
The Influence of Dietary Patterns on Polycystic Ovary Syndrome Management in Women: A Review of Randomized Controlled Trials with and Without an Isocaloric Dietary Design


Abstract
1. Introduction
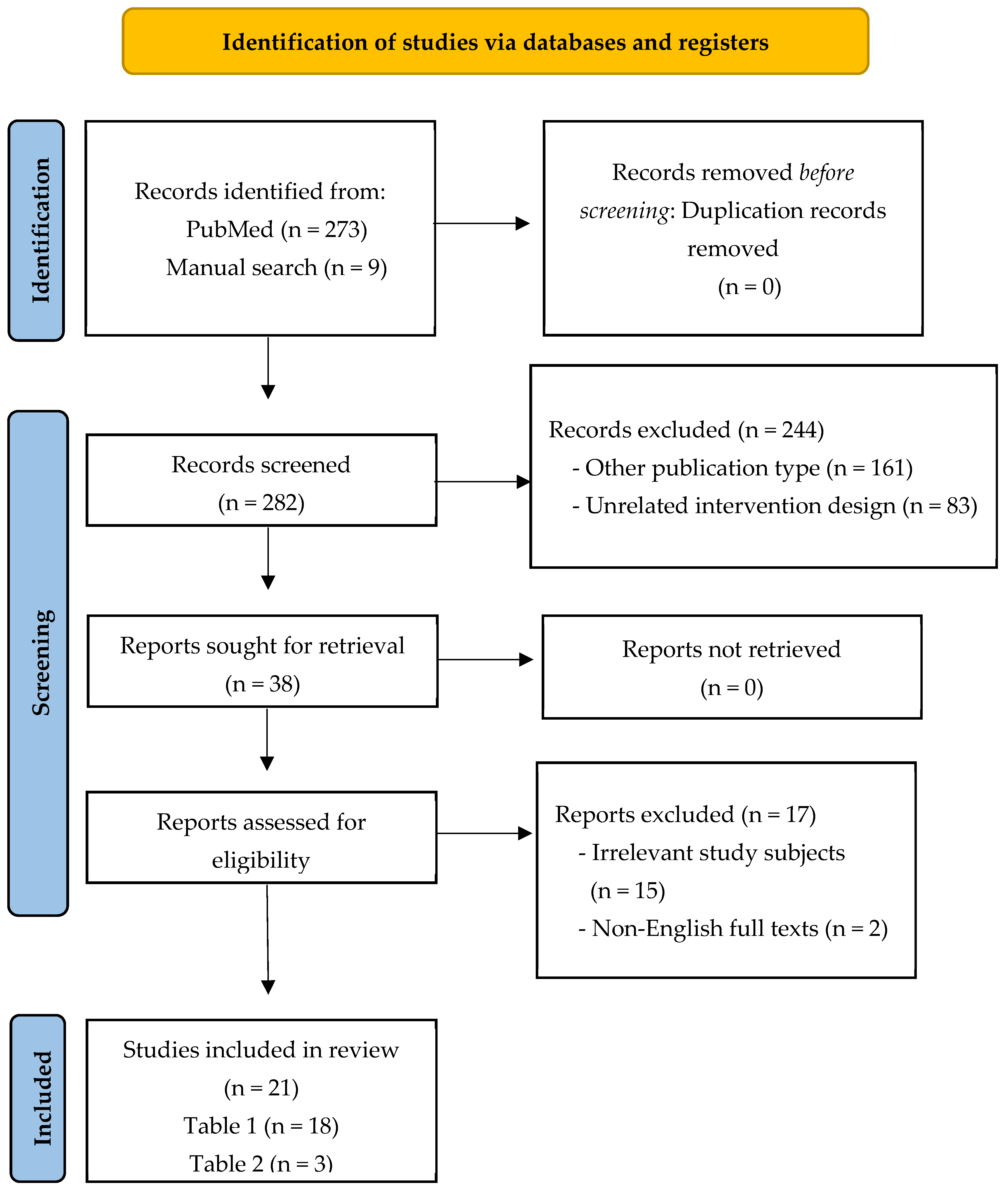
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Results
3.1. Calorie-Restricted Diet
3.1.1. DASH Diet
3.1.2. Ketogenic Diet
3.1.3. Low-Carbohydrate Diet
3.1.4. Low-GI Diet
3.1.5. High-Protein Diet
3.1.6. Low-Calorie Diet
3.2. Non-Calorie-Restricted Diet
3.2.1. Low-Carbohydrate Diet
3.2.2. Low-GI Diet
3.2.3. High-Protein Diet
4. Discussion
4.1. Calorie-Restricted DASH Diet
4.2. Calorie-Restricted Ketogenic Diet
4.3. Low-Carbohydrate Diet
4.4. Low-GI Diet
4.5. High-Protein Diet
4.6. Low-Calorie Diet
4.7. Other Interventions in Women with PCOS and Without PCOS
4.8. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| A4 | androstenedione |
| AIRg | acute insulin response to glucose |
| AUC | area under the curve |
| BMI | body mass index |
| BW | body weight |
| CG | control group |
| CI | confidence interval |
| DASH | Dietary Approaches to Stop Hypertension |
| DBP | diastolic blood pressure |
| DHEAS | dehydroepiandrosterone-sulfate |
| ED | estradiol |
| FAI | free androgen index |
| FBG | fasting blood glucose |
| FBI | fasting blood insulin |
| FFA | free fatty acids |
| FFM | fat-free mass |
| FSH | follicle-stimulating hormone |
| GI | glycemic index |
| GL | glycemic load |
| GLP-1 | glucagon-like peptide-1 |
| HbA1c | hemoglobin A1c |
| HC | hip circumference |
| HDL-C | high-density lipoprotein cholesterol |
| HOMA2-IS | updated homeostasis model assessment of insulin sensitivity |
| HOMA-B | homeostasis model assessment of beta-cell function |
| HOMA-IR | homeostasis model assessment of insulin resistance |
| hs-CRP | high sensitivity C-reactive protein |
| IL-6 | interleukin-6 |
| InG | intervention group |
| KD | ketogenic diet |
| LBM | lean body mass |
| LDL-C | low-density lipoprotein cholesterol |
| LH | luteinizing hormone |
| MD | mean difference |
| MDA | malondialdehyde |
| MED | Mediterranean |
| MUFA | monounsaturated fatty acid |
| NPG | non-polycystic ovary syndrome group |
| OGTT | oral glucose tolerance test |
| PBF | percent of body fat |
| PCOS | polycystic ovary syndrome |
| PG | polycystic ovary syndrome group |
| PhiB | basal beta-cell response to glucose |
| PhiD | dynamic beta-cell response to glucose |
| PUFA | polyunsaturated fatty acid |
| QUICKI | quantitative insulin sensitivity check index |
| RCT | randomized controlled trial |
| SBP | systolic blood pressure |
| SFA | saturated fatty acid |
| SHBG | sex hormone binding globulin |
| Si | insulin sensitivity |
| SMD | standardized mean difference |
| T2DM | type 2 diabetes mellitus |
| TFM | total fat mass |
| WMD | weighted mean difference |
References
- McCartney, C.R.; Marshall, J.C. Clinical Practice. Polycystic Ovary Syndrome. N. Engl. J. Med. 2016, 375, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, K.M.; Dokras, A.; Piltonen, T. Update on PCOS: Consequences, Challenges, and Guiding Treatment. J. Clin. Endocrinol. Metab. 2021, 106, e1071–e1083. [Google Scholar] [CrossRef]
- Wild, R.A.; Carmina, E.; Diamanti-Kandarakis, E.; Dokras, A.; Escobar-Morreale, H.F.; Futterweit, W.; Lobo, R.; Norman, R.J.; Talbott, E.; Dumesic, D.A. Assessment of cardiovascular risk and prevention of cardiovascular disease in women with the polycystic ovary syndrome: A consensus statement by the Androgen Excess and Polycystic Ovary Syndrome (AE-PCOS) Society. J. Clin. Endocrinol. Metab. 2010, 95, 2038–2049. [Google Scholar] [CrossRef]
- Moran, L.J.; Pasquali, R.; Teede, H.J.; Hoeger, K.M.; Norman, R.J. Treatment of obesity in polycystic ovary syndrome: A position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil. Steril. 2009, 92, 1966–1982. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.L.; Buckley, J.D.; Noakes, M.; Clifton, P.M.; Norman, R.J.; Brinkworth, G.D. The effect of a hypocaloric diet with and without exercise training on body composition, cardiometabolic risk profile, and reproductive function in overweight and obese women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 3373–3380. [Google Scholar] [CrossRef]
- Nybacka, Å.; Carlström, K.; Ståhle, A.; Nyrén, S.; Hellström, P.M.; Hirschberg, A.L. Randomized comparison of the influence of dietary management and/or physical exercise on ovarian function and metabolic parameters in overweight women with polycystic ovary syndrome. Fertil. Steril. 2011, 96, 1508–1513. [Google Scholar] [CrossRef] [PubMed]
- Hoeger, K.M.; Kochman, L.; Wixom, N.; Craig, K.; Miller, R.K.; Guzick, D.S. A randomized, 48-week, placebo-controlled trial of intensive lifestyle modification and/or metformin therapy in overweight women with polycystic ovary syndrome: A pilot study. Fertil. Steril. 2004, 82, 421–429. [Google Scholar] [CrossRef]
- Florakis, D.; Diamanti-Kandarakis, E.; Katsikis, I.; Nassis, G.P.; Karkanaki, A.; Georgopoulos, N.; Panidis, D. Effect of hypocaloric diet plus sibutramine treatment on hormonal and metabolic features in overweight and obese women with polycystic ovary syndrome: A randomized, 24-week study. Int. J. Obes. 2008, 32, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. American association of clinical endocrinologists and american college of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr. Pr. 2016, 22 (Suppl. 3), 1–203. [Google Scholar] [CrossRef]
- Çıtar Dazıroğlu, M.E.; Acar Tek, N. The Effect on Inflammation of Adherence to the Mediterranean Diet in Polycystic Ovary Syndrome. Curr. Nutr. Rep. 2023, 12, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Mancin, L.; Giacona, M.C.; Bianco, A.; Caprio, M. Effects of a ketogenic diet in overweight women with polycystic ovary syndrome. J. Transl. Med. 2020, 18, 104. [Google Scholar] [CrossRef]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Tomlinson, L.; Galletly, C.; Norman, R.J. Dietary composition in restoring reproductive and metabolic physiology in overweight women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2003, 88, 812–819. [Google Scholar] [CrossRef]
- Stamets, K.; Taylor, D.S.; Kunselman, A.; Demers, L.M.; Pelkman, C.L.; Legro, R.S. A randomized trial of the effects of two types of short-term hypocaloric diets on weight loss in women with polycystic ovary syndrome. Fertil. Steril. 2004, 81, 630–637. [Google Scholar] [CrossRef]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Norman, R.J. The effect of modifying dietary protein and carbohydrate in weight loss on arterial compliance and postprandial lipidemia in overweight women with polycystic ovary syndrome. Fertil. Steril. 2010, 94, 2451–2454. [Google Scholar] [CrossRef]
- Mehrabani, H.H.; Salehpour, S.; Amiri, Z.; Farahani, S.J.; Meyer, B.J.; Tahbaz, F. Beneficial effects of a high-protein, low-glycemic-load hypocaloric diet in overweight and obese women with polycystic ovary syndrome: A randomized controlled intervention study. J. Am. Coll. Nutr. 2012, 31, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.B.; Søe, M.; Halkier, K.H.; Stigsby, B.; Astrup, A. Effects of increased dietary protein-to-carbohydrate ratios in women with polycystic ovary syndrome. Am. J. Clin. Nutr. 2012, 95, 39–48. [Google Scholar] [CrossRef]
- Gower, B.A.; Chandler-Laney, P.C.; Ovalle, F.; Goree, L.L.; Azziz, R.; Desmond, R.A.; Granger, W.M.; Goss, A.M.; Bates, G.W. Favourable metabolic effects of a eucaloric lower-carbohydrate diet in women with PCOS. Clin. Endocrinol. 2013, 79, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Sabihi, S.S.; Esmaillzadeh, A. Effects of DASH diet on lipid profiles and biomarkers of oxidative stress in overweight and obese women with polycystic ovary syndrome: A randomized clinical trial. Nutrition 2014, 30, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Esmaillzadeh, A. DASH diet, insulin resistance, and serum hs-CRP in polycystic ovary syndrome: A randomized controlled clinical trial. Horm. Metab. Res. 2015, 47, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Marzouk, T.M.; Sayed Ahmed, W.A. Effect of Dietary Weight Loss on Menstrual Regularity in Obese Young Adult Women with Polycystic Ovary Syndrome. J. Pediatr. Adolesc. Gynecol. 2015, 28, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Su, L. Effect of diet intervention on quality of life and fasting insulin levels in patients with polycystic ovary syndrome. Tianjin J. Nurs. 2016, 24, 249–251. [Google Scholar]
- Azadi-Yazdi, M.; Karimi-Zarchi, M.; Salehi-Abargouei, A.; Fallahzadeh, H.; Nadjarzadeh, A. Effects of Dietary Approach to Stop Hypertension diet on androgens, antioxidant status and body composition in overweight and obese women with polycystic ovary syndrome: A randomised controlled trial. J. Hum. Nutr. Diet. 2017, 30, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Foroozanfard, F.; Rafiei, H.; Samimi, M.; Gilasi, H.R.; Gorjizadeh, R.; Heidar, Z.; Asemi, Z. The effects of dietary approaches to stop hypertension diet on weight loss, anti-Müllerian hormone and metabolic profiles in women with polycystic ovary syndrome: A randomized clinical trial. Clin. Endocrinol. 2017, 87, 51–58. [Google Scholar] [CrossRef]
- Xu, L.; Wang, H.; Gong, J.; Hou, X. Effects of Mediterranean diet on reproductive function in patients with obese polycystic ovary syndrome. Matern. Child. Health Care China 2017, 32, 122–124. [Google Scholar]
- Li, J. The effect of dietary guidance on polycystic ovary syndrome. J. Med. Theory Pr. 2017, 30, 3745–3746. [Google Scholar]
- Sun, Z.; Su, J.; Qu, X.; Tang, W. Effects of nutrition intervention with low-carbohydrate diet on glucose and lipid metabolism and conception in obese patients with polycystic ovary syndrome. J. Chin. Physician 2017, 19, 1209–1212. [Google Scholar]
- Qublan, H.S.; Yannakoula, E.K.; Al-Qudah, M.A.; El-Uri, F.I. Dietary intervention versus metformin to improve the reproductive outcome in women with polycystic ovary syndrome. A prospective comparative study. Saudi Med. J. 2007, 28, 1694–1699. [Google Scholar]
- Esfahanian, F.; Zamani, M.M.; Heshmat, R.; Moininia, F. Effect of metformin compared with hypocaloric diet on serum C-reactive protein level and insulin resistance in obese and overweight women with polycystic ovary syndrome. J. Obs. Gynaecol. Res. 2013, 39, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Li, Y.; Li, Y.; Chen, Q.; Zeng, X. Clinical observation of personalized diet intervention and metformin in the treatment of polycystic ovary syndrome. Matern. Child. Health Care China 2017, 32, 2535–2539. [Google Scholar]
- Ge, Q.; Yu, Y.; Liu, X. Effect of individualized diet intervention on insulin resistance and pregnancy in infertile patients with PCOS. ACTA Acad. Med. QINGDAO Univ. 2017, 53, 523–527. [Google Scholar]
- Shang, Y.; Zhou, H.; Hu, M.; Feng, H. Effect of Diet on Insulin Resistance in Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2020, 105, 3346–3360. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Goldenberg, N. Characteristics of obesity in polycystic ovary syndrome: Etiology, treatment, and genetics. Metabolism 2019, 92, 108–120. [Google Scholar] [CrossRef]
- Ryan, D.H.; Yockey, S.R. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Davies, M.J.; Norman, R.J.; Moran, L.J. Overweight, obesity and central obesity in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 618–637. [Google Scholar] [CrossRef]
- Herbert, S.; Woolf, K. Moving beyond Weight: A Narrative Review of the Dietary and Lifestyle Management for Reducing Cardiometabolic Risk in Polycystic Ovary Syndrome (PCOS). Nutrients 2023, 15, 5069. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.T.; Tang, Z.; Feng, Y.; Guan, H.; Huang, Z.; Zhang, W. Lower Fiber Consumption in Women with Polycystic Ovary Syndrome: A Meta-Analysis of Observational Studies. Nutrients 2022, 14, 5285. [Google Scholar] [CrossRef]
- Moran, L.J.; Ranasinha, S.; Zoungas, S.; McNaughton, S.A.; Brown, W.J.; Teede, H.J. The contribution of diet, physical activity and sedentary behaviour to body mass index in women with and without polycystic ovary syndrome. Hum. Reprod. 2013, 28, 2276–2283. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.C.; Norris, L.E.; Oster, R.A.; Darnell, B.E.; Azziz, R.; Gower, B.A. Difference in dietary intake between women with polycystic ovary syndrome and healthy controls. Fertil. Steril. 2006, 86, 411–417. [Google Scholar] [CrossRef]
- Larsson, I.; Hulthén, L.; Landén, M.; Pålsson, E.; Janson, P.; Stener-Victorin, E. Dietary intake, resting energy expenditure, and eating behavior in women with and without polycystic ovary syndrome. Clin. Nutr. 2016, 35, 213–218. [Google Scholar] [CrossRef] [PubMed]
- González, F. Nutrient-Induced Inflammation in Polycystic Ovary Syndrome: Role in the Development of Metabolic Aberration and Ovarian Dysfunction. Semin. Reprod. Med. 2015, 33, 276–286. [Google Scholar] [CrossRef]
- Shorakae, S.; Teede, H.; de Courten, B.; Lambert, G.; Boyle, J.; Moran, L.J. The Emerging Role of Chronic Low-Grade Inflammation in the Pathophysiology of Polycystic Ovary Syndrome. Semin. Reprod. Med. 2015, 33, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Marzullo, P.; Muscogiuri, G.; Di Somma, C.; Scacchi, M.; Orio, F.; Aimaretti, G.; Colao, A.; Savastano, S. Source and amount of carbohydrate in the diet and inflammation in women with polycystic ovary syndrome. Nutr. Res. Rev. 2018, 31, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Minihane, A.M.; Vinoy, S.; Russell, W.R.; Baka, A.; Roche, H.M.; Tuohy, K.M.; Teeling, J.L.; Blaak, E.E.; Fenech, M.; Vauzour, D.; et al. Low-grade inflammation, diet composition and health: Current research evidence and its translation. Br. J. Nutr. 2015, 114, 999–1012. [Google Scholar] [CrossRef]
- Esposito, K.; Nappo, F.; Marfella, R.; Giugliano, G.; Giugliano, F.; Ciotola, M.; Quagliaro, L.; Ceriello, A.; Giugliano, D. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: Role of oxidative stress. Circulation 2002, 106, 2067–2072. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Papalou, O.; Kandaraki, E.A.; Kassi, G. Mechanisms in Endocrinology: Nutrition as a mediator of oxidative stress in metabolic and reproductive disorders in women. Eur. J. Endocrinol. 2017, 176, R79–R99. [Google Scholar] [CrossRef] [PubMed]
- Cincione, I.R.; Graziadio, C.; Marino, F.; Vetrani, C.; Losavio, F.; Savastano, S.; Colao, A.; Laudisio, D. Short-time effects of ketogenic diet or modestly hypocaloric Mediterranean diet on overweight and obese women with polycystic ovary syndrome. J. Endocrinol. Investig. 2023, 46, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Wittert, G.A.; Williams, G.; Norman, R.J. Short-term meal replacements followed by dietary macronutrient restriction enhance weight loss in polycystic ovary syndrome. Am. J. Clin. Nutr. 2006, 84, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Sordia-Hernández, L.H.; Ancer Rodríguez, P.; Saldivar Rodriguez, D.; Trejo Guzman, S.; Servín Zenteno, E.S.; Guerrero González, G.; Ibarra Patiño, R. Effect of a low glycemic diet in patients with polycystic ovary syndrome and anovulation—A randomized controlled trial. Clin. Exp. Obs. Gynecol. 2016, 43, 555–559. [Google Scholar] [CrossRef]
- Atiomo, W.; Read, A.; Golding, M.; Silcocks, P.; Razali, N.; Sarkar, S.; Hardiman, P.; Thornton, J. Local recruitment experience in a study comparing the effectiveness of a low glycaemic index diet with a low calorie healthy eating approach at achieving weight loss and reducing the risk of endometrial cancer in women with polycystic ovary syndrome (PCOS). Contemp. Clin. Trials 2009, 30, 451–456. [Google Scholar] [CrossRef]
- Dou, P.; Zhang, T.T.; Xu, Y.; Xue, Q.; Zhang, Y.; Shang, J.; Yang, X.L. A Randomized Trial of the Efficacy of Three Weight Loss Diet Interventions in Overweight/Obese with Polycystic Ovary Syndrome. Endocr. Metab. Immune Disord. Drug Targets 2024, 24, 1686–1697. [Google Scholar] [CrossRef] [PubMed]
- Kasim-Karakas, S.E.; Almario, R.U.; Cunningham, W. Effects of protein versus simple sugar intake on weight loss in polycystic ovary syndrome (according to the National Institutes of Health criteria). Fertil. Steril. 2009, 92, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, H.; Papageorgiou, M.; Wells, L.; Akbar, S.; Strudwick, T.; Deshmukh, K.; Vitale, S.G.; Rigby, A.; Vince, R.V.; Reid, M.; et al. The Effect of a Very-Low-Calorie Diet (VLCD) vs. a Moderate Energy Deficit Diet in Obese Women with Polycystic Ovary Syndrome (PCOS)-A Randomised Controlled Trial. Nutrients 2023, 15, 3872. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.C.; Gower, B.A.; Darnell, B.E.; Ovalle, F.; Oster, R.A.; Azziz, R. Role of diet in the treatment of polycystic ovary syndrome. Fertil. Steril. 2006, 85, 679–688. [Google Scholar] [CrossRef]
- Goss, A.M.; Chandler-Laney, P.C.; Ovalle, F.; Goree, L.L.; Azziz, R.; Desmond, R.A.; Wright Bates, G.; Gower, B.A. Effects of a eucaloric reduced-carbohydrate diet on body composition and fat distribution in women with PCOS. Metabolism 2014, 63, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Hoover, S.E.; Gower, B.A.; Cedillo, Y.E.; Chandler-Laney, P.C.; Deemer, S.E.; Goss, A.M. Changes in Ghrelin and Glucagon following a Low Glycemic Load Diet in Women with PCOS. J. Clin. Endocrinol. Metab. 2021, 106, e2151–e2161. [Google Scholar] [CrossRef]
- Perelman, D.; Coghlan, N.; Lamendola, C.; Carter, S.; Abbasi, F.; McLaughlin, T. Substituting poly- and mono-unsaturated fat for dietary carbohydrate reduces hyperinsulinemia in women with polycystic ovary syndrome. Gynecol. Endocrinol. 2017, 33, 324–327. [Google Scholar] [CrossRef]
- Flanagan, E.W.; Most, J.; Mey, J.T.; Redman, L.M. Calorie Restriction and Aging in Humans. Annu. Rev. Nutr. 2020, 40, 105–133. [Google Scholar] [CrossRef] [PubMed]
- Heilbronn, L.K.; Ravussin, E. Calorie restriction and aging: Review of the literature and implications for studies in humans. Am. J. Clin. Nutr. 2003, 78, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Siervo, M.; Lara, J.; Chowdhury, S.; Ashor, A.; Oggioni, C.; Mathers, J.C. Effects of the Dietary Approach to Stop Hypertension (DASH) diet on cardiovascular risk factors: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Craddick, S.R.; Elmer, P.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Swain, M.C. The DASH diet and blood pressure. Curr. Atheroscler. Rep. 2003, 5, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Pirouzeh, R.; Heidarzadeh-Esfahani, N.; Morvaridzadeh, M.; Izadi, A.; Yosaee, S.; Potter, E.; Heshmati, J.; Pizarro, A.B.; Omidi, A.; Heshmati, S. Effect of DASH diet on oxidative stress parameters: A systematic review and meta-analysis of randomized clinical trials. Diabetes Metab. Syndr. 2020, 14, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Joyce, B.T.; Wu, D.; Hou, L.; Dai, Q.; Castaneda, S.F.; Gallo, L.C.; Talavera, G.A.; Sotres-Alvarez, D.; Van Horn, L.; Beasley, J.M.; et al. DASH diet and prevalent metabolic syndrome in the Hispanic Community Health Study/Study of Latinos. Prev. Med. Rep. 2019, 15, 100950. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Sabihi, S.S.; Esmaillzadeh, A. A randomized controlled clinical trial investigating the effect of DASH diet on insulin resistance, inflammation, and oxidative stress in gestational diabetes. Nutrition 2013, 29, 619–624. [Google Scholar] [CrossRef]
- Freeman, J.; Veggiotti, P.; Lanzi, G.; Tagliabue, A.; Perucca, E. The ketogenic diet: From molecular mechanisms to clinical effects. Epilepsy Res. 2006, 68, 145–180. [Google Scholar] [CrossRef] [PubMed]
- Masino, S.A.; Rho, J.M. Mechanisms of Ketogenic Diet Action. In Jasper’s Basic Mechanisms of the Epilepsies; Noebels, J.L., Avoli, M., Rogawski, M.A., Olsen, R.W., Delgado-Escueta, A.V., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Sumithran, P.; Proietto, J. Ketogenic diets for weight loss: A review of their principles, safety and efficacy. Obes. Res. Clin. Pr. 2008, 2, 1–13. [Google Scholar] [CrossRef]
- Westman, E.C.; Feinman, R.D.; Mavropoulos, J.C.; Vernon, M.C.; Volek, J.S.; Wortman, J.A.; Yancy, W.S.; Phinney, S.D. Low-carbohydrate nutrition and metabolism. Am. J. Clin. Nutr. 2007, 86, 276–284. [Google Scholar] [CrossRef]
- Kirkpatrick, C.F.; Bolick, J.P.; Kris-Etherton, P.M.; Sikand, G.; Aspry, K.E.; Soffer, D.E.; Willard, K.E.; Maki, K.C. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J. Clin. Lipidol. 2019, 13, 689–711.e681. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Vali, M.; Rezaei, S.; Bazmi, S.; Tabrizi, R.; Lankarani, K.B. Comparison of weight loss effects among overweight/obese adults: A network meta-analysis of mediterranean, low carbohydrate, and low-fat diets. Clin. Nutr. ESPEN 2024, 64, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Hironaka, J.; Hamaguchi, M.; Ichikawa, T.; Nakajima, H.; Okamura, T.; Majima, S.; Senmaru, T.; Okada, H.; Ushigome, E.; Nakanishi, N. Low-carbohydrate diets in East Asians with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. J. Diabetes Investig. 2024, 15, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Manson, J.; Liu, S. Glycemic index, glycemic load, and risk of type 2 diabetes. Am. J. Clin. Nutr. 2002, 76, 274s–280s. [Google Scholar] [CrossRef] [PubMed]
- Radulian, G.; Rusu, E.; Dragomir, A.; Posea, M. Metabolic effects of low glycaemic index diets. Nutr. J. 2009, 8, 5. [Google Scholar] [CrossRef]
- Zafar, M.I.; Mills, K.E.; Zheng, J.; Regmi, A.; Hu, S.Q.; Gou, L.; Chen, L.L. Low-glycemic index diets as an intervention for diabetes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 110, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.; Koh, G. Clinical Evidence and Mechanisms of High-Protein Diet-Induced Weight Loss. J. Obes. Metab. Syndr. 2020, 29, 166–173. [Google Scholar] [CrossRef]
- Marckmann, P.; Osther, P.; Pedersen, A.N.; Jespersen, B. High-protein diets and renal health. J. Ren. Nutr. 2015, 25, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Juhász, A.E.; Stubnya, M.P.; Teutsch, B.; Gede, N.; Hegyi, P.; Nyirády, P.; Bánhidy, F.; Ács, N.; Juhász, R. Ranking the dietary interventions by their effectiveness in the management of polycystic ovary syndrome: A systematic review and network meta-analysis. Reprod. Health 2024, 21, 28. [Google Scholar] [CrossRef]
- Moslehi, N.; Zeraattalab-Motlagh, S.; Rahimi Sakak, F.; Shab-Bidar, S.; Tehrani, F.R.; Mirmiran, P. Effects of nutrition on metabolic and endocrine outcomes in women with polycystic ovary syndrome: An umbrella review of meta-analyses of randomized controlled trials. Nutr. Rev. 2023, 81, 555–577. [Google Scholar] [CrossRef] [PubMed]
- Herrick, J.E.; Panza, G.S.; Gollie, J.M. Leptin, Leptin Soluble Receptor, and the Free Leptin Index following a Diet and Physical Activity Lifestyle Intervention in Obese Males and Females. J. Obes. 2016, 2016, 8375828. [Google Scholar] [CrossRef] [PubMed]
- Belobrajdic, D.P.; Frystyk, J.; Jeyaratnaganthan, N.; Espelund, U.; Flyvbjerg, A.; Clifton, P.M.; Noakes, M. Moderate energy restriction-induced weight loss affects circulating IGF levels independent of dietary composition. Eur. J. Endocrinol. 2010, 162, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Nigro, E.; Scudiero, O.; Monaco, M.L.; Palmieri, A.; Mazzarella, G.; Costagliola, C.; Bianco, A.; Daniele, A. New insight into adiponectin role in obesity and obesity-related diseases. Biomed. Res. Int. 2014, 2014, 658913. [Google Scholar] [CrossRef]
- Soltani, S.; Chitsazi, M.J.; Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) on serum inflammatory markers: A systematic review and meta-analysis of randomized trials. Clin. Nutr. 2018, 37, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Xing, N.N.; Ren, F.; Yang, H. Effects of ketogenic diet on weight loss parameters among obese or overweight patients with polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trails. Food Nutr. Res. 2024, 68. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Bai, W.P.; Jiang, B.; Bai, L.R.; Gu, B.; Yan, S.X.; Li, F.Y.; Huang, B. Ketogenic diet in women with polycystic ovary syndrome and liver dysfunction who are obese: A randomized, open-label, parallel-group, controlled pilot trial. J. Obs. Gynaecol. Res. 2021, 47, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Pandurevic, S.; Mancini, I.; Mitselman, D.; Magagnoli, M.; Teglia, R.; Fazzeri, R.; Dionese, P.; Cecchetti, C.; Caprio, M.; Moretti, C.; et al. Efficacy of very low-calorie ketogenic diet with the Pronokal® method in obese women with polycystic ovary syndrome: A 16-week randomized controlled trial. Endocr. Connect. 2023, 12, e220536. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Bai, W.; Jiang, B.; Wang, Z.; Wang, X.; Sun, Y.; Liu, F.; Cui, G.; Song, X.; Li, J.; et al. Effects of a ketogenic diet in women with PCOS with different uric acid concentrations: A prospective cohort study. Reprod. Biomed. Online 2022, 45, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Avolio, E.; Ferraro, S.; Mocciaro, R.; De Pergola, G.; Buzzanca, F.; Venturella, R.; Pecorella, C.; Palma, G.; Romano, L.; Mahata, S.K. The effect of ketogenic and low carb diet (Cyclic Alternation) on the ovarian morphology and insulin metabolism in polycystic ovary syndrome patients. Clin. Obs. Gynecol. 2020, 6, 1–6. [Google Scholar] [CrossRef]
- Cincione, R.I.; Losavio, F.; Ciolli, F.; Valenzano, A.; Cibelli, G.; Messina, G.; Polito, R. Effects of Mixed of a Ketogenic Diet in Overweight and Obese Women with Polycystic Ovary Syndrome. Int. J. Env. Res. Public Health 2021, 18, 12490. [Google Scholar] [CrossRef]
- Mavropoulos, J.C.; Yancy, W.S.; Hepburn, J.; Westman, E.C. The effects of a low-carbohydrate, ketogenic diet on the polycystic ovary syndrome: A pilot study. Nutr. Metab. 2005, 2, 35. [Google Scholar] [CrossRef] [PubMed]
- Liran, B.; Jian, L.; Litian, N.; Aili, W.; Fengyun, W.; Wenpei, B.; Bo, J. Preliminary report of a single-center clinical study for ketogenic diet intervention of polycystic ovary syndrome. J. Clin. Med. Pract. 2019, 23, 2–5. [Google Scholar]
- Jian, L.; Wenpei, B.; Bo, J.; Feiran, L.; Yanrong, C. Effects of ketogenic diet on vitamin D and glycolipid metabolism in overweight or obese patients with polycystic ovary syndrome. J. Clin. Med. Pract. 2022, 26, 14–17. [Google Scholar]
- Magagnini, M.C.; Condorelli, R.A.; Cimino, L.; Cannarella, R.; Aversa, A.; Calogero, A.E.; La Vignera, S. Does the ketogenic diet improve the quality of ovarian function in obese women? Nutrients 2022, 14, 4147. [Google Scholar] [CrossRef]
- Khalid, K.; Apparow, S.; Mushaddik, I.L.; Anuar, A.; Rizvi, S.A.A.; Habib, A. Effects of Ketogenic Diet on Reproductive Hormones in Women with Polycystic Ovary Syndrome. J. Endocr. Soc. 2023, 7, bvad112. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Bi, D.; Zhang, Y.; Kong, C.; Du, J.; Wu, X.; Wei, Q.; Qin, H. Ketogenic diet for human diseases: The underlying mechanisms and potential for clinical implementations. Signal Transduct. Target. Ther. 2022, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, Y.; Fukuda, T.; Oyabu, C.; Tanaka, M.; Asano, M.; Yamazaki, M.; Fukui, M. Impact of low-carbohydrate diet on body composition: Meta-analysis of randomized controlled studies. Obes. Rev. 2016, 17, 499–509. [Google Scholar] [CrossRef]
- Mansoor, N.; Vinknes, K.J.; Veierød, M.B.; Retterstøl, K. Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2016, 115, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Porchia, L.M.; Hernandez-Garcia, S.C.; Gonzalez-Mejia, M.E.; López-Bayghen, E. Diets with lower carbohydrate concentrations improve insulin sensitivity in women with polycystic ovary syndrome: A meta-analysis. Eur. J. Obs. Gynecol. Reprod. Biol. 2020, 248, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zheng, Y.; Guo, Y.; Lai, Z. The Effect of Low Carbohydrate Diet on Polycystic Ovary Syndrome: A Meta-Analysis of Randomized Controlled Trials. Int. J. Endocrinol. 2019, 2019, 4386401. [Google Scholar] [CrossRef] [PubMed]
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S., Jr.; Brinkworth, G.D. Comparison of low- and high-carbohydrate diets for type 2 diabetes management: A randomized trial. Am. J. Clin. Nutr. 2015, 102, 780–790. [Google Scholar] [CrossRef]
- Laganà, A.S.; Garzon, S.; Casarin, J.; Franchi, M.; Ghezzi, F. Inositol in Polycystic Ovary Syndrome: Restoring Fertility through a Pathophysiology-Based Approach. Trends Endocrinol. Metab. 2018, 29, 768–780. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef]
- Mei, S.; Ding, J.; Wang, K.; Ni, Z.; Yu, J. Mediterranean Diet Combined with a Low-Carbohydrate Dietary Pattern in the Treatment of Overweight Polycystic Ovary Syndrome Patients. Front. Nutr. 2022, 9, 876620. [Google Scholar] [CrossRef]
- Kazemi, M.; Pierson, R.A.; McBreairty, L.E.; Chilibeck, P.D.; Zello, G.A.; Chizen, D.R. A randomized controlled trial of a lifestyle intervention with longitudinal follow-up on ovarian dysmorphology in women with polycystic ovary syndrome. Clin. Endocrinol. 2020, 92, 525–535. [Google Scholar] [CrossRef]
- Turner-McGrievy, G.M.; Davidson, C.R.; Wingard, E.E.; Billings, D.L. Low glycemic index vegan or low-calorie weight loss diets for women with polycystic ovary syndrome: A randomized controlled feasibility study. Nutr. Res. 2014, 34, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, M.; McBreairty, L.E.; Chizen, D.R.; Pierson, R.A.; Chilibeck, P.D.; Zello, G.A. A Comparison of a Pulse-Based Diet and the Therapeutic Lifestyle Changes Diet in Combination with Exercise and Health Counselling on the Cardio-Metabolic Risk Profile in Women with Polycystic Ovary Syndrome: A Randomized Controlled Trial. Nutrients 2018, 10, 1387. [Google Scholar] [CrossRef]
- Kazemi, M.; Hadi, A.; Pierson, R.A.; Lujan, M.E.; Zello, G.A.; Chilibeck, P.D. Effects of dietary glycemic index and glycemic load on cardiometabolic and reproductive profiles in women with polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2021, 12, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Saadati, N.; Haidari, F.; Barati, M.; Nikbakht, R.; Mirmomeni, G.; Rahim, F. The effect of low glycemic index diet on the reproductive and clinical profile in women with polycystic ovarian syndrome: A systematic review and meta-analysis. Heliyon 2021, 7, e08338. [Google Scholar] [CrossRef] [PubMed]
- Manta, A.; Paschou, S.A.; Isari, G.; Mavroeidi, I.; Kalantaridou, S.; Peppa, M. Glycemic Index and Glycemic Load Estimates in the Dietary Approach of Polycystic Ovary Syndrome. Nutrients 2023, 15, 3483. [Google Scholar] [CrossRef]
- Sadeghi, H.M.; Adeli, I.; Calina, D.; Docea, A.O.; Mousavi, T.; Daniali, M.; Nikfar, S.; Tsatsakis, A.; Abdollahi, M. Polycystic Ovary Syndrome: A Comprehensive Review of Pathogenesis, Management, and Drug Repurposing. Int. J. Mol. Sci. 2022, 23, 583. [Google Scholar] [CrossRef]
- Barr, S.; Reeves, S.; Sharp, K.; Jeanes, Y.M. An isocaloric low glycemic index diet improves insulin sensitivity in women with polycystic ovary syndrome. J. Acad. Nutr. Diet. 2013, 113, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Dou, P.; Wei, W.; Liu, P.J. Effects of high-protein diets on the cardiometabolic factors and reproductive hormones of women with polycystic ovary syndrome: A systematic review and meta-analysis. Nutr. Diabetes 2024, 14, 6. [Google Scholar] [CrossRef]
- Yu, Z.; Nan, F.; Wang, L.Y.; Jiang, H.; Chen, W.; Jiang, Y. Effects of high-protein diet on glycemic control, insulin resistance and blood pressure in type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2020, 39, 1724–1734. [Google Scholar] [CrossRef]
- Yang, J.; Liang, J.; Xu, J.; Lin, T.; Ye, Q.; Lin, Q.; Ji, F.; Shi, D. The impact of dietary interventions on polycystic ovary syndrome patients with a BMI ≥25 kg/m(2): A systematic review and meta-analysis of randomized controlled trials. Reprod. Med. Biol. 2024, 23, e12607. [Google Scholar] [CrossRef] [PubMed]
- Cheshmeh, S.; Ghayyem, M.; Khamooshi, F.; Heidarzadeh-Esfahani, N.; Rahmani, N.; Hojati, N.; Mosaieby, E.; Moradi, S.; Pasdar, Y. Green cardamom plus low-calorie diet can decrease the expression of inflammatory genes among obese women with polycystic ovary syndrome: A double-blind randomized clinical trial. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2022, 27, 821–830. [Google Scholar] [CrossRef]
- Tabrizi, F.P.F.; Farhangi, M.A.; Vaezi, M.; Hemmati, S. The effects of spinach-derived thylakoid supplementation in combination with calorie restriction on anthropometric parameters and metabolic profiles in obese women with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled clinical trial. Nutr. J. 2020, 19, 1–13. [Google Scholar]
- Nadjarzadeh, A.; Ghadiri-Anari, A.; Ramezani-Jolfaie, N.; Mohammadi, M.; Salehi-Abargouei, A.; Namayande, S.M.; Mozaffari-Khosravi, H.; Hosseini-Marnani, E. Effect of hypocaloric high-protein, low-carbohydrate diet supplemented with fennel on androgenic and anthropometric indices in overweight and obese women with polycystic ovary syndrome: A randomized placebo-controlled trial. Complement. Ther. Med. 2021, 56, 102633. [Google Scholar] [CrossRef]
- Johnson, L.K.; Holven, K.B.; Nordstrand, N.; Mellembakken, J.R.; Tanbo, T.; Hjelmesæth, J. Fructose content of low calorie diets: Effect on cardiometabolic risk factors in obese women with polycystic ovarian syndrome: A randomized controlled trial. Endocr. Connect. 2015, 4, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Jinhui, W.; Jing, S.; Ping, L.; Huimin, C.; Hongfeng, L.; Minhua, X. The impact of dietary intervention on patients with obese polycystic ovary syndrome. Med. Res. J. 2020, 49, 113–116. [Google Scholar]
- Yu, Y.; Liu, X.; Ge, Q.; Yu, X.; Wang, J. The impact of nutritional intervention on AMH levels and pregnancy rates in patients with obese polycystic ovary syndrome. J. Qingdao Univ. 2018, 54, 588–596. [Google Scholar] [CrossRef]
- Marnani, E.H.; Ghadiri-Anari, A.; Ramezani-Jolfaie, N.; Mohammadi, M.; Namayandeh, S.M.; Mozaffari-Khosravi, H.; Salehi-Abargouei, A.; Nadjarzadeh, A. Effect of fennel supplementation along with high-protein, low-carbohydrate weight-loss diet on insulin resistance and percentage of fat and muscle mass in overweight/obese women with polycystic ovary syndrome. J. Funct. Foods 2020, 67, 103848. [Google Scholar] [CrossRef]
- Shishehgar, F.; Tehrani, F.R.; Vahidi, S. The effects of weight loss on health-related quality of life in obese women with PCOS and controls. BMC Womens Health 2023, 23, 532. [Google Scholar] [CrossRef] [PubMed]
- Shishehgar, F.; Mirmiran, P.; Rahmati, M.; Tohidi, M.; Ramezani Tehrani, F. Does a restricted energy low glycemic index diet have a different effect on overweight women with or without polycystic ovary syndrome? BMC Endocr. Disord. 2019, 19, 93. [Google Scholar] [CrossRef]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Wittert, G.A.; Belobrajdic, D.P.; Norman, R.J. C-reactive protein before and after weight loss in overweight women with and without polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2007, 92, 2944–2951. [Google Scholar] [CrossRef]
- Toscani, M.K.; Mario, F.M.; Radavelli-Bagatini, S.; Wiltgen, D.; Matos, M.C.; Spritzer, P.M. Effect of high-protein or normal-protein diet on weight loss, body composition, hormone, and metabolic profile in southern Brazilian women with polycystic ovary syndrome: A randomized study. Gynecol. Endocrinol. 2011, 27, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Noakes, M.; Clifton, P.M.; Wittert, G.A.; Tomlinson, L.; Galletly, C.; Luscombe, N.D.; Norman, R.J. Ghrelin and measures of satiety are altered in polycystic ovary syndrome but not differentially affected by diet composition. J. Clin. Endocrinol. Metab. 2004, 89, 3337–3344. [Google Scholar] [CrossRef]
- VanHise, K.; Wang, E.T.; Norris, K.; Azziz, R.; Pisarska, M.D.; Chan, J.L. Racial and ethnic disparities in polycystic ovary syndrome. Fertil. Steril. 2023, 119, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Engmann, L.; Jin, S.; Sun, F.; Legro, R.S.; Polotsky, A.J.; Hansen, K.R.; Coutifaris, C.; Diamond, M.P.; Eisenberg, E.; Zhang, H. Racial and ethnic differences in the polycystic ovary syndrome metabolic phenotype. Am. J. Obstet. Gynecol. 2017, 216, 493.e1–493.e13. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.L.; Kar, S.; Vanky, E.; Morin-Papunen, L.; Piltonen, T.; Puurunen, J.; Tapanainen, J.S.; Maciel, G.A.R.; Hayashida, S.A.Y.; Soares, J.M., Jr. Racial and ethnic differences in the prevalence of metabolic syndrome and its components of metabolic syndrome in women with polycystic ovary syndrome: A regional cross-sectional study. Am. J. Obstet. Gynecol. 2017, 217, 189.e1–189.e8. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Dietary Pattern | Reference | Region | Study Design | Subject Health Status | Dietary Intervention | Mean Age (Years) | Study Period | Outcomes |
|---|---|---|---|---|---|---|---|---|
| DASH diet | Azadi-Yazdi et al., 2017 [23] | Iran | Parallel | Overweight and/or obese women with PCOS | InG (n = 28): DASH diet (50 to 55% carbohydrate, 15 to 20% protein, and 25 to 30% fat from total E; sodium < 2400 mg/day) Dietary components (1600 kcal/day): grains: 6 servings (at least 3 servings from whole grains), simple sugar: 2 servings, vegetables: 4 servings, fruits: 4 servings, dairy (<2% fat): 2 servings, meats, poultry and fish: 3 servings, nuts, seeds and legumes: 2 servings, fats and oils: 3 servings (low in SFA and TC) CG (n = 27): control diet (50 to 55% carbohydrate, 15 to 20% protein, and 25 to 30% fat from total E) Dietary components (1600 kcal/day): grains: 9 servings, simple sugar: 4 servings, vegetables: 2 servings, fruits: 2 servings, dairy: 1 serving, meats, poultry and fish: 3 servings, nuts, seeds and legumes: 1 serving, fats and oils: 2 servings Both groups are calorie restricted by BMI (BMI 25 to 29.9 kg/m2: 350 kcal, BMI 30 to 39.9 kg/m2: 500 kcal) Both groups are isocaloric matched | InG: 32.1 ± 6.0 CG: 31.8 ± 6.2 | 12 weeks | ↓ BW, BMI, WC, HC, LBM, and TFM within InG and CG ↓ BW, BMI, and TFM in InG vs. CG ↔ WC, HC, and LBM between InG and CG ↔ WHR ↓ total T, A4, and FAI within InG and CG ↑ SHBG within InG and CG ↓ A4 in InG vs. CG ↑ SHBG in InG vs. CG ↔ total T and FAI between InG and CG ↑ DPPH within InG and CG ↑ DPPH in InG vs. CG |
| DASH diet | Foroozanfard et al., 2017 [24] | Iran | Parallel | Overweight and/or obese women with PCOS | InG (n = 30): DASH diet (52 to 55% carbohydrate, 16 to 18% protein, and 30% fat from total E; sodium < 2400 mg/day) Dietary components (1800 kcal/day): grains: 7 servings (bread and rice; at least 3 servings from whole grains), simple sugar: 2 servings, vegetables: 5 servings (tomatoes, potatoes, carrots, peas, kale, squash, broccoli, turnip greens, collards, spinach, artichokes and beans), fruits: 6 servings (apricots, bananas, grapes, oranges and juice, tangerines, strawberries, melons, peaches, pineapples, prunes, raisins and grapefruit and juice), dairy: 3 servings (milk, buttermilk, yogurt, or cheese; <2% low fat), meats, poultry and fish: 4 servings (4 servings of lean meats), nuts, seeds and legumes: 2 servings (almonds, mixed nuts, walnuts, sunflower seeds, kidney beans and lentils), and fats and oils: 3 servings (hydrogenated oil, vegetable oils and olive oil) CG (n = 30): control diet (52 to 55% carbohydrate, 16 to 18% protein, and 30% fat from total E) Dietary components (1800 kcal/day): grains: 9 servings, simple sugar: 4 servings, vegetables: 4 servings, fruits: 4 servings, dairy: 2 servings, meats, poultry and fish: 4 servings (2 servings of lean meats), nuts, seeds and legumes: 1 serving, and fats and oils: 3 servings Both groups are calorie restricted by BMI (BMI 25 to 27.5 kg/m2: 350 kcal; BMI 27.5 to 31 kg/m2: 500 kcal; BMI > 31 kg/m2: 700 kcal) Both groups are isocaloric matched | InG: 27.1 ± 4.7 CG: 25.6 ± 3.7 | 12 weeks | ↓ BW and BMI in InG vs. CG ↔ FBG within InG and CG ↑ QUICKI within InG ↓ FBI, HOMA-IR, and HOMA-B within InG ↔ FBI, HOMA-IR, HOMA-B, and QUICKI within CG ↓ FBI, HOMA-IR, and HOMA-B in InG vs. CG ↑ QUICKI in InG vs. CG ↔ FBG between InG and CG ↓ FAI within InG ↑ SHBG within InG ↑ AMH within CG ↔ AMH within InG ↔SHBG and FAI within CG ↑ SHBG in InG vs. CG ↓ AMH and FAI in InG vs. CG ↔ total T, FSH, LH, and 17 OH-P ↓ MDA within InG and CG ↑ NO within InG ↔ NO within CG ↓ MDA in InG vs. CG ↑ NO in InG vs. CG |
| DASH diet | Asemi et al., 2015 [20] | Iran | Parallel | Overweight and/or obese women with PCOS | InG (n = 24): DASH diet (52% carbohydrate, 18% protein, and 30% fat from total E; sodium < 2400 mg/day) Dietary components (per day): Grains: 9 servings (≥3 whole grains), simple sugar: 2 servings, vegetables: 5 servings, fruits: 6 servings, low-fat dairy (<2%): 3 servings, lean meat, poultry and fish: 4 servings, nuts, seeds and legumes: 2 servings, and fats and oils: 3 servings CG (n = 24): control diet (52% carbohydrate, 18% protein, and 30% fat from total E) Dietary components (per day): Grains: 9 servings, simple sugar: 5 servings, vegetables: 3 servings, fruits: 3 servings, dairy: 2 servings, meat, poultry and fish: 4 servings (lean meat: 2 servings), nuts, seeds and legumes: 1 serving, and fats and oils: 3 servings Both groups were calorie restricted by BMI (BMI 25 to 27.5 kg/m2: 350 kcal; BMI 27.5 to 31 kg/m2:500 kcal; BMI > 31 kg/m2: 700 kcal) Both groups are isocaloric matched | InG: 30.7 ± 6.7 CG: 29.4 ± 6.2 | 8 weeks | ↓ BW, BMI, WC, and HC in InG vs. CG ↓ FBI and HOMA-IR in InG vs. CG ↑ QUICKI in InG vs. CG ↔ FBG and HOMA-B between InG and CG ↓ hs-CRP in InG vs. CG |
| DASH diet | Asemi et al., 2014 [19] | Iran | Parallel | Overweight and obese women with PCOS | InG (n = 24): DASH diet (52% carbohydrate, 18% protein, and 30% fat from total E) Dietary components (per day): Grains: 6 servings (≥3 servings from whole grains), simple sugar: 2 servings, vegetables: 4 servings, fruits: 5 servings, dairy: 3 servings (<2% low fat), lean meats, poultry and fish: 4 servings, nuts, seeds and legumes: 2 servings, and fats and oils: 3 servings CG (n = 24): control diet (52% carbohydrate, 18% protein, and 30% fat from total E) Dietary components (per day): Grains: 9 servings, simple sugar: 5 servings, vegetables: 2 servings, fruits: 2 servings, dairy: 2 servings, meats, poultry and fish: 4 servings (lean meats: 2 servings), nuts, seeds and legumes: 1 serving, and fats and oils: 3 servings Both groups are calorie restricted by BMI (BMI 25 to 27.5 kg/m2: 350 kcal; BMI 27.5 to 31 kg/m2: 500 kcal; BMI > 31 kg/m2: 700 kcal) Both groups are isocaloric matched | InG: 22.1 ± 3.2 CG: 24.7 ± 6.0 | 8 weeks | ↓ BW and BMI in InG vs. CG ↔ TC, TG, VLDL-C, HDL-C, LDL-C, and TC/HDL-C ratio ↔ TAC within InG and CG ↑ TAC in InG vs. CG ↔ GSH |
| Low-carbohydrate diet | Perelman et al., 2017 [57] | USA | Cross-over | Obese women with PCOS | InG (n = 6): low-carbohydrate diet [40% carbohydrate, 15% protein, and 45% fat (SFA: ≤7% of E; a ratio of PUFA to MUFA of 1.0) from total E; 200 mg cholesterol and 20 g fiber per day] CG (n = 6): control diet [60% carbohydrate, 15% protein, and 25% fat (SFA: ≤7% of E; a ratio of PUFA to MUFA of 1.0) from total E; 200 mg cholesterol and 20 g fiber per day] Both groups are isocaloric matched and maintain BW | 30 ± 7 | 8 weeks (3 weeks for each diet; washout: 2 weeks) | ↔ BW between InG and CG ↓ insulin AUC in InG vs. CG ↔ glucose AUC between InG and CG ↓ LDL-C in InG vs. CG ↔ TC, TG and HDL-C between InG and CG |
| Low-carbohydrate diet | Goss et al., 2014 [55] | USA | Cross-over | Women with PCOS (BMI ≤ 45 kg/m2) | InG (n = 27): low-carbohydrate diet (41% carbohydrate, 19% protein, and 40% fat from total E; ~50 GI) CG (n = 23): control diet (55% carbohydrate, 18% protein, and 27% fat from total E; ~60 GI) Both groups are isocaloric matched and maintain BW | 31 ± 5.8 | 20 weeks (8 weeks for each diet; washout: 4 weeks) | ↓ BW, TFM, and thigh SAT within InG and CG ↓ PBF, IAAT, SAAT, and thigh IMAT within InG ↔ LBM within InG ↔ PBF, IAAT, SAAT, and thigh IMAT within CG ↓ LBM within CG ↔ BW, TFM, PBF, LBM, IAAT, SAAT, thigh SAT, and thigh IMAT between InG and CG ↔ thigh PMAT |
| Low-carbohydrate diet | Gower et al., 2013 [18] | USA | Cross-over | Women with PCOS (BMI ≤ 45 kg/m2) | InG (n = 27): low-carbohydrate diet (41% carbohydrate, 19% protein, and 40% fat from total E; ~50 GI) Dietary components (1800 kcal/day): carbohydrate 187 g, sugar 79 g, GL 81 g (GL/1000 kcal: 45.90), protein 86 g, SFA 24 g, MUFA 28 g, PUFA 22 g, n − 3 FA 1.76 g, and fiber 22 g Dietary components (2500 kcal/day): carbohydrate 261 g, sugar 120 g, GL 114 g (GL/1000 kcal: 46.50), protein 119 g, SFA 34 g, MUFA 40 g, PUFA 29 g, n-3 FA 2.45 g, and fiber 31 g CG (n = 23): control diet (55% carbohydrate, 18% protein, and 27% fat from total E; ~60 GI) Dietary components (1800 kcal/day): carbohydrate 254 g, sugar 110 g, GL 143 g (GL/1000 kcal: 79.00), protein 84 g, SFA 17 g, MUFA 20 g, PUFA 13 g, n-3 FA 0.86 g, and fiber 18 g Dietary components (2500 kcal/day): carbohydrate 350 g, sugar 166 g, GL 192 g (GL/1000 kcal: 76.60), SFA 21 g, MUFA 26 g, PUFA 23 g, n-3 FA 1.30 g, and fiber 23 g Both groups are isocaloric matched and maintain BW | 31.2 ± 5.8 | 20 weeks (8 weeks for each diet; washout: 4 weeks) | ↔ BW between InG and CG ↓ PhiB, HOMA-IR, FBG, and FBI within InG ↑ PhiD, X0, and Si within InG ↔ PhiB, PhiD, X0, Si, HOMA-IR, FBG, and FBI within CG ↔ PhiS and PhiTOT within InG and CG ↓ HDL-C within InG and CG ↓ TC and LDL-C within InG ↑ TC/HDL-C ratio within CG ↔ TG within InG and CG ↔ TC/HDL-C ratio within InG ↔ TC and LDL-C within CG ↓ total T within InG ↔ total T within CG ↔ FSH, LH, SHBG, and FAI within InG and CG |
| Low-carbohydrate diet | Douglas et al., 2006 [54] | USA | Cross-over | Overweight and/or obese women with PCOS | InG1 (n = 11): low-carbohydrate diet [43% carbohydrate, 15% protein, and 45% total fat (8% SFA, 17% PUFA, and 18% MUFA) from total E; 83 mg cholesterol and 29 g fiber per day] InG2 (n = 11): MUFA diet [55% carbohydrate, 15% protein, and 33% fat (7% SFA, 6% PUFA, and 17% MUFA) from total E; 108 mg cholesterol and 24 g fiber per day] CG (n = 11): control diet [56% carbohydrate, 16% protein, and 31% fat (7% SFA, 10% PUFA, and 13% MUFA) from total E; 115 mg cholesterol and 27 g fiber per day] All Groups are isocaloric matched and maintain BW (2000 to 2300 kcal/day) | 33 ± 6 | 48 days +3 weeks (16 days for each diets; washout: 3 weeks) | ↓ BW in InG1 vs. InG2 ↓ FBI in InG1 vs. CG ↓ AIRg in InG1 vs. InG2 ↔ FBG, Si, and disposition index ↓ TC in InG1 vs. CG ↔ TG, FFA, HDL-C, and LDL-C ↑ A4 in InG2 vs. CG ↔ total T, free T, DHEAS, SHBG, LH, and FSH |
| Low-carbohydrate diet | Moran et al., 2006 [48] | Australia | Parallel | Overweight and/or obese women with PCOS | InG (phase 1, n = 18; phase 2, n = 14): low-carbohydrate diet phase 2 (9 to 32 weeks): carbohydrate-restricted BW maintenance diet with low-GI (<120 g carbohydrate/day) CG (phase 1: n = 16, phase 2: n = 9): control diet phase 2 (9 to 32 weeks): fat-restricted BW maintenance diet with low-GI (<50 g fat/day) Both groups are calorie restricted and consumed same diet in phase 1: phase 1 (0 to 8 weeks): 2 meals with replacements (each meal: ~430 kcal) and a low-fat evening meal (~836 kcal; fruit and vegetables: ≥5 servings/day) Both groups are isocaloric matched | InG: 33.2 ± 4.8 CG: 32.1 ± 5.5 | 32 weeks (8 weeks: BW loss diet; 24 weeks: BW maintenance diet) | Phase 1 ↓ BW, WC, TFM, FFM, SBP, REE, and RQ within InG and CG ↔ DBP within InG and CG ↔ BW, WC, TFM, FFM, SBP, DBP, REE, and RQ between InG and CG ↓ FBG within InG and CG ↓ FBI and HOMA-IR within InG and CG ↔ glucose AUC within InG and CG ↔ FBG, glucose AUC, FBI, and HOMA-IR between InG and CG ↓ total T, free T, and FAI within InG and CG ↑ SHBG within InG and CG ↔ total T, free T, FAI, and SHBG between InG and CG Phase 2 ↔ BW, WC, TFM, FFM, SBP, DBP, REE, and RQ between InG and CG ↔ FBG, glucose AUC, FBI, and HOMA–IR between InG and CG ↔ total T, free T, FAI, and SHBG between InG and CG |
| Low-GI diet | Hoover et al., 2021 [56] | USA | Cross-over | Overweight and/or obese women with PCOS | InG (n = 27): low-GI diet (41% carbohydrate, 19% protein, and 40% fat from total E; ~50 GI) CG (n = 27): control diet (55% carbohydrate, 18% protein, and 27% fat from total E; ~60 GI) Both groups are isocaloric matched and maintain BW | 31.2 ± 5.8 | 20 weeks (8 weeks for each diet; 4 weeks: washout) | ↔ BMI between InG and CG ↓ FBG and FBI within InG and CG ↔ FBG and FBI between InG and CG ↔ glucagon ↓ ghrelin and cortisol within InG and CG ↑ GLP-1 within InG and CG ↔ GLP-1, ghrelin, and cortisol between InG and CG ↔ Peptide YY |
| Low-GI diet | Sordia-Hernández et al., 2016 [49] | Mexico | Parallel | Women with PCOS | InG (n = 19): low-GI diet [45% and 50% complex carbohydrate, 15% to 20% protein, and 30% to 40% fat (10% to 15% MUFA, <10% PUFA, and <10% SFA) from total E; 20 to 35 g fiber per day; <45 GI] CG (n = 18): control diet [45% and 50% complex carbohydrate, 15% to 20% protein, and 30% to 40% fat (10% to 15% MUFA, <10% PUFA, and <10% SFA) from total E; 20 to 35 g fiber per day; 50 to 75 GI] Both groups are calorie restricted Both groups are isocaloric matched (1200 to 1500 kcal/day) | InG: 26.1 ± 4.2 CG: 26.1 ± 4.7 | 3 months | ↔ BW ↔ cycle 1, cycle 2, and cycle 3 ovulatory cycle between InG and CG ↑ cycle 1 + 2 and cycle 1 + 2+ 3 ovulatory cycle in InG vs. CG |
| Low-GI diet | Atiomo et al., 2009 [50] | UK | Parallel | Obese women with PCOS | InG (n = 6): low-GI diet CG (n = 5): control diet Both groups are calorie restricted (600 kcal/day) Both groups are isocaloric matched | InG: 35.3 CG: 36.4 | 6 months | ↔ BW, WC, HC, BMI, SBP, and DBP ↔ FBG and FBI ↔ TC, HDL-C, LDL-C, TG, and HDL-C/LDL-C ratio ↔ ED, LH, SHBG, and T ↔ endometrial thickness |
| low-GI plus high-protein diet | Mehrabani et al., 2012 [16] | Iran | Parallel | Overweight and/or obese women with PCOS | InG (n = 23): low-GI plus high-protein diet (40% carbohydrate, 30% protein, and 30% fat from total E; <20 GL foods) CG (n = 26): control diet (55% carbohydrate, 15% protein, and 30% fat from total E) Both groups were calorie restricted by BMI (BMI 21 to 22 kg/m2: 500 to 1000 kcal/day) Both groups are isocaloric matched | InG: 30.5 ± 6.4 CG: 28.5 ± 5.2 | 12 weeks | ↓ BW within InG and CG ↓ WC and HC in InG vs. CG ↔ BW, PBF, percent of LBM, and suprailiac skinfold between InG and CG ↓ FBI and HOMA-IR within InG ↔ FBI and HOMA-IR within CG ↓ adiponectin within InG and CG ↓ FBI and HOMA-IR in InG vs. CG ↔ adiponectin between InG and CG ↓ LDL-C within InG and CG ↔ LDL-C between InG and CG ↔ TG, TC, and HDL-C ↑ SHBG within InG and CG ↓ total T, DHEAS, and FAI within InG and CG ↔ SHBG, total T, DHEAS, and FAI between InG and CG ↔ A4, FSH, and LH ↓ hs-CRP within InG ↔ hs-CRP between InG and CG ↓ TNF-α within InG and CG ↔ TNF-α between InG and CG ↔ IL-6 |
| High-protein diet | Sørensen et al., 2012 [17] | Denmark | Parallel | Women with PCOS | InG (n = 14): high-protein diet (<30% carbohydrate, >40% protein, and 30% fat from total E) CG (n = 13): control diet (>55% carbohydrate, <15% protein, and 30% fat from total E) Both groups are not calorie restricted Both groups are isocaloric matched (mean difference = ~136 kcal; 95% CI ~−134 to ~406 kcal; p = 0.16) | InG: 27.7 ± 5.5 CG: 28.4 ± 5.8 | 6 months | ↓ BW, BMI, TFM, and WC within InG and CG ↓ BW, BMI, TFM, and WC in InG vs. CG ↔ LBM, HC, and WHR ↓ FBG in InG vs. CG ↔ C-peptide between InG and CG ↔ TG, HDL-C, LDL-C, TC, TC/HDL-C ratio, and TG/HDL-C ratio between InG and CG ↔ total T, free T, and SHBG between InG and CG |
| High-protein diet | Moran et al., 2010 [15] | Australia | Parallel | Overweight and/or obese women with PCOS | InG (n = 14): high-protein diet (43% carbohydrate, 27% protein, and 28% fat from total E) CG (n = 14): control diet (57% carbohydrate, 16% protein, and 27% fat from total E) Both groups are calorie restricted Both groups are isocaloric matched (~1434 kcal/day) | 32.8 ± 4.5 | 16 weeks (12 weeks: calorie-restricted diet, 4 weeks: calorie balance diet) | ↓ BW, BMI, and MAP within InG and CG ↔ BW, BMI, and MAP between InG and CG ↓ FBI and insulin AUC within InG and CG ↔ FBG and glucose AUC between InG and CG ↑ LAE and SAE within InG and CG ↔ LAE and SAE between InG and CG ↓ TG and FFA within InG and CG ↔ TG and FFA between InG and CG ↔ TG AUC and FFA AUC ↔ FAI ↓ hs-CRP within InG and CG ↔ hs-CRP between InG and CG |
| High-protein diet | Kasim-Karakas et al., 2009 [52] | USA | Parallel | Overweight and/or obese women with PCOS | InG (n = 11): 240 kcal whey protein + calorie-restricted diet (39.5% carbohydrate, 33.7% protein, and 26.2% fat from total E) CG (n = 13): 240 kcal simple sugars + calorie-restricted diet (56.7% carbohydrate, 16.6% protein, and 25.9% fat from total E) Both groups are calorie restricted (450 kcal/day) Both groups are isocaloric matched | 18 to 45 | 2 months | ↓ BMI within InG and CG ↓ BW and TFM within InG ↔ BW and TFM within CG ↓ BW, BMI, and TFM in InG vs. CG ↔ LBM ↓ leptin and adiponectin within InG ↔ leptin and adiponectin between InG and CG ↔ FBG, FBI, HbA1c, and HOMA-IR ↓ TC, HDL-C, and apo B within InG ↔ TC, HDL-C, and apo B within CG ↓ TC, HDL-C, and apo B in InG vs. CG ↔ TG ↔ T, SHBG, FAI, and DHEAS ↔ hs-CRP |
| High-protein diet | Stamets et al., 2004 [14] | USA | Parallel | Overweight and/or obese women with PCO | InG (n = 13): high-protein diet (40% carbohydrate, 30% protein, and 30% fat from total E) CG (n = 13): control diet (55% carbohydrate, 15% protein, and 30% fat from total E) Both groups are calorie restricted (1000 kcal/day) and consume multivitamin/mineral supplements Both groups are isocaloric matched | InG: 29 ± 4 CG: 26 ± 4 | 4 weeks | ↓ BW within InG and CG ↓ WC within InG ↔ BW, WC, HC, WHR, SBP, and DBP between InG and CG ↓ fasting leptin and leptin AUC within InG ↔ FBI, insulin AUC and FBG/FBI ratio within InG ↔ insulin AUC, glucose AUC, FBG/FBI ratio, fasting leptin, and leptin AUC between InG and CG ↓ TC and LDL-C within InG ↔ TC, HDL-C, LDL-C, and TG between InG and CG ↑ DHEAS within InG ↓ total T and bioavailable T within InG ↔ DHEAS, total T, bioavailable T, LH, and FSH between InG and CG |
| High-protein diet | Moran et al., 2003 [13] | Australia | Parallel | Overweight and/or obese women with PCOS | InG (n = 14): high-protein diet (40% carbohydrate, 30% protein, and 30% fat from total E) CG (n = 14): control diet (55% carbohydrate, 15% protein, and 30% fat from total E) Both groups are calorie restricted and isocaloric matched (~1433 kcal/day) | InG: 32 ± 1.2 CG: 33 ± 1.2 | 16 weeks (12 weeks: calorie-restricted diet; 4 weeks: BW maintenance) | 12 weeks (vs. baseline) ↓ FBI and HOMA-IR within InG and CG ↔ FBI and HOMA-IR between InG and CG ↔ FBG ↓ TC, LDL-C, TG, and TC/HDL-C ratio within InG and CG ↔ HDL-C within InG ↓ HDL-C within CG ↓ HDL-C in CG vs. InG ↓ TC/HDL-C ratio in InG vs. CG ↔ TC, LDL-C, and TG between InG and CG ↑ SHBG within InG and CG ↓ total T and FAI within InG and CG ↔ total T, FAI, and SHBG between InG and CG 16 weeks (vs. baseline) ↔ BW within InG and CG ↓ TFM, LBM, and abdominal fat mass within InG and CG ↔ BW, TFM, LBM, and abdominal fat mass between InG and CG ↓ FBI and HOMA-IR within InG and CG ↑ glucose AUC within CG ↔ FBI, HOMA-IR, and insulin AUC between InG and CG ↔ FBG ↓ TC, LDL-C, and TG within InG and CG ↓ TC/HDL-C in InG vs. CG ↑ HDL-C in InG vs. CG |
| Dietary Pattern | Reference | Region | Study Design | Subject Health Status | Dietary Intervention | Mean Age (Years) | Study Period | Outcomes |
|---|---|---|---|---|---|---|---|---|
| KD | Cincione et al., 2023 [47] | Italy | Parallel | Overweight and/or obese women with PCOS | InG (n = 73): mixed KD with caloric-restriction (~600 kcal/day) [≤30 g carbohydrate, 1.1 to 1.2 g protein/ideal BW (isolated whey protein powder), 30 g lipid (10 g EVOO) per day;multivitamin and multi-mineral supplement] CG (n = 71): MED diet with calorie restriction (500 kcal restriction/day) [55% carbohydrate (whole wheat), 20% protein (fish and legumes), and 25% fat (PUFA from olive oil, almonds, and pistachios) from total E] Both groups are not isocaloric matched | InG: 33.4 ± 5.7 CG: 33.6 ± 4.9 | 45 days | ↓ BW, BMI, WC, HC, WHR, TFM, FFM, REE, BM, and TBW within InG and CG ↓ BW, BMI, WC, HC, WHR, TFM, FFM, REE, BM, and TBW in InG vs. CG ↓ FBG, FBI, HOMA-IR, and C-peptide within InG and CG ↑ albumin within InG and CG ↓ FBG, FBI, HOMA-IR, and C-peptide in InG vs. CG ↑ albumin in InG vs. CG ↓ total T, free T, LH, and LH/FSH ratio within InG and CG ↑ FSH and SHBG within InG and CG ↓ total T, free T, and LH in InG vs. CG ↑ FSH and SHBG in InG vs. CG ↔ LH/FSH ratio between InG and CG ↑ regular menstrual cycle in InG vs. CG |
| High-protein diet | Dou et al., 2024 [51] | China | Parallel | Overweight and/or obese women without PCOS | InG1 (n = 30): balanced diet + high-protein + high-fiber (10 g fiber/day) InG2 (n = 30): balanced diet + high-protein (40 g whey protein; daily protein intake of 1.5 to 2 kg/day) CG (n = 22): balanced diet (55 to 60% carbohydrate, 0.8 to 1.2 g/kg/day protein and 25 to 30% fat from total E) Balanced diet is calorie restricted Balanced dietary components (1000 to 1200 kcal/day): Breakfast: 0.5 to 1 fist-sized cooked staple food (0.5 to 1 tael raw rice and noodles), 250 mL low-fat milk, 1 egg and 100 g leafy vegetables; Lunch: 0.5 to 1 fist-sized cooked staple food (0.5 to 1 tael raw rice and noodles), 100 g low-fat lean meat and leafy vegetables; Dinner: 0.5 to 1 fist-sized cooked staple food (0.5 to 1 tael raw rice and noodles), 100 g bean products, and leafy vegetables; The morning meal and afternoon meal: 100 g fruit, respectively | InG1: 31.3 ± 5.8 InG2: 32.1 ± 5.8 CG: 31.5 ± 2.7 | 8 weeks | ↓ BW, BMI, PBF, and VFA within InG1 and InG2 and CG ↓ FFM within CG ↔ FFM within InG1 and InG2 ↔ FFM index within InG1 and InG2 and CG ↓ BW and PBF in InG1 and InG2 vs. CG ↓ BMI and VFA in InG1 vs. InG2 and CG ↔ FFM and FFM index between InG1 and InG2 and CG ↓ HOMA-IR within InG1 and InG2 and CG ↔ HOMA-IR between InG1 and InG2 and CG ↓ MDA within InG1 and InG2 and CG ↓ MDA in InG1 and InG2 vs. CG ↑ SOD within InG1 and InG2 and CG ↑ SOD in InG1 and InG2 vs. CG |
| Very low-calorie diet | Deshmukh et al., 2023 [53] | UK | Parallel | Obese women with PCOS | InG (n = 11): very low-calorie diet Diet intervention (per day): 800 kcal meal replacement (each meal: 200 kcal; 21 g carbohydrate, 15 g protein, and 3 to 4 g fat) Diet reintroduction: calorie increase (200 kcal/2 weeks) until ~1600 kcal/day CG (n = 11): low-calorie diet (600 kcal restriction/day) | InG: 27.7 ± 3.8 CG: 28.1 ± 5.6 | 16 weeks (8 weeks: intervention; 8 weeks: reintroduction) | 8 weeks ↓ BW, BMI, WC, WHR, TFM, trunk fat, LBM, and FFM within InG ↓ BW, BMI, and TFM within CG ↔ WC, WHR, trunk fat, LBM, and FFM within CG ↓ BW, BMI, WC, WHR, total fat, trunk fat, LBM, and FFM in InG vs. CG ↔ BMC and BMD ↓ FBG within InG ↔ FBG within CG ↓ FBG in InG vs. CG ↔ 2 h glucose OGTT and HbA1c ↓ TC within InG and CG ↔ TC between InG and CG ↔ TG ↓ FAI within InG ↔ FAI and SHBG within CG ↑ SHBG within InG ↑ SHBG in InG vs. CG ↔ FAI between InG and CG ↔ total T, DHEAS, A4, LH, and FSH ↔ CRP, ALT, and AST 16 weeks ↓ BW in InG vs. CG ↔ FAI between InG and CG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Kang, K.; Je, M.; Lee, Y.-M.; Kim, Y. The Influence of Dietary Patterns on Polycystic Ovary Syndrome Management in Women: A Review of Randomized Controlled Trials with and Without an Isocaloric Dietary Design. Nutrients 2025, 17, 674. https://doi.org/10.3390/nu17040674
Choi Y, Kang K, Je M, Lee Y-M, Kim Y. The Influence of Dietary Patterns on Polycystic Ovary Syndrome Management in Women: A Review of Randomized Controlled Trials with and Without an Isocaloric Dietary Design. Nutrients. 2025; 17(4):674. https://doi.org/10.3390/nu17040674
Chicago/Turabian StyleChoi, Yeonjeong, Kyeonghoon Kang, Minkyung Je, Young-Min Lee, and Yoona Kim. 2025. "The Influence of Dietary Patterns on Polycystic Ovary Syndrome Management in Women: A Review of Randomized Controlled Trials with and Without an Isocaloric Dietary Design" Nutrients 17, no. 4: 674. https://doi.org/10.3390/nu17040674
APA StyleChoi, Y., Kang, K., Je, M., Lee, Y.-M., & Kim, Y. (2025). The Influence of Dietary Patterns on Polycystic Ovary Syndrome Management in Women: A Review of Randomized Controlled Trials with and Without an Isocaloric Dietary Design. Nutrients, 17(4), 674. https://doi.org/10.3390/nu17040674