
Temporal Trends and Clinical Impact of Malnutrition on In-Hospital Outcomes Among Patients with Advanced Chronic Kidney Disease: A Nationwide Inpatient Analysis

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Patient Sample
2.2. Study Population
2.3. Covariates and Outcomes Measure
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Prevalence of Malnutrition in Hospitalized Advanced CKD Patients, Stratified by Dialysis Status
3.3. Trends in Mild to Moderate/Severe Malnutrition Prevalence and In-Hospital Mortality
3.4. Association Between Mild to Moderate/Severe Malnutrition and In-Hospital Mortality
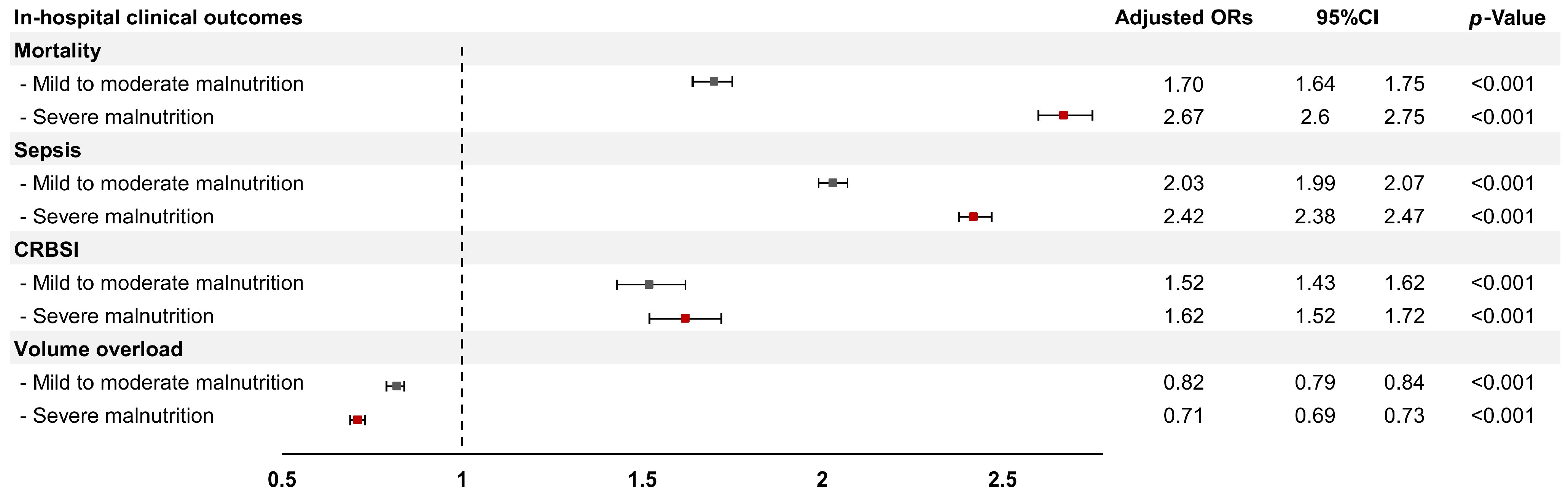
3.5. Association Between Mild to Moderate/Severe Malnutrition and Adverse Clinical Outcomes
3.6. Association Between Mild to Moderate/Severe Malnutrition and Inpatient Treatments
3.7. Association Between Mild to Moderate/Severe Malnutrition and Resource Utilization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AKI | acute kidney injury |
| CKD | chronic kidney disease |
| CRBSI | catheter-related bloodstream infection |
| EN | enteral nutrition |
| ESKD | end-stage kidney disease |
| HD | hemodialysis |
| ICD-10-CM | International Classification of Diseases, Tenth Revision, Clinical Modification |
| IQR | interquartile range |
| KRT | kidney replacement therapy |
| LOS | length of stay |
| NCD | non-communicable disease |
| NIS | National Inpatient Sample |
| ORs | odds ratios |
| PN | parenteral nutrition |
| PD | peritoneal dialysis |
| PEW | protein energy wasting |
| Semi-FFQ | Semi-Quantitative Food Frequency Questionnaire |
| SD | standard deviation |
| TPN | total parenteral nutrition |
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [PubMed]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Bradbury, B.D.; Kewalramani, R.; Barlev, A.; Mohanty, S.A.; Globe, D. Chronic kidney disease and US healthcare resource utilization in a nationally representative sample. Am. J. Nephrol. 2009, 29, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Hsu, C.C.; Lin, M.H.; Sung, J.M.; Kuo, T.H. Healthcare utilization and expenditure among individuals with end-stage kidney disease in Taiwan. J. Formos Med. Assoc. 2022, 121 (Suppl. 1), S47–S55. [Google Scholar] [CrossRef]
- Tahir, H.B.; Khan, M.N.A.; Tariq, R.; Khan, R.; Ahmed, M.B.; Khan, H.W. Assessment of Nutritional Status of Patients on the Maintenance Hemodialysis at Tertiary Care Hospital using Malnutrition Inflammatory Score. Pak. Armed Forces Med. J. 2022, 72, 2006. [Google Scholar] [CrossRef]
- Soeters, P.; Bozzetti, F.; Cynober, L.; Forbes, A.; Shenkin, A.; Sobotka, L. Defining malnutrition: A plea to rethink. Clin. Nutr. 2017, 36, 896–901. [Google Scholar] [CrossRef]
- World Health Organization. Malnutrition: WHO. Available online: https://www.who.int/health-topics/malnutrition#tab=tab_1 (accessed on 18 April 2025).
- Mahmoud, T.; Borgi, L. The Interplay Between Nutrition, Metabolic, and Endocrine Disorders in Chronic Kidney Disease. Semin. Nephrol. 2021, 41, 180–188. [Google Scholar] [CrossRef]
- Carrero, J.J.; Aguilera, A.; Stenvinkel, P.; Gil, F.; Selgas, R.; Lindholm, B. Appetite disorders in uremia. J. Ren. Nutr. 2008, 18, 107–113. [Google Scholar] [CrossRef]
- Raj, D.S.; Sun, Y.; Tzamaloukas, A.H. Hypercatabolism in dialysis patients. Curr. Opin. Nephrol. Hypertens. 2008, 17, 589–594. [Google Scholar] [CrossRef]
- Wang, W.; Liang, S.; Guo, X.; Wang, Y.; Chen, X.; Cai, G. Association of the malnutrition-inflammation score with physical function and functional disability in elderly patients with chronic kidney disease. Asia Pac. J. Clin. Nutr. 2023, 32, 57–62. [Google Scholar]
- Wathanavasin, W.; Banjongjit, A.; Avihingsanon, Y.; Praditpornsilpa, K.; Tungsanga, K.; Eiam-Ong, S.; Susantitaphong, P. Prevalence of Sarcopenia and Its Impact on Cardiovascular Events and Mortality among Dialysis Patients: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4077. [Google Scholar] [CrossRef] [PubMed]
- Tseng, P.W.; Lin, T.Y.; Hung, S.C. Association of Frailty with Nutritional Status in Patients with Chronic Kidney Disease. J. Ren. Nutr. 2024, 34, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Macedo, C.; Amaral, T.F.; Rodrigues, J.; Santin, F.; Avesani, C.M. Malnutrition and Sarcopenia Combined Increases the Risk for Mortality in Older Adults on Hemodialysis. Front. Nutr. 2021, 8, 721941. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.M.; Chen, Y.T.; Hung, S.C.; Shih, C.J.; Lin, C.H.; Chiang, C.K.; Tarng, D.-C.; The Taiwan Geriatric Kidney Disease (TGKD) Research Group. Association of estimated glomerular filtration rate with all-cause and cardiovascular mortality: The role of malnutrition–inflammation–cachexia syndrome. J. Cachexia Sarcopenia Muscle 2016, 7, 144–151. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Sugiyama, H.; Asai, A.; Kitamura, F.; Nobata, H.; Kinashi, H.; Katsuno, T.; Banno, S.; Ito, Y.; Imaizumi, T.; et al. Clinical Impact of Malnutrition According to the Global Leadership Initiative on Malnutrition Criteria Combined with Kidney Dysfunction to Determine Mortality in Inpatients. J. Ren. Nutr. 2024, 34, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, A.J.; Buitrago, G.; Rodríguez, N.; Gómez, G.; Sulo, S.; Gómez, C.; Partridge, J.; Misas, J.; Dennis, R.; Alba, M.J.; et al. Clinical and economic outcomes associated with malnutrition in hospitalized patients. Clin. Nutr. 2019, 38, 1310–1316. [Google Scholar] [CrossRef]
- Starke, J.; Schneider, H.; Alteheld, B.; Stehle, P.; Meier, R. Short-term individual nutritional care as part of routine clinical setting improves outcome and quality of life in malnourished medical patients. Clin. Nutr. 2011, 30, 194–201. [Google Scholar] [CrossRef]
- Bhasin, A.; Huang, L.; Shieh, M.S.; Pekow, P.; Lindenauer, P.K.; Lagu, T. Malnutrition in hospitalized adults in the United States, 2016-2019. J. Hosp. Med. 2024, 19, 1113–1121. [Google Scholar] [CrossRef]
- Slee, A.; Reid, J. Disease-related malnutrition in chronic kidney disease. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 136–141. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cederholm, T.; Avesani, C.M.; Bakker, S.J.; Bellizzi, V.; Cuerda, C.; Cupisti, A.; Sabatino, A.; Schneider, S.; Torreggiani, M.; et al. Nutritional status and the risk of malnutrition in older adults with chronic kidney disease–implications for low protein intake and nutritional care: A critical review endorsed by ERN-ERA and ESPEN. Clin. Nutr. 2023, 42, 443–457. [Google Scholar] [CrossRef]
- Salame, C.; Eaton, S.; Grimble, G.; Davenport, A. Protein Losses and Urea Nitrogen Underestimate Total Nitrogen Losses in Peritoneal Dialysis and Hemodialysis Patients. J. Ren. Nutr. 2018, 28, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Fang, J.; Li, W. Protein restriction for diabetic kidney disease. Cochrane Database Syst. Rev. 2023, 1, CD014906. [Google Scholar] [PubMed]
- Obeid, W.; Hiremath, S.; Topf, J.M. Protein Restriction for CKD: Time to Move On. Kidney360 2022, 3, 1611–1615. [Google Scholar] [CrossRef]
- Wathanavasin, W.; Kittiskulnam, P.; Johansen, K.L. Plant-based diets in patients with chronic kidney disease. Asian Biomed. Res. Rev. News 2024, 18, 2–10. [Google Scholar] [CrossRef]
- Wathanavasin, W.; Cheungpasitporn, W.; Thongprayoon, C.; Fülöp, T. Effects of Dietary Fiber Supplementation on Modulating Uremic Toxins and Inflammation in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Toxins 2025, 17, 57. [Google Scholar] [CrossRef]
- Kim, S.M.; Kang, B.C.; Kim, H.J.; Kyung, M.S.; Oh, H.J.; Kim, J.H.; Kwon, O.; Ryu, D.-R. Comparison of hemodialysis and peritoneal dialysis patients’ dietary behaviors. BMC Nephrol. 2020, 21, 91. [Google Scholar] [CrossRef]
- van Eck van der Sluijs, A.; Bonenkamp, A.A.; van Wallene, V.A.; Hoekstra, T.; Lissenberg-Witte, B.I.; Dekker, F.W.; van Ittersum, F.J.; Verhaar, M.C.; van Jaarsveld, B.C.; Abrahams, A.C.; et al. Differences in hospitalisation between peritoneal dialysis and haemodialysis patients. Eur. J. Clin. Investig. 2022, 52, e13758. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Thomas, F.; Nagy, K.; Arogundade, F.; Avesani, C.M.; Chan, M.; Chmielewski, M.; Cordeiro, A.C.; Espinosa-Cuevas, A.; Fiaccadori, E.; et al. Global prevalence of protein-energy wasting in kidney disease: A meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism. J. Ren. Nutr. 2018, 28, 380–392. [Google Scholar] [CrossRef]
- Bourke, C.D.; Berkley, J.A.; Prendergast, A.J. Immune dysfunction as a cause and consequence of malnutrition. Trends Immunol. 2016, 37, 386–398. [Google Scholar] [CrossRef]
- Cunningham-Rundles, S.; McNeeley, D.F.; Moon, A. Mechanisms of nutrient modulation of the immune response. J. Allergy Clin. Immunol. 2005, 115, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Sarnak, M.J.; Jaber, B.L. Mortality caused by sepsis in patients with end-stage renal disease compared with the general population. Kidney Int. 2000, 58, 1758–1764. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.J.; Foley, R.N.; Chavers, B.; Gilbertson, D.; Herzog, C.; Ishani, A.; Johansen, K.; Kasiske, B.L.; Kutner, N.; Liu, J.; et al. US Renal Data System 2013 Annual Data Report. Am. J. Kidney Dis. 2014, 63, A7. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.H.; Kireta, S.; Leedham, E.; Russ, G.R.; Coates, P.T. Uremia impairs monocyte and monocyte-derived dendritic cell function in hemodialysis patients. Kidney Int. 2007, 72, 1138–1148. [Google Scholar] [PubMed]
- Cohen, G.; Haag-Weber, M.; Hörl, W.H. Immune dysfunction in uremia. Kidney Int. Suppl. 1997, 62, S79–S82. [Google Scholar]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of immune dysfunction in end-stage renal disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar]
- Bou Chebl, R.; Tamim, H.; Abou Dagher, G.; Sadat, M.; Ghamdi, G.; Itani, A.; Saeedi, A.; Arabi, Y.M. Sepsis in end-stage renal disease patients: Are they at an increased risk of mortality? Ann. Med. 2021, 53, 1737–1743. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Pahl, M.V.; Crum, A.; Norris, K. Effect of uremia on structure and function of immune system. J. Ren. Nutr. 2012, 22, 149–156. [Google Scholar] [CrossRef]
- Rashid, I.; Sahu, G.; Tiwari, P.; Willis, C.; Asche, C.V.; Bagga, T.K.; Ghule, P.; Bland, A. Malnutrition as a potential predictor of mortality in chronic kidney disease patients on dialysis: A systematic review and meta-analysis. Clin. Nutr. 2024, 43, 1760–1769. [Google Scholar] [CrossRef]
- Kopp, C.; Linz, P.; Maier, C.; Wabel, P.; Hammon, M.; Nagel, A.M.; Rosenhauer, D.; Horn, S.; Uder, M.; Luft, F.C.; et al. Elevated tissue sodium deposition in patients with type 2 diabetes on hemodialysis detected by 23Na magnetic resonance imaging. Kidney Int. 2018, 93, 1191–1197. [Google Scholar] [CrossRef]
- Kopp, C.; Linz, P.; Wachsmuth, L.; Dahlmann, A.; Horbach, T.; Schöfl, C.; Renz, W.; Santoro, D.; Niendorf, T.; Müller, D.N.; et al. 23Na magnetic resonance imaging of tissue sodium. Hypertension 2012, 59, 167–172. [Google Scholar] [CrossRef]
- Hengel, F.E.; Benitah, J.-P.; Wenzel, U.O. Mosaic theory revised: Inflammation and salt play central roles in arterial hypertension. Cell. Mol. Immunol. 2022, 19, 561–576. [Google Scholar] [CrossRef] [PubMed]
- Moramarco, S.; Morciano, L.; Morucci, L.; Messinese, M.; Gualtieri, P.; Carestia, M.; Ciccacci, F.; Orlando, S.; Buonomo, E.; Legramante, J.M.; et al. Epidemiology of Hypoalbuminemia in Hospitalized Patients: A Clinical Matter or an Emerging Public Health Problem? Nutrients 2020, 12, 3656. [Google Scholar] [CrossRef] [PubMed]
- John, B.; Tan, B.K.; Dainty, S.; Spanel, P.; Smith, D.; Davies, S.J. Plasma volume, albumin, and fluid status in peritoneal dialysis patients. Clin. J. Am. Soc. Nephrol. 2010, 5, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Tan, B.K.; Dainty, S.; Mattey, D.L.; Davies, S.J. Hypoalbuminaemia, systemic albumin leak and endothelial dysfunction in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2012, 27, 4437–4445. [Google Scholar] [CrossRef]
- Boullata, J.I.; Gilbert, K.; Sacks, G.; Labossiere, R.J.; Crill, C.; Goday, P.; Kumpf, V.J.; Mattox, T.W.; Plogsted, S.; Holcombe, B.; et al. ASPEN clinical guidelines: Parenteral nutrition ordering, order review, compounding, labeling, and dispensing. JPEN J. Parenter. Enter. Nutr. 2014, 38, 334–377. [Google Scholar] [CrossRef]
- Berlana, D.; Barraquer, A.; Sabin, P.; Chicharro, L.; Pérez, A.; Puiggrós, C.; Burgos, R.; Martínez-Cutillas, J. Impact of parenteral nutrition standardization on costs and quality in adult patients. Nutr. Hosp. 2014, 30, 351–358. [Google Scholar]
- Babitt, J.L.; Eisenga, M.F.; Haase, V.H.; Kshirsagar, A.V.; Levin, A.; Locatelli, F.; Małyszko, J.; Swinkels, D.W.; Tarng, D.-C.; Cheung, M.; et al. Controversies in optimal anemia management: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2021, 99, 1280–1295. [Google Scholar] [CrossRef]
- Huang, C.H.; Chao, J.Y.; Ling, T.C.; Wu, J.L.; Sung, J.M.; Sun, C.Y.; Cheng, Y.-Y.; Chang, Y.-T. Effect of dialysis modalities on risk of hospitalization for gastrointestinal bleeding. Sci. Rep. 2023, 13, 52. [Google Scholar] [CrossRef]
- Tsai, T.J.; Chen, W.C.; Huang, Y.T.; Yang, Y.H.; Feng, I.C.; Wu, W.C.; Hu, H.-M.; Wu, D.-C.; Hsu, P.-I. Hemodialysis Increases the Risk of Lower Gastrointestinal Bleeding and Angiodysplasia Bleeding: A Nationwide Population Study. Gastroenterol. Res. Pract. 2020, 2020, 7206171. [Google Scholar] [CrossRef]
- Khalatbari-Soltani, S.; Waeber, G.; Marques-Vidal, P. Diagnostic accuracy of undernutrition codes in hospital administrative discharge database: Improvements needed. Nutrition 2018, 55–56, 111–115. [Google Scholar] [CrossRef]
- Rasmussen, N.H.; Thomsen, R.W.; Rasmussen, H.H.; Søgaard, M. Validity of diagnostic coding for undernutrition in hospitals. Clin. Nutr. 2016, 35, 491–495. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variables | No Malnutrition (n = 1,113,043) | Malnutrition | p-Value | |
|---|---|---|---|---|
| Mild to Moderate (n = 67,587) | Severe (n = 63,785) | |||
| Age (years) | 61.3 ± 15.3 | 64.8 ± 14.8 | 65.4 ± 14.5 | <0.001 |
| Male sex, n (%) | 608,460 (54.7) | 35,537 (52.6) | 35,174 (55.2) | <0.001 |
| Race, n (%) | ||||
| White | 440,474 (42.3) | 28,666 (45.3) | 27,388 (45.9) | <0.001 |
| Black | 369,407 (35.4) | 21,207 (33.5) | 20,476 (34.3) | |
| Hispanic | 188,573 (18.1) | 10,407 (16.4) | 8797 (14.7) | |
| Asian or Pacific Islander | 43,859 (4.2) | 3040 (4.8) | 3024 (5.1) | |
| Dialysis status, n (%) | ||||
| Non-dialysis | 513,974 (46.2) | 29,471 (43.6) | 26,603 (41.7) | <0.001 |
| Hemodialysis | 556,788 (50.0) | 34,986 (51.8) | 34,764 (54.5) | |
| Peritoneal dialysis | 42,281 (3.8) | 3130 (4.6) | 2418 (3.8) | |
| Charlson comorbidity score, median (IQR) | 5 (4–6) | 5 (4–7) | 5 (4–7) | <0.001 |
| Elixhauser score, median (IQR) | 6 (4–7) | 7 (6–8) | 7 (6–8) | <0.001 |
| Comorbidity, n (%) | ||||
| Diabetes mellitus | 712,772 (64.0) | 41,117 (60.8) | 33,470 (52.5) | <0.001 |
| Hypertension | 1,057,154 (95.0) | 62,828 (93.0) | 57,409 (90.0) | <0.001 |
| Dyslipidemia | 455,298 (40.9) | 24,768 (36.7) | 20,445 (32.1) | <0.001 |
| Congestive heart failure | 536,736 (48.2) | 35,531 (52.6) | 32,598 (51.1) | <0.001 |
| Coronary artery disease | 178,875 (16.1) | 10,594 (15.7) | 9422 (14.8) | <0.001 |
| Cerebrovascular disease | 94,509 (8.5) | 7726 (11.4) | 6978 (10.9) | <0.001 |
| Peripheral vascular disease | 148,460 (13.3) | 10,883 (16.1) | 9847 (15.4) | <0.001 |
| Cirrhosis | 95,264 (8.6) | 9350 (13.8) | 10,972 (17.2) | <0.001 |
| Malignancy | 51,170 (4.6) | 5089 (7.5) | 6962 (10.9) | <0.001 |
| Dementia/cognitive impairment | 59,434 (5.3) | 6493 (9.6) | 7062 (11.1) | <0.001 |
| Smoking, n (%) | 250,756 (22.5) | 12,232 (18.1) | 11,078 (17.4) | <0.001 |
| Alcohol use, n (%) | 25,986 (2.3) | 2643(3.9) | 3227 (5.1) | <0.001 |
| Elective admission, n (%) | 99,349 (8.9) | 5066 (7.5) | 3691 (5.8) | <0.001 |
| Length of stay, days, median (IQR) | 4 (2–8) | 8 (4–15) | 8 (4–16) | <0.001 |
| Hospitalization cost ($), median (IQR) | 48,155 (25,571–96,002) | 80,674 (40,733–173,328) | 84,957 (41,558–186,404) | <0.001 |
| Hospital location/teaching status, n (%) | ||||
| Rural | 55,734 (5.0) | 2745 (4.1) | 2706 (4.2) | <0.001 |
| Urban—nonteaching | 251,592 (19.4) | 13,612 (20.1) | 12,077 (18.9) | |
| Urban—teaching | 841,717 (75.6) | 51,230 (75.8) | 49,002 (76.8) | |
| Nutritional Status | Total, n (%) (n = 1,244,415) | Dialysis Status, n (%) | p-Value | ||
|---|---|---|---|---|---|
| Non-Dialysis (n = 570,048) | HD (n = 626,538) | PD (n = 47,829) | |||
| No malnutrition | 1,113,043 (89.4) | 513,974 (90.1) | 556,788 (88.9) | 42,281 (88.4) | <0.001 |
| Mild to moderate malnutrition | 67,587 (5.4) | 29,471 (5.2) | 34,986 (5.6) | 3130 (6.5) | <0.001 |
| Severe malnutrition | 63,785 (5.1) | 26,603 (4.7) | 34,764 (5.5) | 2418 (5.1) | <0.001 |
| In-Hospital Outcomes | No Malnutrition (n = 1,113,043) | Mild to Moderate Malnutrition (n = 67,587) | Severe Malnutrition (n = 63,785) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | Univariable Analysis | Multivariable Analysis | ||||||
| OR (95% CI) | p-Value | Adjusted OR * (95% CI) | p-Value | OR (95% CI) | p-Value | Adjusted OR * (95% CI) | p-Value | ||
| Primary outcome | |||||||||
| In-hospital mortality | Ref. | 2.07 (2.00–2.13) | <0.001 | 1.70 (1.64–1.75) | <0.001 | 3.51 (3.42–3.60) | <0.001 | 2.67 (2.60–2.75) | <0.001 |
| Secondary outcomes | |||||||||
| Adverse clinical outcomes | |||||||||
| Sepsis | Ref. | 2.24 (2.20–2.28) | <0.001 | 2.03 (1.99–2.07) | <0.001 | 2.79 (2.74–2.84) | <0.001 | 2.42 (2.38–2.47) | <0.001 |
| Catheter-related bloodstream infection | Ref. | 1.53 (1.44–1.63) | <0.001 | 1.52 (1.43–1.62) | <0.001 | 1.74 (1.64–1.85) | <0.001 | 1.62 (1.52–1.72) | <0.001 |
| Volume overload | Ref. | 0.74 (0.72–0.77) | <0.001 | 0.82 (0.79–0.84) | <0.001 | 0.64 (0.62–0.66) | <0.001 | 0.71 (0.69–0.73) | <0.001 |
| Inpatient treatments | |||||||||
| Need for vasopressors | Ref. | 2.30 (2.17–2.42) | <0.001 | 1.89 (1.79–2.00) | <0.001 | 3.12 (2.98–3.27) | <0.001 | 2.32 (2.21–2.44) | <0.001 |
| TPN use | Ref. | 8.40 (7.71–9.14) | <0.001 | 7.78 (7.12–8.50) | <0.001 | 13.95 (12.93–15.05) | <0.001 | 11.94 (10.99–12.97) | <0.001 |
| Mechanical ventilation | Ref. | 1.18 (1.14–1.23) | <0.001 | 1.11 (1.06–1.15) | <0.001 | 1.30 (1.25–1.35) | <0.001 | 1.19 (1.15–1.24) | <0.001 |
| Blood transfusion | Ref. | 1.75 (1.70–1.80) | <0.001 | 1.61 (1.57–1.66) | <0.001 | 2.03 (1.98–2.09) | <0.001 | 1.77 (1.72–1.82) | <0.001 |
| Resource utilization | |||||||||
| Length of hospital stay (days) | Ref. | 5.78 (5.12–5.95) | <0.001 | 5.32 (5.16–5.47) | <0.001 | 7.65 (7.44–7.86) | <0.001 | 7.00 (6.80–7.20) | <0.001 |
| Hospitalization cost ($) | Ref. | 79,019.5 (75,196.2–82,842.7) | <0.001 | 73,129.5 (69,592.8–76,666.2) | <0.001 | 107,529.6 (102,192.9–112,866.3) | <0.001 | 97,766.6 (92,805.4–102,727.8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wathanavasin, W.; Thongprayoon, C.; Kaewput, W.; Tangpanithandee, S.; Suppadungsuk, S.; Cheungpasitporn, W. Temporal Trends and Clinical Impact of Malnutrition on In-Hospital Outcomes Among Patients with Advanced Chronic Kidney Disease: A Nationwide Inpatient Analysis. Nutrients 2025, 17, 1508. https://doi.org/10.3390/nu17091508
Wathanavasin W, Thongprayoon C, Kaewput W, Tangpanithandee S, Suppadungsuk S, Cheungpasitporn W. Temporal Trends and Clinical Impact of Malnutrition on In-Hospital Outcomes Among Patients with Advanced Chronic Kidney Disease: A Nationwide Inpatient Analysis. Nutrients. 2025; 17(9):1508. https://doi.org/10.3390/nu17091508
Chicago/Turabian StyleWathanavasin, Wannasit, Charat Thongprayoon, Wisit Kaewput, Supawit Tangpanithandee, Supawadee Suppadungsuk, and Wisit Cheungpasitporn. 2025. "Temporal Trends and Clinical Impact of Malnutrition on In-Hospital Outcomes Among Patients with Advanced Chronic Kidney Disease: A Nationwide Inpatient Analysis" Nutrients 17, no. 9: 1508. https://doi.org/10.3390/nu17091508
APA StyleWathanavasin, W., Thongprayoon, C., Kaewput, W., Tangpanithandee, S., Suppadungsuk, S., & Cheungpasitporn, W. (2025). Temporal Trends and Clinical Impact of Malnutrition on In-Hospital Outcomes Among Patients with Advanced Chronic Kidney Disease: A Nationwide Inpatient Analysis. Nutrients, 17(9), 1508. https://doi.org/10.3390/nu17091508