
Sleep Quality, Nutritional Habits, and Physical Activity in Pediatric Cancer Survivors: A Dyadic Analysis Approach

Abstract
1. Introduction
Study Purpose
2. Materials and Methods
2.1. Participants and Setting
2.2. Data Collection
2.3. Data Analysis
2.4. Data Screening
2.5. Covariates
3. Results
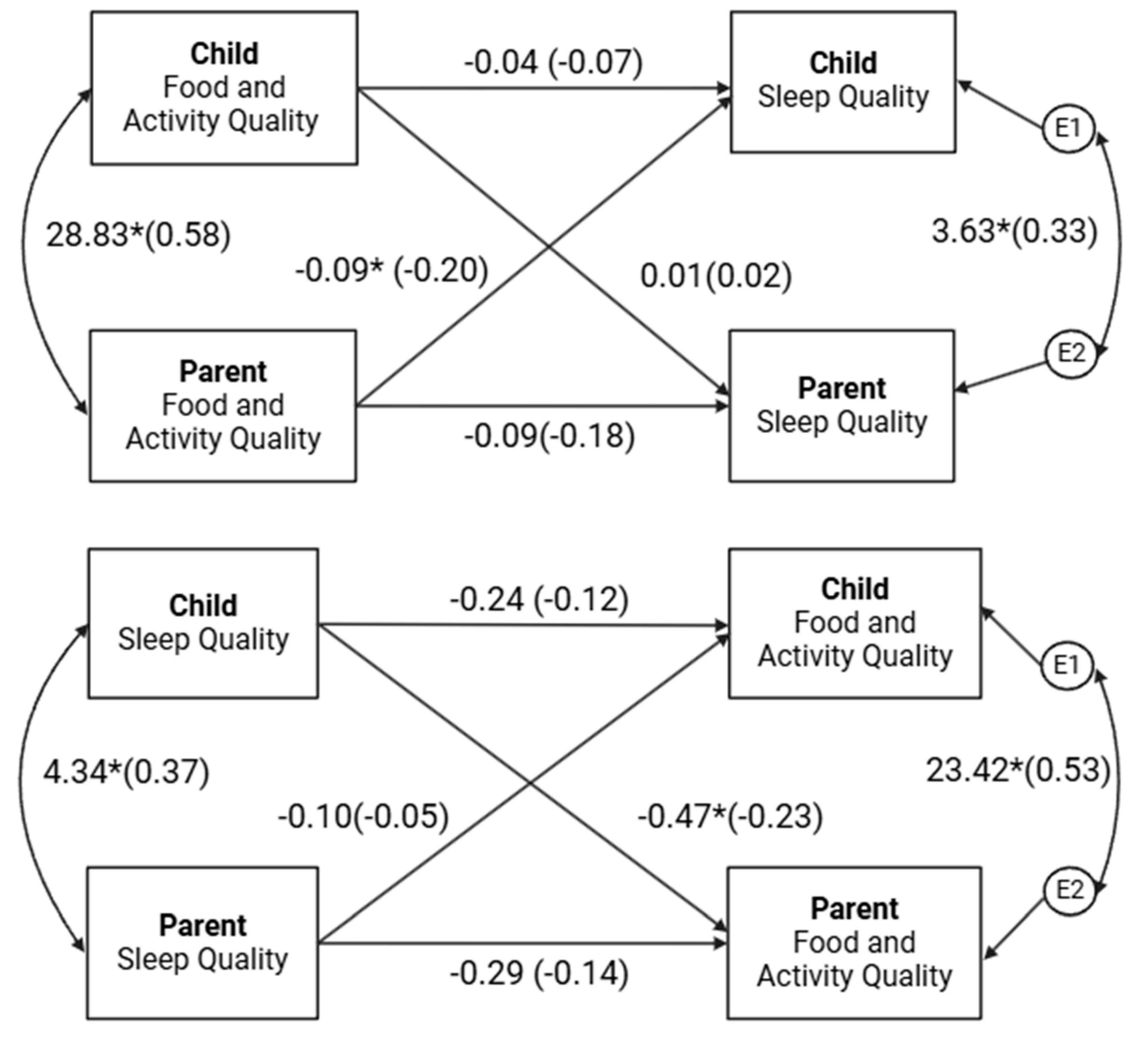
3.1. APIMs
3.2. Physical Activity and Dietary Behavior Effects
4. Discussion
Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phillips, S.M.; Padgett, L.S.; Leisenring, W.M.; Stratton, K.K.; Bishop, K.; Krull, K.R.; Alfano, C.M.; Gibson, T.M.; De Moor, J.S.; Hartigan, D.B.; et al. Survivors of childhood cancer in the United States: Prevalence and burden of morbidity. Cancer Epidemiol. Biomark. Prev. 2015, 24, 653–663. [Google Scholar] [CrossRef]
- Ness, K.K.; Hudson, M.M.; Ginsberg, J.P.; Nagarajan, R.; Kaste, S.C.; Marina, N.; Whitton, J.; Robison, L.L.; Gurney, J.G. Physical performance limitations in the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2009, 27, 2382–2389. [Google Scholar] [CrossRef]
- Zhang, F.F.; Kelly, M.J.; Must, A. Early Nutrition and Physical Activity Interventions in Childhood Cancer Survivors. Curr. Obes. Rep. 2017, 6, 168–177. [Google Scholar] [CrossRef]
- Sheikh, I.N.; Roth, M.; Stavinoha, P.L. Prevalence of Sleep Disturbances in Pediatric Cancer Patients and Their Diagnosis and Management. Children 2021, 8, 1100. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.L.; Hudson, M.M. Survivors of childhood and adolescent cancer: Life-long risks and responsibilities. Nat. Rev. Cancer 2014, 14, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Tonorezos, E.S.; Cohn, R.J.; Glaser, A.W.; Lewin, J.; Poon, E.; Wakefield, C.E.; Oeffinger, K.C. Long-term care for people treated for cancer during childhood and adolescence. Lancet 2022, 399, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.T.; Oeffinger, K.C.; Chen, Y.; Kawashima, T.; Yasui, Y.; Leisenring, W.; Stovall, M.; Chow, E.J.; Sklar, C.A.; Mulrooney, D.A.; et al. Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. J. Clin. Oncol. 2013, 31, 3673–3680. [Google Scholar] [CrossRef] [PubMed]
- Oeffinger, K.C.; Mertens, A.C.; Sklar, C.A.; Yasui, Y.; Fears, T.; Stovall, M.; Vik, T.A.; Inskip, P.D.; Robison, L.L. Obesity in Adult Survivors of Childhood Acute Lymphoblastic Leukemia: A Report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2003, 21, 1359–1365. [Google Scholar] [CrossRef]
- Daniel, L.C.; van Litsenburg, R.R.L.; Rogers, V.E.; Zhou, E.S.; Ellis, S.J.; Wakefield, C.E.; Stremler, R.; Walter, L.; Crabtree, V.M.; on behalf of the International Psycho-Oncology Society Pediatrics Special Interest Group. A call to action for expanded sleep research in pediatric oncology: A position paper on behalf of the International Psycho-Oncology Society Pediatrics Special Interest Group. Psycho-Oncology 2020, 29, 465–474. [Google Scholar] [CrossRef]
- Gomes, R.; Salazar, L.; Fraga, C.; Correia, M.R.; Barbosa-Sequeira, J.; Fernandes, A.; Álvares, S.; Leitão, J.B.; Coelho, M.P. Management of infantile hemangiomas—Experience of a tertiary hospital. Eur. J. Pediatr. 2023, 182, 1611–1618. [Google Scholar] [CrossRef]
- Mogavero, M.P.; Bruni, O.; DelRosso, L.M.; Ferri, R. Neurodevelopmental Consequences of Pediatric Cancer and Its Treatment: The Role of Sleep. Brain Sci. 2020, 10, 411. [Google Scholar] [CrossRef] [PubMed]
- Raber, M.; Swartz, M.C.; Maria, D.S.; O’connor, T.; Baranowski, T.; Li, R.; Chandra, J. Parental involvement in exercise and diet interventions for childhood cancer survivors: A systematic review. Pediatr. Res. 2016, 80, 338–346. [Google Scholar] [CrossRef]
- Murphy, B.R.; Raber, M.P.; Crawford, K.D.; Grasse, L.; Wartenberg, L.; Wu, J.; Dibaj, S.S.; Chandra, J. High Rates of Obesity at Presentation Persist into Survivorship across Childhood Cancer Types. Child. Obes. 2020, 16, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef]
- van Santen, H.M.; Geskus, R.B.; Raemaekers, S.; van Trotsenburg, A.S.P.; Vulsma, T.; van der Pal, H.J.H.; Caron, H.N.; Kremer, L.C.M. Changes in body mass index in long-term childhood cancer survivors. Cancer 2015, 121, 4197–4204. [Google Scholar] [CrossRef]
- Greving, D.M.; Santacroce, S.J. Cardiovascular Late Effects. J. Pediatr. Oncol. Nurs. 2005, 22, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Kamps, W.A.; de Bont, E.S.; Boot, A.M.; Burgerhof, J.G.; Tamminga, R.Y.; Tissing, W.J. Changes in nutritional status in childhood cancer patients: A prospective cohort study. Clin. Nutr. 2015, 34, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.T.; Li, W.H.C.; Ho, L.L.K.; Ho, K.Y.; Chan, G.C.F.; Chung, J.O.K. Physical activity for pediatric cancer survivors: A systematic review of randomized controlled trials. J. Cancer Surviv. 2021, 15, 876–889. [Google Scholar] [CrossRef]
- Brown, N.I.; Sauls, R.; Almendares, M.; Gray, H.L.; Stern, M. Factors impacting physical activity among post-treatment pediatric cancer survivors with overweight and obesity. Eur. J. Pediatr. 2024, 183, 3129–3136. [Google Scholar] [CrossRef] [PubMed]
- Barnard, J.; Roberts, S.; Lastella, M.; Aisbett, B.; Condo, D. The Impact of Dietary Factors on the Sleep of Athletically Trained Populations: A Systematic Review. Nutrients 2022, 14, 3271. [Google Scholar] [CrossRef] [PubMed]
- Hower, I.M.; Harper, S.A.; Buford, T.W. Circadian Rhythms, Exercise, and Cardiovascular Health. J. Circadian Rhythm. 2018, 16, 30210567. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Ma, C.; Wu, G.; Liu, H.; Chen, L.; Yang, G. Effects of exercise on circadian rhythms in humans. Front. Pharmacol. 2023, 14, 1282357. [Google Scholar] [CrossRef]
- Ho, Y.-C.L.; Mahirah, D.; Ho, C.Z.-H.; Thumboo, J. The role of the family in health promotion: A scoping review of models and mechanisms. Health Promot. Int. 2022, 37, daac119. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Bai, Y.; Fu, Y.; Pfledderer, C.D.; Brusseau, T.A. Parent Engagement and Support, Physical Activity, and Academic Performance (PESPAAP): A Proposed Theoretical Model. Int. J. Environ. Res. Public Health 2019, 16, 4698. [Google Scholar] [CrossRef]
- Thompson, T.; Ketcher, D.; Gray, T.F.; Kent, E.E. The Dyadic Cancer Outcomes Framework: A general framework of the effects of cancer on patients and informal caregivers. Soc. Sci. Med. 2021, 287, 114357. [Google Scholar] [CrossRef]
- Van Schoors, M.; De Paepe, A.L.; Lemiere, J.; Morez, A.; Norga, K.; Lambrecht, K.; Goubert, L.; Verhofstadt, L.L. Family Adjustment When Facing Pediatric Cancer: The Role of Parental Psychological Flexibility, Dyadic Coping, and Network Support. Front. Psychol. 2019, 10, 2740. [Google Scholar] [CrossRef] [PubMed]
- Tørslev, M.K.; Thøgersen, D.B.; Bonde, A.H.; Bloch, P.; Varming, A. Supporting Positive Parenting and Promoting Healthy Living through Family Cooking Classes. Int. J. Environ. Res. Public Heal. 2021, 18, 4709. [Google Scholar] [CrossRef] [PubMed]
- Merrigan, J.J.; Volgenau, K.M.; McKay, A.; Mehlenbeck, R.; Jones, M.T.; Gallo, S. Bidirectional Associations between Physical Activity and Sleep in Early-Elementary-Age Latino Children with Obesity. Sports 2021, 9, 26. [Google Scholar] [CrossRef]
- Alnawwar, M.A.; Alraddadi, M.I.; Algethmi, R.A.; Salem, G.A.; Salem, M.A.; Alharbi, A.A. The Effect of Physical Activity on Sleep Quality and Sleep Disorder: A Systematic Review. Cureus 2023, 15, e43595. [Google Scholar] [CrossRef] [PubMed]
- Ward, A.L.; Jospe, M.; Morrison, S.; Reynolds, A.N.; Kuroko, S.; Fangupo, L.J.; Smith, C.; Galland, B.C.; Taylor, R.W. Bidirectional associations between sleep quality or quantity, and dietary intakes or eating behaviors in children 6-12 years old: A systematic review with evidence mapping. Nutr. Rev. 2021, 79, 1079–1099. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.; Gray, H.L.; Ruble, K.; Lozano, S.S.; Albizu-Jacob, A.; Williams, J.M.; Godder, K.; Fuemmeler, B.; Mazzeo, S. A cluster-randomized control trial targeting parents of pediatric cancer survivors with obesity: Rationale and study protocol of NOURISH-T+. Contemp. Clin. Trials 2021, 102, 106296. [Google Scholar] [CrossRef]
- Livestrong Young Adult Alliance. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancer: Report of the Adolescent and Young Adult Oncology Progress Review Group; U.S. Department of Health and Human Services: Washington, DC, USA, 2023. [Google Scholar]
- Smith, A.W.; Seibel, N.L.; Lewis, D.R.; Albritton, K.H.; Blair, D.F.; Blanke, C.D.; Bleyer, W.A.; Freyer, D.R.; Geiger, A.M.; Hayes-Lattin, B.; et al. Next steps for adolescent and young adult oncology workshop: An update on progress and recommendations for the future. Cancer 2016, 122, 988–999. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.K.; Auld, G.; Baker, S.S.; Barale, K.; Franck, K.; Khan, T.; Palmer-Keenan, D.; Walsh, J. Methodology for Developing a New EFNEP Food and Physical Activity Behaviors Questionnaire. J. Nutr. Educ. Behav. 2017, 49, 777–783.e771. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Kenny, D.A.; Kashy, D.A. The Design and Analysis of Data from Dyads and Groups. In Handbook of Research Methods in Social and Personality Psychology, 2nd ed.; Reis, H.T., Judd, C.M., Eds.; Cambridge University Press: Cambridge, UK, 2014; pp. 589–607. [Google Scholar]
- Kenny, D.A. An Interactive Tool for the Estimation and Testing the Actor-Partner Interdependence Model Using Multilevel Modeling [Computer Software]. 2015. Available online: https://davidakenny.shinyapps.io/APIM_MM/ (accessed on 7 January 2025).
- Tabachnik, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson: New York, NY, USA, 2021. [Google Scholar]
- Cook, W.L.; Kenny, D.A. The Actor–Partner Interdependence Model: A model of bidirectional effects in developmental studies. Int. J. Behav. Dev. 2005, 29, 101–109. [Google Scholar] [CrossRef]
- Kenny, D.A. The effect of nonindependence on significance testing in dyadic research. Pers. Relatsh. 1995, 2, 67–75. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bulletin. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Ackerman, R.A.; Kenny, D.A.; APIM Power: An Interactive Tool for Actor-Partner Interdependence Model Power Analysis [Computer Software]. December 2016. Available online: https://robert-a-ackerman.shinyapps.io/apimpower/ (accessed on 7 January 2025).
- Champion, K.E.; Gardner, L.A.; McCann, K.; Hunter, E.; Parmenter, B.; Aitken, T.; Chapman, C.; Spring, B.; Thornton, L.; Slade, T.; et al. Parent-based interventions to improve multiple lifestyle risk behaviors among adolescents: A systematic review and meta-analysis. Prev. Med. 2022, 164, 107247. [Google Scholar] [CrossRef]
- Yang, C.H.; Wang, S.; Wang, W.L.; Belcher, B.R.; Dunton, G.F. Day-level associations of physical activity and sedentary time in mother-child dyads across three years: A multi-wave longitudinal study using accelerometers. J. Behav. Med. 2022, 45, 702–715. [Google Scholar] [CrossRef]
- Petersen, T.L.; Møller, L.B.; Brønd, J.C.; Jepsen, R.; Grøntved, A. Association between parent and child physical activity: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 67. [Google Scholar] [CrossRef]
- John, J.C.; Ho, J.; Raber, M.; Basen-Engquist, K.; Jacobson, L.; Strong, L.L. Dyad and group-based interventions in physical activity, diet, and weight loss: A systematic review of the evidence. J. Behav. Med. 2024, 47, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Orsey, A.D.; Wakefield, D.B.; Cloutier, M.M. Physical activity (PA) and sleep among children and adolescents with cancer. Pediatr. Blood Cancer 2013, 60, 1908–1913. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Zhou, E.S.; Chevalier, L.; Lun, P.; Davidson, R.D.; Pariseau, E.M.; Long, K.A. Parental Behaviors, Emotions at Bedtime, and Sleep Disturbances in Children with Cancer. J. Pediatr. Psychol. 2020, 45, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Crowder, S.L.; Buro, A.W.; Stern, M. Physical activity interventions in pediatric, adolescent, and young adult cancer survivors: A systematic review. Support. Care Cancer 2022, 30, 4635–4649. [Google Scholar] [CrossRef]
- Feit, T.; Beals, E.; Dandekar, S.; Kadan-Lottick, N.; Joffe, L. Nutritional assessment and dietary intervention among survivors of childhood cancer: Current landscape and a look to the future. Front. Nutr. 2023, 10, 1343104. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-León, A.E.; Avila-Prado, J.; Bracamontes-Picos, L.R.; Haby, M.M.; Stein, K.; Astiazaran-Garcia, H.; Lopez-Teros, V. Nutritional interventions in children with acute lymphoblastic leukemia undergoing antineoplastic treatment: A systematic review. BMC Nutr. 2024, 10, 89. [Google Scholar] [CrossRef]
- Napartuk, M.; Bélanger, V.; Bouchard, I.; Meloche, C.; Curnier, D.; Sultan, S.; Laverdière, C.; Sinnett, D.; Marcil, V. Improvement of Diet after an Early Nutritional Intervention in Pediatric Oncology. Children 2023, 10, 667. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, L.; Sun, Q.; Xiao, P.; Duan, Y.; Liu, X.; Zhou, J.; Xie, J.; Cheng, A.S. Effect of Two Interventions on Sleep Quality for Adolescent and Young Adult Cancer Survivors: A Pilot Randomized Controlled Trial. Cancer Nurs. 2022, 45, E560–E572. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between diet and sleep quality: A systematic review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef] [PubMed]
- Neugebauer, C.; Mastergeorge, A.M. The Family Stress Model in the Context of Pediatric Cancer: A Systematic Review. J. Child Fam. Stud. 2021, 30, 1099–1122. [Google Scholar] [CrossRef]
- Bates, C.R.; Pallotto, I.K.; Moore, R.M.; Fornander, M.J.; Covitz, L.M.; Gillette, M.L.D. Family rules, routines, and caregiver distress during the first year of pediatric cancer treatment. Psycho-Oncology 2021, 30, 1590–1599. [Google Scholar] [CrossRef]

{kind=link}
| Parent (n = 127) | Child (n = 127) | |
|---|---|---|
| Age (mean ± SD) years | 43.2 ± 7.6 | 11.0 ± 2.7 |
| a BMI (mean ± SD) kg/m2 | 33.4 ± 9.3 | 34.4 ± 8.72 |
| a BMI Percentile (mean ± SD) | -- | 95.6 ± 2.2 |
| Gender | ||
| Female: n (%) | 90 (72.3) | 67 (52.8) |
| Race/Ethnicity: n (%) | ||
| White | 51 (40.2) | 51 (40.2) |
| Black/African American | 23 (18.1) | 23 (18.1) |
| Hispanic/Latine | 44 (34.6) | 44 (34.6) |
| Asian/ Pacific Islander | 4 (3.1) | 4 (3.1) |
| Other | 2 (1.6) | 2 (1.6) |
| Missing | 3 (2.4) | 3 (2.4) |
| Cancer Diagnosis | ||
| b ALL | -- | 57 (44.9) |
| Tumor | -- | 31 (24.4) |
| c MDS | -- | 1 (0.8) |
| d AML | -- | 11 (8.7) |
| Missing | -- | 27 (21.3) |
| Time since Diagnosis | -- | 6.2 ± 3.0 |
| Income: n (%) | ||
| <USD 20 K | 25 (19.7) | -- |
| USD 20–34,999 | 24 (18.9) | -- |
| USD 35–49,999 | 13 (10.2) | -- |
| USD 50–69,999 | 11 (8.7) | -- |
| >USD 70 K | 52 (40.9) | -- |
| Missing | 2 (1.6) | -- |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. Parent FAQ | - | |||||||
| 2. Child FAQ | 0.576 ** | - | ||||||
| 3. Parent PSQI | −0.201 * | −0.104 | - | |||||
| 4. Child PSQI | −0.250 ** | −0.194 * | 0.357 ** | - | ||||
| 5. Child age | −0.159 | −0.236 * | 0.032 | 0.063 | - | |||
| 6. Parent Age | −0.101 | −0.172 | −0.031 | 0.090 | 0.195 * | - | ||
| 7. Parent BMI | −0.166 | −0.189 * | 0.099 | 0.128 | 0.614 ** | 0.005 | - | |
| 8. Child BMI | −0.193 * | −0.066 | 0.061 | 0.135 | −0.045 | 0.002 | 0.084 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serpas, D.G.; Sauls, R.; Gray, H.L.; Stern, M. Sleep Quality, Nutritional Habits, and Physical Activity in Pediatric Cancer Survivors: A Dyadic Analysis Approach. Nutrients 2025, 17, 250. https://doi.org/10.3390/nu17020250
Serpas DG, Sauls R, Gray HL, Stern M. Sleep Quality, Nutritional Habits, and Physical Activity in Pediatric Cancer Survivors: A Dyadic Analysis Approach. Nutrients. 2025; 17(2):250. https://doi.org/10.3390/nu17020250
Chicago/Turabian StyleSerpas, Dylan G., Rachel Sauls, Heewon L. Gray, and Marilyn Stern. 2025. "Sleep Quality, Nutritional Habits, and Physical Activity in Pediatric Cancer Survivors: A Dyadic Analysis Approach" Nutrients 17, no. 2: 250. https://doi.org/10.3390/nu17020250
APA StyleSerpas, D. G., Sauls, R., Gray, H. L., & Stern, M. (2025). Sleep Quality, Nutritional Habits, and Physical Activity in Pediatric Cancer Survivors: A Dyadic Analysis Approach. Nutrients, 17(2), 250. https://doi.org/10.3390/nu17020250