
Stepwise Incremental Hemodialysis and Low-Protein Diet Supplemented with Keto-Analogues Preserve Residual Kidney Function: A Randomized Controlled Trial †

 , , , ,
, , , , Highlights
- Incremental HD with once-weekly dialysis combined with a low-protein diet supplemented with ketoanalogues may help preserve residual kidney function (RKF) and urine volume compared to twice-weekly HD in selected patients with substantial RKF and adequate nutritional status.
- This approach has the potential to provide a patient-centered and cost-effective option, especially in low- and middle-income countries, while maintaining acceptable clinical outcomes.
- Our findings suggest that the regimen was well-tolerated concerning metabolic and nutritional parameters; however, the small sample size limits the strength of the conclusions and highlights the need for validation in larger studies.
Abstract
1. Introduction
2. Materials and Methods
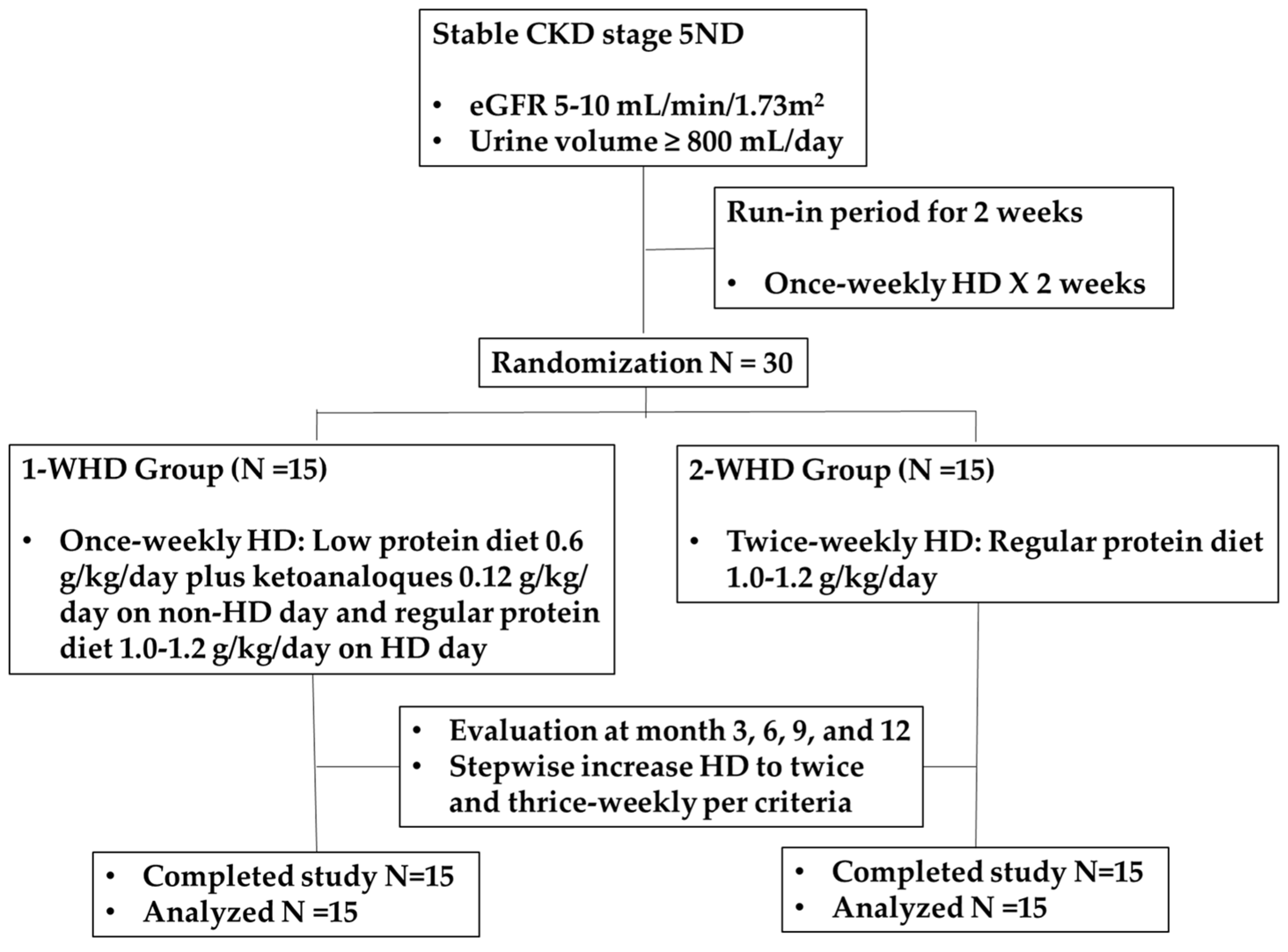
2.1. Study Design and Participants
2.2. Run-In Period and Randomization
2.3. Follow-Up Evaluation
2.4. Statistical Analysis
3. Results
3.1. Baseline Data of Participants
3.2. Residual Kidney Function (RKF) and Urine Volume
3.3. Laboratory Results, β2 Microglobulin (β2M) and Protein-Bound Uremic Toxin
3.4. Skeletal Muscle Mass, Ultrafiltration Rate per HD Session, and Furosemide Dose
3.5. Quality of Life
3.6. Incremental HD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RCT | Randomized controlled trial |
| RKF | Residual kidney function |
| 1-WHD | Once-weekly HD with low-protein diet (0.6 g/kg/day), and KAs (0.12 g/kg/day) on non-dialysis days, and a regular-protein diet (1.0–1.2 g/kg/day) on dialysis days |
| 2-WHD | Twice-weekly HD with a regular-protein diet (1.0–1.2 g/kg/day) |
| KA | Keto-analogues |
| QoL | Quality of life |
| β2M | β2-microglobulin |
References
- Vilar, E.; Farrington, K. Emerging importance of residual renal function in end-stage renal failure. Semin. Dial. 2011, 24, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.T.; Fishbane, S.; Obi, Y.; Kalantar-Zadeh, K. Preservation of residual kidney function in hemodialysis patients: Reviving an old concept. Kidney Int. 2016, 90, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Rhee, C.M.; Mathew, A.T.; Shah, G.; Streja, E.; Brunelli, S.M.; Kovesdy, C.P.; Mehrotra, R.; Kalantar-Zadeh, K. Residual Kidney Function Decline and Mortality in Incident Hemodialysis Patients. J. Am. Soc. Nephrol. 2016, 27, 3758–3768. [Google Scholar] [CrossRef] [PubMed]
- Perl, J.; Bargman, J.M. The importance of residual kidney function for patients on dialysis: A critical review. Am. J. Kidney Dis. 2009, 53, 1068–1081. [Google Scholar] [CrossRef] [PubMed]
- Daugirdas, J.T.; Greene, T.; Rocco, M.V.; Kaysen, G.A.; Depner, T.A.; Levin, N.W.; Chertow, G.M.; Ornt, D.B.; Raimann, J.G.; Larive, B.; et al. Effect of frequent hemodialysis on residual kidney function. Kidney Int. 2013, 83, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Pham, N.M.; Montez-Rath, M.E.; Bolanos, C.G.; Bonde, S.S.; Meyer, T.W.; Sirich, T.L. Twice Weekly versus Thrice Weekly Hemodialysis—A Pilot Cross-Over Equivalence Trial. Clin. J. Am. Soc. Nephrol. 2024, 19, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Streja, E.; Rhee, C.M.; Ravel, V.; Amin, A.N.; Cupisti, A.; Chen, J.; Mathew, A.T.; Kovesdy, C.P.; Mehrotra, R.; et al. Incremental Hemodialysis, Residual Kidney Function, and Mortality Risk in Incident Dialysis Patients: A Cohort Study. Am. J. Kidney Dis. 2016, 68, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, C.; Borrelli, S.; De Stefano, T.; Provenzano, M.; Andreucci, M.; Cabiddu, G.; La Milia, V.; Vizzardi, V.; Sandrini, M.; Cancarini, G.; et al. Incremental dialysis in ESRD: Systematic review and meta-analysis. J. Nephrol. 2019, 32, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Takkavatakarn, K.; Jintanapramote, K.; Phannajit, J.; Praditpornsilpa, K.; Eiam-Ong, S.; Susantitaphong, P. Incremental versus conventional haemodialysis in end-stage kidney disease: A systematic review and meta-analysis. Clin. Kidney J. 2023, 17, sfad280. [Google Scholar] [CrossRef] [PubMed]
- Takkavatakarn, K.; Kittiskulnam, P.; Tiranathanagul, K.; Katavetin, P.; Wongyai, N.; Mahatanan, N.; Tungsanga, K.; Eiam-Ong, S.; Praditpornsilpa, K.; Susantitaphong, P. The role of once-weekly online hemodiafiltration with low protein diet for initiation of renal replacement therapy: A case series. Int. J. Artif. Organs 2021, 44, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Ahmed, S.B.; Carrero, J.J.; Foster, B.; Francis, A.; Hall, R.K.; Herrington, W.G.; Hill, G.; Inker, L.A.; Kazancıoğlu, R.; et al. Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: Known knowns and known unknowns. Kidney Int. 2024, 105, 684–701. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-gray, L.D.; Campbell, K.L.; Carrero, J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update. Am. J. Kidney Dis. 2020, 76, 1–107. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Vennegoor, M.; Ter Wee, P.; Wanner, C.; Basci, A.; Canaud, B.; Haage, P.; Konner, K.; Kooman, J.; Martin-Malo, A.; et al. EBPG guideline on nutrition. Nephrol. Dial. Transpl. 2007, 22, ii45–ii87. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D. National kidney foundation K/DOQI clinical practice guidelines for nutrition in chronic renal failure. Am. J. Kidney Dis. 2001, 37, S66–S70. [Google Scholar] [CrossRef] [PubMed]
- Garibotto, G.; Sofia, A.; Parodi, E.L.; Ansaldo, F.; Bonanni, A.; Picciotto, D.; Signori, A.; Vettore, M.; Tessari, P.; Verzola, D. Effects of Low-Protein, and Supplemented Very Low-Protein Diets, on Muscle Protein Turnover in Patients With CKD. Kidney Int. Rep. 2018, 3, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Seubsman, S.-A.; Sleigh, A. Thai SF-36 health survey: Tests of data quality, scaling assumptions, reliability, and validity in healthy men and women. Health Qual. Life Outcomes 2008, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Daugirdas, J.T. Solute solver ’what if’ module for modeling urea kinetics. Nephrol. Dial. Transplant. 2016, 31, 1934–1937. [Google Scholar] [CrossRef] [PubMed]
- Rocco, M.V.; Daugirdas, J.T.; Depner, T.A.; Inrig, J.; Mehrotra, R.; Suri, R.S.; Weiner, D.E.; Greer, N.; Ishani, A.; MacDonald, R.; et al. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am. J. Kidney Dis. 2015, 66, 884–930. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, M.; Li, H.; Yu, P.; Yuan, L.; Hao, C.; Chen, J.; Kalantar-Zadeh, K. Association of initial twice-weekly hemodialysis treatment with preservation of residual kidney function in ESRD patients. Am. J. Nephrol. 2014, 40, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Huang, J.; Wu, M.; Chu, T.; Lin, S.; Chen, Y.; Tsai, T.; Wu, K. Comparison of residual renal function in patients undergoing twice-weekly versus three-times-weekly haemodialysis. Nephrology 2009, 14, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.T.; Obi, Y.; Rhee, C.M.; Chou, J.A.; Kalantar-Zadeh, K. Incremental dialysis for preserving residual kidney function—Does one size fit all when initiating dialysis? Semin. Dial. 2018, 31, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.P.; Kalantar-Zadeh, K.; Kopple, J.D. Is there a role for ketoacid supplements in the management of CKD? Am. J. Kidney Dis. 2015, 65, 659–673. [Google Scholar] [CrossRef] [PubMed]
- Nakao, T.; Kanazawa, Y.; Takahashi, T. Once-weekly hemodialysis combined with low-protein and low-salt dietary treatment as a favorable therapeutic modality for selected patients with end-stage renal failure: A prospective observational study in japanese patients. BMC Nephrol. 2018, 19, 151. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Andrulli, S.; Pontoriero, G.; Di Filippo, S.; Bigi, M.C. Supplemented low-protein diet and once-weekly hemodialysis. Am. J. Kidney Dis. 1994, 24, 192–204. [Google Scholar] [CrossRef] [PubMed]
- Caria, S.; Cupisti, A.; Sau, G.; Bolasco, P. The incremental treatment of ESRD: A low-protein diet combined with weekly hemodialysis may be beneficial for selected patients. BMC Nephrol. 2014, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Bolasco, P.; Cupisti, A.; Locatelli, F.; Caria, S.; Kalantar-Zadeh, K. Dietary management of incremental transition to dialysis therapy: Once-weekly hemodialysis combined with low-protein diet. J. Ren. Nutr. 2016, 26, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Chewcharat, A.; Takkavatakarn, K.; Wongrattanagorn, S.; Panrong, K.; Kittiskulnam, P.; Eiam-Ong, S.; Susantitaphong, P. The Effects of Restricted Protein Diet Supplemented with Ketoanalogue on Renal Function, Blood Pressure, Nutritional Status, and Chronic Kidney Disease-Mineral and Bone Disorder in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis. J. Ren. Nutr. 2020, 30, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Ghahremani-Ghajar, M.; Rojas-Bautista, V.; Lau, W.L.; Pahl, M.; Hernandez, M.; Jin, A.; Reddy, U.; Chou, J.; Obi, Y.; Kalantar-Zadeh, K.; et al. Incremental Hemodialysis: The University of California Irvine Experience. Semin. Dial. 2017, 30, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Qian, J.; Sun, W.; Lin, A.; Cao, L.; Wang, Q.; Ni, Z.; Wan, Y.; Linholm, B.; Axelsson, J.; et al. Better preservation of residual renal function in peritoneal dialysis patients treated with a low-protein diet supplemented with keto acids: A prospective, randomized trial. Nephrol. Dial. Transplant. 2009, 24, 2551–2558. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| 1-WHD: Once-Weekly HD with Low-Protein Diet 0.6 g/kg/d Plus KAs 0.12 g/kg/day (n = 15) | 2-WHD: Twice-Weekly HD with Regular-Protein Diet 1.0–1.2 g/kg/day (n = 15) | p | |
|---|---|---|---|
| Male/Female (cases) | 9/6 | 7/8 | 0.43 |
| Age (years) | 58.0 ± 19.3 | 61.9 ± 16.8 | 0.56 |
| DM (cases) | 7/15 | 7/15 | 0.99 |
| Hypertension (cases) | 12/15 | 10/15 | 0.29 |
| Body Weight (kg) | 68.0 ± 11.7 | 61.6 ± 10.5 | 0.12 |
| BMI (kg/m2) | 24.0 ± 3.8 | 23.5 ± 3.6 | 0.71 |
| Serum BUN (mg/dL) | 75.1 ± 19.2 | 78.1 ± 17.6 | 0.65 |
| Serum Cr (mg/dL) | 8.2 ± 2.2 | 8.7 ± 2.3 | 0.51 |
| eGFR (mL/min/1.73 m2) | 6.9 ± 1.4 | 6.2 ± 1.9 | 0.26 |
| Urine Volume (mL/day) | 2226 ± 743 | 1690 ± 985 | 0.10 |
| Urine CUrea (mL/min) | 4.6 ± 2.5 | 4.1 ± 2.8 | 0.55 |
| Urine CCr (mL/min) | 8.5 ± 4.2 | 6.9 ± 2.8 | 0.23 |
| Serum Ca2+ (mg/dL) | 8.4 ± 0.7 | 8.4 ± 0.7 | 0.90 |
| Serum PO42− (mg/dL) | 4.2 ± 0.7 | 4.6 ± 1.1 | 0.37 |
| Serum K+ (mmol/L) | 4.3 ± 0.6 | 4.2 ± 0.9 | 0.50 |
| Serum Albumin (g/dL) | 3.8 ± 0.3 | 3.7 ± 0.3 | 0.20 |
| Serum Uric Acid (g/dL) | 7.8 ± 2.3 | 8.0 ± 2.4 | 0.85 |
| Hb (g/dL) | 9.0 ± 1.1 | 8.7 ± 1.1 | 0.47 |
| Serum HCO3− (mmol/L) | 22.3 ± 3.6 | 23.3 ± 3.2 | 0.44 |
| iPTH (pg/mL) | 376 ± 113 | 307 ± 172 | 0.21 |
| Serum β2-microglobulin (mg/L) | 14.9 ± 3.0 | 18.7 ± 4.7 | 0.02 |
| Serum p-cresol (μg/mL) | 7.6 ± 5.2 | 7.9 ± 5.3 | 0.88 |
| Serum Indoxyl sulfate (μg/mL) | 30.1 ± 13.6 | 28.8 ± 17.6 | 0.82 |
| Skeletal Muscle Mass (kg/m2) | 8.7 ± 3.2 | 9.9 ± 2.3 | 0.26 |
| SGA Score: (cases) | 0.15 | ||
| Class A | 14 | 11 | |
| Class B | 1 | 4 |
| Month 3 | Month 6 | Month 9 | Month 12 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1-WHD Group | 2-WHD Group | p | 1-WHD: Group | 2-WHD Group | p | 1-WHD: Group | 2-WHD Group | p | 1-WHD: Group | 2-WHD Group | p | |
| Urine CUrea (mL/min) | 3.8 ± 2.9 | 2.2 ± 1.0 | 0.06 | 3.2 ± 2.3 | 1.7 ± 1.0 | 0.03 | 2.9 ± 2.3 | 1.5 ± 0.6 | 0.03 | 3.3 ± 2.3 | 1.5 ± 1.0 | 0.01 |
| Urine CCr (mL/min) | 7.6 ± 6.4 | 6.1 ± 5.1 | 0.48 | 5.9 ± 3.6 | 3.8 ± 1.4 | 0.04 | 4.4 ± 1.8 | 3.1 ± 1.1 | 0.03 | 4.6 ± 1.9 | 2.5 ± 1.2 | 0.01 |
| Urine volume (mL/day) | 1921 ± 767 | 1305 ± 599 | 0.02 | 1859 ± 775 | 918 ± 468 | <0.01 | 1645 ± 652 | 926 ± 411 | <0.01 | 1738 ± 744 | 878 ± 464 | <0.01 |
| nPCR (g/kg/day) | 0.89 ± 0.22 | 1.08 ± 0.27 | 0.04 | 0.83 ± 0.22 | 1.09 ± 0.25 | 0.01 | 0.90 ± 0.24 | 1.05 ± 0.31 | 0.15 | 0.86 ± 0.20 | 1.10 ± 0.23 | 0.01 |
| Month 3 | Month 6 | Month 9 | Month 12 | |||||
|---|---|---|---|---|---|---|---|---|
| 1-WHD Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | |
| Hb (g/dL) | 9.6 ± 1.8 | 10.4 ± 1.1 | 10.7 ± 1.1 | 11.1 ± 1.5 | 10.8 ± 1.4 | 10.3 ± 1.0 | 10.9 ± 1.2 | 10.8 ± 0.9 |
| BUN (mg/dL) | 81.1 ± 21.3 | 77.7 ± 19.9 | 73.3 ± 14.9 | 73.1 ± 20.6 | 74.5 ± 18.8 | 75.8 ± 15.2 | 71.7 ± 18.1 | 68.9 ± 21.3 |
| Cr (mg/dL) | 9.9 ± 3.8 | 9.4 ± 2.8 | 9.8 ± 3.5 | 9.2 ± 2.5 | 10.3 ± 4.0 | 9.5 ± 2.4 | 10.1 ± 3.9 | 10.0 ± 3.0 |
| K+ (mmol/L) | 4.4 ± 0.5 | 4.2 ± 0.5 | 4.3 ± 0.5 | 4.3 ± 0.5 | 4.2 ± 0.5 | 4.2 ± 0.4 | 4.3 ± 0.6 | 4.4 ± 0.7 |
| HCO3− (mmol/L) | 22.9 ± 3.6 | 22.6 ± 3.9 | 24.1 ± 3.9 | 24.5 ± 2.8 | 23.3 ± 2.7 | 22.5 ± 2.0 | 23.7 ± 2.5 | 23.7 ± 2.8 |
| Alb (g/dL) | 4.0 ± 0.3 | 3.9 ± 0.3 | 4.0 ± 0.3 | 3.9 ± 0.3 | 3.9 ± 0.3 | 3.7 ± 0.3 | 4.0 ± 0.2 | 3.9 ± 0.3 |
| Ca2+ (mg/dL) | 8.9 ± 0.8 | 8.8 ± 0.4 | 9.1 ± 1.0 | 9.1 ± 0.7 | 9.0 ± 0.8 | 8.7 ± 0.5 | 9.0 ± 1.0 | 8.6 ± 0.9 |
| PO42− (mg/dL) | 4.3 ± 1.2 | 5.3 ± 1.2 | 4.3 ± 0.8 | 4.3 ± 0.9 | 4.4 ± 1.4 | 4.5 ± 1.4 | 4.4 ± 1.8 | 4.1 ± 1.4 |
| Uric acid (mg/dL) | 7.9 ± 1.8 | 7.3 ± 1.9 | 7.1 ± 2.1 | 7.5 ± 2.0 | 7.1 ± 1.8 | 7.0 ± 1.8 | 6.4 ± 1.8 | 6.9 ± 1.2 |
| β2M (mg/L) | - | - | 22.9 ± 9.4 | 22.2 ± 5.3 | - | - | 23.2 ± 6.9 | 22.7 ± 3.8 |
| p-cresol (μg/mL) | - | - | 5.7 ± 4.8 | 9.6 ± 5.9 | - | - | 10.4 ± 9.5 | 9.4 ± 8.1 |
| Indoxyl sulfate (μg/mL) | - | - | 39.4 ± 18.3 | 38.5 ± 5.1 | - | - | 38.9 ± 20.9 | 41.5 ± 19.0 |
| Month 3 | Month 6 | Month 9 | Month 12 | |||||
|---|---|---|---|---|---|---|---|---|
| 1-WHD Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | 1-WHD: Group | 2-WHD Group | |
| Skeletal muscle mass (kg/m2) | 8.6 ± 2.3 | 9.3 ± 1.7 | 8.6 ± 2.2 | 9.6 ± 2.7 | 8.7 ± 2.1 | 9.5 ± 1.8 | 8.7 ± 2.1 | 9.5 ± 1.7 |
| UF rate per HD (mL/kg dry weight) | 24.7 ± 20.2 | 30.8 ± 11.5 | 25.6 ± 18.9 | 33.2 ± 13.6 | 26.2± 15.4 | 36.0 ± 17.5 | 28.9 ± 15.3 | 36.4 ± 14.6 |
| Furosemide dose (mg/day) | 219 ± 305 | 329 ± 300 | 335 ± 339 | 370 ± 339 | 385 ± 318 | 610 ± 371 | 480 ± 397 | 729 ± 325 |
| SGA score: (cases) | ||||||||
| Class A | 13 | 13 | 14 | 13 | 14 | 13 | 14 | 14 |
| Class B | 2 | 2 | 1 | 2 | 1 | 2 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kittiskulnam, P.; Tiranathanagul, K.; Susantitaphong, P.; Phannajit, J.; Chongpison, Y.; Asavapujanamanee, P.; Surattichaiyakul, B.; Takkavatakarn, K.; Katavetin, P.; Metta, K.; et al. Stepwise Incremental Hemodialysis and Low-Protein Diet Supplemented with Keto-Analogues Preserve Residual Kidney Function: A Randomized Controlled Trial. Nutrients 2025, 17, 2422. https://doi.org/10.3390/nu17152422
Kittiskulnam P, Tiranathanagul K, Susantitaphong P, Phannajit J, Chongpison Y, Asavapujanamanee P, Surattichaiyakul B, Takkavatakarn K, Katavetin P, Metta K, et al. Stepwise Incremental Hemodialysis and Low-Protein Diet Supplemented with Keto-Analogues Preserve Residual Kidney Function: A Randomized Controlled Trial. Nutrients. 2025; 17(15):2422. https://doi.org/10.3390/nu17152422
Chicago/Turabian StyleKittiskulnam, Piyawan, Khajohn Tiranathanagul, Paweena Susantitaphong, Jeerath Phannajit, Yuda Chongpison, Pagaporn Asavapujanamanee, Bongkod Surattichaiyakul, Kullaya Takkavatakarn, Pisut Katavetin, Kamonchanok Metta, and et al. 2025. "Stepwise Incremental Hemodialysis and Low-Protein Diet Supplemented with Keto-Analogues Preserve Residual Kidney Function: A Randomized Controlled Trial" Nutrients 17, no. 15: 2422. https://doi.org/10.3390/nu17152422
APA StyleKittiskulnam, P., Tiranathanagul, K., Susantitaphong, P., Phannajit, J., Chongpison, Y., Asavapujanamanee, P., Surattichaiyakul, B., Takkavatakarn, K., Katavetin, P., Metta, K., & Praditpornsilpa, K. (2025). Stepwise Incremental Hemodialysis and Low-Protein Diet Supplemented with Keto-Analogues Preserve Residual Kidney Function: A Randomized Controlled Trial. Nutrients, 17(15), 2422. https://doi.org/10.3390/nu17152422