
Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake
 , ,
, ,  , ,
, ,  ,
, 
Abstract

1. Introduction
2. Search Methods
3. General Effects of Magnesium on Hormonal Balance and Metabolism
3.1. Magnesium and Thyroid Hormone Regulation
3.2. Magnesium on Cortisol and Stress Regulation
3.3. Magnesium’s Role in Insulin Sensitivity, Glucose Homeostasis and Vascular Health
4. Magnesium Deficiency: Epidemiological Data and Health Implications
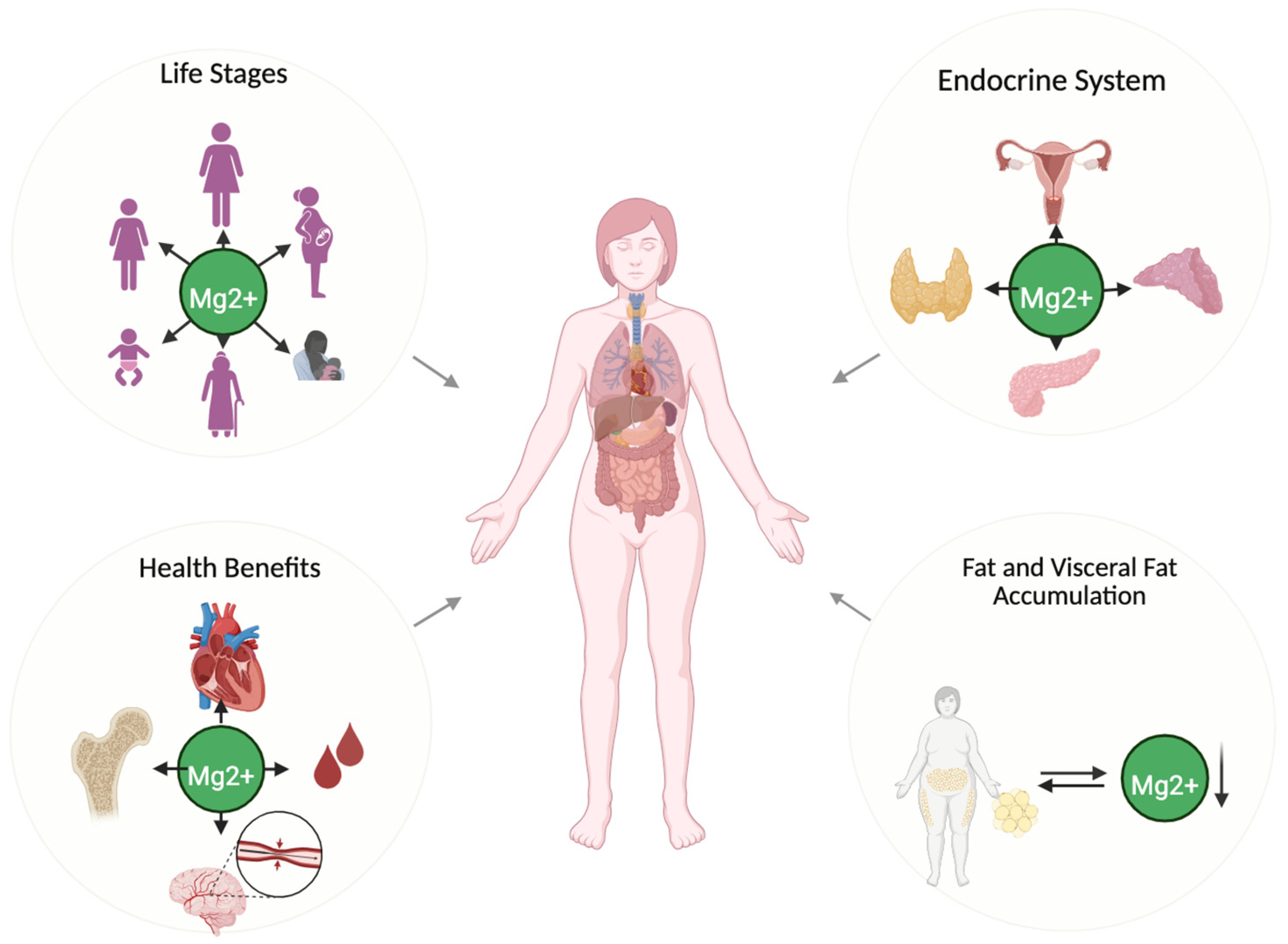
5. Magnesium and Gender Differences: Physiological and Metabolic Implications
5.1. Magnesium and Women’s Physiology: A Key Nutrient in Health
5.1.1. Menstrual Cycle and Premenstrual Syndrome (PMS): Magnesium’s Role in Symptom Modulation
5.1.2. Magnesium, Body Composition, and Visceral Fat Regulation in Women
5.2. Magnesium and Male Physiology: Roles and Health Implications
5.2.1. Magnesium on Sex Hormones and Testosterone Levels
5.2.2. Muscle Mass in Men
5.2.3. Fat Mass and Visceral Fat
6. Strategies for Enhancing Magnesium Status and Preventing Deficiency
6.1. Dietary Sources of Magnesium and Gender-Specific Needs
Magnesium-Rich Foods and Dietary Sources
6.2. Magnesium and Factors Influencing Bioavailability
Dietary and Nutritional Factors Affecting Magnesium Bioavailability
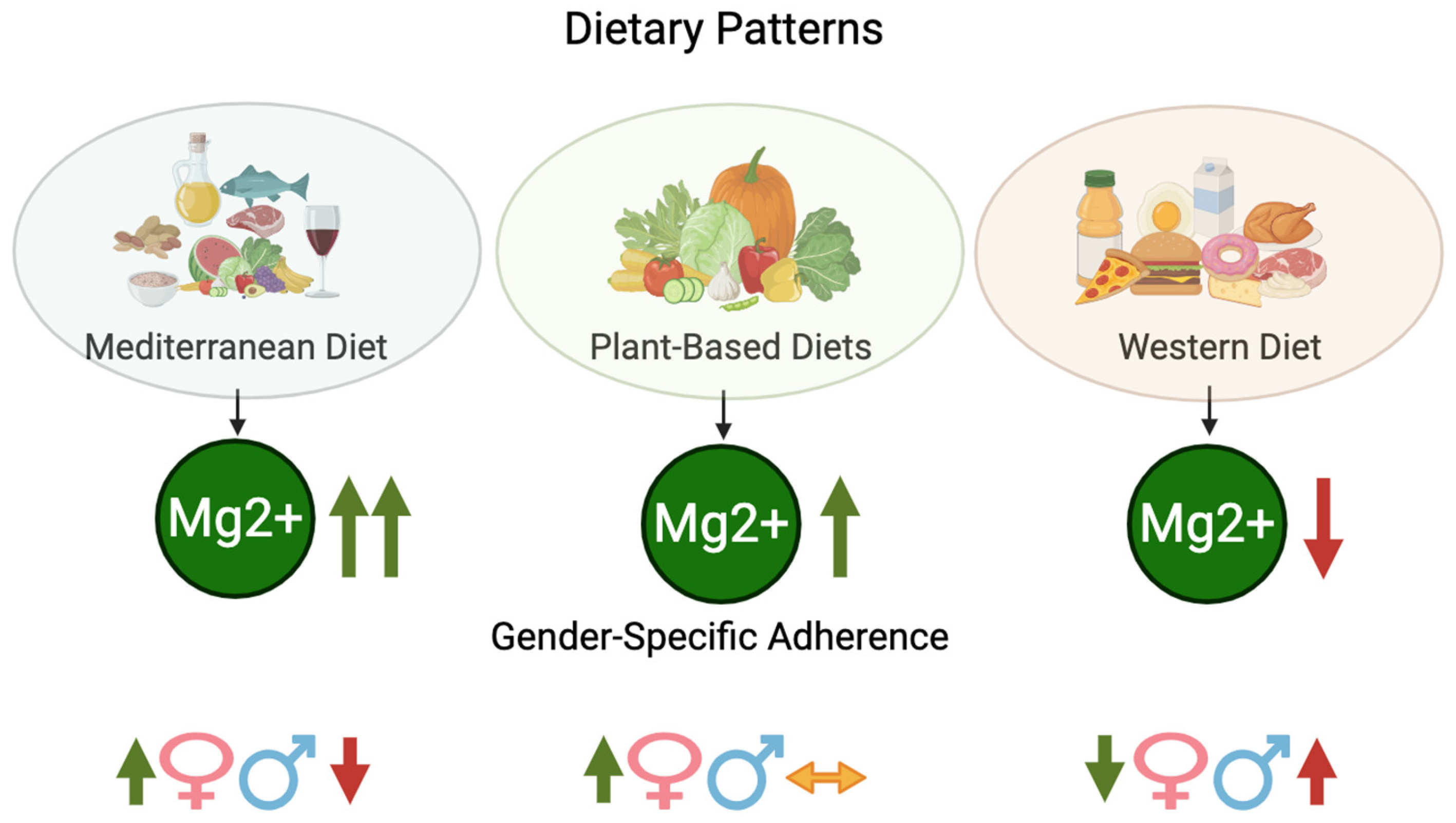
6.3. Dietary Patterns and Magnesium: A Gender Perspective
6.3.1. Mediterranean Diet
6.3.2. Plant-Based Diets
6.3.3. Western Diet
7. Dietary Strategies and Supplementation for Optimizing Magnesium Intake: A Gender-Perspective Magnesium Intake Through Diet and Supplementation
- Increasing Magnesium-Rich Food Consumption. Individuals following plant-based dietary patterns, such as the Mediterranean or vegetarian diets, typically exhibit higher magnesium intake compared to those adhering to conventional Western diets, which are often low in whole grains, fruits, vegetables, and nuts. These plant-based diets are naturally richer in magnesium, making them a beneficial strategy to improve magnesium status. The most straightforward method for enhancing magnesium intake is through the consumption of magnesium-rich foods. Leafy green vegetables (e.g., spinach, kale), legumes (e.g., beans, lentils), nuts and seeds (e.g., almonds, pumpkin seeds), whole grains (e.g., brown rice, quinoa), and certain fish (e.g., mackerel, salmon) are all excellent sources of magnesium. For example, 100 g of cooked spinach provide approximately 79 mg of magnesium, while 30 g (about one ounce) of almonds contain around 81 mg. Similarly, 30 g of pumpkin seeds can provide up to 150 mg, and 100 g of cooked quinoa provide approximately 64 mg of magnesium. Incorporating these foods into daily meals can significantly help meet the recommended dietary intake of magnesium.
- Optimizing Magnesium Absorption. The bioavailability of magnesium in foods can be influenced by several factors. Phytates, found in whole grains and legumes, as well as oxalates, present in certain leafy vegetables, can bind magnesium and hinder its absorption. To counteract these effects, specific food preparation techniques can be utilized, such as soaking, fermenting, or sprouting grains and legumes. These methods help break down phytates and enhance the bioavailability of magnesium for absorption. Moreover, vitamin D plays a critical role in optimizing magnesium absorption in the gastrointestinal tract [139]. Ensuring sufficient vitamin D levels, either through sunlight exposure or dietary sources (e.g., fatty fish, fortified foods), can further improve magnesium intake and its overall bioavailability.
- Addressing Magnesium Losses in the Diet. Magnesium intake can be compromised not only by inadequate consumption of magnesium-rich foods but also by factors that increase magnesium excretion. Diets high in processed foods, sugar-sweetened beverages, and excessive alcohol intake can lead to greater magnesium losses through urine. As a result, reducing the consumption of these foods and beverages is an important strategy in supporting magnesium retention and balance. Additionally, variations in digestive function may influence magnesium absorption, making dietary adjustments a useful strategy in optimizing intake.
- Magnesium Supplementation. When dietary intake alone is inadequate, magnesium supplementation may be an option. Supplements are available in various forms, such as magnesium citrate, magnesium oxide, and magnesium glycinate, each differing in absorption rates and bioavailability. The choice of supplementation should be individualized, particularly for those with higher magnesium needs, such as older adults and individuals following restricted diets. Healthcare professionals can provide guidance on the most suitable forms and dosages to optimize magnesium intake.
- Public Health Recommendations and Education. Public health initiatives and nutrition education programs play a key role in raising awareness about magnesium’s importance in nutrition. These efforts should aim to inform populations about the advantages of magnesium-rich foods, effective food preparation techniques to improve absorption, and the potential consequences of excessive magnesium loss. Furthermore, dietary guidelines should emphasize magnesium intake as an integral part of achieving overall nutritional adequacy.
8. Conclusions and Future Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- de Baaij, J.H.F.; Hoenderop, J.G.J.; Bindels, R.J.M. Magnesium in Man: Implications for Health and Disease. Physiol. Rev. 2015, 95, 1–46. [Google Scholar] [CrossRef]
- Al Alawi, A.M.; Majoni, S.W.; Falhammar, H. Magnesium and Human Health: Perspectives and Research Directions. Int. J. Endocrinol. 2018, 2018, 9041694. [Google Scholar] [CrossRef]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef]
- Dutta, P.; Layton, A.T. Modeling Calcium and Magnesium Balance: Regulation by Calciotropic Hormones and Adaptations Under Varying Dietary Intake. iScience 2024, 27, 111077. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Magnesium. EFSA J. 2015, 13, 4186. [Google Scholar]
- Olza, J.; Aranceta-Bartrina, J.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, A. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef]
- Fatima, G.; Dzupina, A.; BAlhmadi, H.; Magomedova, A.; Siddiqui, Z.; Mehdi, A.; Hadi, N. Magnesium Matters: A Comprehensive Review of its Vital Role in Health and Diseases. Cureus 2024, 16, e71392. [Google Scholar] [CrossRef]
- Song, J.; Zhang, Y.; Lin, Z.; Tang, J.; Yang, X.; Liu, F. Higher Magnesium Depletion Score Increases the Risk of all-Cause and Cardiovascular Mortality in Hypertension Participants. Biol. Trace Elem. Res. 2024, 203, 1287–1296. [Google Scholar] [CrossRef]
- Kumar, S.R.; Kumar, K.G.S.; Gayathri, R. Hypomagnesemia in Patients with Type 2 Diabetes Mellitus. J. Assoc. Physicians India 2024, 72, 25–28. [Google Scholar]
- Kokubo, Y.; Saito, I.; Iso, H.; Yamagishi, K.; Yatsuya, H.; Ishihara, J.; Maruyama, K.; Inoue, M.; Sawada, N.; Tsugane, S.; et al. Dietary Magnesium Intake and Risk of Incident Coronary Heart Disease in Men: A Prospective Cohort Study. Clin. Nutr. 2018, 37, 1602–1608. [Google Scholar] [CrossRef]
- Zhao, L.; Hu, M.; Yang, L.; Xu, H.; Song, W.; Qian, Y.; Zhao, M. Quantitative Association between Serum/Dietary Magnesium and Cardiovascular Disease/Coronary Heart Disease Risk: A Dose-Response Meta-Analysis of Prospective Cohort Studies. J. Cardiovasc. Pharmacol. 2019, 74, 516–527. [Google Scholar] [CrossRef]
- Swaminathan, R. Magnesium Metabolism and its Disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar]
- Liu, L.; Luo, P.; Wen, P.; Xu, P. The Role of Magnesium in the Pathogenesis of Osteoporosis. Front. Endocrinol. 2024, 15, 1406248. [Google Scholar] [CrossRef]
- Mazza, E.; Troiano, E.; Ferro, Y.; Lisso, F.; Tosi, M.; Turco, E.; Pujia, R.; Montalcini, T. Obesity, Dietary Patterns, and Hormonal Balance Modulation: Gender-Specific Impacts. Nutrients 2024, 16, 1629. [Google Scholar] [CrossRef]
- Conforto, R.; Rizzo, V.; Russo, R.; Mazza, E.; Maurotti, S.; Pujia, C.; Succurro, E.; Arturi, F.; Ferro, Y.; Sciacqua, A.; et al. Advances in Body Composition and Gender Differences in Susceptibility to Frailty Syndrome: Role of Osteosarcopenic Obesity. Metabolism 2024, 161, 156052. [Google Scholar] [CrossRef]
- Fiorentini, D.; Cappadone, C.; Farruggia, G.; Prata, C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to its Deficiency. Nutrients 2021, 13, 1136. [Google Scholar] [CrossRef]
- Uwitonze, A.M.; Razzaque, M.S. Role of Magnesium in Vitamin D Activation and Function. J. Am. Osteopath. Assoc. 2018, 118, 181–189. [Google Scholar] [CrossRef]
- Castiglioni, S.; Cazzaniga, A.; Albisetti, W.; Maier, J.A.M. Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions. Nutrients 2013, 5, 3022–3033. [Google Scholar] [CrossRef]
- Rude, R.K.; Gruber, H.E. Magnesium Deficiency and Osteoporosis: Animal and Human Observations. J. Nutr. Biochem. 2004, 15, 710–716. [Google Scholar] [CrossRef]
- Kopp, P.; Cooper, D.S.; Braverman, L.E. Werner and Ingbar’s the Thyroid: A Fundamental and Clinical Text; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Rifai, N. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics-E-Book: Tietz Textbook of Clinical Chemistry and Molecular Diagnostics-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Kolanu, B.R.; Vadakedath, S.; Boddula, V.; Kandi, V. Activities of Serum Magnesium and Thyroid Hormones in Pre-, Peri-, and Post-Menopausal Women. Cureus 2020, 12, e6554. [Google Scholar] [CrossRef]
- Pickering, G.; Mazur, A.; Trousselard, M.; Bienkowski, P.; Yaltsewa, N.; Amessou, M.; Noah, L.; Pouteau, E. Magnesium Status and Stress: The Vicious Circle Concept Revisited. Nutrients 2020, 12, 3672. [Google Scholar] [CrossRef]
- Mbiydzenyuy, N.E.; Qulu, L. Stress, Hypothalamic-Pituitary-Adrenal Axis, Hypothalamic-Pituitary-Gonadal Axis, and Aggression. Metab. Brain Dis. 2024, 39, 1613–1636. [Google Scholar] [CrossRef]
- Sartori, S.B.; Whittle, N.; Hetzenauer, A.; Singewald, N. Magnesium Deficiency Induces Anxiety and HPA Axis Dysregulation: Modulation by Therapeutic Drug Treatment. Neuropharmacology 2012, 62, 304–312. [Google Scholar] [CrossRef]
- Cazzola, R.; Della Porta, M.; Piuri, G.; Maier, J.A. Magnesium: A Defense Line to Mitigate Inflammation and Oxidative Stress in Adipose Tissue. Antioxidants 2024, 13, 893. [Google Scholar] [CrossRef]
- Akarachkova, E. The Role of Magnesium Deficiency in the Formation of Clinical Manifestation of Stress in Women. Probl. Women Health 2013, 8, 57. [Google Scholar]
- Akimbekov, N.S.; Coban, S.O.; Atfi, A.; Razzaque, M.S. The Role of Magnesium in Pancreatic Beta-Cell Function and Homeostasis. Front. Nutr. 2024, 11, 1458700. [Google Scholar] [CrossRef]
- Oost, L.J.; Kurstjens, S.; Ma, C.; Hoenderop, J.G.J.; Tack, C.J.; de Baaij, J.H.F. Magnesium Increases Insulin-Dependent Glucose Uptake in Adipocytes. Front. Endocrinol. 2022, 13, 986616. [Google Scholar] [CrossRef]
- Petersen, M.C.; Shulman, G.I. Mechanisms of Insulin Action and Insulin Resistance. Physiol. Rev. 2018, 98, 2133–2223. [Google Scholar] [CrossRef]
- Hamilton, K.P.; Zelig, R.; Parker, A.R.; Haggag, A. Insulin Resistance and Serum Magnesium Concentrations among Women with Polycystic Ovary Syndrome. Curr. Dev. Nutr. 2019, 3, nzz108. [Google Scholar] [CrossRef]
- Veronese, N.; Dominguez, L.J.; Pizzol, D.; Demurtas, J.; Smith, L.; Barbagallo, M. Oral Magnesium Supplementation for Treating Glucose Metabolism Parameters in People with Or at Risk of Diabetes: A Systematic Review and Meta-Analysis of Double-Blind Randomized Controlled Trials. Nutrients 2021, 13, 4074. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Magnesium Improves the Beta-cell Function to Compensate Variation of Insulin Sensitivity: Double-blind, Randomized Clinical Trial. Eur. J. Clin. Investig. 2011, 41, 405–410. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Tamez-Perez, H.E.; Gonzalez-Gonzalez, G.e.; Salinas-Martinez, A.M.; Montes-Villarreal, J.; Trevino-Ortiz, J.H.; Rodriguez-Moran, M. Oral Magnesium Supplementation Improves Insulin Sensitivity in Non-Diabetic Subjects with Insulin Resistance. A Double-Blind Placebo-Controlled Randomized Trial. Diabetes Metab. 2004, 30, 253–258. [Google Scholar] [CrossRef]
- Shechter, M. Magnesium and Cardiovascular System. Magnes. Res. 2010, 23, 60–72. [Google Scholar]
- Liu, M.; Dudley, S.C.J. Magnesium, Oxidative Stress, Inflammation, and Cardiovascular Disease. Antioxidants 2020, 9, 907. [Google Scholar] [CrossRef]
- AlShanableh, Z.; Ray, E.C. Magnesium in Hypertension: Mechanisms and Clinical Implications. Front. Physiol. 2024, 15, 1363975. [Google Scholar] [CrossRef]
- Fang, X.; Han, H.; Li, M.; Liang, C.; Fan, Z.; Aaseth, J.; He, J.; Montgomery, S.; Cao, Y. Dose-Response Relationship between Dietary Magnesium Intake and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Regression Analysis of Prospective Cohort Studies. Nutrients 2016, 8, 739. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodriguez-Moran, M. Low Serum Magnesium Levels and Metabolic Syndrome. Acta Diabetol. 2002, 39, 209–213. [Google Scholar] [CrossRef]
- Adebamowo, S.N.; Spiegelman, D.; Willett, W.C.; Rexrode, K.M. Association between Intakes of Magnesium, Potassium, and Calcium and Risk of Stroke: 2 Cohorts of US Women and Updated Meta-Analyses. Am. J. Clin. Nutr. 2015, 101, 1269–1277. [Google Scholar] [CrossRef]
- Nie, Z.; Wang, Z.; Zhou, B.; Tang, Z.; Wang, S. Magnesium Intake and Incidence of Stroke: Meta-Analysis of Cohort Studies. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 169–176. [Google Scholar] [CrossRef]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y. Dietary Magnesium Intake and the Risk of Cardiovascular Disease, Type 2 Diabetes, and all-Cause Mortality: A Dose–response Meta-Analysis of Prospective Cohort Studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef]
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time has Come. Adv. Nutr. 2016, 7, 977–993. [Google Scholar] [CrossRef]
- Workinger, J.L.; Doyle, R.P.; Bortz, J. Challenges in the Diagnosis of Magnesium Status. Nutrients 2018, 10, 1202. [Google Scholar] [CrossRef]
- Pelczyńska, M.; Moszak, M.; Bogdański, P. The Role of Magnesium in the Pathogenesis of Metabolic Disorders. Nutrients 2022, 14, 1714. [Google Scholar] [CrossRef]
- Maggio, M.; De Vita, F.; Lauretani, F.; Nouvenne, A.; Meschi, T.; Ticinesi, A.; Dominguez, L.J.; Barbagallo, M.; Dall’aglio, E.; Ceda, G.P. The Interplay between Magnesium and Testosterone in Modulating Physical Function in Men. Int. J. Endocrinol. 2014, 2014, 525249. [Google Scholar] [CrossRef]
- Takeda, Y. Understanding the Life Stages of Women to Enhance Your Practice. JMAJ 2010, 53, 273–278. [Google Scholar]
- DiNicolantonio, J.J.; O’Keefe, J.H.; Wilson, W. Subclinical Magnesium Deficiency: A Principal Driver of Cardiovascular Disease and a Public Health Crisis. Open Heart 2018, 5, e000668. [Google Scholar] [CrossRef]
- Porri, D.; Biesalski, H.K.; Limitone, A.; Bertuzzo, L.; Cena, H. Effect of Magnesium Supplementation on Women’s Health and Well-Being. NFS J. 2021, 23, 30–36. [Google Scholar] [CrossRef]
- Fouhy, L.E.; Mangano, K.M.; Zhang, X.; Hughes, B.D.; Tucker, K.L.; Noel, S.E. Association between a Calcium-to-Magnesium Ratio and Osteoporosis among Puerto Rican Adults. J. Nutr. 2023, 153, 2642–2650. [Google Scholar] [CrossRef]
- Shukla, V.; Parvez, S.; Fatima, G.; Singh, S.; Magomedova, A.; Batiha, G.E.; Alexiou, A.; Papadakis, M.; Welson, N.N.; Hadi, N. Micronutrient Interactions: Magnesium and its Synergies in Maternal-Fetal Health. Food Sci. Nutr. 2024, 12, 6913–6928. [Google Scholar] [CrossRef]
- Tonick, S.; Muneyyirci-Delale, O. Magnesium in Women’s Health and Gynecology. Open J. Obstet. Gynecol. 2016, 6, 325–333. [Google Scholar] [CrossRef]
- Parazzini, F.; Di Martino, M.; Pellegrino, P. Magnesium in the Gynecological Practice: A Literature Review. Magnes. Res. 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Mazza, E.; Troiano, E.; Mazza, S.; Ferro, Y.; Abbinante, A.; Agneta, M.T.; Montalcini, T.; Pujia, A. The Impact of Endometriosis on Dietary Choices and Activities of Everyday Life: A Cross-Sectional Study. Front. Nutr. 2023, 10, 1273976. [Google Scholar] [CrossRef]
- Botturi, A.; Ciappolino, V.; Delvecchio, G.; Boscutti, A.; Viscardi, B.; Brambilla, P. The Role and the Effect of Magnesium in Mental Disorders: A Systematic Review. Nutrients 2020, 12, 1661. [Google Scholar] [CrossRef]
- Naraoka, Y.; Hosokawa, M.; Minato-Inokawa, S.; Sato, Y. Severity of Menstrual Pain is Associated with Nutritional Intake and Lifestyle Habits. Healthcare 2023, 11, 1289. [Google Scholar] [CrossRef]
- Saeedian Kia, A.; Amani, R.; Cheraghian, B. The Association between the Risk of Premenstrual Syndrome and Vitamin D, Calcium, and Magnesium Status among University Students: A Case Control Study. Health Promot. Perspect. 2015, 5, 225–230. [Google Scholar] [CrossRef]
- Oboza, P.; Ogarek, N.; Wójtowicz, M.; Rhaiem, T.B.; Olszanecka-Glinianowicz, M.; Kocełak, P. Relationships between Premenstrual Syndrome (PMS) and Diet Composition, Dietary Patterns and Eating Behaviors. Nutrients 2024, 16, 1911. [Google Scholar] [CrossRef]
- Sahin, S.; Ozdemir, K.; Unsal, A. Evaluation of Premenstrual Syndrome and Quality of Life in University Students. J. Pak. Med. Assoc. 2014, 64, 915–922. [Google Scholar]
- Kapper, C.; Oppelt, P.; Ganhör, C.; Gyunesh, A.A.; Arbeithuber, B.; Stelzl, P.; Rezk-Füreder, M. Minerals and the Menstrual Cycle: Impacts on Ovulation and Endometrial Health. Nutrients 2024, 16, 1008. [Google Scholar] [CrossRef]
- Kostov, K. Effects of Magnesium Deficiency on Mechanisms of Insulin Resistance in Type 2 Diabetes: Focusing on the Processes of Insulin Secretion and Signaling. Int. J. Mol. Sci. 2019, 20, 1351. [Google Scholar] [CrossRef]
- Zendehdel, M.; Elyasi, F. Biopsychosocial Etiology of Premenstrual Syndrome: A Narrative Review. J. Fam. Med. Prim. Care 2018, 7, 346–356. [Google Scholar] [CrossRef]
- Connolly, M. Premenstrual Syndrome: An Update on Definitions, Diagnosis and Management. Adv. Psychiatr. Treat. 2001, 7, 469–477. [Google Scholar] [CrossRef]
- Costanian, C.; Akiki, Z.; Rabah, Z.; Daou, S.; Assaad, S. Factors Associated with Premenstrual Syndrome and its Different Symptom Domains among University Students in Lebanon. Int. J. Womens Health Wellness 2018, 4, 68. [Google Scholar]
- Siminiuc, R.; Ţurcanu, D. Impact of Nutritional Diet Therapy on Premenstrual Syndrome. Front. Nutr. 2023, 10, 1079417. [Google Scholar] [CrossRef]
- Facchinetti, F.; Sances, G.; Borella, P.; Genazzani, A.R.; Nappi, G. Magnesium Prophylaxis of Menstrual Migraine: Effects on Intracellular Magnesium. Headache 1991, 31, 298–301. [Google Scholar] [CrossRef]
- Quaranta, S.; Buscaglia, M.A.; Meroni, M.G.; Colombo, E.; Cella, S. Pilot Study of the Efficacy and Safety of a Modified-Release Magnesium 250 mg Tablet (Sincromag) for the Treatment of Premenstrual Syndrome. Clin. Drug Investig. 2007, 27, 51–58. [Google Scholar] [CrossRef]
- Walker, A.F.; De Souza, M.C.; Vickers, M.F.; Abeyasekera, S.; Collins, M.L.; Trinca, L.A. Magnesium Supplementation Alleviates Premenstrual Symptoms of Fluid Retention. J. Womens Health 1998, 7, 1157–1165. [Google Scholar] [CrossRef]
- Rosenstein, D.L.; Elin, R.J.; Hosseini, J.M.; Grover, G.; Rubinow, D.R. Magnesium Measures Across the Menstrual Cycle in Premenstrual Syndrome. Biol. Psychiatry 1994, 35, 557–561. [Google Scholar] [CrossRef]
- Yaralizadeh, M.; Nezamivand-Chegini, S.; Najar, S.; Namjoyan, F.; Abedi, P. Effectiveness of Magnesium on Menstrual Symptoms among Dysmenorrheal College Students: A Randomized Controlled Trial. Int. J. Women’s Health Reprod. Sci. 2024, 12, 70–76. [Google Scholar] [CrossRef]
- Sultan, C.; Gaspari, L.; Paris, F. Adolescent Dysmenorrhea. Endocr Dev. 2012, 22, 171–180. [Google Scholar]
- Christensen, K. Dysmenorrhoea: An Update on Primary Healthcare Management. Aust. J. Gen. Pract. 2024, 53, 19–22. [Google Scholar] [CrossRef]
- Rubio Perez, G.; Quevedo Cordoba, A.; Varela Silva, L.; Alvarez Silvares, E. Update on the Diagnosis and Treatment of Dysmenorrhoea. Semergen 2025, 51, 102331. [Google Scholar]
- Seifert, B.; Wagler, P.; Dartsch, S.; Schmidt, U.; Nieder, J. Magnesium—A New Therapeutic Alternative in Primary Dysmenorrhea. Zentralbl. Gynakol. 1989, 111, 755–760. [Google Scholar]
- Proctor, M.L.; Murphy, P.A. Herbal and Dietary Therapies for Primary and Secondary Dysmenorrhoea. Cochrane Database Syst. Rev. 2001, 3, CD002124. [Google Scholar]
- Benassi, L.; Barletta, F.P.; Baroncini, L.; Bertani, D.; Filippini, F.; Beski, L.; Nani, A.; Tesauri, P.; Tridenti, G. Effectiveness of Magnesium Pidolate in the Prophylactic Treatment of Primary Dysmenorrhea. Clin. Exp. Obstet. Gynecol. 1992, 19, 176–179. [Google Scholar]
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F.; AMPP Advisory Group. Migraine Prevalence, Disease Burden, and the Need for Preventive Therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef]
- Diener, H.; Solbach, K.; Holle, D.; Gaul, C. Integrated Care for Chronic Migraine Patients: Epidemiology, Burden, Diagnosis and Treatment Options. Clin. Med. 2015, 15, 344–350. [Google Scholar] [CrossRef]
- Peikert, A.; Wilimzig, C.; Köhne-Volland, R. Prophylaxis of Migraine with Oral Magnesium: Results from a Prospective, Multi-Center, Placebo-Controlled and Double-Blind Randomized Study. Cephalalgia 1996, 16, 257–263. [Google Scholar] [CrossRef]
- Bigal, M.E.; Bordini, C.A.; Tepper, S.J.; Speciali, J.G. Intravenous Magnesium Sulphate in the Acute Treatment of Migraine without Aura and Migraine with Aura. A Randomized, Double-Blind, Placebo-Controlled Study. Cephalalgia 2002, 22, 345–353. [Google Scholar] [CrossRef]
- Laarakker, M.C.; van Lith, H.A.; Ohl, F. Behavioral Characterization of A/J and C57BL/6J Mice using a Multidimensional Test: Association between Blood Plasma and Brain Magnesium-Ion Concentration with Anxiety. Physiol. Behav. 2011, 102, 205–219. [Google Scholar] [CrossRef]
- Parashar, R.; Bhalla, P.; Rai, N.K.; Pakhare, A.; Babbar, R. Migraine: Is it Related to Hormonal Disturbances or Stress? Int. J. Womens Health 2014, 6, 921–925. [Google Scholar] [CrossRef]
- Kodoth, V.; Scaccia, S.; Aggarwal, B. Adverse Changes in Body Composition during the Menopausal Transition and Relation to Cardiovascular Risk: A Contemporary Review. Womens Health Rep. 2022, 3, 573–581. [Google Scholar] [CrossRef]
- Babapour, M.; Mohammadi, H.; Kazemi, M.; Hadi, A.; Rezazadegan, M.; Askari, G. Associations between Serum Magnesium Concentrations and Polycystic Ovary Syndrome Status: A Systematic Review and Meta-Analysis. Biol. Trace Elem. Res. 2021, 199, 1297–1305. [Google Scholar] [CrossRef]
- Askari, M.; Mozaffari, H.; Jafari, A.; Ghanbari, M.; Darooghegi Mofrad, M. The Effects of Magnesium Supplementation on Obesity Measures in Adults: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 2921–2937. [Google Scholar] [CrossRef]
- Castellanos-Gutiérrez, A.; Sánchez-Pimienta, T.G.; Carriquiry, A.; da Costa, T.H.M.; Ariza, A.C. Higher Dietary Magnesium Intake is Associated with Lower Body Mass Index, Waist Circumference and Serum Glucose in Mexican Adults. Nutr. J. 2018, 17, 114. [Google Scholar] [CrossRef]
- Souza, A.C.R.; Vasconcelos, A.R.; Dias, D.D.; Komoni, G.; Name, J.J. The Integral Role of Magnesium in Muscle Integrity and Aging: A Comprehensive Review. Nutrients 2023, 15, 5127. [Google Scholar] [CrossRef]
- Groenendijk, I.; van Delft, M.; Versloot, P.; van Loon, L.J.C.; de Groot, L.C.P.G.M. Impact of Magnesium on Bone Health in Older Adults: A Systematic Review and Meta-Analysis. Bone 2022, 154, 116233. [Google Scholar] [CrossRef]
- Touyz, R.M. Transient Receptor Potential Melastatin 6 and 7 Channels, Magnesium Transport, and Vascular Biology: Implications in Hypertension. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, 1103. [Google Scholar] [CrossRef]
- Houston, M. The Role of Magnesium in Hypertension and Cardiovascular Disease. J. Clin. Hypertens. 2011, 13, 843–847. [Google Scholar] [CrossRef]
- Morais, J.B.S.; Severo, J.S.; de Alencar, G.R.R.; de Oliveira, A.R.S.; Cruz, K.J.C.; Marreiro, D.d.N.; Freitas, B.d.J.e.S.d.A.; de Carvalho, C.M.R.; do Carmo de Carvalho e Martins, M.; Frota, K.d.M.G. Effect of Magnesium Supplementation on Insulin Resistance in Humans: A Systematic Review. Nutrition 2017, 38, 54–60. [Google Scholar] [CrossRef]
- Maggio, M.; Ceda, G.P.; Lauretani, F.; Cattabiani, C.; Avantaggiato, E.; Morganti, S.; Ablondi, F.; Bandinelli, S.; Dominguez, L.J.; Barbagallo, M.; et al. Magnesium and Anabolic Hormones in Older Men. Int. J. Androl. 2011, 34, 594. [Google Scholar] [CrossRef]
- Arianayagam, R.; Arianayagam, M.; McGrath, S.; Rashid, P. Androgen Deficiency in the Aging Man. Aust. Fam. Physician 2010, 39, 752–755. [Google Scholar]
- Cinar, V.; Polat, Y.; Baltaci, A.K.; Mogulkoc, R. Effects of Magnesium Supplementation on Testosterone Levels of Athletes and Sedentary Subjects at Rest and After Exhaustion. Biol. Trace Elem. Res. 2011, 140, 18–23. [Google Scholar] [CrossRef]
- Green, D.J.; Chasland, L.C.; Yeap, B.B.; Naylor, L.H. Comparing the Impacts of Testosterone and Exercise on Lean Body Mass, Strength and Aerobic Fitness in Aging Men. Sports Med. Open 2024, 10, 30. [Google Scholar] [CrossRef]
- Liguori, S.; Moretti, A.; Paoletta, M.; Gimigliano, F.; Iolascon, G. Role of Magnesium in Skeletal Muscle Health and Neuromuscular Diseases: A Scoping Review. Int. J. Mol. Sci. 2024, 25, 11220. [Google Scholar] [CrossRef]
- Lukaski, H.C. Vitamin and Mineral Status: Effects on Physical Performance. Nutrition 2004, 20, 632–644. [Google Scholar] [CrossRef]
- Brilla, L.R.; Conte, V. Effects of a Novel Zinc-Magnesium Formulation on Hormones and Strength. J. Exerc. Physiol. Online 2000, 3, 26–36. [Google Scholar]
- Dickens, B.F.; Weglicki, W.B.; Li, Y.; Mak, I.T. Magnesium Deficiency in Vitro Enhances Free Radical-Induced Intracellular Oxidation and Cytotoxicity in Endothelial Cells. FEBS Lett. 1992, 311, 187–191. [Google Scholar] [CrossRef]
- Short, K.R.; Bigelow, M.L.; Kahl, J.; Singh, R.; Coenen-Schimke, J.; Raghavakaimal, S.; Nair, K.S. Decline in Skeletal Muscle Mitochondrial Function with Aging in Humans. Proc. Natl. Acad. Sci. USA 2005, 102, 5618–5623. [Google Scholar] [CrossRef]
- Rayssiguier, Y.; Durlach, J.; Gueux, E.; Rock, E.; Mazur, A. Magnesium and Ageing. I. Experimental Data: Importance of Oxidative Damage. Magnes. Res. 1993, 6, 369–378. [Google Scholar]
- Schaap, L.A.; Pluijm, S.M.F.; Deeg, D.J.H.; Visser, M. Inflammatory Markers and Loss of Muscle Mass (Sarcopenia) and Strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef]
- Nauli, A.M.; Matin, S. Why do Men Accumulate Abdominal Visceral Fat? Front. Physiol. 2019, 10, 1486. [Google Scholar] [CrossRef]
- Kuk, J.L.; Katzmarzyk, P.T.; Nichaman, M.Z.; Church, T.S.; Blair, S.N.; Ross, R. Visceral Fat is an Independent Predictor of all-Cause Mortality in Men. Obesity 2006, 14, 336–341. [Google Scholar] [CrossRef]
- Venu, L.; Padmavathi, I.J.; Kishore, Y.D.; Bhanu, N.V.; Rao, K.R.; Sainath, P.B.; Ganeshan, M.; Raghunath, M. Long-term Effects of Maternal Magnesium Restriction on Adiposity and Insulin Resistance in Rat Pups. Obesity 2008, 16, 1270–1276. [Google Scholar] [CrossRef]
- He, K.; Liu, K.; Daviglus, M.L.; Morris, S.J.; Loria, C.M.; Van Horn, L.; Jacobs, D.R.J.; Savage, P.J. Magnesium Intake and Incidence of Metabolic Syndrome among Young Adults. Circulation 2006, 113, 1675–1682. [Google Scholar] [CrossRef]
- Sales, C.H.; Santos, A.R.d.; Cintra, D.E.C.; Colli, C. Magnesium-Deficient High-Fat Diet: Effects on Adiposity, Lipid Profile and Insulin Sensitivity in Growing Rats. Clin. Nutr. 2014, 33, 879–888. [Google Scholar] [CrossRef]
- Seelig, M.S. Interrelationship of Magnesium and Estrogen in Cardiovascular and Bone Disorders, Eclampsia, Migraine and Premenstrual Syndrome. J. Am. Coll. Nutr. 1993, 12, 442–458. [Google Scholar] [CrossRef]
- Erem, S.; Atfi, A.; Razzaque, M.S. Anabolic Effects of Vitamin D and Magnesium in Aging Bone. J. Steroid Biochem. Mol. Biol. 2019, 193, 105400. [Google Scholar] [CrossRef]
- Welch, A.A.; Skinner, J.; Hickson, M. Dietary Magnesium may be Protective for Aging of Bone and Skeletal Muscle in Middle and Younger Older Age Men and Women: Cross-Sectional Findings from the UK Biobank Cohort. Nutrients 2017, 9, 1189. [Google Scholar] [CrossRef]
- Ghiselli, A.; Rossi, L.; Brighenti, F.; Cairella, G.; D’Amicis, A.; Leclercq, C.; Porrini, M.; Scalfi, L. LARN, Livelli di Assunzione di Riferimento di Nutrienti Ed Energia per la Popolazione Italiana, 4th ed.; SINU: Milano, Italy, 2014. [Google Scholar]
- Institute of Medicine (US) Food and Nutrition Board. Dietary Reference Intakes: A Risk Assessment Model for Establishing Upper Intake Levels for Nutrients. Washington (DC): National Academies Press (US). Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK45188/ (accessed on 17 June 2025).
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Substantiation of Health Claims Related to Magnesium and Electrolyte Balance (ID 238), Energy-yielding Metabolism (ID 240, 247, 248), Neurotransmission and Muscle Contraction Including Heart Muscle (ID 241, 242), Cell Division (ID 365), Maintenance of Bone (ID 239), Maintenance of Teeth (ID 239), Blood Coagulation (ID 357) and Protein Synthesis (ID 364) Pursuant to Article 13 (1) of Regulation (EC) no 1924/2006. EFSA J. 2009, 7, 1216. [Google Scholar]
- Azoulay, A.; Garzon, P.; Eisenberg, M.J. Comparison of the Mineral Content of Tap Water and Bottled Waters. J. Gen. Intern. Med. 2001, 16, 168–175. [Google Scholar] [CrossRef]
- Fine, K.D.; Santa Ana, C.A.; Porter, J.L.; Fordtran, J.S. Intestinal Absorption of Magnesium from Food and Supplements. J. Clin. Investig. 1991, 88, 396–402. [Google Scholar] [CrossRef]
- Miketinas, D.; Luo, H.; Firth, J.A.; Bailey, A.; Bender, T.; Gross, G.; Brink, L. Macronutrient and Micronutrient Intake among US Women Aged 20 to 44 Years. JAMA Netw. Open 2024, 7, e2438460. [Google Scholar] [CrossRef]
- Orlova, S.; Dikke, G.; Pickering, G.; Yaltseva, N.; Konchits, S.; Starostin, K.; Bevz, A. Risk Factors and Comorbidities Associated with Magnesium Deficiency in Pregnant Women and Women with Hormone-Related Conditions: Analysis of a Large Real-World Dataset. BMC Pregnancy Childbirth 2021, 21, 76. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Salvini, S.; Parpinel, M. Food Composition Database for Epidemiological Studies in Italy; Version 1.2022 [Internet]; European Institute of Oncology: Milan, Italy, 2022; Available online: https://bda.ieo.it/ (accessed on 25 May 2025).
- Wang, Z.; Hassan, M.U.; Nadeem, F.; Wu, L.; Zhang, F.; Li, X. Magnesium Fertilization Improves Crop Yield in most Production Systems: A Meta-Analysis. Front. Plant Sci. 2020, 10, 495191. [Google Scholar] [CrossRef]
- Rylander, R.; Mégevand, Y.; Lasserre, B.; Amstutz, W.; Granbom, S. Moderate Alcohol Consumption and Urinary Excretion of Magnesium and Calcium. Scand. J. Clin. Lab. Investig. 2001, 61, 401–405. [Google Scholar] [CrossRef]
- Macías Ruiz, M.D.C.; Cuenca Bermejo, L.; Veronese, N.; Fernández Villalba, E.; González Cuello, A.M.; Kublickiene, K.; Raparelli, V.; Norris, C.M.; Kautzky-Willer, A.; Pilote, L.; et al. Magnesium in Kidney Function and Disease-Implications for Aging and Sex-A Narrative Review. Nutrients 2023, 15, 1710. [Google Scholar] [CrossRef]
- Killilea, D.W.; Maier, J.A. A Connection between Magnesium Deficiency and Aging: New Insights from Cellular Studies. Magnes. Res. Off. Organ Int. Soc. Dev. Res. Magnes. 2008, 21, 77. [Google Scholar]
- Perna, S.; Alalwan, T.A.; Al-Thawadi, S.; Negro, M.; Parimbelli, M.; Cerullo, G.; Gasparri, C.; Guerriero, F.; Infantino, V.; Diana, M. Evidence-Based Role of Nutrients and Antioxidants for Chronic Pain Management in Musculoskeletal Frailty and Sarcopenia in Aging. Geriatrics 2020, 5, 16. [Google Scholar] [CrossRef]
- Ismail, A.A.; Ismail, Y.; Ismail, A.A. Clinical Assessment of Magnesium Status in the Adult: An Overview. Magnes. Hum. Health Dis. 2013, 3–34. [Google Scholar] [CrossRef]
- Piano, F.L.; Corsonello, A.; Corica, F. Magnesium and Elderly Patient: The Explored Paths and the Ones to be Explored: A Review. Magnes. Res. 2019, 32, 1–15. [Google Scholar]
- Kunutsor, S.K.; Whitehouse, M.R.; Blom, A.W.; Laukkanen, J.A. Low Serum Magnesium Levels are Associated with Increased Risk of Fractures: A Long-Term Prospective Cohort Study. Eur. J. Epidemiol. 2017, 32, 593–603. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Mérida, D.M.; Donat-Vargas, C.; Banegas, J.R.; Veronese, N.; Barbagallo, M.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Higher Magnesium Intake is Associated with a Lower Risk of Frailty in Older Adults. J. Am. Med. Dir. Assoc. 2025, 26, 105335. [Google Scholar] [CrossRef]
- Zhou, B.F.; Stamler, J.; Dennis, B.; Moag-Stahlberg, A.; Okuda, N.; Robertson, C.; Zhao, L.; Chan, Q.; Elliott, P. Nutrient Intakes of Middle-Aged Men and Women in China, Japan, United Kingdom, and United States in the Late 1990s: The INTERMAP Study. J. Hum. Hypertens. 2003, 17, 623–630. [Google Scholar] [CrossRef]
- Schiopu, C.; Ștefănescu, G.; Diaconescu, S.; Bălan, G.G.; Gimiga, N.; Rusu, E.; Moldovan, C.A.; Popa, B.; Tataranu, E.; Olteanu, A.V. Magnesium Orotate and the Microbiome–gut–brain Axis Modulation: New Approaches in Psychological Comorbidities of Gastrointestinal Functional Disorders. Nutrients 2022, 14, 1567. [Google Scholar] [CrossRef]
- Crowley, E.K.; Long-Smith, C.M.; Murphy, A.; Patterson, E.; Murphy, K.; O’Gorman, D.M.; Stanton, C.; Nolan, Y.M. Dietary Supplementation with a Magnesium-Rich Marine Mineral Blend Enhances the Diversity of Gastrointestinal Microbiota. Marine Drugs 2018, 16, 216. [Google Scholar] [CrossRef]
- Fransen, F.; van Beek, A.A.; Borghuis, T.; Meijer, B.; Hugenholtz, F.; van der Gaast-de Jongh, C.; Savelkoul, H.F.; de Jonge, M.I.; Faas, M.M.; Boekschoten, M.V.; et al. The Impact of Gut Microbiota on Gender-Specific Differences in Immunity. Front. Immunol. 2017, 8, 754. [Google Scholar] [CrossRef]
- Qi, X.; Yun, C.; Pang, Y.; Qiao, J. The Impact of the Gut Microbiota on the Reproductive and Metabolic Endocrine System. Gut Microbes 2021, 13, 1894070. [Google Scholar] [CrossRef]
- Conlon, M.A.; Bird, A.R. The Impact of Diet and Lifestyle on Gut Microbiota and Human Health. Nutrients 2014, 7, 17–44. [Google Scholar] [CrossRef]
- Melse-Boonstra, A. Bioavailability of Micronutrients from Nutrient-Dense Whole Foods: Zooming in on Dairy, Vegetables, and Fruits. Front. Nutr. 2020, 7, 101. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium—An Update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef]
- Severo, J.S.; Morais, J.B.S.; Freitas, T.d.; Cruz, K.J.C.; Oliveira, A.d.; Poltronieri, F.; Marreiro, D.d.N. Metabolic and Nutritional Aspects of Magnesium. Nutr. Clin. Y Diet. Hosp. 2015, 35, 67–74. [Google Scholar]
- Nielsen, F.H.; Milne, D.B. A Moderately High Intake Compared to a Low Intake of Zinc Depresses Magnesium Balance and Alters Indices of Bone Turnover in Postmenopausal Women. Eur. J. Clin. Nutr. 2004, 58, 703–710. [Google Scholar] [CrossRef]
- Deng, X.; Song, Y.; Manson, J.E.; Signorello, L.B.; Zhang, S.M.; Shrubsole, M.J.; Ness, R.M.; Seidner, D.L.; Dai, Q. Magnesium, Vitamin D Status and Mortality: Results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III. BMC Med. 2013, 11, 187. [Google Scholar] [CrossRef]
- Pouteau, E.; Kabir-Ahmadi, M.; Noah, L.; Mazur, A.; Dye, L.; Hellhammer, J.; Pickering, G.; DuBray, C. Superiority of Combined Magnesium (MG) and Vitamin B6 (VITB6) Supplementation Over Magnesium Alone on Severe Stress in Adults with Low Magnesemia: A Randomised, Single Blind Trial. Clin. Nutr. 2018, 37, S289–S290. [Google Scholar] [CrossRef]
- Vegarud, G.E.; Langsrud, T.; Svenning, C. Mineral-Binding Milk Proteins and Peptides; Occurrence, Biochemical and Technological Characteristics. Br. J. Nutr. 2000, 84, 91–98. [Google Scholar] [CrossRef]
- KITANO, T.; ESASHI, T.; AZAMI, S. Effect of Protein Intake on Mineral (Calcium, Magnesium, and Phosphorus) Balance in Japanese Males. J. Nutr. Sci. Vitaminol. 1988, 34, 387–398. [Google Scholar] [CrossRef]
- Johnson, S. The Multifaceted and Widespread Pathology of Magnesium Deficiency. Med. Hypotheses 2001, 56, 163–170. [Google Scholar] [CrossRef]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, S.; Montalcini, T.; Pujia, A. Mediterranean Diet in Healthy Aging. J. Nutr. Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean Diet and Health Status: Active Ingredients and Pharmacological Mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef]
- Pierre-Anne, R.L.; Stallard, N.; Momenian, Y.; Oshirak, K.; Stella, L.V. Magnesium Intake in the Mediterranean Diet. In Food Safety; Ahmad, R.S., Ed.; IntechOpen: Rijeka, Croatia, 2022; Chapter 8. [Google Scholar]
- Barrea, L.; Verde, L.; Suárez, R.; Frias-Toral, E.; Vásquez, C.A.; Colao, A.; Savastano, S.; Muscogiuri, G. Sex-Differences in Mediterranean Diet: A Key Piece to Explain Sex-Related Cardiovascular Risk in Obesity? A Cross-Sectional Study. J. Transl. Med. 2024, 22, 44. [Google Scholar] [CrossRef]
- Rose, L.; Wood, A.; Gill, T. Gender Differences in Adherence and Retention in Mediterranean Diet Interventions with a Weight-Loss Outcome: A Systematic Review and Meta-Analysis. Obes. Rev. 2024, 25, e13824. [Google Scholar] [CrossRef]
- Ostfeld, R.J. Definition of a Plant-Based Diet and Overview of this Special Issue. J. Geriatr. Cardiol. 2017, 14, 315. [Google Scholar]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef]
- Koebnick, C.; Leitzmann, R.; García, A.L.; Heins, U.A.; Heuer, T.; Golf, S.; Katz, N.; Hoffmann, I.; Leitzmann, C. Long-Term Effect of a Plant-Based Diet on Magnesium Status during Pregnancy. Eur. J. Clin. Nutr. 2005, 59, 219–225. [Google Scholar] [CrossRef]
- López-Moreno, M.; Garcés-Rimón, M.; Miguel, M. Antinutrients: Lectins, Goitrogens, Phytates and Oxalates, Friends Or Foe? J. Funct. Foods 2022, 89, 104938. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Redondo-Flórez, L.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Global Impacts of Western Diet and its Effects on Metabolism and Health: A Narrative Review. Nutrients 2023, 15, 2749. [Google Scholar] [CrossRef]
- Moshfegh, A.; Goldman, J.; Ahuja, J.; Rhodes, D.; LaComb, R. What We Eat in America, NHANES 2005–2006: Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorus, and Magnesium; U.S. Department of Agriculture, Agricultural Research Service: Beltsville, MD, USA, 2009. Available online: http://www.ars.usda.gov/ba/bhnrc/fsrg2 (accessed on 26 May 2025).
- Shah, N.C.; Shah, G.J.; Li, Z.; Jiang, X.; Altura, B.T.; Altura, B.M. Short-Term Magnesium Deficiency Downregulates Telomerase, Upregulates Neutral Sphingomyelinase and Induces Oxidative DNA Damage in Cardiovascular Tissues: Relevance to Atherogenesis, Cardiovascular Diseases and Aging. Int. J. Clin. Exp. Med. 2014, 7, 497. [Google Scholar]
- Shakersain, B.; Santoni, G.; Larsson, S.C.; Faxén-Irving, G.; Fastbom, J.; Fratiglioni, L.; Xu, W. Prudent Diet may Attenuate the Adverse Effects of Western Diet on Cognitive Decline. Alzheimer’s Dement. 2016, 12, 100–109. [Google Scholar] [CrossRef]
- D’Amico, D.; Parrott, M.D.; Greenwood, C.E.; Ferland, G.; Gaudreau, P.; Belleville, S.; Laurin, D.; Anderson, N.D.; Kergoat, M.; Morais, J.A.; et al. Sex Differences in the Relationship between Dietary Pattern Adherence and Cognitive Function among Older Adults: Findings from the NuAge Study. Nutr. J. 2020, 19, 58. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mg2+ Actions | Women | Men | References |
|---|---|---|---|
| Hormonal Regulation | Estrogen enhances Mg2+ absorption and retention; levels decline after menopause, increasing deficiency risk. | Stable absorption; Mg2+ positively influences testosterone levels; deficiency may impair anabolic hormone production. | [21,93,95,109] |
| Life Stages Requirements | Increased requirements during pregnancy, lactation, and menopause; hormonal fluctuations affect Mg2+ homeostasis. | Higher needs among physically active men; aging reduces absorption efficiency and increases urinary loss. | [46,50,52,93] |
| Body Composition | More subcutaneous fat; menopause increases visceral fat; low Mg2+ linked to altered body composition and inflammation. | Higher visceral fat accumulation; inverse association between Mg2+ intake and waist circumference. | [15,16,84,86,87,107] |
| Metabolic Effects | Mg2+ modulates insulin sensitivity, especially during hormonal fluctuations; impacts premenstrual symptoms and metabolic stability. | Supports insulin sensitivity, glucose regulation, and testosterone balance; influences metabolic efficiency. | [31,58,70,89] |
| Bone and Musculoskeletal Health | Supports bone mineralization; deficiency post-menopause increases osteoporosis risk. | Essential for bone integrity and muscle maintenance; deficiency linked to sarcopenia in aging men. | [89,110,111] |
| Neurological and Emotional Effects | Regulates neurotransmitters, mood, and neuromuscular balance; involved in PMS, menstrual migraines, and dysmenorrhea management. | Contributes to neuromuscular function and muscle performance; Mg2+ status associated with muscle strength and functionality. | [56,69,80,88,99] |
| Gender | Group (Years) | LARN 2024 (Italy) [112] AIs | IOM (USA) [113] RDAs | EFSA (EU) [114] AIs |
|---|---|---|---|---|
| Men | 7–12 months | 80 | 75 | 80 |
| 1–3 years | 120 | 80 | 170 | |
| 4–6 years | 150 | 130 | 230 | |
| 7–10 years | 220 | 240 | 230 | |
| 11–14 years | 290 | 240 | 300 | |
| 15–18 years | 380 | 410 | 300 | |
| 19–69 years | 350 | 400 | 350 | |
| ≥70 years | 350 | 400 | 350 | |
| Women | 7–12 months | 80 | 75 | 80 |
| 1–3 years | 120 | 80 | 170 | |
| 4–6 years | 150 | 130 | 230 | |
| 7–10 years | 220 | 240 | 230 | |
| 11–14 years | 290 | 240 | 250 | |
| 15–18 years | 380 | 360 | 250 | |
| 19–69 years | 350 | 310 | 300 | |
| ≥70 years | 350 | 310 | 300 | |
| Pregnancy | 350 | 400–350 * | 300 | |
| Lactation | 350 | 310–360 § | 300 |
| Category | Food Item | Magnesium (mg/100 g) | Magnesium (mg/Serving) | Standard Serving Size |
|---|---|---|---|---|
| Nuts and Seeds | Almonds | 264 | 79 | 30 g |
| Pine nuts | 270 | 81 | 30 g | |
| Cashew nuts | 260 | 78 | 30 g | |
| Peanuts, raw | 210 | 63 | 30 g | |
| Whole Grains | Quinoa, raw | 189 | 189 | 100 g |
| Oat, raw | 177 | 177 | 100 g | |
| Wheat, durum | 160 | 160 | 100 g | |
| Rice, brown, wholegrain, raw | 116 | 116 | 100 g | |
| Millet, shelled | 160 | 160 | 100 g | |
| Leafy Greens | Spinach | 60 | 120 | 200 g |
| Swiss chard | 81 | 162 | 200 g | |
| Fish and Seafood | Shrimp or prawn | 43 | 65 | 150 g |
| Mackerel | 21 | 42 | 200 g | |
| Dairy Products | Low-fat yogurt | 18 | 27 | 150 g |
| Milk | 11 | 33 | 300 mL | |
| Chocolate and Derivatives | Dark chocolate (≥70%) | 230 | 115 | 50 g |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazza, E.; Maurotti, S.; Ferro, Y.; Castagna, A.; Pujia, C.; Sciacqua, A.; Pujia, A.; Montalcini, T. Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake. Nutrients 2025, 17, 2226. https://doi.org/10.3390/nu17132226
Mazza E, Maurotti S, Ferro Y, Castagna A, Pujia C, Sciacqua A, Pujia A, Montalcini T. Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake. Nutrients. 2025; 17(13):2226. https://doi.org/10.3390/nu17132226
Chicago/Turabian StyleMazza, Elisa, Samantha Maurotti, Yvelise Ferro, Alberto Castagna, Carmelo Pujia, Angela Sciacqua, Arturo Pujia, and Tiziana Montalcini. 2025. "Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake" Nutrients 17, no. 13: 2226. https://doi.org/10.3390/nu17132226
APA StyleMazza, E., Maurotti, S., Ferro, Y., Castagna, A., Pujia, C., Sciacqua, A., Pujia, A., & Montalcini, T. (2025). Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake. Nutrients, 17(13), 2226. https://doi.org/10.3390/nu17132226