
Characterization of Beverage Viscosity Based on the International Dysphagia Diet Standardisation Initiative and Its Correspondence to the Japanese Dysphagia Diet 2021



Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Creation
2.2. Measuring Instruments and Conditions
- Viscometry: The viscosity of each sample was measured using an E-type simple viscometer (JOVITM, Neutri Corporation, Mie, Japan). The shear rate was 50 s−1, and the maximum viscosity of measurement was 500 mPa·s. For the measurement, two viscometers were prepared, each was calibrated, and two inspectors measured one liquid sample simultaneously.
- IDDSI flow test: A total of 10 mL of the sample liquid was injected into a funnel officially approved by the IDDSI and commercially available. Then, the funnel tip was opened, the liquid was dropped for 10 s, and the funnel tip was closed to measure the residual volume (mL) [26]. The liquid was then classified based on IDDSI levels 0–3. Two inspectors simultaneously measured one liquid sample using two funnels.
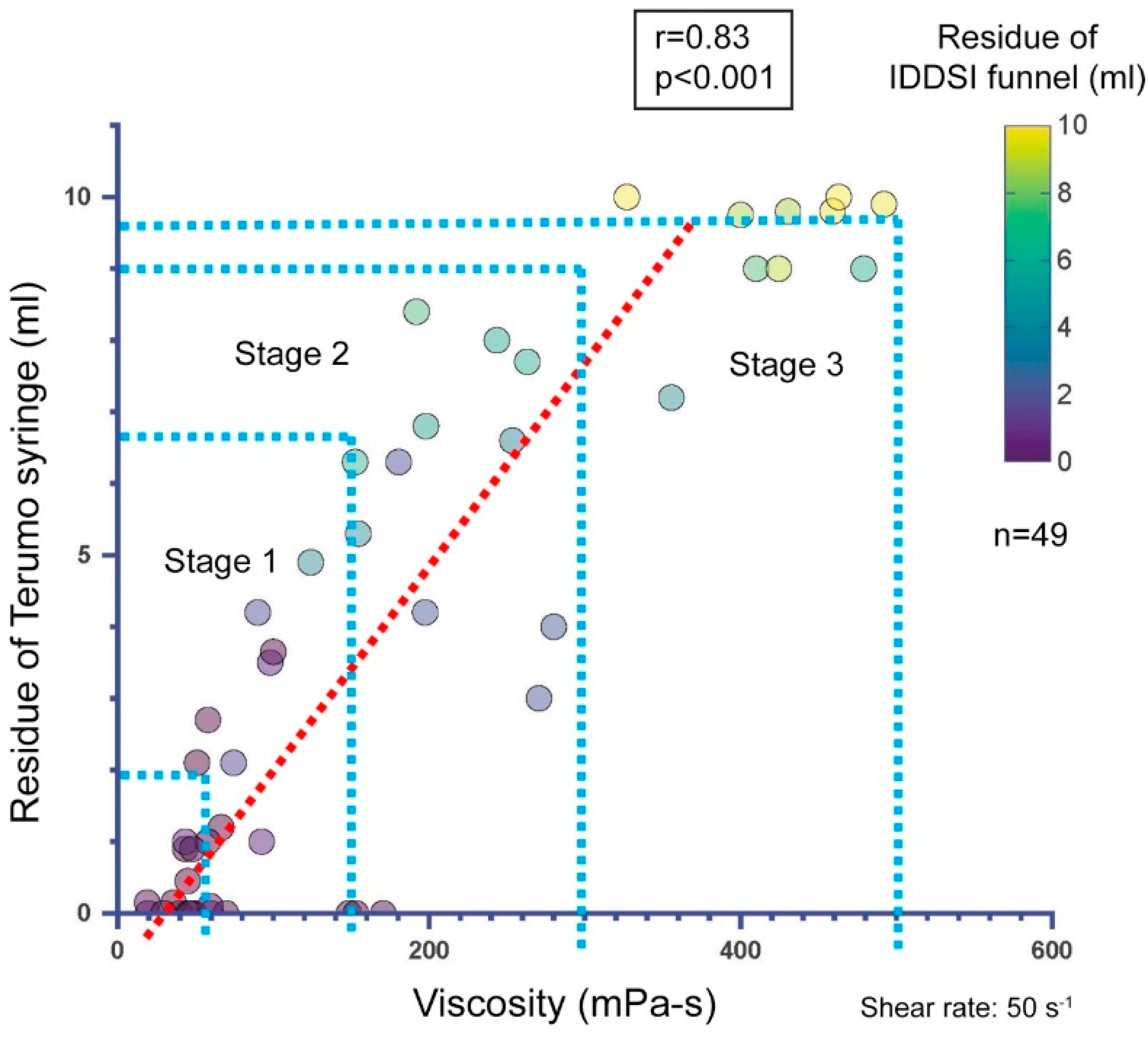
- JDD syringe test: Using a Terumo 10 mL syringe, which was officially adopted in JDD2021, 10 mL of the sample liquid was injected, the syringe tip was opened, the liquid was dropped for 10 s, and the syringe tip was closed to measure the residual volume (mL) [27]. The liquid was then classified according to the JDD2021 classification [13,23]. In JDD2021, the thickness of the liquids is classified into three categories, stage 1 (mildly thick), stage 2 (moderately thick), and stage 3 (extremely thick). Liquids thinner than stage 1 are considered inappropriate for patients with dysphagia. Two examiners measured each liquid sample simultaneously using two syringes.
2.3. Measurement Process
- The thickened beverages were mixed to ensure uniformity and adjusted according to the method indicated in Section 2.2.
- The prepared samples were measured twice using two separate viscometers, and the viscosity was recorded in mPa·s.
- The IDDSI flow test and JDD syringe test were performed using samples prepared under the same conditions as the viscosity measurement to avoid time differences and temperature changes from preparation to measurement, and the residual volume (mL) of each was recorded. Each sample was measured twice.
- The average value of the results (two measurements) was calculated for each sample.
2.4. Statistical Analysis
- Descriptive statistics: Mean viscosities were calculated for each beverage sample (Table 2). The maximum, minimum, and median viscosities were recorded. All samples were classified using the JDD syringe test and the IDDSI flow test. The distribution of viscosity and residual volume are shown in the descriptive statistics. Scatter plots show the distributions of the viscosity measurement and the residual volume of the JDD syringe test using the Terumo syringe (Figure 1), the residual volume of the IDDSI flow test using the IDDSI funnel (Figure 2), and the distribution of the IDDSI funnel residue and the Terumo syringe residue (Figure 3). The matching ratios between the results from the viscometer and the JDD classification obtained from the value in the Terumo syringe test were calculated for each JDD stage.
- 2.
- Correlation analysis: Using Spearman’s rank correlation analysis, we evaluated the correlation between residual volumes and viscosity measurements obtained through the IDDSI flow test and the JDD syringe test. The correlation between the residual volume of the IDDSI funnel and that of the Terumo syringe was also evaluated and correlation coefficients were calculated.
- 3.
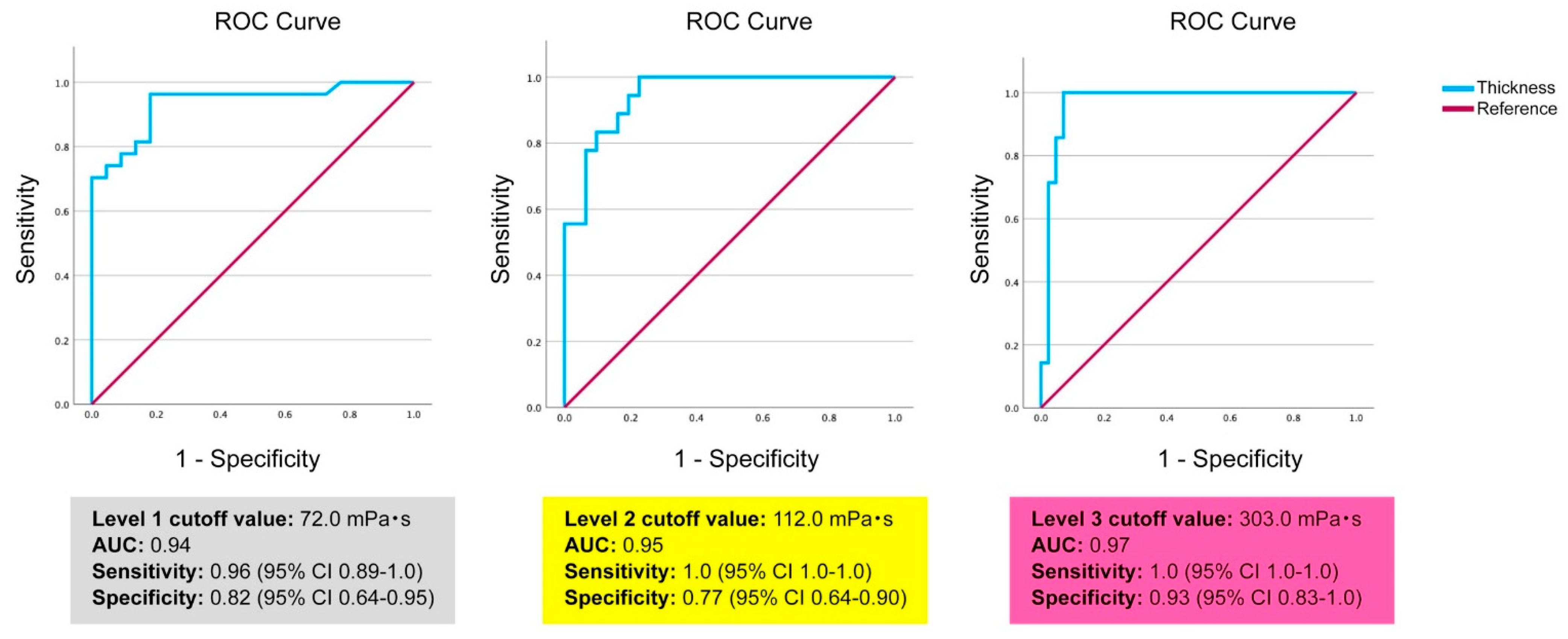
- Receiver operating characteristic (ROC) analysis: This analysis was performed to determine the viscosity cutoff value for each IDDSI level.
- 4.
- Multiple regression analysis: This analysis was performed using viscosity measurements (log-transformed) as the dependent variable and IDDSI funnel residue (residual volume), fat content of the beverage, sodium content, pH, and static time for settling as independent variables to determine the extent to which the beverages’ nature influenced the determination of viscosity and IDDSI funnel residue [22,23]. The static time was used as a ranking variable, with 1 being 5 min of static time, 2 being 10 min of static time, and 0 being no settling time.
3. Results
3.1. Descriptive Statistics
3.2. Correlation Analysis
3.3. ROC Analysis
3.4. Multiple Regression Analysis
4. Discussion
4.1. IDDSI Level Viscosity Characteristics
4.2. Correspondence Between the JDD2021 and IDDSI
- IDDSI level 0 (0–72 mPa·s, funnel residue 0.0–1.0 mL): Corresponds to liquids thinner than JDD stage 1 and some stage 1 liquids.
- IDDSI level 1 (72–112 mPa·s, funnel residue 1.0–4.0 mL): Corresponds to JDD stage 1 (mildly thick).
- IDDSI level 2 (112–303 mPa·s, funnel residue 4.0–8.0 mL): Spans across JDD stage 1 (mildly thick) and portions of stage 2 (moderately thick).
- IDDSI level 3 (>303 mPa·s, funnel residue 8.0–10.0 mL): Closely corresponds to JDD stage 3 (extremely thick).
4.3. Practical Impact on Dysphagia Management in Clinics or Facilities
- Refinement of clinical assessment and prescription: The clarified viscosity correspondence table enables clinicians to accurately convert patient assessment results and prescription contents between different classification systems. This facilitates communication during international hospital transfers or among multinational staff familiar with different systems. Notably for patients with severe dysphagia (requiring high-viscosity thickeners), consistent and safe care can be provided across systems.
- Individualized approaches based on beverage characteristics: The discovery that beverage characteristics such as fat content and static time influence measurement values demonstrates the need for individualized thickener adjustments in clinical settings. Even with identical thickener concentrations, viscosity is dependent on the beverage type, providing scientific evidence for the individual adjustment of patients’ preferred beverages. This contributes to optimizing patient meal satisfaction and nutritional intake.
- Enhanced risk assessment: The finding that flow measurement accuracy varies by viscosity range necessitates a more refined aspiration risk assessment, particularly in the intermediate viscosity range (IDDSI level 2 or JDD stages 1–2). Clinicians can exercise more careful interpretation of measurements in this range and, when necessary, combine multiple measurement methods to achieve a more accurate assessment of risk and to aid in planning care.
- Streamlined interfacility and international collaboration: The established conversion framework facilitates information sharing and continuity of care between facilities using different classification systems. This provides a practical tool for ensuring continuity of safe care, especially in international medical institutions or in facilities with patients and staff of several different nationalities.
4.4. Potential for Improvement in Standardization Processes
- Need for an integrated approach for viscosity measurement: Current standardization processes do not adequately consider fundamental differences between systems. While the IDDSI does not specify viscosity values, the JDD2021 defines specific viscosity ranges. Future standardization would benefit from an integrated approach combining flow measurements and absolute viscosity values to enhance scientific precision while respecting different cultural backgrounds and clinical traditions.
- Introduction of correction factors based on beverage characteristics: Results of multiple regression analysis suggest the value of introducing correction factors based on beverage characteristics (fat content, sodium content, static time, etc.) into standardization processes. This would improve measurement consistency across different beverage types, enabling more reliable classification.
- Development of evaluation methods optimized for specific viscosity ranges: Our research demonstrated that measurement accuracy varies for each viscosity range. Future standardization requires development and validation of assessment methods specialized for each viscosity range. New measurement protocols and equipment to improve reliability in the moderate viscosity range are particularly desirable.
- Flexible framework reflecting cultural diversity and clinical realities: International standardization must respect differences in cultural eating habits and medical resources. Future improvements should focus on building flexible frameworks that allow for regional adaptations while maintaining scientific consistency. For example, supplementary guidelines should be developed for region-specific beverages and foods.
- Establishment of verification systems based on clinical outcomes: The final evaluation of standardization processes should be based on clinical outcomes. An international verification system to systematically assess how different classification systems affect actual aspiration rates, pneumonia incidence, nutritional status, and patient satisfaction is desirable.
4.5. Reliability and Limitations of Measurement Methods
4.6. Research Limitations and Future Directions
4.7. Additional Research Needed for International Standardization
- Multinational collaborative validation studies: Large-scale collaborative research involving research institutions representing multiple countries and regions is necessary. This would identify regional differences in measurement methods and interpretation and allow for the development of universally applicable validation protocols. The cross-validation of measurements between regions with different classification systems and clinical standards, such as Japan, Europe, North America, and Australia, is of particular importance.
- Systematic comparison of diverse thickener types: While this study focused on xanthan-based thickeners, systematic comparisons of the flow characteristics of thickener types used worldwide, including starch-based and guar gum-based products, is needed. This would enable the development of algorithms to predict and correct for variations in measurements due to thickener type.
- Patient-centered outcome research: Long-term prospective studies evaluating how different classification systems and viscosity levels affect real-world patient outcomes (aspiration pneumonia rates, nutritional status, QOL, patient satisfaction, etc.) are needed. It is especially important to clarify how subtle viscosity differences near system conversion points affect clinical results.
- Analysis of cultural and dietary habit influences: Research investigating how regional food cultures and beverage preferences affect viscosity perception and optimal viscosity levels is necessary. It has been suggested that the effect of adding a thickening agent to alcoholic and other flavored beverages could be evaluated. This would enable the development of standardization approaches that maintain scientific consistency while respecting cultural diversity.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IDDSI | International Dysphagia Diet Standardisation Initiative |
| JDD2021 | Japanese Dysphagia Diet 2021 |
| TMD | Texture-modified diet |
| JDD | Japanese Dysphagia Diet |
| ROC | Receiver Operation Characteristic |
| AUC | Area Under the Curve |
References
- Speyer, R.; Cordier, R.; Farneti, D.; Nascimento, W.; Pilz, W.; Verin, E.; Walshe, M.; Woisard, V. White paper by the European society for swallowing disorders: Screening and non-instrumental assessment for dysphagia in adults. Dysphagia 2022, 37, 333–349. [Google Scholar] [CrossRef]
- Jotz, G.P. Dysphagia: An overview. Int. Arch. Otorhinolaryngol. 2023, 27, e377–e379. [Google Scholar] [CrossRef]
- Yang, S.; Park, J.W.; Min, K.; Lee, Y.S.; Song, Y.J.; Choi, S.H.; Kim, D.Y.; Lee, S.H.; Yang, H.S.; Cha, W.; et al. Clinical practice guidelines for oropharyngeal dysphagia. Ann. Rehabil. Med. 2023, 47, S1–S26. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; McRae, J.; Clunie, G.; Gillivan-Murphy, P.; Inamoto, Y.; Kalf, H.; Pillay, M.; Pownall, S.; Ratcliffe, P.; Richard, T.; et al. An International Commentary on dysphagia and dysphonia during the COVID-19 pandemic. Dysphagia 2022, 37, 1349–1374. [Google Scholar] [CrossRef] [PubMed]
- Thiyagalingam, S.; Kulinski, A.E.; Thorsteinsdottir, B.; Shindelar, K.L.; Takahashi, P.Y. Dysphagia in older adults. Mayo Clin. Proc. 2021, 96, 488–497. [Google Scholar] [CrossRef]
- Doan, T.N.; Ho, W.C.; Wang, L.H.; Chang, F.C.; Nhu, N.T.; Chou, L.W. Prevalence and methods for assessment of oropharyngeal dysphagia in older adults: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 2605. [Google Scholar] [CrossRef] [PubMed]
- Nakao-Kato, M.; Rathore, F.A. An overview of the management and rehabilitation of dysphagia. J. Pak. Med. Assoc. 2023, 73, 1749–1752. [Google Scholar] [CrossRef]
- Adkins, C.; Takakura, W.; Spiegel, B.M.R.; Lu, M.; Vera-Llonch, M.; Williams, J.; Almario, C.V. Prevalence and characteristics of dysphagia based on a population-based survey. Clin. Gastroenterol. Hepatol. 2020, 18, 1970–1979.e2. [Google Scholar] [CrossRef]
- Inui, A.; Takahashi, I.; Kurauchi, S.; Soma, Y.; Oyama, T.; Tamura, Y.; Noguchi, T.; Murashita, K.; Nakaji, S.; Kobayashi, W. Oral conditions and dysphagia in Japanese, community-dwelling middle- and older- aged adults, independent in daily living. Clin. Interv. Aging 2017, 12, 515–521. [Google Scholar] [CrossRef]
- Roberts, H.; Lambert, K.; Walton, K. The prevalence of dysphagia in individuals living in residential aged care facilities: A systematic review and meta-analysis. Healthcare 2024, 12, 649. [Google Scholar] [CrossRef]
- Mateos-Nozal, J.; Montero-Errasquín, B.; Sánchez García, E.; Romero Rodríguez, E.; Cruz-Jentoft, A.J. High prevalence of oropharyngeal dysphagia in acutely hospitalized patients aged 80 years and older. J. Am. Med. Dir. Assoc. 2020, 21, 2008–2011. [Google Scholar] [CrossRef] [PubMed]
- Cichero, J.A.Y.; Lam, P.; Steele, C.M.; Hanson, B.; Chen, J.; Dantas, R.O.; Duivestein, J.; Kayashita, J.; Lecko, C.; Murray, J.; et al. Development of international terminology and definitions for texture-modified foods and thickened fluids used in dysphagia management: The IDDSI framework. Dysphagia 2017, 32, 293–314. [Google Scholar] [CrossRef]
- Dysphagia Diet Committee of the Japanese Society of Dysphagia Rehabilitation; Kayashita, J.; Fujishima, I.; Fujitani, J.; Hironaka, S.; Kojo, A.; Mizukami, M.; Senda, N.; Moriwaki, M.; Watanabe, E. The Japanese dysphagia diet of 2021 by the Japanese society of dysphagia rehabilitation. Jpn. J. Compr. Rehabil. Sci. Internet 2022, 13, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Cichero, J.A.Y.; Lam, P.T.L.; Chen, J.; Dantas, R.O.; Duivestein, J.; Hanson, B.; Kayashita, J.; Pillay, M.; Riquelme, L.F.; Steele, C.M.; et al. Release of updated International Dysphagia Diet Standardisation Initiative Framework (IDDSI 2.0). J. Texture Stud. 2020, 51, 195–196. [Google Scholar] [CrossRef]
- Dahlström, S.; Henning, I.; McGreevy, J.; Bergström, L. How valid and reliable is the International Dysphagia Diet Standardisation Initiative (IDDSI) when translated into another language? Dysphagia 2023, 38, 667–675. [Google Scholar] [CrossRef]
- Yoon, J.A. Update of guidelines: International dysphagia diet standardization initiative 2019. J. Korean Dysphagia Soc. 2022, 12, 79–84. [Google Scholar] [CrossRef]
- Watanabe, E.; Yamagata, Y.; Fujitani, J.; Fujishima, I.; Takahashi, K.; Uyama, R.; Ogoshi, H.; Kojo, A.; Maeda, H.; Ueda, K.; et al. The criteria of thickened liquid for dysphagia management in Japan. Dysphagia 2018, 33, 26–32. [Google Scholar] [CrossRef]
- Giudice, V.; Downie, L.; Lindsay, F.; Ryan, E.; MacKay, A. Improving the communication of dysphagia recommendations in the inpatient setting. Clin. Nutr. ESPEN 2020, 35, 242. [Google Scholar] [CrossRef]
- Lam, P.; Soenke, S.; Rizwana, Z.; Cichero, J. The international dysphagia diet standardisation initiative (IDDSI) framework: The kempen pilot. Br. J. Neurosci. Nurs. 2017, 13, S18–S26. [Google Scholar] [CrossRef]
- Jukic Peladic, N.; Orlandoni, P.; Di Rosa, M.; Giulioni, G.; Bartoloni, L.; Venturini, C. Multidisciplinary assessment and individualized nutritional management of dysphagia in older outpatients. Nutrients 2023, 15, 1103. [Google Scholar] [CrossRef]
- Cichero, J.A.Y. Age-Related Changes to Eating and Swallowing Impact Frailty: Aspiration, Choking Risk, Modified Food Texture and Autonomy of Choice. Geriatrics 2018, 3, 69. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Chan, K.M.K.; Wong, T.T.; Tang, H.W.; Chung, H.Y.; Kwan, H.S. Quantitative textural and rheological data on different levels of texture-modified food and thickened liquids classified using the International Dysphagia Diet Standardisation Initiative (IDDSI) guideline. Foods 2023, 12, 3765. [Google Scholar] [CrossRef]
- Wang, X.; Rong, L.; Shen, M.; Yu, Q.; Chen, Y.; Li, J.; Xie, J. Rheology, texture and swallowing characteristics of a texture-modified dysphagia food prepared using common supplementary materials. Foods 2023, 12, 2287. [Google Scholar] [CrossRef]
- Kayashita, J. A comparison of viscosity classifications between the Japanese dysphagia diet 2013 criteria and the international dysphagia diet standardisation initiative. EC Nutr. 2017, 10, 185–194. [Google Scholar]
- Sato, M.; Yamagata, Y.; Kayashita, J. Study of syringe test as a simple evaluation method for thickened liquid. Jpn. J. Dysphagia Rehabil. 2021, 21, 102–113. (In Japanese) [Google Scholar]
- Hanson, B.; Jamshidi, R.; Redfearn, A.; Begley, R.; Steele, C.M. Experimental and computational investigation of the IDDSI flow test of liquids used in dysphagia management. Ann. Biomed. Eng. 2019, 47, 2296–2307. [Google Scholar] [CrossRef] [PubMed]
- Takata, N.; Yamagata, Y.; Kayashita, J. Conference Report. 2017. Available online: https://api.semanticscholar.org/CorpusID:212439199 (accessed on 16 February 2025).
- Barbon, C.E.A.; Steele, C.M. Thickened liquids for dysphagia management: A current review of the measurement of liquid flow. Curr. Phys. Med. Rehabil. Rep. 2018, 6, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Vergara, J.; Teixeira, H.S.; de Souza, C.M.; Ataide, J.A.; de Souza Ferraz, F.; Mazzola, P.G.; Mourão, L.F. Flow test by the International Dysphagia Diet Standardization Initiative reveals distinct viscosity parameters of three thickening agents. J. Food Sci. Technol. 2022, 59, 3627–3633. [Google Scholar] [CrossRef]
- Jeong, Y.; Lim, W.; Yoo, B. Relationship between syringe flow measurements and viscosity of nectar-thick beverages for dysphagia management. Foods 2021, 10, 1981. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Thickening Agent (g) Beverages | Mixing | 30 mPa·s | 50 mPa·s | 100 mPa·s | 200 mPa·s | 400 mPa·s | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mixing Time (sec) [1] | Static Time (min) | Mixing Time (sec) [2] | ||||||||
| 30 | 5 | 10 | 30 | B | C | D | F | H | ||
| 1 | Mineral water | X | 0.3 | 0.4 | 0.5 | 1.0 | 2.0 | |||
| 2 | Tea (Oi Ocha™) | X | 0.3 | 0.4 | 0.5 | 1.0 | 1.6 | |||
| 3 | Coffee (Boss™ Black Coffee unsweetened) | X | 0.3 | 0.4 | 0.5 | 1.0 | 1.6 | |||
| 4 | Black tea (Afternoon tea™, straight, unsweetened) | X | 0.3 | 0.4 | 0.5 | 1.0 | 1.6 | |||
| 5 | Oolong tea | X | 0.3 | 0.4 | 0.5 | 1.0 | 1.8 | |||
| 6 | 100% Orange juice (Pom Juice) | X | X | X | 0.5 | 0.6 | 0.7 | 1.2 | 1.6 | |
| 7 | Sports drink (Pocari Sweat™) | X | X | X | 0.5 | 0.6 | 0.7 | 1.2 | 1.7 | |
| 8 | Milk (Meiji Oishii Gyunyu™) | X | X | X | 0.5 | 0.6 | 0.7 | 1.2 | 2.0 | |
| 9 | Tomato juice | X | X | X | - | 0.5 | 0.6 | 0.7 | 1.2 | |
| 10 | Lactic acid beverage (Yakult™) | X | X | X | 0.5 | 0.6 | 0.7 | 1.2 | 1.8 | |
| № | Target viscosity (mPa·s) | 30 | 50 | 100 | 200 | 400 |
| Solution n = 2; Average Viscosity (mPa·s) | B | C | D | F | H | |
| 1 | MINERAL water | 43.5 | 58 | 90 | 192.5 | 327.5 |
| 2 | Tea (Oi Ocha™) | 19.5 | 49 | 66.5 | 253.5 | 400 |
| 3 | Coffee (Boss™ Black Coffee unsweetened) | 36 | 58 | 51 | 180.5 | 410 |
| 4 | Black tea (Afternoon tea™, straight, unsweetened) | 45.5 | 48 | 98 | 263 | 430.5 |
| 5 | Oolong tea (Suntory cooperation) | 29.5 | 45 | 100 | 243.5 | 553.5 |
| 6 | 100% orange juice | 40 | 60 | 69.5 | 197.5 | 355.5 |
| 7 | Sports Drink (Pocari Sweat™) | 47 | 59.5 | 92.5 | 280 | 481 |
| 8 | Milk (Meiji Oishii Gyunyu™) | 19 | 43.5 | 74.5 | 152.5 | 479 |
| 9 | Tomato juice | - | 124 | 154.5 | 198 | 424.5 |
| 10 | lactic acid beverage (Yakult™) | 148.5 | 153 | 170.5 | 270.5 | 463 |
| Viscosity (mPa·s) | Definition of JDD2021 | JDD Syringe Test Using the Terumo Syringe Degree of Agreement with Results |
|---|---|---|
| <50 | Thinner than Stage 1 | 92% |
| 50–150 | Stage 1 (Mildly thick) | 46% |
| 150–300 | Stage 2 (Moderately thick) | 23% |
| 300–500 | Stage 3 (Extremely Thick) | 40% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakao-Kato, M.; Takahashi, A.; Magara, J. Characterization of Beverage Viscosity Based on the International Dysphagia Diet Standardisation Initiative and Its Correspondence to the Japanese Dysphagia Diet 2021. Nutrients 2025, 17, 1051. https://doi.org/10.3390/nu17061051
Nakao-Kato M, Takahashi A, Magara J. Characterization of Beverage Viscosity Based on the International Dysphagia Diet Standardisation Initiative and Its Correspondence to the Japanese Dysphagia Diet 2021. Nutrients. 2025; 17(6):1051. https://doi.org/10.3390/nu17061051
Chicago/Turabian StyleNakao-Kato, Mari, Aya Takahashi, and Jin Magara. 2025. "Characterization of Beverage Viscosity Based on the International Dysphagia Diet Standardisation Initiative and Its Correspondence to the Japanese Dysphagia Diet 2021" Nutrients 17, no. 6: 1051. https://doi.org/10.3390/nu17061051
APA StyleNakao-Kato, M., Takahashi, A., & Magara, J. (2025). Characterization of Beverage Viscosity Based on the International Dysphagia Diet Standardisation Initiative and Its Correspondence to the Japanese Dysphagia Diet 2021. Nutrients, 17(6), 1051. https://doi.org/10.3390/nu17061051