
Development, Validity, and Reliability of a Food Frequency Questionnaire for Omani Adults


 ,
,  , ,
, ,
Abstract
1. Introduction
1.1. Prevalence of Overweight and Obesity in Oman
1.2. Non-Communicable Diseases in Oman
2. Materials and Methods
2.1. Ethical Approval
2.2. Development of the Food Frequency Questionnaire
2.2.1. Modifications to the Food Frequency Questionnaire
2.2.2. Face and Content Validity
2.2.3. Pilot Testing
2.2.4. Components of the Food Frequency Questionnaire
2.3. Reliability Study
2.3.1. Study Population and Sample Size
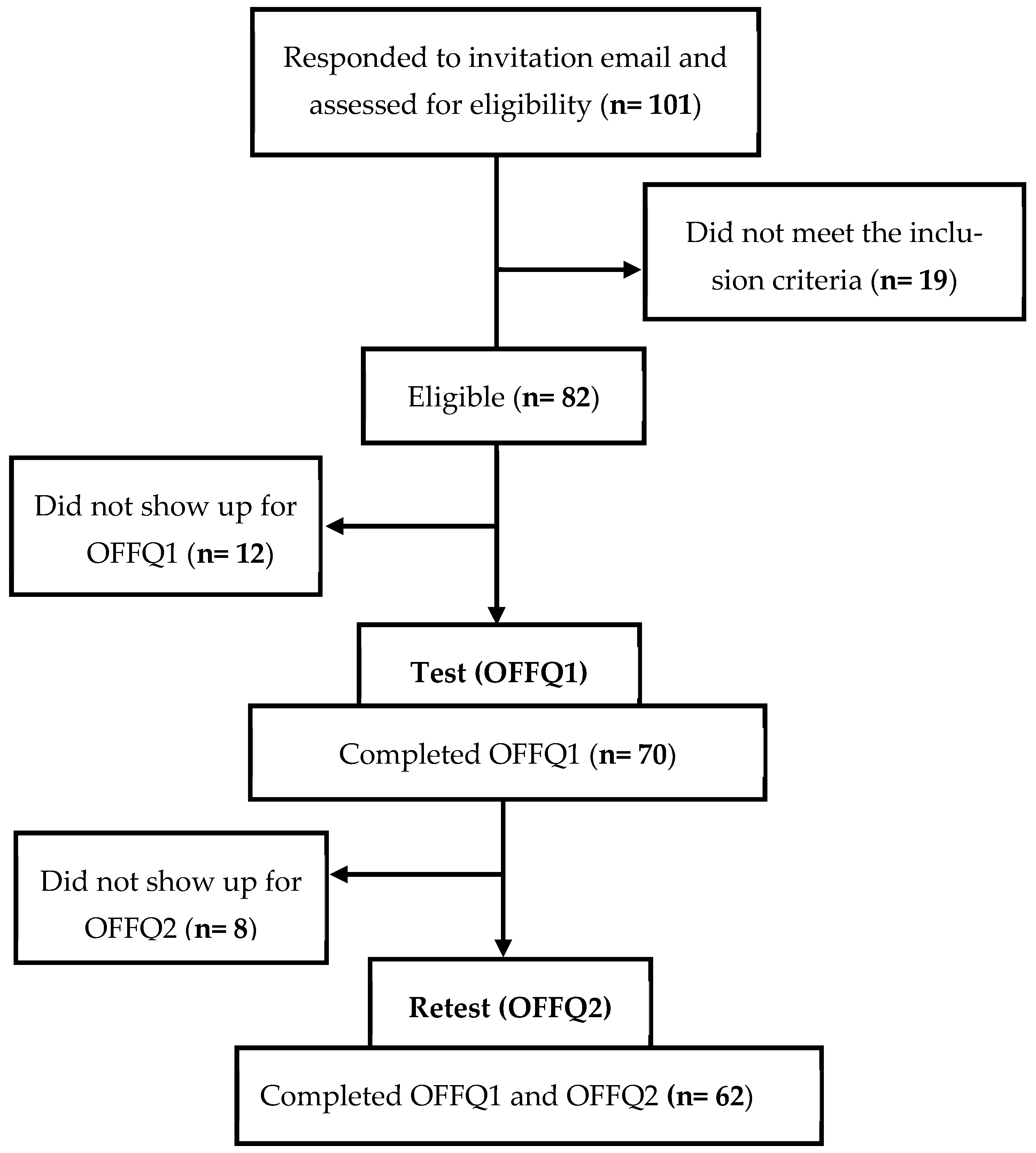
2.3.2. Recruitment and Screening Process
2.3.3. Inclusion and Exclusion Criteria
2.3.4. Procedure for Data Collection
2.4. Data Management
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Reliability Study Sample
3.2. Test–Retest Reliability
3.3. Internal Consistency
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alkerwi, A. Diet quality concept. Nutrition 2014, 30, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Wirt, A.; Collins, C.E. Diet quality–what is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef]
- McNaughton, S.A. Dietary patterns and diet quality: Approaches to assessing complex exposures in nutrition. Australas. Epidemiol. 2010, 17, 35–37. [Google Scholar]
- Angelopoulos, P.; Kourlaba, G.; Kondaki, K.; Fragiadakis, G.A.; Manios, Y. Assessing children’s diet quality in Crete based on Healthy Eating Index: The Children Study. Eur. J. Clin. Nutr. 2009, 63, 964–969. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.; Bassett, J. What can we learn from dietary pattern analysis? Public Health Nutr. 2016, 19, 191–194. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Gerber, M. The comprehensive approach to diet: A critical review. J. Nutr. 2001, 131, 3051S–3055S. [Google Scholar] [CrossRef]
- Agnoli, C.; Pounis, G.; Krogh, V. Dietary pattern analysis. In Analysis in Nutrition Research; Elsevier: Amsterdam, The Netherlands, 2019; pp. 75–101. [Google Scholar]
- Pinto, A.; Severo, M.; Oliveira, A. Use of a hybrid method to derive dietary patterns in 7 years olds with explanatory ability of body mass index at age 10. Eur. J. Clin. Nutr. 2021, 75, 1598–1606. [Google Scholar] [CrossRef]
- Ocké, M.C. Evaluation of methodologies for assessing the overall diet: Dietary quality scores and dietary pattern analysis. Proc. Nutr. Soc. 2013, 72, 191–199. [Google Scholar] [CrossRef]
- Schulze, M.B.; Hoffmann, K.; Kroke, A.; Boeing, H. An approach to construct simplified measures of dietary patterns from exploratory factor analysis. Br. J. Nutr. 2003, 89, 409–419. [Google Scholar] [CrossRef]
- Previdelli, Á.N.; de Andrade, S.C.; Fisberg, R.M.; Marchioni, D.M. Using two different approaches to assess dietary patterns: Hypothesis-driven and data-driven analysis. Nutrients 2016, 8, 593. [Google Scholar] [CrossRef]
- Hoffmann, K.; Schulze, M.B.; Schienkiewitz, A.; Nöthlings, U.; Boeing, H. Application of a new statistical method to derive dietary patterns in nutritional epidemiology. Am. J. Epidemiol. 2004, 159, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Satija, A.; Rimm, E.B.; Spiegelman, D.; Sampson, L.; Rosner, B.; Camargo, C.A., Jr.; Stampfer, M.; Willett, W.C. Diet assessment methods in the nurses’ health studies and contribution to evidence-based nutritional policies and guidelines. Am. J. Public Health 2016, 106, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Lenart, E. Reproducibility and validity of food frequency questionnaires. Nutr. Epidemiol. 2013, 122, 51–65. [Google Scholar]
- Walton, J. Dietary assessment methodology for nutritional assessment. Top. Clin. Nutr. 2015, 30, 33–46. [Google Scholar] [CrossRef]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 24 July 2024).
- Al-Lawati, J.A.; Mabry, R.; Mohammed, A.J. Addressing the threat of chronic diseases in Oman. Prev. Chronic Dis. 2008, 5, A99. [Google Scholar]
- Al-Riyami, A.A.; Afifi, M.M. Prevalence and correlates of obesity and central obesity among Omani adults. Saudi Med. J. 2003, 24, 641–646. [Google Scholar]
- Al-Mawali, A.; Jayapal, S.K.; Morsi, M.; Al-Shekaili, W.; Pinto, A.D.; Al-Kharusi, H.; Al-Harrasi, A.; Al-Balushi, Z.; Idikula, J. Prevalence of risk factors of non-communicable diseases in the Sultanate of Oman: STEPS survey 2017. PLoS ONE 2021, 16, e0259239. [Google Scholar] [CrossRef]
- Badran, M.; Laher, I. Obesity in Arabic-speaking countries. J. Obes. 2011, 2011, 686430. [Google Scholar] [CrossRef]
- Okati-Aliabad, H.; Ansari-Moghaddam, A.; Kargar, S.; Jabbari, N. Prevalence of obesity and overweight among adults in the Middle East countries from 2000 to 2020: A systematic review and meta-analysis. J. Obes. 2022, 2022, 8074837. [Google Scholar] [CrossRef] [PubMed]
- Al-Mawali, A. Non-communicable diseases: Shining a light on cardiovascular disease, Oman’s biggest killer. Oman Med. J. 2015, 30, 227. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Fact Sheet. 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 24 July 2024).
- World Health Organization. Noncommunicable Diseases: Progress Monitor 2022. Available online: https://iris.who.int/handle/10665/353048 (accessed on 15 January 2023).
- Subar, A.F.; Thompson, F.E.; Kipnis, V.; Midthune, D.; Hurwitz, P.; McNutt, S.; McIntosh, A.; Rosenfeld, S. Comparative validation of the Block, Willett, and National Cancer Institute food frequency questionnaires: The Eating at America’s Table Study. Am. J. Epidemiol. 2001, 154, 1089–1099. [Google Scholar] [CrossRef]
- Kristal, A.R.; Kolar, A.S.; Fisher, J.L.; Plascak, J.J.; Stumbo, P.J.; Weiss, R.; Paskett, E.D. Evaluation of web-based, self-administered, graphical food frequency questionnaire. J. Acad. Nutr. Diet. 2014, 114, 613–621. [Google Scholar] [CrossRef]
- Fallaize, R.; Forster, H.; Macready, A.L.; Walsh, M.C.; Mathers, J.C.; Brennan, L.; Gibney, E.R.; Gibney, M.J.; Lovegrove, J.A. Online dietary intake estimation: Reproducibility and validity of the Food4Me food frequency questionnaire against a 4-day weighed food record. J. Med. Internet Res. 2014, 16, e3355. [Google Scholar] [CrossRef]
- Labonté, M.-È.; Cyr, A.; Baril-Gravel, L.; Royer, M.; Lamarche, B. Validity and reproducibility of a web-based, self-administered food frequency questionnaire. Eur. J. Clin. Nutr. 2012, 66, 166–173. [Google Scholar] [CrossRef]
- Liu, L.; Wang, P.P.; Roebothan, B.; Ryan, A.; Tucker, C.S.; Colbourne, J.; Baker, N.; Cotterchio, M.; Yi, Y.; Sun, G. Assessing the validity of a self-administered food-frequency questionnaire (FFQ) in the adult population of Newfoundland and Labrador, Canada. Nutr. J. 2013, 12, 49. [Google Scholar] [CrossRef]
- Dehghan, M.; Al-Hamad, N.; McMillan, C.R.; Prakash, P.; Merchant, A.T. Comparison of a semi-quantitative food frequency questionnaire with 24-hour dietary recalls to assess dietary intake of adult Kuwaitis. Saudi Med. J. 2009, 30, 159–161. [Google Scholar]
- Alawadhi, B.; Fallaize, R.; Franco, R.Z.; Hwang, F.; Lovegrove, J. Web-based dietary intake estimation to assess the reproducibility and relative validity of the eatwellq8 food frequency questionnaire: Validation study. JMIR Form. Res. 2021, 5, e13591. [Google Scholar] [CrossRef]
- Bawadi, H.; Akasheh, R.T.; Kerkadi, A.; Haydar, S.; Tayyem, R.; Shi, Z. Validity and reproducibility of a food frequency questionnaire to assess macro and micro-nutrient intake among a convenience cohort of healthy adult Qataris. Nutrients 2021, 13, 2002. [Google Scholar] [CrossRef]
- Gosadi, I.M.; Alatar, A.A.; Otayf, M.M.; AlJahani, D.M.; Ghabbani, H.M.; AlRajban, W.A.; Alrsheed, A.M.; Al-Nasser, K.A. Development of a Saudi Food Frequency Questionnaire and testing its reliability and validity. Saudi Med. J. 2017, 38, 636. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires–A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Background on Diet History Questionnaire II (DHQ-II) for U.S. & Canada. 2023. Available online: https://epi.grants.cancer.gov/dhq2/about/ (accessed on 30 January 2024).
- Musaiger, A.O. Food Composition Tables for Arab Gulf Countries (Gulfoods); Arab Center for Nutrition: Manama, Bahrain, 2006. [Google Scholar]
- Sawaya, W.N.; Al-Awadi, F.; Eid, N.; Dashti, B.H. Food Composition Kuwaiti Composite Dishes, 1st ed.; Kuwaiti Institute for Scientific Research (KISR) Press, 1998. [Google Scholar]
- United States Department of Agriculture. Food Data Central. 2024. Available online: https://fdc.nal.usda.gov/ (accessed on 13 August 2024).
- Data Mining. Estebyan. 2024. Available online: https://eqp.datamining.om/ (accessed on 13 August 2024).
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef]
- Collins, C.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.; Hutchesson, M.J.; Burrows, T.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Aoun, C.; Bou Daher, R.; El Osta, N.; Papazian, T.; Khabbaz, L.R. Reproducibility and relative validity of a food frequency questionnaire to assess dietary intake of adults living in a Mediterranean country. PLoS ONE 2019, 14, e0218541. [Google Scholar] [CrossRef]
- Shahar, S.; Shahril, M.R.; Abdullah, N.; Borhanuddin, B.; Kamaruddin, M.A.; Yusuf, N.A.M.; Dauni, A.; Rosli, H.; Zainuddin, N.S.; Jamal, R. Development and relative validity of a semiquantitative food frequency questionnaire to estimate dietary intake among a multi-ethnic population in the Malaysian Cohort Project. Nutrients 2021, 13, 1163. [Google Scholar] [CrossRef]
- Sam, C.H.; Skeaff, S.; Skidmore, P.M. A comprehensive FFQ developed for use in New Zealand adults: Reliability and validity for nutrient intakes. Public Health Nutr. 2014, 17, 287–296. [Google Scholar] [CrossRef]
- Kelemen, L.E.; Anand, S.S.; Vuksan, V.; Yi, Q.; Teo, K.K.; Devanesen, S.; Yusuf, S. Development and evaluation of cultural food frequency questionnaires for South Asians, Chinese, and Europeans in North America. J. Am. Diet. Assoc. 2003, 103, 1178–1184. [Google Scholar] [CrossRef]
- Zhuang, M.; Yuan, Z.; Lin, L.; Hu, B.; Wang, X.; Yang, Y.; Chen, X.; Jin, L.; Lu, M.; Ye, W. Reproducibility and relative validity of a food frequency questionnaire developed for adults in Taizhou, China. PLoS ONE 2012, 7, e48341. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Tayyem, R.F.; Abu-Mweis, S.S.; Bawadi, H.A.; Agraib, L.; Bani-Hani, K. Validation of a food frequency questionnaire to assess macronutrient and micronutrient intake among Jordanians. J. Acad. Nutr. Diet. 2014, 114, 1046–1052. [Google Scholar] [CrossRef]
- El Kinany, K.; Garcia-Larsen, V.; Khalis, M.; Deoula, M.M.S.; Benslimane, A.; Ibrahim, A.; Benjelloun, M.C.; El Rhazi, K. Adaptation and validation of a food frequency questionnaire (FFQ) to assess dietary intake in Moroccan adults. Nutr. J. 2018, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Flood, V.M.; Wen, L.M.; Hardy, L.L.; Rissel, C.; Simpson, J.M.; Baur, L.A. Reliability and validity of a short FFQ for assessing the dietary habits of 2–5-year-old children, Sydney, Australia. Public Health Nutr. 2014, 17, 498–509. [Google Scholar] [CrossRef]
- El Sayed Ahmad, R.; Baroudi, M.; Shatila, H.; Nasreddine, L.; Chokor, F.A.Z.; Chehab, R.F.; Forman, M.R.; Naja, F. Validity and reproducibility of a culture-specific food frequency questionnaire in Lebanon. Nutrients 2020, 12, 3316. [Google Scholar] [CrossRef]
- Athanasiadou, E.; Kyrkou, C.; Fotiou, M.; Tsakoumaki, F.; Dimitropoulou, A.; Polychroniadou, E.; Menexes, G.; Athanasiadis, A.P.; Biliaderis, C.G.; Michaelidou, A.-M. Development and validation of a Mediterranean oriented culture-specific semi-quantitative food frequency questionnaire. Nutrients 2016, 8, 522. [Google Scholar] [CrossRef] [PubMed]
- Marchioni, D.M.L.; Voci, S.M.; Lima, F.E.L.d.; Fisberg, R.M.; Slater, B. Reproducibility of a food frequency questionnaire for adolescents. Cad. Saude Publica 2007, 23, 2187–2196. [Google Scholar] [CrossRef]
- Gliem, J.A.; Gliem, R.R. Calculating, interpreting, and reporting Cronbach’s alpha reliability coefficient for Likert-type scales. In Proceedings of the Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education, Columbus, OH, USA, 9–11 October 2003; pp. 82–87. [Google Scholar]
- Marshidi, S.; Kaur, S.; Chin, K.H.; Ulaganathan, V.; Tarif, M. Development, Validation, and Reproducibility of a Food Frequency Questionnaire (FFQ) for Adult Population in Brunei Darussalam. Malays. J. Med. Health Sci. 2024, 20, 1. [Google Scholar] [CrossRef]
- Nindya, T.S.; Mahmudiono, T.; Rachmah, Q. The estimation of cholesterol intake in elderly: Reliability and validity of short, Semi-Quantitative Food Frequency Questionnaire (SQ-FFQ). J. Nutr. Health 2021, 54, 95–103. [Google Scholar] [CrossRef]
- Cade, J.E.; Burley, V.J.; Warm, D.L.; Thompson, R.L.; Margetts, B.M. Food-frequency questionnaires: A review of their design, validation and utilisation. Nutr. Res. Rev. 2004, 17, 5–22. [Google Scholar] [CrossRef]
- Block, G.; Hartman, A.M. Issues in reproducibility and validity of dietary studies. Am. J. Clin. Nutr. 1989, 50, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Bohlscheid-Thomas, S.; Hoting, I.; Boeing, H.; Wahrendorf, J. Reproducibility and relative validity of food group intake in a food frequency questionnaire developed for the German part of the EPIC project. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26, S59–S70. [Google Scholar] [CrossRef] [PubMed]
- Toorang, F.; Sasanfar, B.; Jahromi, S.R.; Koujan, S.E.; Narmcheshm, S.; Rafei, A.; Zendehdel, K. Validation of diet history questionnaire in assessing energy and nutrient intakes of Iranian population. Iran. J. Public Health 2019, 48, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Kowalkowska, J.; Slowinska, M.A.; Slowinski, D.; Dlugosz, A.; Niedzwiedzka, E.; Wadolowska, L. Comparison of a full food-frequency questionnaire with the three-day unweighted food records in young Polish adult women: Implications for dietary assessment. Nutrients 2013, 5, 2747–2776. [Google Scholar] [CrossRef]
- Rockett, H.R.; Berkey, C.S.; Colditz, G.A. Comparison of a short food frequency questionnaire with the Youth/Adolescent Questionnaire in the Growing Up Today Study. Int. J. Pediatr. Obes. 2007, 2, 31–39. [Google Scholar] [CrossRef]

{kind=link}
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 3 (23%) |
| Female | 10 (77%) |
| Age (years) | |
| 18–24 | 8 (61.5%) |
| ≥25 | 5 (38.5%) |
| Permanent Residency (Governorate) | |
| Al Dakhiliyah | 2 (15.4%) |
| Al Dhahirah | 1 (7.7%) |
| North Al Batinah | 1 (7.7%) |
| South Al Batinah | 3 (23%) |
| Musandam | 1 (7.7%) |
| Muscat | 3 (23%) |
| North Al Sharqiyah | 2 (15.4%) |
| Employment status | |
| Employee | 5 (38.5%) |
| Student | 8 (61.5%) |
| Highest level of education | |
| High school | 7 (53.8%) |
| Postgraduate degree | 6 (46.2%) |
| Marital status | |
| Married | 4 (30.8%) |
| Unmarried | 9 (69.2%) |
| Individual monthly income (OMR) | |
| Less than 500 | 7 (53.8%) |
| More than 500 | 6 (46.2%) |
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 30 (48.4%) |
| Female | 32 (51.6%) |
| Age (years) | |
| 18–24 | 50 (80.6%) |
| ≥25 | 12 (19.4%) |
| Permanent Residency (Governorate) | |
| Al Dakhiliyah | 13 (21%) |
| Al Dhahirah | 7 (11.3%) |
| North Al Batinah | 7 (11.3%) |
| South Al Batinah | 9 (14.5%) |
| Musandam | 1 (1.6%) |
| Al Buraymi | 1 (1.6%) |
| Muscat | 21 (33.9%) |
| Dhofar | 3 (4.8%) |
| Employment status | |
| Employee | 8 (12.9%) |
| Student | 54 (87.1%) |
| Highest level of education | |
| High school | 45 (72.6%) |
| Post-secondary diploma | 4 (6.5%) |
| Postgraduate degree | 13 (21%) |
| Marital status | |
| Married | 4 (6.5%) |
| Unmarried | 58 (93.5%) |
| Individual monthly income (OMR) | |
| No source of income | 31 (50%) |
| Less than 500 | 22 (35.5%) |
| More than 500 | 9 (14.5%) |
| BMI (kg/m2) | |
| <25 | 40 (64.5%) |
| 25–29.9 | 15 (24.2%) |
| ≥30 | 7 (11.3%) |
| Food Group | KW a | ICC b |
|---|---|---|
| Beverages | 0.545 | 0.725 |
| Fruits | 0.548 | 0.803 |
| Vegetables, potatoes, dried beans | 0.488 | 0.745 |
| Soups, Middle Eastern foods | 0.601 | 0.807 |
| Rice, pasta, pizza | 0.476 | 0.705 |
| Cereal, qaroos, breads | 0.425 | 0.709 |
| Date molasses, jam, peanut butter | 0.513 | 0.735 |
| Mashakik, shiwa, cold cuts | 0.379 | 0.576 |
| Meat, poultry, fish | 0.468 | 0.689 |
| Eggs, meat alternatives | 0.398 | 0.569 |
| Chips, rusk, other snacks | 0.524 | 0.773 |
| Yoghurt, cheese | 0.427 | 0.716 |
| Sweets, baked goods, desserts | 0.395 | 0.695 |
| Food Group | KW a | ICC b |
|---|---|---|
| Beverages | 0.500 | 0.692 |
| Fruits | 0.429 | 0.696 |
| Vegetables, potatoes, dried beans | 0.422 | 0.639 |
| Soups, Middle Eastern foods | 0.580 | 0.821 |
| Rice, pasta, pizza | 0.432 | 0.656 |
| Cereal, qaroos, breads | 0.401 | 0.639 |
| Date molasses, jam, peanut butter | 0.462 | 0.728 |
| Mashakik, shiwa, cold cuts | 0.403 | 0.713 |
| Meat, poultry, fish | 0.481 | 0.727 |
| Eggs, meat alternatives | 0.551 | 0.793 |
| Chips, rusk, other snacks | 0.489 | 0.697 |
| Yoghurt, cheese | 0.259 | 0.395 |
| Sweets, baked goods, desserts | 0.402 | 0.621 |
| Test | Retest | |
|---|---|---|
| Food Group | Cronbach’s α | Cronbach’s α |
| Beverages | 0.386 | 0.502 |
| Fruits | 0.789 | 0.798 |
| Vegetables, potatoes, dried beans | 0.863 | 0.871 |
| Soups, Middle Eastern foods | 0.390 | 0.267 |
| Rice, pasta, pizza | 0.500 | 0.484 |
| Cereal, qaroos, breads | 0.560 | 0.516 |
| Date molasses, jam, peanut butter | 0.330 | 0.414 |
| Mashakik, shiwa, cold cuts | 0.502 | 0.347 |
| Meat, poultry, fish | 0.700 | 0.751 |
| Eggs, meat alternatives | - | - |
| Chips, rusk, other snacks | 0.568 | 0.633 |
| Yoghurt, cheese | 0.455 | 0.293 |
| Sweets, baked goods, desserts | 0.744 | 0.720 |
| Test | Retest | |
|---|---|---|
| Food Group | Cronbach’s α | Cronbach’s α |
| Beverages | - | - |
| Fruits | - | - |
| Vegetables, potatoes, dried beans | - | - |
| Soups, Middle Eastern foods | 0.603 | 0.593 |
| Rice, pasta, pizza | - | 0.810 |
| Cereal, qaroos, breads | 0.731 | 0.955 |
| Date molasses, jam, peanut butter | 0.520 | 0.272 |
| Mashakik, shiwa, cold cuts | 0.645 | 0.538 |
| Meat, poultry, fish | - | - |
| Eggs, meat alternatives | - | - |
| Chips, rusk, other snacks | - | - |
| Yoghurt, cheese | 0.404 | 0.286 |
| Sweets, baked goods, desserts | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Uraimi, T.; Al Subhi, L.K.; Waly, M.; Al Rizeiqi, M.; Al Balushi, R.; Al Kharusi, A. Development, Validity, and Reliability of a Food Frequency Questionnaire for Omani Adults. Nutrients 2025, 17, 2220. https://doi.org/10.3390/nu17132220
Al Uraimi T, Al Subhi LK, Waly M, Al Rizeiqi M, Al Balushi R, Al Kharusi A. Development, Validity, and Reliability of a Food Frequency Questionnaire for Omani Adults. Nutrients. 2025; 17(13):2220. https://doi.org/10.3390/nu17132220
Chicago/Turabian StyleAl Uraimi, Tasnim, Lyutha K. Al Subhi, Mostafa Waly, Mohammed Al Rizeiqi, Ruqaiya Al Balushi, and Aaisha Al Kharusi. 2025. "Development, Validity, and Reliability of a Food Frequency Questionnaire for Omani Adults" Nutrients 17, no. 13: 2220. https://doi.org/10.3390/nu17132220
APA StyleAl Uraimi, T., Al Subhi, L. K., Waly, M., Al Rizeiqi, M., Al Balushi, R., & Al Kharusi, A. (2025). Development, Validity, and Reliability of a Food Frequency Questionnaire for Omani Adults. Nutrients, 17(13), 2220. https://doi.org/10.3390/nu17132220