
The Non-High-Density Lipoprotein Cholesterol (Non-HDL-C) to HDL-C Ratio (NHHR) and Its Association with Chronic Kidney Disease in Chinese Adults with Type 2 Diabetes: A Preliminary Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Sample Size Calculation
2.3. Data Collection
2.4. Definitions of Variables
2.4.1. Definitions of CKD and NHHR
2.4.2. Definitions of Covariates
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of Participants
3.2. Multivariable Regression Analysis of NHHR Quartiles in Relation to CKD
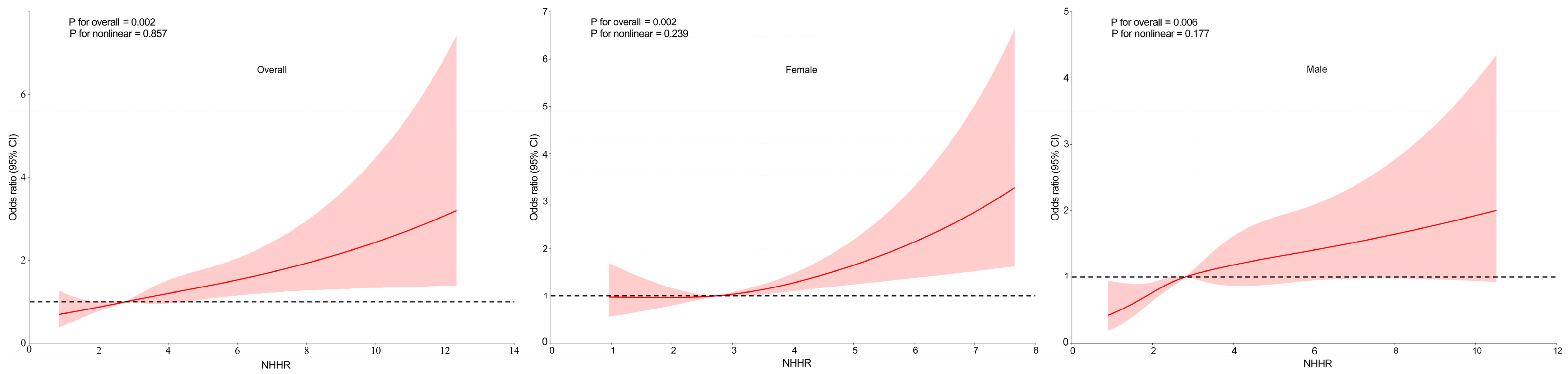
3.3. RCS Analysis of the Association Between NHHR and CKD
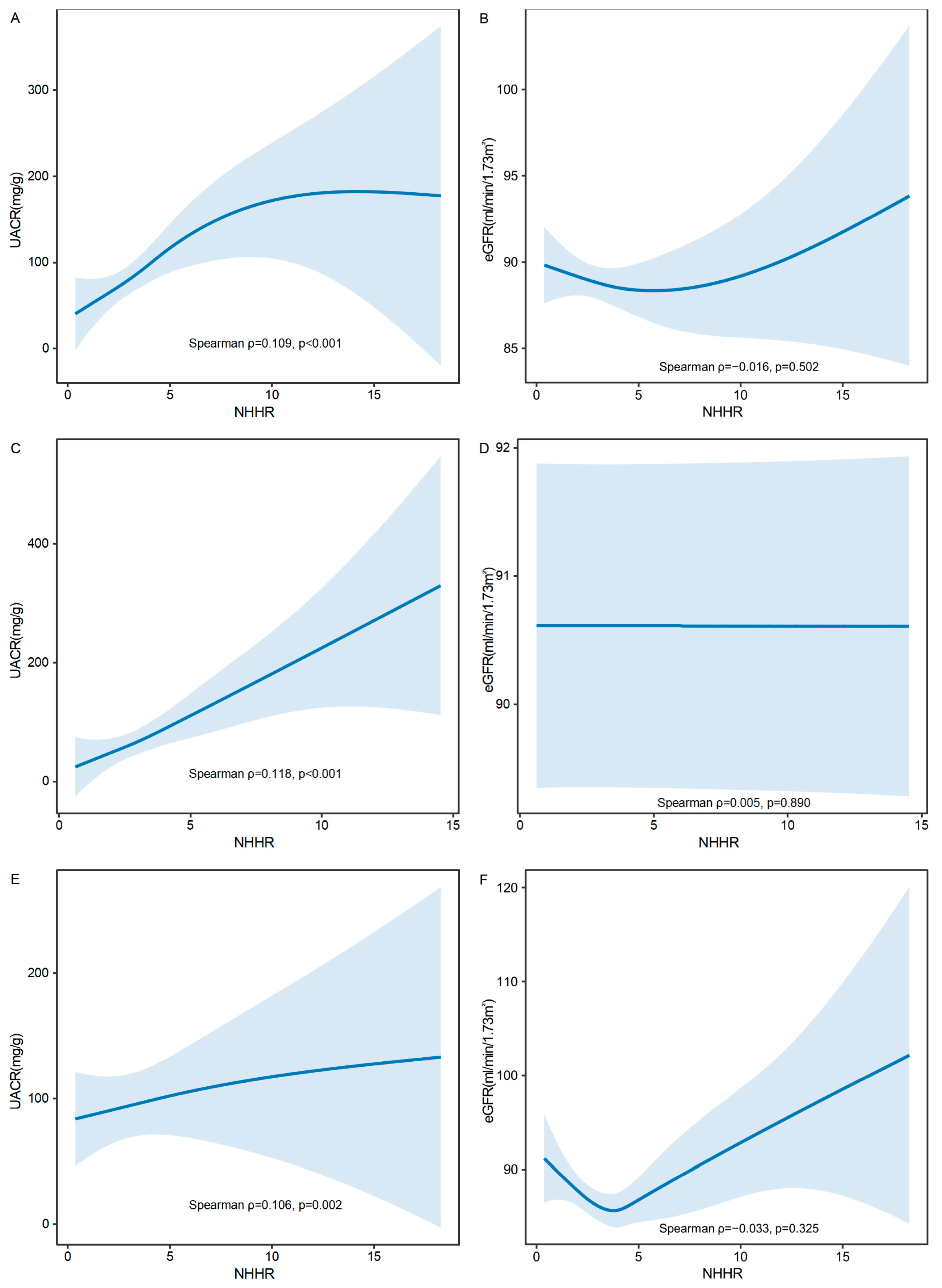
3.4. GAM Analysis of NHHR with UACR and eGFR
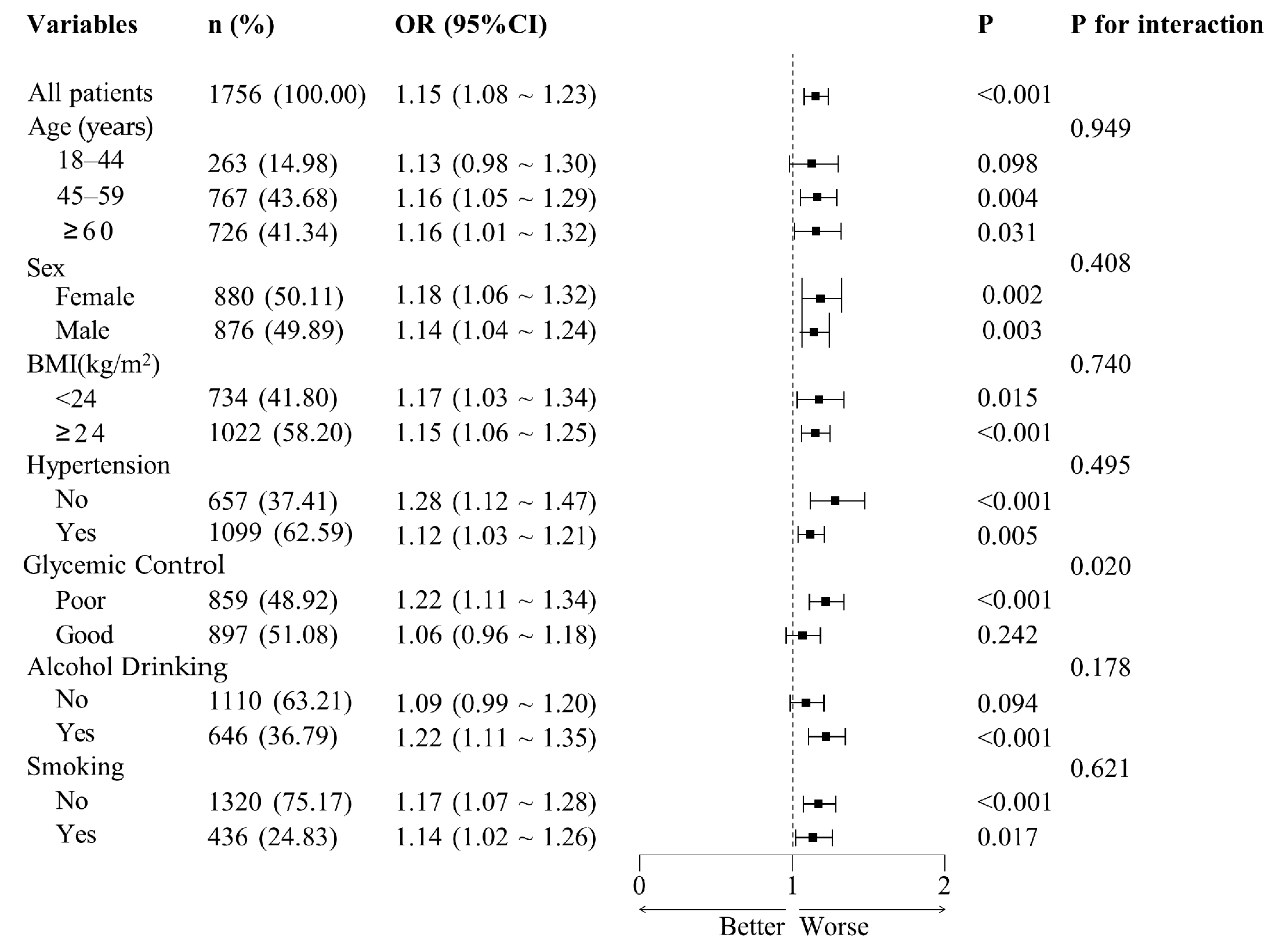
3.5. Results of Subgroup Analyses
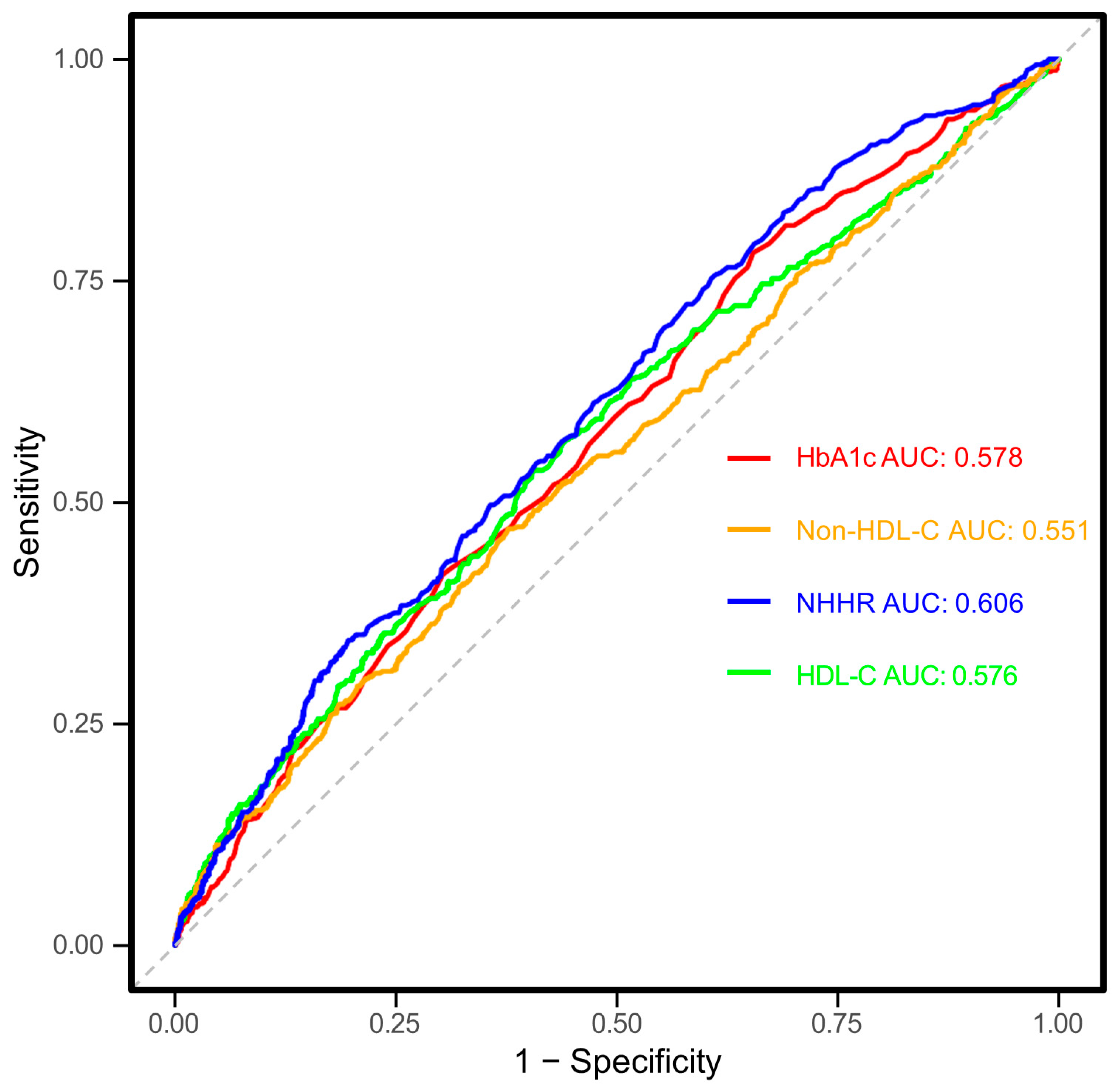
3.6. Roc Curve Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HDL-C | High-density lipoprotein cholesterol |
| Non-HDL-C | Non-high-density lipoprotein cholesterol |
| NHHR | Non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio |
| T2DM | Type 2 diabetes mellitus |
| CKD | Chronic kidney disease |
| RCS | Restricted cubic spline |
| GAM | Generalized additive models |
| UACR | Urinary albumin-to-creatinine ratio |
| eGFR | Estimated glomerular filtration rate |
| BMI | Body mass index |
| TC | Total cholesterol |
| TG | Triglycerides |
| SUA | Serum uric acid |
| LDL-C | Low-density lipoprotein cholesterol |
| VLDL-C | Very-low-density lipoprotein cholesterol |
| IR | Insulin resistance |
| HbA1c | Hemoglobin A1c |
| FPG | Fasting blood glucose |
| SD | Standard deviation |
| IQR | Interquartile range |
| OR | Odds ratio |
| CI | Confidence interval |
| Q1 | First quartile |
| Q2 | Second quartile |
| Q3 | Third quartile |
| Q4 | Fourth quartile |
| PSM | Propensity score matching |
| SMD | Standardized mean difference |
| ANOVA | Analysis of variance |
| RAAS | Renin-angiotensin-aldosterone system |
| NHANES | National Health and Nutrition Examination Survey |
References
- Deng, W.; Zhao, L.; Chen, C.; Ren, Z.; Jing, Y.; Qiu, J.; Liu, D. National burden and risk factors of diabetes mellitus in China from 1990 to 2021: Results from the Global Burden of Disease study 2021. J. Diabetes 2024, 16, e70012. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Peng, W.; Zhao, Z.; Zhang, M.; Shi, Z.; Song, Z.; Zhang, X.; Li, C.; Huang, Z.; Sun, X.; et al. Prevalence and Treatment of Diabetes in China, 2013–2018. JAMA-J. Am. Med. Assoc. 2021, 326, 2498–2506. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Presslie, C.; Rutter, M.K.; McGuire, D.K. Cardiovascular and Kidney Risks in Individuals with Type 2 Diabetes: Contemporary Understanding with Greater Emphasis on Excess Adiposity. Diabetes Care 2024, 47, 531–543. [Google Scholar] [CrossRef]
- Chaudhry, K.; Karalliedde, J. Chronic kidney disease in type 2 diabetes: The size of the problem, addressing residual renal risk and what we have learned from the CREDENCE trial. Diabetes Obes. Metab. 2024, 26 (Suppl. S5), 25–34. [Google Scholar] [CrossRef]
- Sardar, M.B.; Nadeem, Z.A.; Babar, M. Tirzepatide: A novel cardiovascular protective agent in type 2 diabetes mellitus and obesity. Curr. Probl. Cardiol. 2024, 49, 102489. [Google Scholar] [CrossRef]
- Triozzi, J.L.; Parker, G.L.; Virani, S.S.; Navaneethan, S.D. Management of type 2 diabetes in chronic kidney disease. BMJ Open Diab. Res. Care 2021, 9, e002300. [Google Scholar] [CrossRef]
- Pan, X.; Lin, X.; Huang, X.; Xu, J.; Ye, L.; Zhang, T.; Hu, S.; Jiang, H.; Ren, Y.; Shan, P.F. The Burden of Diabetes-Related Chronic Kidney Disease in China From 1990 to 2019. Front. Endocrinol. 2022, 13, 892860. [Google Scholar] [CrossRef]
- Giardini, E.; Moore, D.; Sadlier, D.; Godson, C.; Brennan, E. The dual role of lipids in chronic kidney disease: Pathogenic culprits and therapeutic allies. Atherosclerosis 2024, 398, 118615. [Google Scholar] [CrossRef]
- Chiesa, S.T.; Charakida, M. High-Density Lipoprotein Function and Dysfunction in Health and Disease. Cardiovasc. Drugs Ther. 2019, 33, 207–219. [Google Scholar] [CrossRef]
- Calabresi, L.; Gomaraschi, M.; Franceschini, G. Endothelial protection by high-density lipoproteins: From bench to bedside. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1724–1731. [Google Scholar] [CrossRef]
- Jourde-Chiche, N.; Fakhouri, F.; Dou, L.; Bellien, J.; Burtey, S.; Frimat, M.; Jarrot, P.A.; Kaplanski, G.; Le Quintrec, M.; Pernin, V.; et al. Endothelium structure and function in kidney health and disease. Nat. Rev. Nephrol. 2019, 15, 87–108. [Google Scholar] [PubMed]
- Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 2017, 38, 2478–2486. [Google Scholar]
- Kaur, N.; Pandey, A.; Negi, H.; Shafiq, N.; Reddy, S.; Kaur, H.; Chadha, N.; Malhotra, S. Effect of HDL-raising drugs on cardiovascular outcomes: A systematic review and meta-regression. PLoS ONE 2014, 9, e94585. [Google Scholar]
- Guan, X.M.; Shi, H.P.; Xu, S.; Chen, Y.; Zhang, R.F.; Dong, Y.X.; Gao, L.J.; Wu, S.L.; Xia, Y.L. Cumulative non-high-density lipoprotein cholesterol burden and risk of atherosclerotic cardiovascular disease: A prospective community-based study. Front. Cardiovasc. Med. 2023, 10, 1105342. [Google Scholar]
- Roumeliotis, S.; Roumeliotis, A.; Georgianos, P.I.; Stamou, A.; Manolopoulos, V.G.; Panagoutsos, S.; Liakopoulos, V. Oxidized LDL Is Associated with eGFR Decline in Proteinuric Diabetic Kidney Disease: A Cohort Study. Oxidative Med. Cell. Longev. 2021, 2021, 2968869. [Google Scholar]
- Zhang, F.; Li, Z.; Wang, M.; Wang, Y.; Lu, C. Association of non-highdensity lipoprotein cholesterol to highdensity lipoprotein cholesterol ratio (NHHR) and subsequent hypertension and heart diseases: Findings from the CHARLS cohort. Aging Clin. Exp. Res. 2025, 37, 26. [Google Scholar]
- Han, Y.Z.; Du, B.X.; Zhu, X.Y.; Wang, Y.Z.; Zheng, H.J.; Liu, W.J. Lipid metabolism disorder in diabetic kidney disease. Front. Endocrinol. 2024, 15, 1336402. [Google Scholar]
- Lu, C.F.; Liu, W.S.; Chen, Z.H.; Hua, L.Y.; Wang, X.Q.; Huang, H.Y. Comparisons of the Relationships Between Multiple Lipid Indices and Diabetic Kidney Disease in Patients with Type 2 Diabetes: A Cross-Sectional Study. Front. Endocrinol. 2022, 13, 888599. [Google Scholar]
- Su, X.; Rao, H.; Zhao, C.; Wu, J.; Zhang, X.; Li, D. Association between the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and mortality among hypertension patients. Sci. Rep. 2025, 15, 6012. [Google Scholar]
- Liu, C.; Dhindsa, D.; Almuwaqqat, Z.; Ko, Y.A.; Mehta, A.; Alkhoder, A.A.; Alras, Z.; Desai, S.R.; Patel, K.J.; Hooda, A.; et al. Association Between High-Density Lipoprotein Cholesterol Levels and Adverse Cardiovascular Outcomes in High-risk Populations. JAMA Cardiol. 2022, 7, 672–680. [Google Scholar]
- Hashem, C.; Altin, S.E.; Guyton, J.R.; Boden, W.E. Nonlinearity of the inverse relationship between high-density lipoprotein (HDL) cholesterol and incident cardiovascular risk: Is it time to revisit the “HDL hypothesis”? J. Clin. Lipidol. 2024, in press. [Google Scholar] [CrossRef]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martin, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.H.; Wang, L.M.; Chen, S.Y.; Liang, Y.B.; Zhang, M.; Huang, Z.J.; Chen, H.L.; Wu, J.Z.; Wu, J.; Jia, W.P. Data Resource Profile: A Protocol of China National Diabetic Chronic Complications Study. Biomed. Environ. Sci. 2022, 35, 633–640. [Google Scholar] [PubMed]
- Guo, K.; Zhang, L.; Zhao, F.; Lu, J.; Pan, P.; Yu, H.; Bao, Y.; Chen, H.; Jia, W. Prevalence of chronic kidney disease and associated factors in Chinese individuals with type 2 diabetes: Cross-sectional study. J. Diabetes Complicat. 2016, 30, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Stempniewicz, N.; Vassalotti, J.A.; Cuddeback, J.K.; Ciemins, E.; Storfer-Isser, A.; Sang, Y.; Matsushita, K.; Ballew, S.H.; Chang, A.R.; Levey, A.S.; et al. Chronic Kidney Disease Testing Among Primary Care Patients with Type 2 Diabetes Across 24 U.S. Health Care Organizations. Diabetes Care 2021, 44, 2000–2009. [Google Scholar] [CrossRef]
- Chen, T.K.; Knicely, D.H.; Grams, M.E. Chronic Kidney Disease Diagnosis and Management: A Review. JAMA-J. Am. Med. Assoc. 2019, 322, 1294–1304. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.R.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Y.; Luo, D.; Chen, B.; Lai, C.; He, C.; Li, S. Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and cardiometabolic multimorbidity among middle-aged and older adults in China. BMC Public Health 2025, 25, 570. [Google Scholar] [CrossRef]
- Wang, J.G.; Zhang, W.; Li, Y.; Liu, L. Hypertension in China: Epidemiology and treatment initiatives. Nat. Rev. Cardiol. 2023, 20, 531–545. [Google Scholar] [CrossRef]
- Zeng, Q.; Li, N.; Pan, X.F.; Chen, L.; Pan, A. Clinical management and treatment of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 393–405. [Google Scholar] [CrossRef]
- Wang, X.; Tian, B.; Zhang, S.; Zhang, J.; Yang, W.; Li, J.; Wang, W.; Wang, Y.; Zhang, W. Diabetes knowledge predicts HbA1c levels of people with type 2 diabetes mellitus in rural China: A ten-month follow-up study. Sci. Rep. 2023, 13, 18248. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wu, Y.; Bai, Z.; Xu, X.; Su, D.; Chen, J.; He, R.; Sun, J. The Association Between Family Health and Frailty with the Mediation Role of Health Literacy and Health Behavior Among Older Adults in China: Nationwide Cross-Sectional Study. JMIR Public Health Surveill. 2023, 9, e44486. [Google Scholar]
- Chen, X.; Du, X.; Lu, F.; Zhang, J.; Xu, C.; Liang, M.; Chen, L.; Zhong, J. The Association Between the Triglyceride-Glucose Index, Its Combination with the Body Roundness Index, and Chronic Kidney Disease in Patients with Type 2 Diabetes in Eastern China: A Preliminary Study. Nutrients 2025, 17, 492. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Li, M.; Yu, Z.; Zheng, T.; Feng, X.; Gao, A.; Zhang, H.; Gao, R. The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) as a predictor of all-cause and cardiovascular mortality in US adults with diabetes or prediabetes: NHANES 1999–2018. BMC Med. 2024, 22, 317. [Google Scholar]
- Tsoupras, A.; Lordan, R.; Zabetakis, I. Inflammation, not Cholesterol, Is a Cause of Chronic Disease. Nutrients 2018, 10, 604. [Google Scholar] [CrossRef]
- Lu, J.; Wang, X.; Wang, W.; Muniyappa, H.; Deshmukh, A.; Hu, C.; Das, K.; Mehta, J.L. Abrogation of lectin-like oxidized LDL receptor-1 attenuates acute myocardial ischemia-induced renal dysfunction by modulating systemic and local inflammation. Kidney Int. 2012, 82, 436–444. [Google Scholar]
- Xu, Z.; Yang, S.; Cui, L. Understanding the heterogeneity and dysfunction of HDL in chronic kidney disease: Insights from recent reviews. BMC Nephrol. 2024, 25, 400. [Google Scholar]
- Fioretto, P.; Zambon, A.; Rossato, M.; Busetto, L.; Vettor, R. SGLT2 Inhibitors and the Diabetic Kidney. Diabetes Care 2016, 39 (Suppl. S2), S165–S171. [Google Scholar] [CrossRef]
- Huang, J.K.; Lee, H.C. Emerging Evidence of Pathological Roles of Very-Low-Density Lipoprotein (VLDL). Int. J. Mol. Sci. 2022, 23, 4300. [Google Scholar] [CrossRef]
- Ma, K.; Gao, W.; Xu, H.; Liang, W.; Ma, G. Role and Mechanism of the Renin-Angiotensin-Aldosterone System in the Onset and Development of Cardiorenal Syndrome. J. Renin-Angiotensin-Aldosterone Syst. 2022, 2022, 3239057. [Google Scholar]
- Kang, H.M.; Ahn, S.H.; Choi, P.; Ko, Y.A.; Han, S.H.; Chinga, F.; Park, A.S.; Tao, J.; Sharma, K.; Pullman, J.; et al. Defective fatty acid oxidation in renal tubular epithelial cells has a key role in kidney fibrosis development. Nat. Med. 2015, 21, 37–46. [Google Scholar] [PubMed]
- Long, Z.; Luo, Y.; Yu, M.; Wang, X.; Zeng, L.; Yang, K. Targeting ferroptosis: A new therapeutic opportunity for kidney diseases. Front. Immunol. 2024, 15, 1435139. [Google Scholar]
- Tang, P.M.; Zhang, Y.Y.; Mak, T.S.; Tang, P.C.; Huang, X.R.; Lan, H.Y. Transforming growth factor-beta signalling in renal fibrosis: From Smads to non-coding RNAs. J. Physiol. 2018, 596, 3493–3503. [Google Scholar]
- Liu, K.; Cooper, M.E.; Chai, Z.; Liu, F. High-Density Lipoprotein in Patients with Diabetic Kidney Disease: Friend or Foe? Int. J. Mol. Sci. 2025, 26, 1683. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Chertow, G.M.; Devarajan, P.; Levin, A.; Andreoli, S.P.; Bangalore, S.; Warady, B.A. Chronic Inflammation in Chronic Kidney Disease Progression: Role of Nrf2. Kidney Int. Rep. 2021, 6, 1775–1787. [Google Scholar]
- Hwang, S.W.; Lee, T.; Uh, Y.; Lee, J.Y. Urinary albumin creatinine ratio is associated with lipid profile. Sci. Rep. 2024, 14, 14870. [Google Scholar]
- Li, Y.; Liu, Y.; Liu, S.; Gao, M.; Wang, W.; Chen, K.; Huang, L.; Liu, Y. Diabetic vascular diseases: Molecular mechanisms and therapeutic strategies. Signal Transduct. Target. Ther. 2023, 8, 152. [Google Scholar]
- Agrawal, S.; Zaritsky, J.J.; Fornoni, A.; Smoyer, W.E. Dyslipidaemia in nephrotic syndrome: Mechanisms and treatment. Nat. Rev. Nephrol. 2018, 14, 57–70. [Google Scholar]
- Zsom, L.; Zsom, M.; Salim, S.A.; Fulop, T. Estimated Glomerular Filtration Rate in Chronic Kidney Disease: A Critical Review of Estimate-Based Predictions of Individual Outcomes in Kidney Disease. Toxins 2022, 14, 127. [Google Scholar] [CrossRef]
- Tonneijck, L.; Muskiet, M.H.; Smits, M.M.; van Bommel, E.J.; Heerspink, H.J.; van Raalte, D.H.; Joles, J.A. Glomerular Hyperfiltration in Diabetes: Mechanisms, Clinical Significance, and Treatment. J. Am. Soc. Nephrol. 2017, 28, 1023–1039. [Google Scholar] [CrossRef]
- Nankivell, B.J.; Nankivell, L.; Elder, G.J.; Gruenewald, S.M. How unmeasured muscle mass affects estimated GFR and diagnostic inaccuracy. Eclinicalmedicine 2020, 29–30, 100662. [Google Scholar] [CrossRef] [PubMed]
- Bowling, C.B.; Olsen, M.K.; Berkowitz, T.; Smith, B.; Floyd, B.; Majette, N.; Miles, A.L.; Crowley, S.D.; Wang, V.; Maciejewski, M.L.; et al. Reserve and resilience in CKD: Concept introduction and baseline results from the Physical REsilience Prediction in Advanced REnal Disease (PREPARED) study. BMC Nephrol. 2022, 23, 418. [Google Scholar]
- Bridges, C.C.; Zalups, R.K. The aging kidney and the nephrotoxic effects of mercury. J. Toxicol. Environ. Health-Part B-Crit. Rev. 2017, 20, 55–80. [Google Scholar]
- Kellum, J.A.; Romagnani, P.; Ashuntantang, G.; Ronco, C.; Zarbock, A.; Anders, H.J. Acute kidney injury. Nat. Rev. Dis. Primers 2021, 7, 52. [Google Scholar] [CrossRef]
- Gonzalez, P.; Lozano, P.; Ros, G.; Solano, F. Hyperglycemia and Oxidative Stress: An Integral, Updated and Critical Overview of Their Metabolic Interconnections. Int. J. Mol. Sci. 2023, 24, 9352. [Google Scholar] [CrossRef]
- Wang, N.; Zhang, C. Oxidative Stress: A Culprit in the Progression of Diabetic Kidney Disease. Antioxidants 2024, 13, 455. [Google Scholar] [CrossRef]
- Denimal, D. Antioxidant and Anti-Inflammatory Functions of High-Density Lipoprotein in Type 1 and Type 2 Diabetes. Antioxidants 2023, 13, 57. [Google Scholar] [CrossRef]
- Fan, Z.; Yun, J.; Yu, S.; Yang, Q.; Song, L. Alcohol Consumption Can be a “Double-Edged Sword” for Chronic Kidney Disease Patients. Med. Sci. Monit. 2019, 25, 7059–7072. [Google Scholar]
- Pan, J.; Li, C.; Zhang, J.; Sun, Z.; Yu, X.; Wan, Q.; Ruan, Z.; Wang, W.; Li, Y. Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and diabetic kidney disease in patients with diabetes in the United States: A cross-sectional study. Lipids Health Dis. 2024, 23, 317. [Google Scholar] [CrossRef]
- Zhang, L.; Fan, D.; Zhu, T.; Geng, L.; Gan, L.; Ou, S.; Yin, D. The ratio of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol is associated with diabetic kidney disease: A cross-sectional study. PLoS ONE 2024, 19, e311620. [Google Scholar] [CrossRef]
- Huang, D.; He, Y. Association between non-high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio and macroalbuminuria: Evidence from NHANES 1999–2018. Front. Endocrinol. 2025, 16, 1503780. [Google Scholar]
- Hong, H.; He, Y.; Gong, Z.; Feng, J.; Qu, Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and kidney stones: A cross-sectional study. Lipids Health Dis. 2024, 23, 102. [Google Scholar]
- Du, Y.Z.; Dong, Q.X.; Hu, H.J.; Guo, B.; Li, Y.H.; Zhang, J.; Li, F.C.; Guo, J. A cross-sectional analysis of the relationship between the non-high density to high density lipoprotein cholesterol ratio (NHHR) and kidney stone risk in American adults. Lipids Health Dis. 2024, 23, 158. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 1756) | CKD Group (n = 485) | Non-CKD Group (n = 1271) | χ2/t/z | p |
|---|---|---|---|---|---|
| Sex, n (%) | 0.048 b | 0.827 | |||
| Female | 880 (50.11) | 241 (49.69) | 639 (50.28) | ||
| Male | 876 (49.89) | 244 (50.31) | 632 (49.72) | ||
| BMI, mean ± SD, kg/m2 | 24.76 ± 3.43 | 25.43 ± 3.56 | 24.51 ± 3.35 | −5.06 a | <0.001 *** |
| Age, mean ± SD, years | 57.23 ± 10.15 | 59.09 ± 10.54 | 56.52 ± 9.92 | −4.77 a | <0.001 *** |
| Marriage status | 0.58 b | 0.446 | |||
| Married | 1604 (91.34) | 439 (90.52) | 1165 (91.66) | ||
| Others | 152 (8.66) | 46 (9.48) | 106 (8.34) | ||
| Educational attainment, n (%) | 8.12 b | 0.017 * | |||
| Secondary education or below | 1541 (87.76) | 411 (84.74) | 1130 (88.90) | ||
| Senior high school | 171 (9.74) | 63 (12.99) | 108 (8.50) | ||
| College education or above | 44 (2.50) | 11 (2.27) | 33 (2.60) | ||
| Residence, n (%) | 1.30 b | 0.255 | |||
| Urban | 881 (50.17) | 254 (52.37) | 627 (49.33) | ||
| Rural | 875 (49.83) | 231 (47.63) | 644 (50.67) | ||
| Hypertension, n (%) | 1099 (62.59) | 385 (79.38) | 714 (56.18) | 80.73 b | <0.001 *** |
| TG, median (IQR), mmol/L | 1.60 (1.12–2.42) | 1.87 (1.30–2.94) | 1.51 (1.06–2.26) | 47.47 c | <0.001 *** |
| TC, mean ± SD, mmol/L | 4.65 ± 1.07 | 4.78 ± 1.29 | 4.61 ± 0.97 | −2.64 a | 0.009 ** |
| HDL-C, mean ± SD, mmol/L | 1.25 ± 0.36 | 1.18 ± 0.37 | 1.28 ± 0.35 | 4.96 a | <0.001 *** |
| Non-HDL-C, mean ± SD, mmol/L | 3.41 ± 1.09 | 3.60 ± 1.30 | 3.34 ± 0.99 | −4.07 a | <0.001 *** |
| LDL-C, mean ± SD, mmol/L | 2.73 ± 0.90 | 2.70 ± 1.02 | 2.75 ± 0.85 | 0.98 a | 0.325 |
| HbA1c, mean ± SD, % | 7.27 ± 1.49 | 7.61 ± 1.65 | 7.14 ± 1.40 | −5.43 a | <0.001 *** |
| FPG, mean ± SD, mmol/L | 7.94 ± 2.58 | 8.54 ± 3.11 | 7.72 ± 2.31 | −5.32 a | <0.001 *** |
| SUA, mean ± SD, μmol/L | 5.63 ± 1.59 | 6.01 ± 1.87 | 5.48 ± 1.44 | −5.66 a | <0.001 *** |
| eGFR, mean ± SD, mL/min/1.73 m2 | 88.92 ± 19.03 | 78.76 ± 25.61 | 92.80 ± 14.01 | 11.44 a | <0.001 *** |
| UACR, median (IQR), mg/g | 10.88 (4.83, 28.26) | 62.62 (37.25, 159.50) | 7.18 (3.85, 13.24) | −28.60 c | <0.001 *** |
| Diabetes duration, median(IQR), years | 6.00 (3.00, 10.00) | 7.00 (4.00, 13.00) | 6.00 (3.00, 10.00) | −4.73 c | <0.001 *** |
| Smoking, n (%) | 436 (24.83) | 118 (24.33) | 318 (25.02) | 0.09 b | 0.765 |
| Alcohol drinking, n (%) | 646 (36.79) | 160 (32.99) | 486 (38.24) | 4.16 b | 0.042 * |
| Routine exercise, n (%) | 290 (16.51) | 74 (15.26) | 216 (16.99) | 0.77 b | 0.381 |
| NHHR, median (IQR) | 2.76 (2.02, 3.66) | 2.99 (2.23, 4.04) | 2.66 (1.94, 3.49) | −5.69 c | <0.001 *** |
| Variables | Total (n = 1756) | Q1 (n = 439) | Q2 (n = 439) | Q3 (n = 439) | Q4 (n = 439) | χ2/F | p |
|---|---|---|---|---|---|---|---|
| Sex, n (%) | 6.23 a | 0.101 | |||||
| Female | 880 (50.11) | 219 (49.89) | 231 (52.62) | 231 (52.62) | 199 (45.33) | ||
| Male | 876 (49.89) | 220 (50.11) | 208 (47.38) | 208 (47.38) | 240 (54.67) | ||
| Age, Mean ± SD, years | 57.23 ± 10.15 | 57.87 ± 9.82 | 58.31 ± 9.78 | 57.14 ± 10.13 | 55.59 ± 10.68 | 6.12 b | <0.001 *** |
| Educational attainment, n (%) | 11.59 a | 0.072 | |||||
| Secondary education or lower | 1541 (87.76) | 396 (90.21) | 396 (90.21) | 379 (86.33) | 370 (84.28) | ||
| Senior high school | 171 (9.74) | 32 (7.29) | 36 (8.20) | 48 (10.93) | 55 (12.53) | ||
| College education or above | 44 (2.51) | 11 (2.51) | 7 (1.59) | 12 (2.73) | 14 (3.19) | ||
| Residence, n (%) | 7.64 a | 0.054 | |||||
| Urban | 875 (49.83) | 234 (53.30) | 228 (51.94) | 217 (49.43) | 196 (44.65) | ||
| Rural | 881 (50.17) | 205 (46.70) | 211 (48.06) | 222 (50.57) | 243 (55.35) | ||
| BMI, Mean ± SD, kg/m2 | 24.76 ± 3.43 | 23.41 ± 3.35 | 24.48 ± 3.24 | 25.31 ± 3.17 | 25.84 ± 3.48 | 45.00 b | <0.001 *** |
| HDL-C, mean ± SD, mmol/L | 1.25 ± 0.36 | 1.60 ± 0.36 | 1.32 ± 0.25 | 1.15 ± 0.20 | 0.93 ± 0.20 | 528.98 b | <0.001 *** |
| Non-HDL-C, mean ± SD, mmol/L | 3.41 ± 1.09 | 2.41 ± 0.58 | 3.14 ± 0.61 | 3.64 ± 0.63 | 4.44 ± 1.20 | 501.15 b | <0.001 *** |
| SUA, mean ± SD, μmol/L | 334.65 ± 94.44 | 309.93 ± 89.57 | 329.18 ± 91.91 | 336.56 ± 87.71 | 362.92 ± 100.63 | 24.65 b | <0.001 *** |
| Elevated HbA1c, n (%) | 859 (48.92) | 181 (41.23) | 190 (43.28) | 224 (51.03) | 264 (60.14) | 38.86 a | <0.001 *** |
| Elevated FPG, n (%) | 989 (56.32) | 229 (52.16) | 226 (51.48) | 259 (59.00) | 275 (62.64) | 15.67 a | 0.001 ** |
| Hypertension, n (%) | 1099 (62.59) | 237 (53.99) | 271 (61.73) | 285 (64.92) | 306 (69.70) | 24.52 a | <0.001 *** |
| Smoking, n (%) | 436 (24.83) | 96 (21.87) | 93 (21.18) | 102 (23.23) | 145 (33.03) | 21.60 a | <0.001 *** |
| Alcohol drinking, n (%) | 646 (36.79) | 174 (39.64) | 155 (35.31) | 160 (36.45) | 157 (35.76) | 2.16 a | 0.539 |
| Routine exercise, n (%) | 290 (16.51) | 65 (14.81) | 74 (16.86) | 80 (18.22) | 71 (16.17) | 1.93 a | 0.586 |
| Diabetes duration, median (IQR), years | 6.00 (3.00, 10.00) | 7.00 (4.00, 11.00) | 6.00 (3.00, 10.00) | 6.00 (3.00, 10.00) | 5.00 (2.00, 10.00) | 11.10 c | 0.011 * |
| UACR, median (IQR), mg/g | 10.88 (4.83, 28.26) | 9.80 (4.26, 20.81) | 10.47 (4.76, 25.26) | 10.66 (4.95, 31.64) | 12.69 (5.40, 43.10) | 18.09 c | <0.001 *** |
| eGFR, mean ± SD, mL/min/1.73 m2 | 88.92 ± 19.03 | 90.18 ± 16.97 | 88.20 ± 18.87 | 89.65 ± 18.50 | 87.66 ± 21.47 | 1.71 b | 0.162 |
| CKD, n (%) | 485 (27.62) | 89 (20.27) | 113 (25.74) | 123 (28.02) | 160 (36.45) | 29.77 a | <0.001 *** |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| NHHR per SD | 1.34 (1.21–1.49) | <0.001 *** | 1.40 (1.26–1.56) | <0.001 *** | 1.23 (1.09–1.37) | <0.001 *** |
| NHHR quartile | ||||||
| Q1 (n = 439) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | |||
| Q2 (n = 439) | 1.36 (0.99–1.87) | 0.055 | 1.37 (0.99–1.88) | 0.056 | 1.29 (0.92–1.79) | 0.135 |
| Q3 (n = 439) | 1.53 (1.12–2.09) | 0.008 ** | 1.59 (1.16–2.18) | 0.004 ** | 1.31 (0.94–1.83) | 0.110 |
| Q4 (n = 439) | 2.26 (1.67–3.05) | <0.001 *** | 2.45 (1.80–3.33) | <0.001 *** | 1.87 (1.34–2.60) | <0.001 *** |
| p for trend | 1.32 (1.19–1.46) | <0.001 *** | 1.36 (1.23–1.51) | <0.001 *** | 1.21 (1.08–1.36) | 0.001 ** |
| Female | ||||||
| NHHR per SD | 1.38 (1.19–1.60) | <0.001 *** | 1.43 (1.23–1.66) | <0.001 *** | 1.22 (1.05–1.45) | 0.011 * |
| NHHR quartile | ||||||
| Q1 (n = 220) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | |||
| Q2 (n = 220) | 1.11 (0.71–1.73) | 0.651 | 1.17 (0.75–1.84) | 0.495 | 0.95 (0.59–1.52) | 0.819 |
| Q3 (n = 220) | 1.16 (0.75–1.81) | 0.501 | 1.19 (0.76–1.86) | 0.452 | 1.08 (0.68–1.72) | 0.736 |
| Q4 (n = 220) | 2.16 (1.42–3.27) | <0.001 *** | 2.32 (1.51–3.55) | <0.001 *** | 1.77 (1.13–2.79) | 0.013 * |
| p for trend | 1.34 (1.15–1.56) | <0.001 *** | 1.37 (1.18–1.61) | <0.001 *** | 1.24 (1.05–1.47) | 0.010 * |
| Male | ||||||
| NHHR per SD | 1.32 (1.14–1.53) | <0.001 *** | 1.39 (1.19–1.61) | <0.001 *** | 1.25 (1.03–1.47) | 0.008 ** |
| NHHR quartile | ||||||
| Q1 (n = 219) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | |||
| Q2 (n = 219) | 1.57 (1.00–2.49) | 0.051 | 1.58 (1.00–2.50) | 0.050 | 1.62 (1.00–2.64) | 0.050 |
| Q3 (n = 219) | 2.06 (1.32–3.12) | 0.002 ** | 2.14 (1.37–3.36) | <0.001 *** | 1.86 (1.15–3.03) | 0.012 * |
| Q4 (n = 219) | 2.48 (1.59–3.85) | <0.001 *** | 2.75 (1.76–4.31) | <0.001 *** | 2.19 (1.34–3.60) | 0.002 ** |
| p for trend | 1.33 (1.16–1.52) | <0.001 *** | 1.38 (1.20–1.58) | <0.001 *** | 1.27 (1.08–1.48) | 0.003 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, X.; Liang, M.; Zhang, J.; Xu, C.; Chen, L.; Hu, R.; Zhong, J. The Non-High-Density Lipoprotein Cholesterol (Non-HDL-C) to HDL-C Ratio (NHHR) and Its Association with Chronic Kidney Disease in Chinese Adults with Type 2 Diabetes: A Preliminary Study. Nutrients 2025, 17, 1125. https://doi.org/10.3390/nu17071125
Chen X, Liang M, Zhang J, Xu C, Chen L, Hu R, Zhong J. The Non-High-Density Lipoprotein Cholesterol (Non-HDL-C) to HDL-C Ratio (NHHR) and Its Association with Chronic Kidney Disease in Chinese Adults with Type 2 Diabetes: A Preliminary Study. Nutrients. 2025; 17(7):1125. https://doi.org/10.3390/nu17071125
Chicago/Turabian StyleChen, Xiangyu, Mingbin Liang, Jie Zhang, Chunxiao Xu, Lijin Chen, Ruying Hu, and Jieming Zhong. 2025. "The Non-High-Density Lipoprotein Cholesterol (Non-HDL-C) to HDL-C Ratio (NHHR) and Its Association with Chronic Kidney Disease in Chinese Adults with Type 2 Diabetes: A Preliminary Study" Nutrients 17, no. 7: 1125. https://doi.org/10.3390/nu17071125
APA StyleChen, X., Liang, M., Zhang, J., Xu, C., Chen, L., Hu, R., & Zhong, J. (2025). The Non-High-Density Lipoprotein Cholesterol (Non-HDL-C) to HDL-C Ratio (NHHR) and Its Association with Chronic Kidney Disease in Chinese Adults with Type 2 Diabetes: A Preliminary Study. Nutrients, 17(7), 1125. https://doi.org/10.3390/nu17071125