


Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study

 , ,
, ,
Abstract

1. Introduction
2. Methods
2.1. Study Design
2.2. Study Cohorts
2.3. Data Analysis
3. Results
3.1. Geographic Distribution of Patients
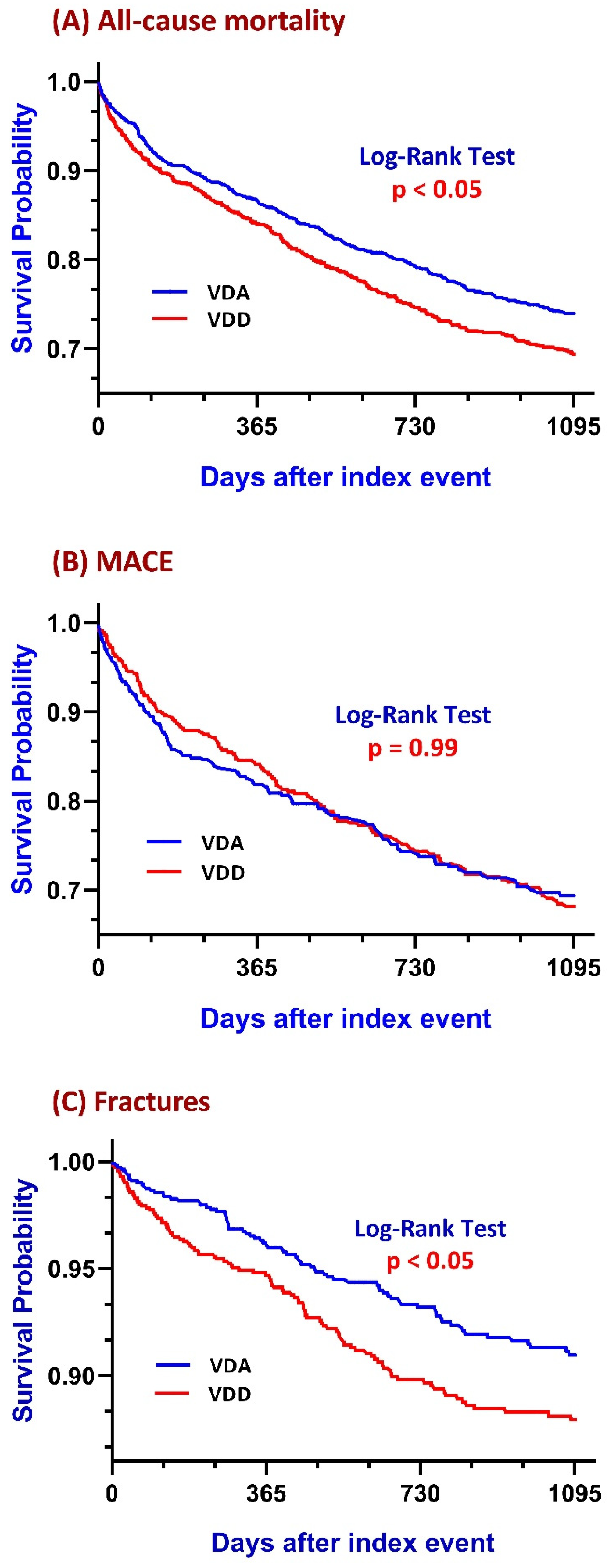
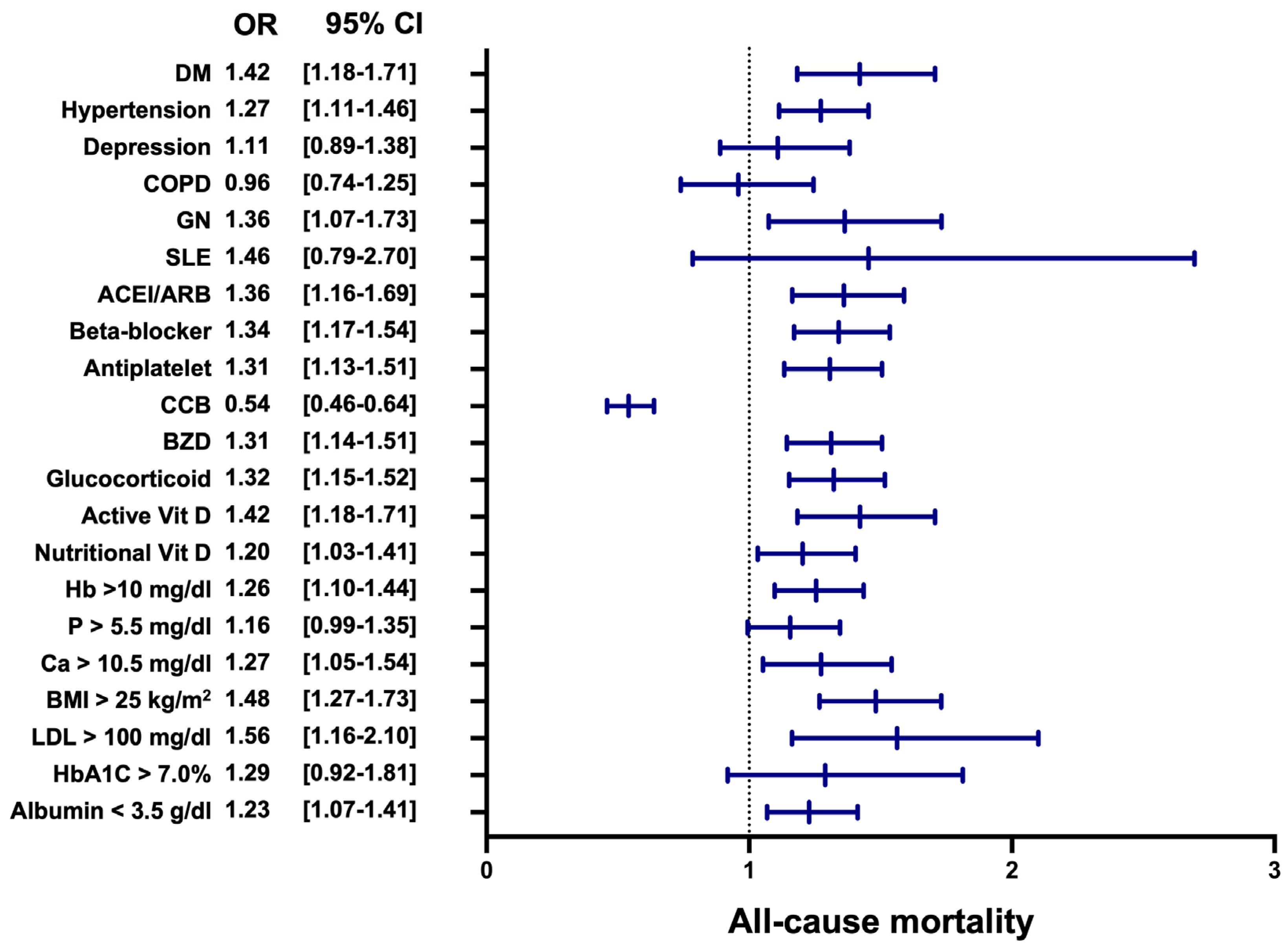
3.2. All-Cause Mortality
3.3. Major Adverse Cardiovascular Events
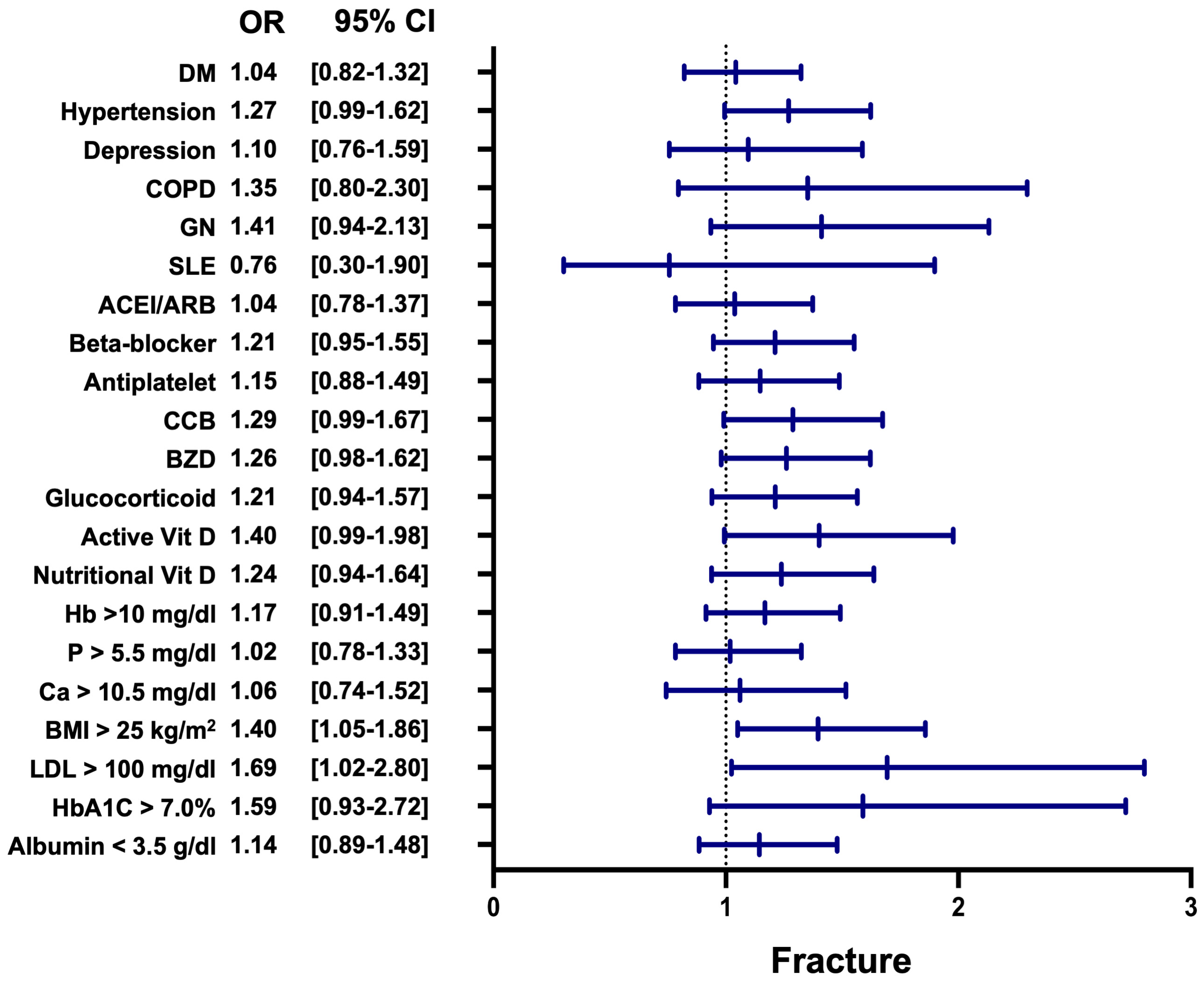
3.4. Fracture
3.5. Incidence of Hypocalcemia (Ca ≤ 8.5 mg/dL)
3.6. Proportion of Cases with Intact Parathyroid Hormone (PTH ≤ 300 pg/mL) Following Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Full Form |
| ACEI | angiotensin-converting enzyme inhibitor |
| ARB | angiotensin II receptor blocker |
| CaSRs | calcium-sensing receptors |
| CKD | chronic kidney disease |
| DM | diabetes mellitus |
| MACEs | major adverse cardiovascular events |
| PTH | parathyroid hormone |
| SHPT | secondary hyperparathyroidism |
| VDD | vitamin D deficiency |
| VDA | vitamin D adequate |
References
- Foley, R.N.; Parfrey, P.; Sarnak, M. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Clemens, T.L.; Cormier, S.; Eichinger, A.; Endlich, K.; Fiaschi-Taesch, N.; Fischer, E.; Friedman, P.A.; Karaplis, A.C.; Massfelder, T.; Rossert, J.; et al. Parathyroid hormone-related protein and its receptors: Nuclear functions and roles in the renal and cardiovascular systems, the placental trophoblasts and the pancreatic islets. Br. J. Pharmacol. 2001, 134, 1113–1136. [Google Scholar] [CrossRef] [PubMed]
- Block, G.A.; Klassen, P.S.; Lazarus, J.M.; Ofsthun, N.; Lowrie, E.G.; Chertow, G.M. Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J. Am. Soc. Nephrol. 2004, 15, 2208–2218. [Google Scholar] [CrossRef]
- Hagström, E.; Hellman, P.; Larsson, T.E.; Ingelsson, E.; Berglund, L.; Sundström, J.; Melhus, H.; Held, C.; Lind, L.; Michaëlsson, K.; et al. Plasma Parathyroid Hormone and the Risk of Cardiovascular Mortality in the Community. Circulation 2009, 119, 2765–2771. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Block, G.A.; Correa-Rotter, R.; Drüeke, T.B.; Floege, J.; Goodman, W.G.; Parfrey, P.S. Cinacalcet for Cardiovascular Disease in Patients Undergoing Dialysis. N. Engl. J. Med. 2012, 367, 2482–2494. [Google Scholar]
- Lozano-Ortega, G.; Waser, N.; E Bensink, M.; Goring, S.; Bennett, H.; A Block, G.; Chertow, G.M.; Trotman, M.-L.; Cooper, K.; Levy, A.R.; et al. Effects of calcimimetics on long-term outcomes in dialysis patients: Literature review and Bayesian meta-analysis. J. Comp. Eff. Res. 2018, 7, 693–707. [Google Scholar] [CrossRef]
- Zu, Y.; Lu, X.; Song, J.; Yu, L.; Li, H.; Wang, S. Cinacalcet Treatment Significantly Improves All-Cause and Cardiovascular Survival in Dialysis Patients: Results from a Meta-Analysis. Kidney Blood Press. Res. 2019, 44, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; Mavridis, D.; Johnson, D.W.; Tonelli, M.; Ruospo, M.; Strippoli, G.F. Comparative Effectiveness of Calcimimetic Agents for Secondary Hyperparathyroidism in Adults: A Systematic Review and Network Meta-analysis. Am. J. Kidney Dis. 2020, 76, 321–330. [Google Scholar] [CrossRef]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Vitamin D in Chronic Kidney Disease and Dialysis Patients. Nutrients 2017, 9, 328. [Google Scholar] [CrossRef]
- Li, L.; Zhao, J. Association of serum 25-hydroxyvitamin D with cardiovascular and all-cause mortality in patients with chronic kidney disease: NHANES 2007–2018 results. Clinics 2024, 79, 100437. [Google Scholar] [CrossRef]
- Palchuk, M.B.; London, J.W.; Perez-Rey, D.; Drebert, Z.J.; Winer-Jones, J.P.; Thompson, C.N.; Esposito, J.; Claerhout, B. A global federated real-world data and analytics platform for research. JAMIA Open 2023, 6, ooad035. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.J.; Huff, S.M.; Suico, J.G.; Hill, G.; Leavelle, D.; Aller, R.; Forrey, A.; Mercer, K.; DeMoor, G.; Hook, J.; et al. LOINC, a Universal Standard for Identifying Laboratory Observations: A 5-Year Update. Clin. Chem. 2003, 49, 624–633. [Google Scholar] [CrossRef]
- Giacalone, M.; Agata, Z.; Cozzucoli, P.C.; Alibrandi, A. Bonferroni-Holm and permutation tests to compare health data: Methodological and applicative issues. BMC Med. Res. Methodol. 2018, 18, 81. [Google Scholar] [CrossRef]
- Wolf, M.; Shah, A.; Gutierrez, O.; Ankers, E.; Monroy, M.; Tamez, H.; Steele, D.; Chang, Y.; Camargo, C.; Tonelli, M.; et al. Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int. 2007, 72, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Chertow, G.M.; Johansen, K.L.; Grimes, B.; Dalrymple, L.S.; Kaysen, G.A.; Tamura, M.K. Vitamin D Deficiency and Mortality in Patients Receiving Dialysis: The Comprehensive Dialysis Study. J. Ren. Nutr. 2013, 23, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Yin, K.; Agrawal, D.K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar]
- Leopold, J.A. Vascular calcification: Mechanisms of vascular smooth muscle cell calcification. Trends Cardiovasc. Med. 2015, 25, 267–274. [Google Scholar] [CrossRef]
- Khundmiri, S.J.; Murray, R.D.; Lederer, E. PTH and Vitamin D. Compr. Physiol. 2016, 6, 561–601. [Google Scholar] [CrossRef]
- Kota, S.K.; Kota, S.K.; Jammula, S.; Meher, L.K.; Panda, S.; Tripathy, P.R.; Modi, K.D. Renin-angiotensin system activity in vitamin D deficient, obese individuals with hypertension: An urban Indian study. Indian J. Endocrinol. Metab. 2011, 15 (Suppl. S4), S395–S401. [Google Scholar] [CrossRef]
- Löffler, F.; Garlichs, J.C.; Uehlein, S.; Löffler, L.; Leitolf, H.; Terkamp, C.; Bauersachs, J.; Westhoff-Bleck, M. Vitamin D deficiency and secondary hyperparathyroidism in adult Fontan patients. Int. J. Cardiol. Congenit. Heart Dis. 2024, 17, 100521. [Google Scholar] [CrossRef]
- Babeș, E.E.; Lucuța, D.A.; Petcheși, C.D.; Zaha, A.A.; Ilyes, C.; Jurca, A.D.; Vesa, C.M.; Zaha, D.C.; Babeș, V.V. Clinical Features and Outcome of Infective Endocarditis in a University Hospital in Romania. Medicina 2021, 57, 158. [Google Scholar] [CrossRef] [PubMed]
- Galușca, D.; Popoviciu, M.S.; Babeș, E.E.; Vidican, M.; Zaha, A.A.; Babeș, V.V.; Jurca, A.D.; Zaha, D.C.; Bodog, F. Vitamin D Implications and Effect of Supplementation in Endocrine Disorders: Autoimmune Thyroid Disorders (Hashimoto’s Disease and Grave’s Disease), Diabetes Mellitus and Obesity. Medicina 2022, 58, 194. [Google Scholar] [CrossRef] [PubMed]
- Hewison, M. Vitamin D and Innate and Adaptive Immunity. Vitam. Horm. 2011, 86, 23–62. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Meza, C.A.; Clarke, H.; Kim, J.-S.; Hickner, R.C. Vitamin D and Endothelial Function. Nutrients 2020, 12, 575. [Google Scholar] [CrossRef]
- Shimizu, T.; Tanaka, T.; Iso, T.; Kawai-Kowase, K.; Kurabayashi, M. Azelnidipine Inhibits Msx2-Dependent Osteogenic Differentiation and Matrix Mineralization of Vascular Smooth Muscle Cells. Int. Heart J. 2012, 53, 331–335. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Ikizler, T.; Block, G.; Avram, M.M.; Kopple, J.D. Malnutrition-inflammation complex syndrome in dialysis patients: Causes and consequences. Am. J. Kidney Dis. 2003, 42, 864–881. [Google Scholar] [CrossRef]
- Wu, X.; Zhou, L.; Zhan, X.; Wen, Y.; Wang, X.; Feng, X.; Wang, N.; Peng, F.; Wu, J. Low-Density Lipoprotein Cholesterol and Mortality in Peritoneal Dialysis. Front. Nutr. 2022, 9, 910348. [Google Scholar] [CrossRef]
- Drechsler, C.; Verduijn, M.; Pilz, S.; Dekker, F.W.; Krediet, R.T.; Ritz, E.; Wanner, C.; Boeschoten, E.W.; Brandenburg, V. For the NECOSAD Study Group Vitamin D status and clinical outcomes in incident dialysis patients: Results from the NECOSAD study. Nephrol. Dial. Transplant. 2010, 26, 1024–1032. [Google Scholar] [CrossRef]
- Krause, R.; Schober-Halstenberg, H.-J.; Edenharter, G.; Haas, K.; Roth, H.J.; Frei, U. Vitamin D status and mortality of German hemodialysis patients. Anticancer. Res. 2012, 32, 391–395. [Google Scholar]
- Zhang, Y.; Darssan, D.; Pascoe, E.M.; Johnson, D.W.; Pi, H.; Dong, J. Vitamin D status and mortality risk among patients on dialysis: A systematic review and meta-analysis of observational studies. Nephrol. Dial. Transplant. 2018, 33, 1742–1751. [Google Scholar] [CrossRef]
- Grant, W.B.; Boucher, B.J. How Follow-Up Period in Prospective Cohort Studies Affects Relationship Between Baseline Serum 25(OH)D Concentration and Risk of Stroke and Major Cardiovascular Events. Nutrients 2024, 16, 3759. [Google Scholar] [CrossRef] [PubMed]
- Marti-Soler, H.; Gonseth, S.; Gubelmann, C.; Stringhini, S.; Bovet, P.; Chen, P.-C.; Wojtyniak, B.; Paccaud, F.; Tsai, D.-H.; Zdrojewski, T.; et al. Seasonal Variation of Overall and Cardiovascular Mortality: A Study in 19 Countries from Different Geographic Locations. PLoS ONE 2014, 9, e113500. [Google Scholar] [CrossRef]
- Kop, W.J.; Stein, P.K.; Tracy, R.P.; Barzilay, J.I.; Schulz, R.; Gottdiener, J.S. Autonomic Nervous System Dysfunction and Inflammation Contribute to the Increased Cardiovascular Mortality Risk Associated With Depression. Psychosom. Med. 2010, 72, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef] [PubMed]
- Anders, H.-J.; Kitching, A.R.; Leung, N.; Romagnani, P. Glomerulonephritis: Immunopathogenesis and immunotherapy. Nat. Rev. Immunol. 2023, 23, 453–471. [Google Scholar] [CrossRef]
- Mahmoodi, B.K.; ten Kate, M.K.; Waanders, F.; Veeger, N.J.G.M.; Brouwer, J.-L.P.B.; Vogt, L.; Navis, J.; van der Meer, J. High Absolute Risks and Predictors of Venous and Arterial Thromboembolic Events in Patients With Nephrotic Syndrome: Results from a Large Retrospective Cohort Study. J. Vasc. Surg. 2008, 48, 1633. [Google Scholar] [CrossRef]
- Matsushita, K.; Van Der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; De Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef]
- Neves, K.-R.; Graciolli, F.-G.; dos Reis, L.-M.; Graciolli, R.-G.; Neves, C.-L.; Magalhães, A.-O.; Custódio, M.-R.; Batista, D.-G.; Jorgetti, V.; Moysés, R. Vascular calcification: Contribution of parathyroid hormone in renal failure. Kidney Int. 2007, 71, 1262–1270. [Google Scholar] [CrossRef]
- Wu, M.; Tang, R.-N.; Liu, H.; Pan, M.-M.; Liu, B.-C. Cinacalcet ameliorates aortic calcification in uremic rats via suppression of endothelial-to-mesenchymal transition. Acta Pharmacol. Sin. 2016, 37, 1423–1431. [Google Scholar] [CrossRef]
- Raggi, P.; Chertow, G.M.; Torres, P.U.; Csiky, B.; Naso, A.; Nossuli, K.; Moustafa, M.; Goodman, W.G.; Lopez, N.; Downey, G.; et al. The ADVANCE study: A randomized study to evaluate the effects of cinacalcet plus low-dose vitamin D on vascular calcification in patients on hemodialysis. Nephrol. Dial. Transplant. 2010, 26, 1327–1339. [Google Scholar] [CrossRef]
- Wang, T.; He, C. Pro-inflammatory cytokines: The link between obesity and osteoarthritis. Cytokine Growth Factor Rev. 2018, 44, 38–50. [Google Scholar] [CrossRef]
- Pogoda, P.; Egermann, M.; Schnell, J.C.; Priemel, M.; Schilling, A.F.; Alini, M.; Schinke, T.; Rueger, J.M.; Schneider, E.; Clarke, I.; et al. Leptin Inhibits Bone Formation Not Only in Rodents, but Also in Sheep. J. Bone Miner. Res. 2006, 21, 1591–1599. [Google Scholar] [CrossRef] [PubMed]
- Benova, A.; Tencerova, M. Obesity-Induced Changes in Bone Marrow Homeostasis. Front. Endocrinol. 2020, 11, 294. [Google Scholar] [CrossRef]
- Mazière, C.; Savitsky, V.; Galmiche, A.; Gomila, C.; Massy, Z.; Mazière, J.-C. Oxidized low density lipoprotein inhibits phosphate signaling and phosphate-induced mineralization in osteoblasts. Involvement of oxidative stress. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2010, 1802, 1013–1019. [Google Scholar] [CrossRef]
- Manolagas, S.C. From Estrogen-Centric to Aging and Oxidative Stress: A Revised Perspective of the Pathogenesis of Osteoporosis. Endocr. Rev. 2010, 31, 266–300. [Google Scholar] [CrossRef] [PubMed]
- Wauquier, F.; Leotoing, L.; Coxam, V.; Guicheux, J.; Wittrant, Y. Oxidative stress in bone remodelling and disease. Trends Mol. Med. 2009, 15, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.; Uday, S. Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention. Nutrients 2023, 15, 2805. [Google Scholar] [CrossRef]
- Clarke, R.; Shipley, M.; Lewington, S.; Youngman, L.; Collins, R.; Marmot, M.; Peto, R. Underestimation of Risk Associations Due to Regression Dilution in Long-term Follow-up of Prospective Studies. Am. J. Epidemiol. 1999, 150, 341–353. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| VDD (n = 2714) | VDA (n = 2410) | Std. Diff. | VDD (n = 1744) | VDA (n = 1744) | Std. Diff. | |
| Demographics | ||||||
| Age at index date (mean ± SD) | 54.7 +/− 14.1 | 60.0 +/− 14.3 | 0.37 | 57.2 +/− 13.4 | 57.3 +/− 14.3 | 0.01 |
| Male, (%) | 48.9% | 50.5% | 0.03 | 50.2% | 50.8% | 0.01 |
| White, (%) | 29.8% | 42.5% | 0.27 | 36.1% | 37.1% | 0.02 |
| Black or African American, (%) | 45.5% | 34.2% | 0.23 | 40.1% | 39.6% | 0.01 |
| Comorbidities (%) | ||||||
| Hypertension | 69.6% | 71.4% | 0.04 | 71.7% | 71.3% | 0.01 |
| Diabetes mellitus | 38.8% | 40.6% | 0.04 | 40.7% | 40.5% | <0.01 |
| Depressive episode | 11.3% | 9.5% | 0.06 | 10.7% | 10.6% | <0.01 |
| Chronic obstructive pulmonary disease | 6.5% | 7.1% | 0.02 | 7.3% | 7.2% | <0.01 |
| Glomerular diseases | 6.5% | 5.1% | 0.06 | 5.4% | 5.9% | 0.02 |
| Systemic lupus erythematosus | 3.0% | 2.7% | 0.02 | 3.1% | 3.2% | <0.01 |
| Medications (%) | ||||||
| ACEI | 14.1% | 11.2% | 0.09 | 12.4% | 11.8% | 0.02 |
| ARB | 10.9% | 12.1% | 0.04 | 11.7% | 11.1% | 0.02 |
| Beta-blockers | 56.7% | 47.5% | 0.19 | 50.1% | 51.5% | 0.03 |
| CCB | 42.5% | 35.6% | 0.14 | 39.4% | 38.3% | 0.02 |
| Diuretics | 9.1% | 7.9% | 0.04 | 8.7% | 8.6% | <0.01 |
| Vitamin D | 29.4% | 31.7% | 0.05 | 30.3% | 30.0% | <0.01 |
| Insulin | 40.6% | 31.6% | 0.19 | 35.7% | 35.3% | <0.01 |
| Cholecalciferol | 11.6% | 17.3% | 0.16 | 14.7% | 14.5% | <0.01 |
| Doxercalciferol | 2.1% | 1.1% | 0.08 | 1.5% | 1.3% | 0.02 |
| Ergocalciferol | 7.1% | 8.5% | 0.05 | 7.3% | 8.1% | 0.03 |
| Calcitriol | 11.2% | 9.2% | 0.07 | 10.3% | 10.0% | 0.01 |
| Paricalcitol | 4.5% | 2.4% | 0.12 | 3.3% | 3.1% | 0.01 |
| Glucocorticoids | 47.2% | 40.8% | 0.13 | 44.3% | 42.8% | 0.03 |
| Laboratory, Mean ± SD | ||||||
| Intact parathyroid hormone, pg/mL | 567.3 +/− 668.5 | 384.2 +/− 443.6 | 0.32 | 508.9 +/− 587.5 | 404.0 +/− 466.7 | 0.20 |
| Calcidiol, ng/mL | 12.2 +/− 4.4 | 45.3 +/− 14.2 | 3.15 | 12.6 +/− 4.3 | 44.7 +/− 14.3 | 3.04 |
| Sodium, mmol/L | 137.0 +/− 4.5 | 137.5 +/− 3.9 | 0.13 | 137.0 +/− 4.4 | 137.4 +/− 3.9 | 0.09 |
| Potassium, mmol/L | 4.4 +/− 0.7 | 4.4 +/− 0.7 | 0.01 | 4.4 +/− 0.7 | 4.5 +/− 0.7 | 0.07 |
| Calcium, mg/dL | 9.3 +/− 1.3 | 9.5 +/− 1.2 | 0.17 | 9.3 +/− 1.3 | 9.5 +/− 1.2 | 0.09 |
| Phosphate, mg/dL | 4.6 +/− 2.2 | 4.2 +/− 1.8 | 0.21 | 4.5 +/− 2.1 | 4.3 +/− 1.9 | 0.12 |
| HbA1c, % | 6.4 +/− 1.9 | 6.2 +/− 1.5 | 0.11 | 6.4 +/− 2.0 | 6.1 +/− 1.6 | 0.13 |
| Albumin, g/dL | 3.5 +/− 0.8 | 3.7 +/− 0.7 | 0.28 | 3.5 +/− 0.7 | 3.6 +/− 0.7 | 0.25 |
| LDL, mg/dL | 77.2 +/− 39.7 | 74.2 +/− 35.4 | 0.08 | 76.3 +/− 41.2 | 74.9 +/− 36.8 | 0.04 |
| Hemoglobin, g/dL | 10.2 +/− 2.2 | 10.8 +/− 2.2 | 0.24 | 10.4 +/− 2.2 | 10.7 +/− 2.2 | 0.13 |
| BMI, kg/m2 | 29.2 +/− 7.8 | 28.7 +/− 7.2 | 0.07 | 29.3 +/− 7.7 | 28.8 +/− 7.3 | 0.07 |
| Region | Number of Patients in VDD Group |
|---|---|
| United States (US Network) | 2192 patients |
| Europe and Middle East (EMEA Network) | 106 patients |
| Asia–Pacific (APAC Network) | 0 patients |
| Latin America (LATAM Network) | 0 patients |
| Global Total | 2298 patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, K.-C.; Wang, J.; Zheng, C.-M.; Tsai, K.-W.; Hou, Y.-C.; Lu, C.-L. Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study. Nutrients 2025, 17, 1536. https://doi.org/10.3390/nu17091536
Lu K-C, Wang J, Zheng C-M, Tsai K-W, Hou Y-C, Lu C-L. Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study. Nutrients. 2025; 17(9):1536. https://doi.org/10.3390/nu17091536
Chicago/Turabian StyleLu, Kuo-Cheng, Joshua Wang, Cai-Mei Zheng, Kuo-Wang Tsai, Yi-Chou Hou, and Chien-Lin Lu. 2025. "Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study" Nutrients 17, no. 9: 1536. https://doi.org/10.3390/nu17091536
APA StyleLu, K.-C., Wang, J., Zheng, C.-M., Tsai, K.-W., Hou, Y.-C., & Lu, C.-L. (2025). Vitamin D Deficiency and the Clinical Outcomes of Calcimimetic Therapy in Dialysis Patients: A Population-Based Study. Nutrients, 17(9), 1536. https://doi.org/10.3390/nu17091536