
Connecting Diagnostics and Clinical Relevance of the α-Gal Syndrome—Individual Sensitization Patterns of Patients with Suspected α-Gal-Associated Allergy


Abstract

1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Detection of Allergen-Specific IgE Antibodies by ImmunoCAP
2.3. In Vitro Cross-Reactivity Analysis of sIgE Against Different α-Gal-Containing Proteins by sIgE Cross-Reactivity Immune Profiling (ICRIP)
3. Results
3.1. Demographic and Clinical Characteristics of Patients with Suspected AGS
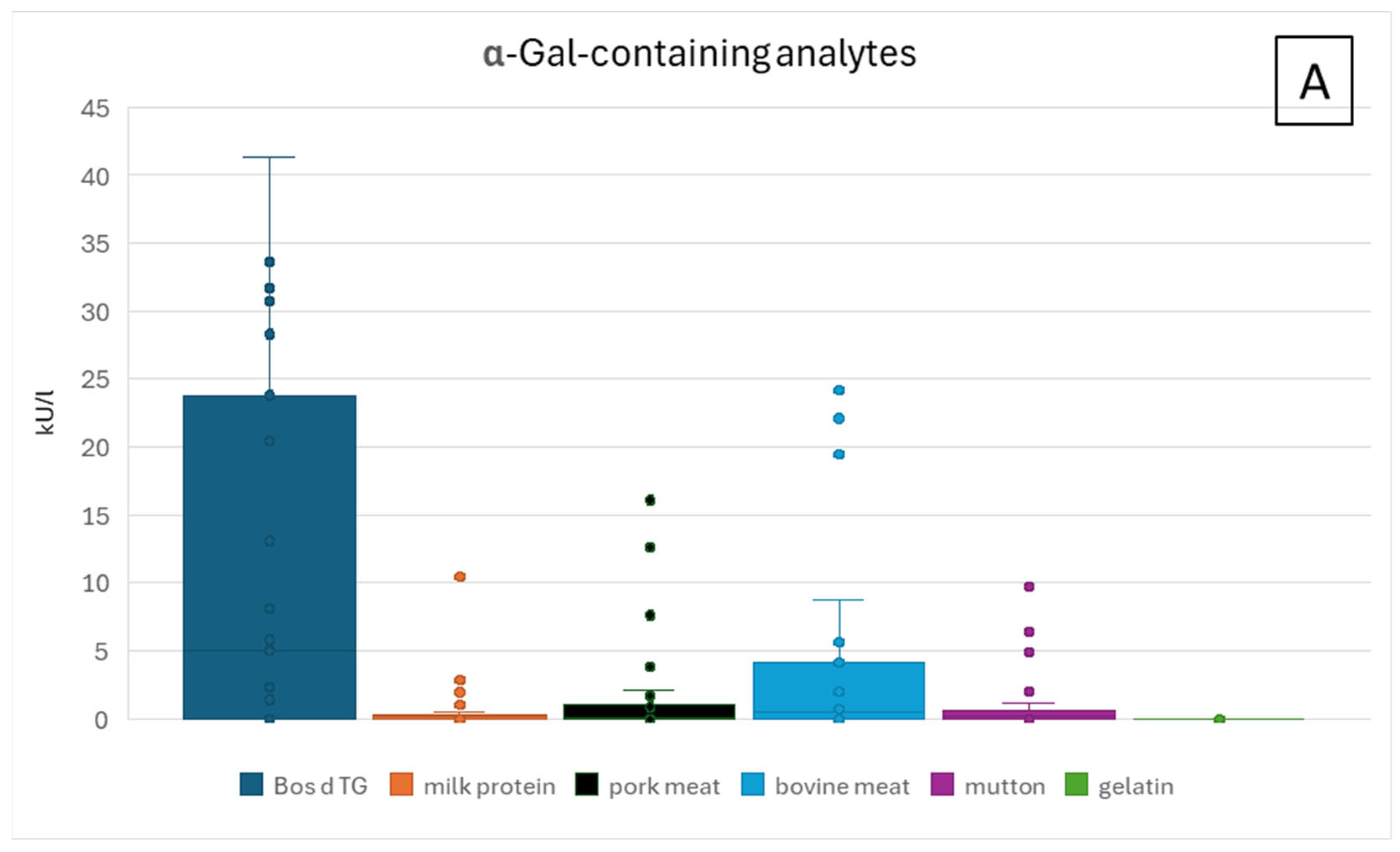
3.1.1. ImmunoCAP Analysis of Patient Sera
3.1.2. ImmunoCAP Analysis of Patient Sera Positive for sIgE Against Bos d TG
3.1.3. ImmunoCAP Analysis of Patient Sera Negative for sIgE Against Bos d TG
3.1.4. Patient Sera IgE Analysis by sIgE-Cross-Reactivity-Immune Profiling (ICRIP)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AD | atopic dermatitis |
| AGS | α-Gal-syndrome |
| α-Gal | galactose-(α-1,3)-galactose |
| Bos d TG | bovine thyroglobulin |
| BSA | bovine serum albumin |
| CCD | cross-reactive carbohydrate determinants |
| CTX | cetuximab |
| EoE | eosinophilic esophagitis |
| GI | gastrointestinal |
| HDM | house dust mite |
| HSA | human serum albumin |
| ICRIP | IgE-cross-reactivity immune profiling |
| IFX | infliximab |
| Ig | immunoglobulin |
| n.a. | not applicable |
| n.d. | not determined |
| OC | oral challenge |
| OAS | oral allergy syndrome |
| SPT | skin prick test |
References
- Hilger, C.; Kohnen, M.; Grigioni, F.; Lehners, C.; Hentges, F. Allergic Cross-reactions between Cat and Pig Serum Albumin: Study at the Protein and DNA Levels. Allergy 1997, 52, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.H.; Mirakhur, B.; Chan, E.; Le, Q.-T.; Berlin, J.; Morse, M.; Murphy, B.A.; Satinover, S.M.; Hosen, J.; Mauro, D.; et al. Cetuximab-Induced Anaphylaxis and IgE Specific for Galactose-α-1,3-Galactose. N. Engl. J. Med. 2008, 358, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Erickson, L.; Levin, M.; Ailsworth, S.M.; Commins, S.P.; Platts-Mills, T.A.E. Tick Bites, IgE to Galactose-alpha-1,3-galactose and Urticarial or Anaphylactic Reactions to Mammalian Meat: The Alpha-gal Syndrome. Allergy 2024, 79, 1440–1454. [Google Scholar] [CrossRef] [PubMed]
- Chitnavis, M.; Stein, D.J.; Commins, S.; Schuyler, A.J.; Behm, B. First-Dose Anaphylaxis to Infliximab: A Case of Mammalian Meat Allergy. J. Allergy Clin. Immunol. Pract. 2017, 5, 1425–1426. [Google Scholar] [CrossRef]
- Corominas, M.; Gastaminza, G.; Lobera, T. Hypersensitivity Reactions to Biological Drugs. J. Investig. Allergol. Clin. Immunol. 2014, 24, 212–225, quiz 1p following 225. [Google Scholar]
- Mullins, R.J.; James, H.; Platts-Mills, T.A.E.; Commins, S. Relationship between Red Meat Allergy and Sensitization to Gelatin and Galactose-α-1,3-Galactose. J. Allergy Clin. Immunol. 2012, 129, 1334–1342.e1. [Google Scholar] [CrossRef]
- Jappe, U.; Minge, S.; Kreft, B.; Ludwig, A.; Przybilla, B.; Walker, A.; Varga, R.; Seidel, P.; Biedermann, T.; Anemüller, W.; et al. Meat Allergy Associated with Galactosyl-α-(1,3)-galactose (α-Gal)—Closing Diagnostic Gaps by anti-α-Gal IgE Immune Profiling. Allergy 2018, 73, 93–105. [Google Scholar] [CrossRef]
- Apostolovic, D.; Tran, T.A.T.; Sánchez-Vidaurre, S.; Cirkovic Velickovic, T.; Starkhammar, M.; Hamsten, C.; van Hage, M. Red Meat Allergic Patients Have a Selective IgE Response to the α-Gal Glycan. Allergy 2015, 70, 1497–1500. [Google Scholar] [CrossRef]
- Commins, S.P.; Platts-Mills, T.A.E. Delayed Anaphylaxis to Red Meat in Patients with IgE Specific for Galactose Alpha-1,3-Galactose (Alpha-Gal). Curr. Allergy Asthma Rep. 2013, 13, 72–77. [Google Scholar] [CrossRef]
- Apostolovic, D.; Grundström, J.; Kiewiet, M.B.G.; Perusko, M.; Hamsten, C.; Starkhammar, M.; Paulie, S.; Van Hage, M. Th2-Skewed T Cells Correlate with B Cell Response to α-Gal and Tick Antigens in α-Gal Syndrome. J. Clin. Investig. 2023, 133, e158357. [Google Scholar] [CrossRef]
- Platts-Mills, T.A.; Hilger, C.; Jappe, U.; Van Hage, M.; Gadermaier, G.; Spillner, E.; Lidholm, J.; Keshavarz, B.; Aalberse, R.C.; Van Ree, R.; et al. Carbohydrate Epitopes Currently Recognized as Targets for IgE Antibodies. Allergy 2021, 76, 2383–2394. [Google Scholar] [CrossRef] [PubMed]
- Homann, A.; Schramm, G.; Jappe, U. Glycans and Glycan-Specific IgE in Clinical and Molecular Allergology: Sensitization, Diagnostics, and Clinical Symptoms. J. Allergy Clin. Immunol. 2017, 140, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Platts-Mills, T.A.E.; Li, R.; Keshavarz, B.; Smith, A.R.; Wilson, J.M. Diagnosis and Management of Patients with the α-Gal Syndrome. J. Allergy Clin. Immunol. Pract. 2020, 8, 15–23.e1. [Google Scholar] [CrossRef] [PubMed]
- Commins, S.P. Diagnosis & Management of Alpha-Gal Syndrome: Lessons from 2,500 Patients. Expert. Rev. Clin. Immunol. 2020, 16, 667–677. [Google Scholar] [CrossRef]
- Thompson, J.M.; Carpenter, A.; Kersh, G.J.; Wachs, T.; Commins, S.P.; Salzer, J.S. Geographic Distribution of Suspected Alpha-Gal Syndrome Cases—United States, January 2017–December 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 815–820. [Google Scholar] [CrossRef]
- Mollah, F.; Zacharek, M.A.; Benjamin, M.R. What Is Alpha-Gal Syndrome? JAMA 2024, 331, 86. [Google Scholar] [CrossRef]
- Ailsworth, S.M.; Susi, A.; Workman, L.J.; Ji, Y.-S.; Patel, J.; Nelson, M.R.; Platts-Mills, T.A.E.; Nylund, C.M.; Wilson, J.M. Alpha-Gal IgE Prevalence Patterns in the United States: An Investigation of 3,000 Military Recruits. J. Allergy Clin. Immunol. Pract. 2024, 12, 175–184.e5. [Google Scholar] [CrossRef]
- Fischer, J.; Huynh, H.-N.; Hebsaker, J.; Forchhammer, S.; Yazdi, A.S. Prevalence and Impact of Type I Sensitization to Alpha-Gal in Patients Consulting an Allergy Unit. Int. Arch. Allergy Immunol. 2020, 181, 119–127. [Google Scholar] [CrossRef]
- McGill, S.K.; Levin, M.E.; Shaheen, N.J.; Cotton, C.C.; Platts-Mills, T.A.; Commins, S.P. Gastrointestinal-Isolated Distress Is Common in Alpha-Gal Allergic Patients on Mammalian Meat Challenge. J. Clin. Gastroenterol. 2024, 58, 80–84. [Google Scholar] [CrossRef]
- Wilson, J.M.; Nguyen, A.T.; Schuyler, A.J.; Commins, S.P.; Taylor, A.M.; Platts-Mills, T.A.E.; McNamara, C.A. IgE to the Mammalian Oligosaccharide Galactose-α-1,3-Galactose Is Associated with Increased Atheroma Volume and Plaques with Unstable Characteristics—Brief Report. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 1665–1669. [Google Scholar] [CrossRef]
- Perusko, M.; Apostolovic, D.; Kiewiet, M.B.G.; Grundström, J.; Hamsten, C.; Starkhammar, M.; Cirkovic Velickovic, T.; Van Hage, M. Bovine Γ-globulin, Lactoferrin, and Lactoperoxidase Are Relevant Bovine Milk Allergens in Patients with α-Gal Syndrome. Allergy 2021, 76, 3766–3775. [Google Scholar] [CrossRef] [PubMed]
- Chakrapani, N.; Fischer, J.; Swiontek, K.; Codreanu-Morel, F.; Hannachi, F.; Morisset, M.; Mugemana, C.; Bulaev, D.; Blank, S.; Bindslev-Jensen, C.; et al. α-Gal Present on Both Glycolipids and Glycoproteins Contributes to Immune Response in Meat-Allergic Patients. J. Allergy Clin. Immunol. 2022, 150, 396–405.e11. [Google Scholar] [CrossRef] [PubMed]
- Arkestål, K.; Sibanda, E.; Thors, C.; Troye-Blomberg, M.; Mduluza, T.; Valenta, R.; Grönlund, H.; Van Hage, M. Impaired Allergy Diagnostics among Parasite-Infected Patients Caused by IgE Antibodies to the Carbohydrate Epitope Galactose-A1,3-Galactose. J. Allergy Clin. Immunol. 2011, 127, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.-Y.; Henao-Martínez, A.F.; Agudelo Higuita, N.I. Incidence of Anaphylaxis in Patients with Alpha-Gal Syndrome Receiving Gelatin-Containing Vaccines: A Large Database Analysis. J. Allergy Clin. Immunol. Pract. 2025, 13, 421–423.e1. [Google Scholar] [CrossRef]
- Germán-Sánchez, A.; Alonso-Llamazares, A.; García-González, F.; Matala-Ahmed, B.; Melgar-Reyes, C.S.; Antepara-Ercoreca, I. Diagnostic Validity of Specific Immunoglobulin E Levels to Alpha-Gal in Alpha-Gal Syndrome: A Cross-Sectional Analysis. Allergy Asthma Clin. Immunol. 2023, 19, 102. [Google Scholar] [CrossRef]
- Lesmana, E.; Rao, S.; Keehn, A.; Edwinson, A.L.; Makol, A.; Grover, M. Clinical Presentation and Outcomes of Alpha-Gal Syndrome. Clin. Gastroenterol. Hepatol. 2025, 23, 69–78. [Google Scholar] [CrossRef]
- Homann, A.; Röckendorf, N.; Kromminga, A.; Frey, A.; Platts-Mills, T.A.; Jappe, U. Glycan and Peptide IgE Epitopes of the TNF-Alpha Blockers Infliximab and Adalimumab—Precision Diagnostics by Cross-Reactivity Immune Profiling of Patient Sera. Theranostics 2017, 7, 4699–4709. [Google Scholar] [CrossRef]
- Lis, K.; Ukleja-Sokołowska, N.; Karwowska, K.; Wernik, J.; Pawłowska, M.; Bartuzi, Z. Clinical Use of the ImmunoCAP Inhibition Test in the Diagnosis of Meat Allergy Caused by a Tick Bite in an Adult Male with No Previous Atopic History. Life 2023, 13, 699. [Google Scholar] [CrossRef]
- Recke, A.; Becker, M.; Jappe, U. Neu Erworbene Milchallergie Im Erwachsenenalter. Allergologie 2021, 44, 592–595. [Google Scholar] [CrossRef]
- Anemüller, W.; Mohr, M.; Brans, R.; Homann, A.; Jappe, U. Alpha-Gal-assoziierte verzögerte Anaphylaxie gegen rotes Fleisch als Berufskrankheit. Hautarzt 2018, 69, 848–852. [Google Scholar] [CrossRef]
- Cabezas-Cruz, A.; De La Fuente, J.; Fischer, J.; Hebsaker, J.; Lupberger, E.; Blumenstock, G.; Aichinger, E.; Yazdi, A.S.; Enkel, S.; Oehme, R.; et al. Prevalence of Type I Sensitization to Alpha-gal in Forest Service Employees and Hunters: Is the Blood Type an Overlooked Risk Factor in Epidemiological Studies of the α-Gal Syndrome? Allergy 2017, 72, 2044–2047. [Google Scholar] [CrossRef] [PubMed]
- Anvari, S.; Miller, J.; Yeh, C.-Y.; Davis, C.M. IgE-Mediated Food Allergy. Clin. Rev. Allerg. Immunol. 2019, 57, 244–260. [Google Scholar] [CrossRef]
- Guhsl, E.E.; Hofstetter, G.; Lengger, N.; Hemmer, W.; Ebner, C.; Fröschl, R.; Bublin, M.; Lupinek, C.; Breiteneder, H.; Radauer, C. IgE, IgG4 and IgA Specific to Bet v 1-related Food Allergens Do Not Predict Oral Allergy Syndrome. Allergy 2015, 70, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Sampson, H.A.; Ho, D.G. Relationship between Food-Specific IgE Concentrations and the Risk of Positive Food Challenges in Children and Adolescents. J. Allergy Clin. Immunol. 1997, 100, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, D.M.; Burks, A.W. Pitfalls in Food Allergy Diagnosis: Serum IgE Testing. J. Pediatr. 2015, 166, 8–10. [Google Scholar] [CrossRef]
- Sampson, H.A. Utility of Food-Specific IgE Concentrations in Predicting Symptomatic Food Allergy. J. Allergy Clin. Immunol. 2001, 107, 891–896. [Google Scholar] [CrossRef]
- Pearce, O.M.T.; Läubli, H. Sialic Acids in Cancer Biology and Immunity. Glycobiology 2016, 26, 111–128. [Google Scholar] [CrossRef]
- Mehlich, J.; Fischer, J.; Hilger, C.; Swiontek, K.; Morisset, M.; Codreanu-Morel, F.; Schiener, M.; Blank, S.; Ollert, M.; Darsow, U.; et al. The Basophil Activation Test Differentiates between Patients with Alpha-Gal Syndrome and Asymptomatic Alpha-Gal Sensitization. J. Allergy Clin. Immunol. 2019, 143, 182–189. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Bos d TG | Milk Protein | Pork Meat | Bovine Meat | Mutton | Gelatin |
|---|---|---|---|---|---|---|
| P01 | <0.1 | <0.1 | <0.1 | 0.27 | <0.1 | <0.1 |
| P02 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| P03 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| P04 | 5.62 | 0.46 | 0.65 | 1.14 | 0.63 | <0.1 |
| P05 | <0.1 | 0.17 | <0.1 | <0.1 | <0.1 | <0.1 |
| P06 | >100 | 0.31 | 2.15 | 5.65 | 0.61 | <0.1 |
| P07 | 0.11 | <0.1 | <0.1 | <0.1 | n.d. | <0.1 |
| P08 | 28.3 | 0.21 | <0.1 | <0.1 | <0.1 | <0.1 |
| P09 | <0.1 | <0.1 | <0.1 | <0.1 | n.d. | <0.1 |
| P10 | 4.96 | <0.1 | <0.1 | 0.14 | <0.1 | <0.1 |
| P11 | 33.6 | 0.23 | 0.43 | 0.98 | 0.36 | <0.1 |
| P12 | 8.7 | 0.29 | 0.27 | 0.69 | 0.38 | <0.1 |
| P13 | 0.10 | 0.16 | 0.18 | 0.13 | 0.16 | 0.12 |
| P14 | 30.7 | 2.83 | 16.1 | 22.1 | 6.39 | <0.1 |
| P15 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| P16 | 20.4 | 0.23 | 1.64 | 4.84 | 2.61 | <0.1 |
| P17 | 8.10 | <0.1 | 0.86 | 2.03 | 0.17 | <0.1 |
| P18 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| P19 | 41.3 | 1.95 | 12.6 | 24.2 | 4.86 | <0.1 |
| P20 | 23.8 | 0.27 | 3.86 | 8.8 | 0.58 | <0.1 |
| P21 | 65.3 | 2.57 | 7.62 | 19.5 | 6.57 | 0.2 |
| P22 | 31.7 | <0.1 | 0.94 | 4.8 | 0.48 | <0.1 |
| P23 | 5.96 | 0.14 | 0.89 | 2.41 | 0.26 | <0.1 |
| P24 | 13.1 | <0.1 | 1.26 | 4.18 | 1.99 | <0.1 |
| P25 | <0.1 | <0.1 | <0.1 | 0.32 | <0.1 | <0.1 |
| P26 | 1.61 | <0.1 | 0.12 | 0.30 | <0.1 | <0.1 |
| P27 | 1.41 | 0.20 | 0.1 | 0.55 | <0.1 | <0.1 |
| P28 | 0.48 | <0.1 | <0.1 | <0.1 | <0.1 | <0.1 |
| P29 | <0.1 | 1.0 | <0.1 | 0.79 | <0.1 | <0.1 |
| P30 | >100 | 10.5 | 12.7 | 46.5 | 9.72 | 0.17 |
| P31 | 1.94 | <0.1 | <0.1 | 0.23 | <0.1 | <0.1 |
| P32 | 2.29 | n.d. | 0.12 | 0.44 | n.d. | <0.1 |
| P33 | 5.79 | 0.18 | 1.04 | 2.09 | 1.19 | <0.1 |
| ID | Bos d 4 (α-Lactalbumin) | Bos d 5 (β-Lactoglobulin) | Bos d 6 (BSA) | Bos d 8 (Casein) |
|---|---|---|---|---|
| P01 | <0.1 | <0.1 | <0.1 | <0.1 |
| P02 | <0.1 | <0.1 | <0.1 | <0.1 |
| P03 | <0.1 | <0.1 | <0.1 | <0.1 |
| P04 | <0.1 | <0.1 | <0.1 | <0.1 |
| P05 | <0.1 | 0.13 | <0.1 | <0.1 |
| P06 | <0.1 | <0.1 | <0.1 | <0.1 |
| P07 | <0.1 | <0.1 | <0.1 | <0.1 |
| P08 | <0.1 | <0.1 | <0.1 | <0.1 |
| P09 | <0.1 | <0.1 | <0.1 | <0.1 |
| P10 | <0.1 | <0.1 | <0.1 | <0.1 |
| P11 | <0.1 | <0.1 | <0.1 | <0.1 |
| P12 | 0.15 | <0.1 | <0.1 | <0.1 |
| P13 | 0.25 | 0.27 | 0.19 | 0.18 |
| P14 | <0.1 | <0.1 | <0.1 | 0.31 |
| P15 | <0.1 | <0.1 | <0.1 | <0.1 |
| P16 | <0.1 | <0.1 | <0.1 | <0.1 |
| P17 | <0.1 | <0.1 | <0.1 | <0.1 |
| P18 | <0.1 | <0.1 | <0.1 | <0.1 |
| P19 | <0.1 | <0.1 | <0.1 | 9.2 |
| P20 | <0.1 | <0.1 | <0.1 | <0.1 |
| P21 | 0.26 | 0.27 | 0.33 | 0.29 |
| P22 | <0.1 | <0.1 | <0.1 | <0.1 |
| P23 | <0.1 | <0.1 | <0.1 | <0.1 |
| P24 | <0.1 | <0.1 | <0.1 | <0.1 |
| P25 | <0.1 | <0.1 | <0.1 | <0.1 |
| P26 | <0.1 | <0.1 | <0.1 | <0.1 |
| P27 | <0.1 | <0.1 | <0.1 | <0.1 |
| P28 | <0.1 | <0.1 | <0.1 | <0.1 |
| P29 | 0.73 | 0.28 | <0.1 | 0.35 |
| P30 | 0.22 | <0.1 | <0.1 | <0.1 |
| P31 | <0.1 | <0.1 | <0.1 | <0.1 |
| P32 | <0.1 | <0.1 | <0.1 | <0.1 |
| P33 | <0.1 | <0.1 | <0.1 | <0.1 |
| ID | CTX | IFX | HSA | HSA-α-Gal3 | Bos d TG | Bos d 6 |
|---|---|---|---|---|---|---|
| P01 | - | - | - | - | + | n.d. |
| P02 | - | - | - | - | + | - |
| P03 | - | - | - | - | + | - |
| P04 | + | - | - | + | - | - |
| P05 | - | - | - | - | - | - |
| P06 | + | - | - | + | + | - |
| P07 | - | - | - | - | - | - |
| P08 | + | n.d. | - | + | + | - |
| P09 | + | - | - | - | + | - |
| P10 | + | + | - | - | - | - |
| P11 | + | - | - | + | + | - |
| P12 | + | - | - | + | + | - |
| P13 | + | - | - | - | - | - |
| P14 | + | - | - | + | + | - |
| P15 | - | - | - | - | - | - |
| P16 | + | - | - | + | + | - |
| P17 | + | - | - | + | + | - |
| P18 | - | - | - | - | + | - |
| P19 | + | - | - | + | + | - |
| P20 | + | - | - | - | - | - |
| P21 | + | - | - | + | + | - |
| P22 | + | - | - | + | + | - |
| P23 | + | - | - | + | + | - |
| P24 | + | - | - | - | - | - |
| P25 | - | - | - | - | - | + |
| P26 | + | - | - | - | - | - |
| P27 | + | - | - | - | + | + |
| P28 | + | - | - | - | - | - |
| P29 | - | - | - | - | + | - |
| P30 | + | + | - | + | + | - |
| P31 | + | - | - | - | + | - |
| P32 | + | - | - | - | - | - |
| P33 | + | - | - | + | + | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jappe, U.; Kolaly, T.; de Vries, M.S.; Gülsen, A.; Homann, A. Connecting Diagnostics and Clinical Relevance of the α-Gal Syndrome—Individual Sensitization Patterns of Patients with Suspected α-Gal-Associated Allergy. Nutrients 2025, 17, 1541. https://doi.org/10.3390/nu17091541
Jappe U, Kolaly T, de Vries MS, Gülsen A, Homann A. Connecting Diagnostics and Clinical Relevance of the α-Gal Syndrome—Individual Sensitization Patterns of Patients with Suspected α-Gal-Associated Allergy. Nutrients. 2025; 17(9):1541. https://doi.org/10.3390/nu17091541
Chicago/Turabian StyleJappe, Uta, Tahmina Kolaly, Mareike S. de Vries, Askin Gülsen, and Arne Homann. 2025. "Connecting Diagnostics and Clinical Relevance of the α-Gal Syndrome—Individual Sensitization Patterns of Patients with Suspected α-Gal-Associated Allergy" Nutrients 17, no. 9: 1541. https://doi.org/10.3390/nu17091541
APA StyleJappe, U., Kolaly, T., de Vries, M. S., Gülsen, A., & Homann, A. (2025). Connecting Diagnostics and Clinical Relevance of the α-Gal Syndrome—Individual Sensitization Patterns of Patients with Suspected α-Gal-Associated Allergy. Nutrients, 17(9), 1541. https://doi.org/10.3390/nu17091541