 109, each | 4 wks (24–28 wks in diet controlled GDM women) | Glycemic control in women with GDM. | ↓ FPG and serum insulin levels. ↑ Insulin sensitivity. | |
| Jamilian [58], 2019 | D-B, P-CCT | 87 (29/28, Vit. D + probiotic n = 30) | 27/28.2 | 31.2/29.9 | - L. acidophilus - Lmb. reuteri - Limosilactobacillus fermentum (formerly Lactobacillus fermentum) - B. bifidum | 2 × 109, each plus Vit. D 50,000 IU/every 2 wks | 4 wks (at 24–28 wks, in women with GDM, aged 18–40 yrs) | Metabolic status and pregnancy outcomes in women with GDM. | ↓ FPG, serum insulin, triglycerides, HDL/total cholesterol ratio, hs-CRP, malondialdehyde. ↑ Insulin sensitivity check index, HDL-cholesterol, TAC. | |
| Babadi [59], 2019 | D-B, P-CCT | 48 (24/24) | 26.9/27.3 | 28.8/29.0 |
- L. acidophilus - Lbs.casei - Lmb. fermentum - B. bifidum | 2 × 109, each | 6 wks (at 24–28 wks in women with GDM) | Gene expression related to insulin and inflammation, glycemic control, lipid profiles, inflammatory markers, and oxidative stress. | Upregulated PPAR-γ, TGF-β, VEGF; downregulated gene expression of TNF-∝. ↓ FPG, serum insulin levels, insulin resistance, VLDL- cholesterol, triglycerides, total/HDL-cholesterol ratio, malondialdehyde. ↑ Insulin sensitivity, HDL-cholesterol, nitric oxide, TAC. | |
| Asgharian [60], 2020 | D-B, P-CCT | 65 (211/204) | 40/42 | 29.5/29.4 | - S. thermophilus - L. helveticus NCIMB 30440 - L. acidophilus La5 - B. lactis Bb-12 | 1 × 107, 1 × 107 5 × 108 5 × 108 | From 22–24 wks until delivery. At 24 wks extra probiotics (L. acidophilus La5, B. lactis Bb12) | Maternal plasma glucose, maternal and infant complications in overweight/obese women with no GDM. | Probiotic supplementation has some beneficial effects on glucose metabolism of overweight/obese pregnant women. | |
| Shahriari [61], 2021 | Single-center, D-B, P-CCT | 542 (271/271) | 30.2/30.2 | 31.8/32.2 | - L. acidophilus LA1 - B. longum sp54 - B. bifidum sp9 | >7.5 × 109 >1.5 × 109 >6 × 109 | >26 wks (<12 wks, singleton) | Risk of GDM and maternal/neonatal outcomes | Probiotic supplementation from the first half of the T2 does not reduce the risk of GDM. | |
| Chen [62], 2021 | D-B, P-CCT | 348 (172/176) | 25.1/25.8 | 33.1/33.8 | - Lcb. rhamnosus HN001 | 6 × 109 | From 14–16 wks until delivery | Effects on fasting lipids, insulin resistance, and bile acids (BA). | ↓ Conjugated BA, which has a possible role in improving glucose metabolism; has no significant effect on fasting lipids. | |
| Amirani [63], 2022 | D-B, P-CCT | 60 (30/30) | N/A | N/A | - L. acidophilus - B. bifidum - B. lactis - B. lactis NCIMB 30435 plus selenium | 2 × 109, each plus 200 μg/day selenium | 6 wks in women diagnosed with GDM | Effects on glycemic status, insulin metabolism, lipid profiles, PPAR-γ, and LDL receptor expression. | ↓ FPG, insulin levels, insulin resistance, triglycerides, total/LDL-cholesterol. ↑ Insulin sensitivity, gene expression of PPAR-γ/LDLR. | |
| Nachum [64], 2024 | Multicenter, prospective, D-B, P-CCT | 85 (41/44) | N/A | N/A | - Lcb. rhamnosus - L. acidophilus - Lcb. paracasei - B. bifidum - B. lactis - S. thermophilus | >6 × 109/ capsule, 2 capsules/day | From the time of diagnosis of GDM until delivery | Maternal glycemic parameters and pregnancy outcomes. | Did not affect the glycemic control of women with GDM. | |
Low risk; High risk.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varlas, V.N.; Bohîlțea, L.-C.; Suciu, N. The Influences of Oral Probiotics on the Immunometabolic Response During Pregnancy and Lactation: A Systematic Review. Nutrients 2025, 17, 1535. https://doi.org/10.3390/nu17091535
Varlas VN, Bohîlțea L-C, Suciu N. The Influences of Oral Probiotics on the Immunometabolic Response During Pregnancy and Lactation: A Systematic Review. Nutrients. 2025; 17(9):1535. https://doi.org/10.3390/nu17091535
Chicago/Turabian StyleVarlas, Valentin Nicolae, Laurențiu-Camil Bohîlțea, and Nicolae Suciu. 2025. "The Influences of Oral Probiotics on the Immunometabolic Response During Pregnancy and Lactation: A Systematic Review" Nutrients 17, no. 9: 1535. https://doi.org/10.3390/nu17091535
APA StyleVarlas, V. N., Bohîlțea, L.-C., & Suciu, N. (2025). The Influences of Oral Probiotics on the Immunometabolic Response During Pregnancy and Lactation: A Systematic Review. Nutrients, 17(9), 1535. https://doi.org/10.3390/nu17091535